TIM-3 Genetic Variants Are Associated with Altered Clinical Outcome and Susceptibility to Gram-Positive Infections in Patients with Sepsis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Collective
2.2. Data Collection
2.3. Genotyping
2.4. Statistical Analysis
2.5. Data Availability
3. Results
3.1. Allele Distribution and Linkage Disequilibrium Analysis
3.2. Baseline Characteristics
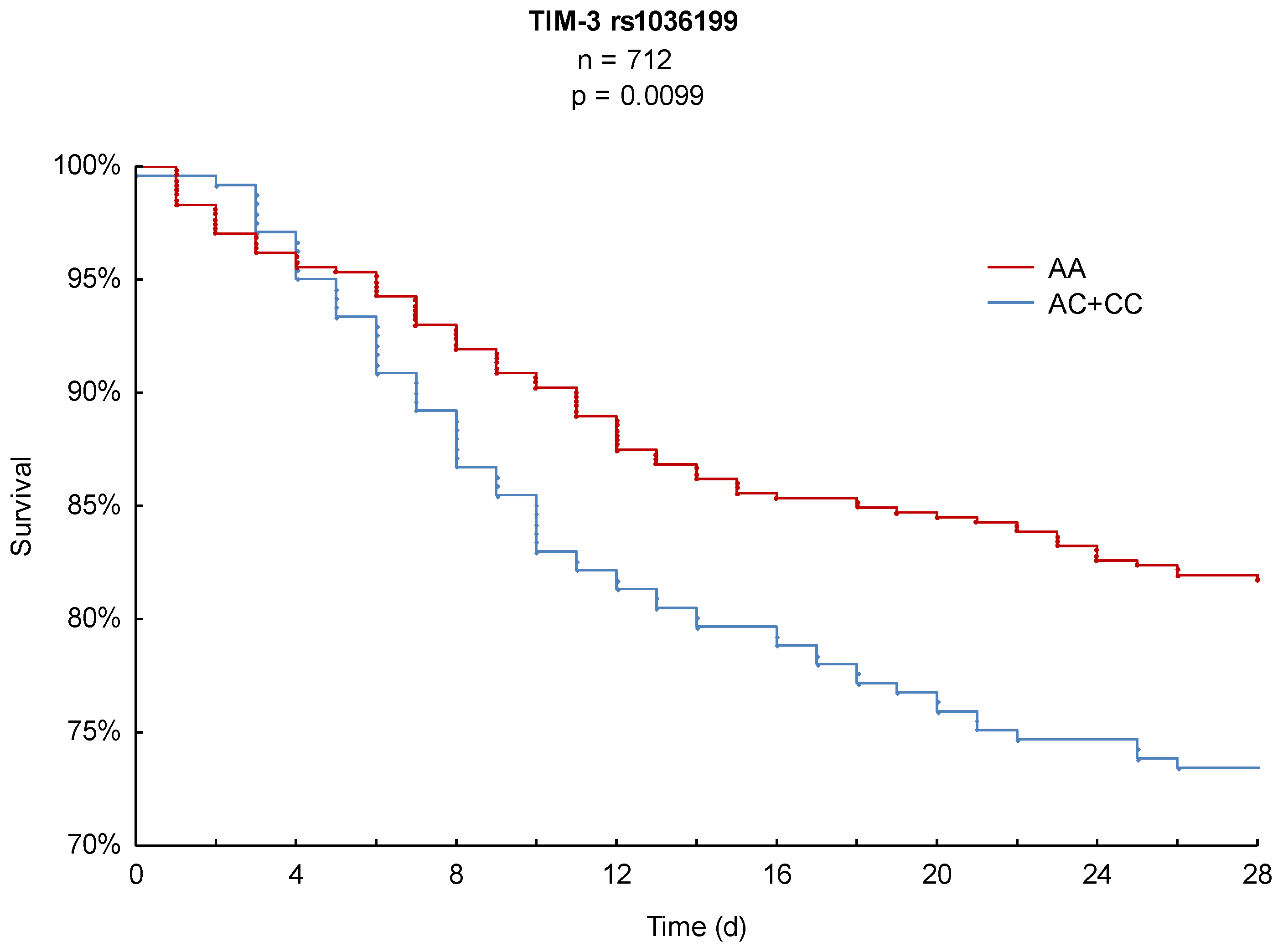
3.3. Kaplan–Meier Survival Analysis
3.4. Disease Severity
3.5. Microbiological Analysis
3.6. Multivariate Cox Regression Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| APACHE | Acute Physiology and Chronic Health Evaluation |
| BMI | Body mass index |
| CD4+ | CD4-positive T cell |
| CD8+ | CD8-positive cytotoxic T cell |
| COPD | Chronic obstructive pulmonary disease |
| CRF | Clinical report form |
| CRP | C-reactive protein |
| CTLA-4 | Cytotoxic T-lymphocyte associated protein 4 |
| DC | Dendritic cell |
| Gal-9 | Galectin-9 |
| HAVCR2 | Hepatitis A virus cellular receptor 2 |
| ICU | Intensive care unit |
| LD | Linkage disequilibrium |
| NK | Natural killer cell |
| NYHA | New York Heart Association |
| PCR | Polymerase chain reaction |
| PD-1 | Programmed cell death protein 1 |
| SNP | Single nucleotide polymorphism |
| SOFA | Sequential Organ Failure Assessment |
| TIM-3 | T cell immunoglobulin and mucin domain-containing protein 3 |
| TReg | Regulatory T cells |
| WHO | World Health Organization |
References
- WHO. Improving the Prevention, Diagnosis and Clinical Management of Sepsis. Available online: http://www.who.int/servicedeliverysafety/areas/sepsis/en/ (accessed on 19 September 2019).
- Reinhart, K.; Daniels, R.; Kissoon, N.; Machado, F.R.; Schachter, R.D.; Finfer, S. Recognizing Sepsis as a Global Health Priority—A WHO Resolution. N. Engl. J. Med. 2017, 377, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Thomas–Rueddel, D.O.; Hartmann, M.; Hartog, C.S.; Welte, T.; Heublein, S.; Dennler, U.; Reinhart, K. Hospital Incidence and Mortality Rates of Sepsis. Dtsch. Aerzteblatt Int. 2016, 113, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Chang, D.W.; Tseng, C.-H.; Shapiro, M.F. Rehospitalizations Following Sepsis: Common and Costly. Crit. Care Med. 2015, 43, 2085–2093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am. J. Respir. Crit. Care Med. 2015, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Paoli, C.J.; Reynolds, M.A.; Sinha, M.; Gitlin, M.; Crouser, E. Epidemiology and Costs of Sepsis in the United States—An Analysis Based on Timing of Diagnosis and Severity Level*. Crit. Care Med. 2018, 46, 1889–1897. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- De La Rica, A.S.; Gilsanz, F.; Maseda, E. Epidemiologic trends of sepsis in western countries. Ann. Transl. Med. 2016, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Immunosuppression in sepsis: A novel understanding of the disorder and a new therapeutic approach. Lancet Infect. Dis. 2013, 13, 260–268. [Google Scholar] [CrossRef] [Green Version]
- Mewes, C.; Büttner, B.; Hinz, J.; Alpert, A.; Popov, A.F.; Ghadimi, M.; Beissbarth, T.; Tzvetkov, M.; Shen-Orr, S.; Bergmann, I.; et al. The CTLA-4 rs231775 GG genotype is associated with favorable 90-day survival in Caucasian patients with sepsis. Sci. Rep. 2018, 8, 15140. [Google Scholar] [CrossRef] [Green Version]
- Mewes, C.; Büttner, B.; Hinz, J.; Alpert, A.; Popov, A.F.; Ghadimi, M.; Beissbarth, T.; Tzvetkov, M.; Jensen, O.; Runzheimer, J.; et al. CTLA-4 genetic variants predict survival in patients with sepsis. J. Clin. Med. 2019, 8, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansur, A.; Hinz, J.; Hillebrecht, B.; Bergmann, I.; Popov, A.F.; Ghadimi, M.; Bauer, M.; Beissbarth, T.; Mihm, S. Ninety-day survival rate of patients with sepsis relates to programmed cell death 1 genetic polymorphism rs11568821. J. Investig. Med. 2014, 62, 638–643. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Wen, D.; Wang, X.; Gan, L.; Du, J.; Sun, J.; Zeng, L.; Jiang, J.; Zhang, A. Host genetic variants in sepsis risk: A field synopsis and meta-analysis. Crit. Care 2019, 23. [Google Scholar] [CrossRef] [Green Version]
- Wolf, Y.; Anderson, A.C.; Kuchroo, V.K. TIM3 comes of age as an inhibitory receptor. Nat. Rev. Immunol. 2019, 20, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Joller, N.; Kuchroo, V.K. Tim-3, Lag-3, and TIGIT. Curr. Top. Microbiol. Immunol. 2017, 410, 127–156. [Google Scholar] [CrossRef] [Green Version]
- Monney, L.; Sabatos, C.A.; Gaglia, J.L.; Ryu, A.; Waldner, H.; Chernova, T.; Manning, S.; Greenfield, E.A.; Coyle, A.J.; Sobel, R.A.; et al. Th1-specific cell surface protein Tim-3 regulates macrophage activation and severity of an autoimmune disease. Nature 2002, 415, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Yu, G.; Han, Q.; Cui, C.; Zhang, B. TIM-3: An Emerging Target in the Liver Diseases. Scand. J. Immunol. 2019, 91, e12825. [Google Scholar] [CrossRef]
- Murphy, K.; Weaver, C. Janeway Immunologie; Springer: Berlin/Heidelberg, Germany, 2018; ISBN 978-3-662-56003-7. [Google Scholar]
- Li, Z.; Ju, Z.; Frieri, M. The T-cell immunoglobulin and mucin domain (Tim) gene family in asthma, allergy, and autoimmunity. Allergy Asthma Proc. 2013, 34, e21–e26. [Google Scholar] [CrossRef] [PubMed]
- Tang, F.; Wang, F.; An, L.; Wang, X. Upregulation of Tim-3 on CD4+ T cells is associated with Th1/Th2 imbalance in patients with allergic asthma. Int. J. Clin. Exp. Med. 2015, 8, 3809–3816. [Google Scholar]
- Razi, B.; Reykandeh, S.E.; Alizadeh, S.; Amirzargar, A.; Saghazadeh, A.; Rezaei, N. TIM family gene polymorphism and susceptibility to rheumatoid arthritis: Systematic review and meta-analysis. PLoS ONE 2019, 14, e0211146. [Google Scholar] [CrossRef]
- Song, Y.W.; Im, C.H.; Park, J.H.; Lee, Y.J.; Lee, E.Y.; Lee, E.B.; Park, K. T-cell immunoglobulin and mucin domain 3 genetic polymorphisms are associated with rheumatoid arthritis independent of a shared epitope status. Hum. Immunol. 2011, 72, 652–655. [Google Scholar] [CrossRef] [PubMed]
- Brück, P.; Ramos-Lopez, E.; Bartsch, W.; Böhme, A.; Badenhoop, K. TIM-3 polymorphisms in type 1 diabetes families. J. Hum. Genet. 2008, 53, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Jiang, X.; Chen, G.; Xiao, Y.; Geng, S.; Kang, C.; Zhou, T.; Li, Y.; Guo, X.; Xiao, H.; et al. T Cell Ig Mucin-3 Promotes Homeostasis of Sepsis by Negatively Regulating the TLR Response. J. Immunol. 2013, 190, 2068–2079. [Google Scholar] [CrossRef] [Green Version]
- Gleason, M.K.; Lenvik, T.R.; McCullar, V.; Felices, M.; O’Brien, M.S.; Cooley, S.A.; Verneris, M.R.; Cichocki, F.; Holman, C.J.; Panoskaltsis-Mortari, A.; et al. Tim-3 is an inducible human natural killer cell receptor that enhances interferon gamma production in response to galectin-9. Blood 2012, 119, 3064–3072. [Google Scholar] [CrossRef]
- Zhu, C.; Anderson, A.C.; Schubart, A.; Xiong, H.; Imitola, J.; Khoury, S.J.; Zheng, X.X.; Strom, T.B.; Kuchroo, V.K. The Tim-3 ligand galectin-9 negatively regulates T helper type 1 immunity. Nat. Immunol. 2005, 6, 1245–1252. [Google Scholar] [CrossRef]
- Wang, F.; Xu, J.; Liao, Y.; Wang, Y.; Liu, C.; Zhu, X.; Chen, Z.K.; Sun, Z. Tim-3 ligand galectin-9 reduces IL-17 level and accelerates Klebsiella pneumoniae infection. Cell. Immunol. 2011, 269, 22–28. [Google Scholar] [CrossRef]
- Zhao, Z.; Jiang, X.; Kang, C.; Xiao, Y.; Hou, C.; Yu, J.; Wang, R.; Xiao, H.; Zhou, T.; Wen, Z.; et al. Blockade of the T cell immunoglobulin and mucin domain protein 3 pathway exacerbates sepsis-induced immune deviation and immunosuppression. Clin. Exp. Immunol. 2014, 178, 279–291. [Google Scholar] [CrossRef]
- Xia, Q.; Wei, L.; Zhang, Y.; Sheng, J.; Wu, W.; Zhang, Y. Immune Checkpoint Receptors Tim-3 and PD-1 Regulate Monocyte and T Lymphocyte Function in Septic Patients. Mediat. Inflamm. 2018, 2018. [Google Scholar] [CrossRef]
- Marshall, J.C. Why have clinical trials in sepsis failed? Trends Mol. Med. 2014, 20, 195–203. [Google Scholar] [CrossRef]
- Yealy, D.M.; Huang, D.T.; Delaney, A.; Knight, M.; Randolph, A.G.; Daniels, R.; Nutbeam, T. Recognizing and managing sepsis: What needs to be done? BMC Med. 2015, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.; Wang, X.; Chen, X.; Wang, S.; Zhang, H. TIM-3 rs1036199 polymorphism increases susceptibility to autoimmune diseases: Evidence based on 4200 subjects. Biosci. Rep. 2018, 38. [Google Scholar] [CrossRef]
- Lee, J.; Phong, B.; Egloff, A.M.; Kane, L.P. TIM polymorphisms—Genetics and function. Genes Immun. 2011, 12, 595–604. [Google Scholar] [CrossRef]
- Rs1036199 RefSNP Report-dbSNP-NCBI. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/snp/rs1036199 (accessed on 11 February 2020).
- Rs10515746 RefSNP Report-dbSNP-NCBI. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/snp/rs10515746 (accessed on 11 February 2020).
- Hinz, J.; Büttner, B.; Kriesel, F.; Steinau, M.; Popov, A.F.; Ghadimi, M.; Beissbarth, T.; Tzvetkov, M.; Bergmann, I.; Mansur, A. The FER rs4957796 TT genotype is associated with unfavorable 90-day survival in Caucasian patients with severe ARDS due to pneumonia. Sci. Rep. 2017, 7, 9887. [Google Scholar] [CrossRef] [Green Version]
- Mewes, C.; Böhnke, C.; Alexander, T.; Büttner, B.; Hinz, J.; Popov, A.-F.; Ghadimi, M.; Beißbarth, T.; Raddatz, D.; Meissner, K.; et al. Favorable 90-Day Mortality in Obese Caucasian Patients with Septic Shock According to the Sepsis-3 Definition. J. Clin. Med. 2020, 9, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, M.; Fink, M.; Marshall, J.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.; Vincent, J.L.; Ramsay, G. 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Crit. Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef]
- Rangachari, M.; Zhu, C.; Sakuishi, K.; Xiao, S.; Karman, J.; Chen, A.; Angin, M.; Wakeham, A.; Greenfield, E.A.; Sobel, R.A.; et al. Bat3 promotes T cell responses and autoimmunity by repressing Tim-3–mediated cell death and exhaustion. Nat. Med. 2012, 18, 1394–1400. [Google Scholar] [CrossRef] [Green Version]
- Anderson, A.C.; Anderson, D.E.; Bregoli, L.; Hastings, W.D.; Kassam, N.; Lei, C.; Chandwaskar, R.; Karman, J.; Su, E.W.; Hirashima, M.; et al. Promotion of tissue inflammation by the immune receptor Tim-3 expressed on innate immune cells. Science 2007, 318, 1141–1143. [Google Scholar] [CrossRef]
- Anderson, A.C.; Joller, N.; Kuchroo, V.K. Lag-3, Tim-3, and TIGIT: Co-inhibitory Receptors with Specialized Functions in Immune Regulation. Immunity 2016, 44, 989–1004. [Google Scholar] [CrossRef] [Green Version]
- McIntire, J.J.; Umetsu, S.E.; Akbari, O.; Potter, M.; Kuchroo, V.K.; Barsh, G.S.; Freeman, G.J.; Umetsu, D.T.; DeKruyff, R.H. Identification of Tapr (an airway hyperreactivity regulatory locus) and the linked Tim gene family. Nat. Immunol. 2001, 2, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Frisancho-Kiss, S.; Nyland, J.F.; Davis, S.E.; Barrett, M.A.; Gatewood, S.J.L.; Njoku, D.B.; Cihakova, D.; Silbergeld, E.K.; Rose, N.R.; Fairweather, D. Cutting Edge: T Cell Ig Mucin-3 Reduces Inflammatory Heart Disease by Increasing CTLA-4 during Innate Immunity. J. Immunol. 2006, 176, 6411–6415. [Google Scholar] [CrossRef] [Green Version]
- Uchida, Y.; Ke, B.; Freitas, M.C.S.; Yagita, H.; Akiba, H.; Busuttil, R.W.; Najafian, N.; Kupiec-Weglinski, J.W. T-cell immunoglobulin mucin-3 determines severity of liver ischemia/reperfusion injury in mice in a TLR4-dependent manner. Gastroenterology 2010, 139, 2195–2206. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All (n = 712) | AC + CC (n = 241) | AA (n = 471) | p-Value |
|---|---|---|---|---|
| Basic Conditions | ||||
| Age [years] | 63 ± 15 | 63 ± 15 | 63 ± 15 | 0.9015 |
| Male sex [%] | 65 | 68 | 64 | 0.3231 |
| Body mass index (BMI) [kg/m2] | 28 ± 7 | 28 ± 8 | 28 ± 6 | 0.7304 |
| Severity on Sepsis Onset (Day 1) | ||||
| Sequential Organ Failure Assessment (SOFA) | 10 ± 4 | 10 ± 4 | 10 ± 4 | 0.9595 |
| Acute Physiology And Chronic Health Evaluation (APACHE II) | 22 ± 7 | 21 ± 7 | 22 ± 7 | 0.1826 |
| Procalcitonin [ng/dl] | 10 ± 29 | 13 ± 34 | 9 ± 25 | 0.5192 |
| Use of vasopressor [%] | 70 | 71 | 70 | 0.6323 |
| Mechanical ventilation [%] | 86 | 85 | 87 | 0.3360 |
| Renal replacement therapy [%] | 10 | 12 | 8 | 0.0935 |
| Comorbidities [%] | ||||
| Arterial hypertension [%] | 54 | 54 | 53 | 0.7872 |
| Chronic obstructive pulmonary disease (COPD) [%] | 15 | 13 | 16 | 0.2199 |
| Bronchial asthma [%] | 3 | 2 | 3 | 0.2911 |
| Renal dysfunction [%] | 10 | 12 | 9 | 0.2626 |
| Non-insulin-dependent diabetes mellitus (NIDDM) [%] | 9 | 8 | 9 | 0.7818 |
| Insulin-dependent diabetes mellitus (IDDM) [%] | 10 | 10 | 10 | 0.8687 |
| Chronic liver disease [%] | 6 | 6 | 6 | 0.9669 |
| History of myocardial infarction [%] | 5 | 5 | 6 | 0.9443 |
| History of stroke [%] | 6 | 5 | 6 | 0.3825 |
| History of cancer [%] | 14 | 16 | 13 | 0.2670 |
| Medication on Sepsis Onset [%] | ||||
| Statins [%] | 23 | 24 | 23 | 0.5984 |
| Beta-blocker [%] | 37 | 38 | 36 | 0.5859 |
| ACE inhibitor [%] | 29 | 31 | 28 | 0.4926 |
| Bronchodilator [%] | 10 | 6 | 13 | 0.0052 |
| Diuretics [%] | 33 | 34 | 33 | 0.7649 |
| Anticoagulation during the last 6 months [%] | 25 | 28 | 24 | 0.1974 |
| Recent Surgical History [%] | ||||
| Elective surgery [%] | 27 | 24 | 29 | |
| Emergency surgery [%] | 52 | 54 | 51 | 0.3330 |
| No surgery [%] | 21 | 22 | 20 | |
| Site of Infection [%] | ||||
| Lung [%] | 63 | 61 | 64 | |
| Abdomen [%] | 19 | 22 | 17 | |
| Bone or soft tissue [%] | 3 | 2 | 4 | |
| Surgical wound [%] | 2 | 2 | 1 | 0.4211 |
| Urogenital [%] | 2 | 2 | 3 | |
| Primary bacteremia [%] | 6 | 6 | 6 | |
| Other [%] | 5 | 5 | 5 |
| Characteristics | All (n = 712) | AA + AC (n = 247) | CC (n = 465) | p-Value |
|---|---|---|---|---|
| Basic Conditions | ||||
| Age [years] | 63 ± 15 | 63 ± 15 | 63 ± 15 | 0.9536 |
| Male sex [%] | 65 | 68 | 64 | 0.2451 |
| Body mass index (BMI) [kg/m2] | 28 ± 7 | 28 ± 8 | 28 ± 6 | 0.7976 |
| Severity on Sepsis Onset (Day 1) | ||||
| Sequential Organ Failure Assessment (SOFA) | 10 ± 4 | 10 ± 4 | 10 ± 4 | 0.9343 |
| Acute Physiology And Chronic Health Evaluation (APACHE II) | 22 ± 7 | 21 ± 7 | 22 ± 7 | 0.1738 |
| Procalcitonin [ng/dl] | 10 ± 29 | 12 ± 34 | 9 ± 25 | 0.7732 |
| Use of vasopressor [%] | 70 | 70 | 69 | 0.7857 |
| Mechanical ventilation [%] | 86 | 85 | 87 | 0.3181 |
| Renal replacement therapy [%] | 10 | 12 | 9 | 0.2123 |
| Comorbidities [%] | ||||
| Arterial hypertension [%] | 54 | 53 | 54 | 0.6908 |
| Chronic obstructive pulmonary disease (COPD) [%] | 15 | 13 | 16 | 0.3269 |
| Bronchial asthma [%] | 3 | 2 | 3 | 0.5325 |
| Renal dysfunction [%] | 10 | 12 | 9 | 0.3401 |
| Non-insulin-dependent diabetes mellitus (NIDDM) [%] | 9 | 8 | 9 | 0.6736 |
| Insulin-dependent diabetes mellitus (IDDM) [%] | 10 | 10 | 10 | 0.9953 |
| Chronic liver disease [%] | 6 | 6 | 6 | 0.7929 |
| History of myocardial infarction [%] | 5 | 5 | 6 | 0.8546 |
| History of stroke [%] | 6 | 5 | 6 | 0.5211 |
| History of cancer [%] | 14 | 17 | 12 | 0.1095 |
| Medication on Sepsis Onset [%] | ||||
| Statins [%] | 23 | 24 | 23 | 0.6532 |
| Beta-blocker [%] | 37 | 38 | 36 | 0.7305 |
| ACE inhibitor [%] | 29 | 32 | 28 | 0.2832 |
| Bronchodilator [%] | 10 | 6 | 12 | 0.0155 |
| Diuretics [%] | 33 | 34 | 33 | 0.8960 |
| Anticoagulation during the last 6 months [%] | 25 | 28 | 24 | 0.3142 |
| Recent Surgical History [%] | ||||
| Elective surgery [%] | 27 | 25 | 29 | |
| Emergency surgery [%] | 52 | 54 | 51 | 0.5589 |
| No surgery [%] | 21 | 21 | 21 | |
| Site of Infection [%] | ||||
| Lung [%] | 63 | 62 | 64 | |
| Abdomen [%] | 19 | 22 | 17 | |
| Bone or soft tissue [%] | 3 | 2 | 4 | |
| Surgical wound [%] | 2 | 2 | 2 | 0.2890 |
| Urogenital [%] | 2 | 2 | 3 | |
| Primary bacteremia [%] | 6 | 6 | 6 | |
| Other [%] | 5 | 5 | 5 |
| Characteristics | All (n = 712) | AC + CC (n = 241) | AA (n = 471) | p-Value |
|---|---|---|---|---|
| Sepsis Severity | ||||
| Sequential Organ Failure Assessment (SOFA) | 7.2 ± 3.7 | 7.3 ± 3.8 | 7.2 ± 3.6 | 0.9064 |
| Patients in septic shock [%] | 50 | 53 | 49 | 0.3291 |
| Days in septic shock | 2 ± 3 | 2 ± 2 | 2 ± 3 | 0.5047 |
| Inflammatory Values | ||||
| Leukocytes [1000/µL] | 13.2 ± 5.0 | 13.7 ± 5.2 | 13.0 ± 4.9 | 0.0619 |
| C-reactive Protein [mg/L] | 150.6 ± 85.9 | 148.0 ± 81.3 | 152.1 ± 88.5 | 0.7630 |
| Procalcitonin [ng/dL] | 4.4 ± 10.4 | 4.9 ± 10.4 | 4.1 ± 10.4 | 0.1922 |
| Fever [%] | 88 | 88 | 87 | 0.7188 |
| Respiratory Values | ||||
| SOFA respiratory subscore | 2.0 ± 0.8 | 1.9 ± 0.8 | 2.0 ± 0.8 | 0.2940 |
| Patients with mechanical ventilation [%] | 94 | 95 | 93 | 0.5335 |
| Ventilation days/observation days [%] | 68 ± 32 | 66 ± 32 | 69 ± 32 | 0.3608 |
| Coagulation | ||||
| SOFA coagulation subscore | 0.4 ± 0.6 | 0.4 ± 0.7 | 0.4 ± 0.6 | 0.7182 |
| Thrombocytes [1000/µL] | 292 ± 151 | 292 ± 150 | 292 ± 151 | 0.6663 |
| Liver Values | ||||
| SOFA hepatic subscore | 0.4 ± 0.7 | 0.4 ± 0.7 | 0.4 ± 0.7 | 0.2591 |
| Bilirubin [mg/dL] | 1.2 ± 2.1 | 1.2 ± 1.9 | 1.3 ± 2.2 | 0.7229 |
| AST (GOT) [IU/L] | 179 ± 599 | 190 ± 574 | 174 ± 612 | 0.8124 |
| ALT (GPT) [IU/L] | 97 ± 195 | 98 ± 208 | 97 ± 187 | 0.4376 |
| Cardiovascular Values | ||||
| SOFA cardiovascular subscore | 1.6 ± 1.0 | 1.6 ± 1.1 | 1.6 ± 1.0 | 0.9143 |
| Patients with vasopressor treatment [%] | 81 | 81 | 81 | 0.8456 |
| Vasopressor days/observation days [%] | 37 ± 32 | 37 ± 33 | 36 ± 31 | 0.8398 |
| Central Nervous System | ||||
| SOFA central nervous system | 2.1 ± 1.1 | 2.0 ± 1.1 | 2.1 ± 1.1 | 0.1701 |
| Glasgow Coma Scale (GCS) | 9.8 ± 3.2 | 10.0 ± 3.3 | 9.7 ± 3.2 | 0.2311 |
| Renal Values | ||||
| SOFA renal subscore | 0.8 ± 1.2 | 0.9 ± 1.2 | 0.8 ± 1.2 | 0.2780 |
| Creatinine [mg/dL] | 1.2 ± 0.9 | 1.3 ± 0.9 | 1.2 ± 0.9 | 0.2977 |
| Urine output [mL/d] | 2906 ± 1345 | 2915 ± 1420 | 2901 ± 1307 | 0.7551 |
| Urine output [mL/kg/d] | 1.5 ± 0.8 | 1.5 ± 0.8 | 1.5 ± 0.8 | 0.9251 |
| Patients with renal replacement therapy [%] | 22 | 23 | 22 | 0.7266 |
| Dialysis days/observation days [%] | 11 ± 25 | 12 ± 26 | 10 ± 24 | 0.7023 |
| Characteristics | All (n = 712) | AA + AC (n = 247) | CC (n = 465) | p-Value |
|---|---|---|---|---|
| Sepsis Severity | ||||
| Sequential Organ Failure Assessment (SOFA) | 7.2 ± 3.7 | 7.2 ± 3.7 | 7.3 ± 3.7 | 0.7846 |
| Patients in Septic Shock [%] | 50 | 53 | 49 | 0.3326 |
| Days in Septic Shock | 2 ± 3 | 2 ± 2 | 2 ± 3 | 0.5087 |
| Inflammatory Values | ||||
| Leukocytes [1000/µL] | 13.2 ± 5.0 | 13.7 ± 5.2 | 13.0 ± 4.9 | 0.0550 |
| C-reactive Protein [mg/L] | 150.6 ± 85.9 | 149.5 ± 82.1 | 151.2 ± 88.2 | 0.9759 |
| Procalcitonin [ng/dL] | 4.4 ± 10.4 | 4.8 ± 10.3 | 4.2 ± 10.5 | 0.2529 |
| Fever [%] | 88 | 88 | 88 | 0.7687 |
| Respiratory Values | ||||
| SOFA respiratory subscore | 2.0 ± 0.8 | 1.9 ± 0.8 | 2.0 ± 0.8 | 0.3020 |
| Patients with mechanical ventilation [%] | 94 | 94 | 94 | 0.6794 |
| Ventilation days/observation days [%] | 68 ± 32 | 66 ± 32 | 69 ± 31 | 0.3060 |
| Coagulation | ||||
| SOFA coagulation subscore | 0.4 ± 0.6 | 0.4 ± 0.7 | 0.4 ± 0.6 | 0.5976 |
| Thrombocytes [1000/µL] | 292 ± 151 | 296 ± 155 | 290 ± 149 | 0.4882 |
| Liver Values | ||||
| SOFA hepatic subscore | 0.4 ± 0.7 | 0.4 ± 0.7 | 0.4 ± 0.7 | 0.2398 |
| Bilirubin [mg/dL] | 1.2 ± 2.1 | 1.2 ± 1.9 | 1.3 ± 2.2 | 0.5271 |
| AST (GOT) [IU/L] | 179 ± 599 | 190 ± 566 | 174 ± 616 | 0.8599 |
| ALT (GPT) [IU/L] | 97 ± 195 | 98 ± 207 | 97 ± 188 | 0.4824 |
| Cardiovascular Values | ||||
| SOFA cardiovascular subscore | 1.6 ± 1.0 | 1.6 ± 1.1 | 1.6 ± 1.0 | 0.6821 |
| Patients with vasopressor treatment [%] | 81 | 80 | 81 | 0.7154 |
| Vasopressor days/observation days [%] | 37 ± 32 | 36 ± 33 | 37 ± 31 | 0.6091 |
| Central Nervous System | ||||
| SOFA central nervous system | 2.1 ± 1.1 | 2.0 ± 1.1 | 2.1 ± 1.1 | 0.1644 |
| Glasgow Coma Scale (GCS) | 9.8 ± 3.2 | 10.0 ± 3.3 | 9.7 ± 3.2 | 0.1946 |
| Renal Values | ||||
| SOFA renal subscore | 0.8 ± 1.2 | 0.9 ± 1.2 | 0.8 ± 1.2 | 0.4042 |
| Creatinine [mg/dL] | 1.2 ± 0.9 | 1.3 ± 0.9 | 1.2 ± 1.0 | 0.3852 |
| Urine output [mL/d] | 2906 ± 1345 | 2923 ± 1404 | 2896 ± 1314 | 0.6595 |
| Urine output [mL/kg/d] | 1.5 ± 0.8 | 1.5 ± 0.8 | 1.5 ± 0.8 | 1.0000 |
| Patients with renal replacement therapy [%] | 22 | 23 | 22 | 0.9257 |
| Dialysis days/observation days [%] | 11 ± 25 | 11 ± 25 | 10 ± 24 | 0.8644 |
| Variable | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age | 1.0299 | 1.0163–1.0436 | <0.0001 |
| Male sex | 1.1144 | 0.7886–1.5746 | 0.5393 |
| BMI | 0.9576 | 0.9277–0.9884 | 0.0073 |
| SOFA score at sepsis onset | 1.0887 | 1.0333–1.1471 | 0.0014 |
| APACHE II score at sepsis onset | 1.0376 | 1.0043–1.0719 | 0.0264 |
| Use of bronchodilators at sepsis onset | 0.9733 | 0.5734–1.6522 | 0.9202 |
| TIM-3 rs1036199 AA genotype | 0.6714 | 0.4825–0.9341 | 0.0180 |
| Variable | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age | 1.0300 | 1.0165–1.0438 | <0.0001 |
| Male sex | 1.1132 | 0.7875–1.5736 | 0.5436 |
| BMI | 0.9573 | 0.9273–0.9882 | 0.0071 |
| SOFA score at sepsis onset | 1.0907 | 1.0354–1.1489 | 0.0011 |
| APACHE II score at sepsis onset | 1.0366 | 1.0035–1.0707 | 0.0297 |
| Use of bronchodilators at sepsis onset | 0.9670 | 0.5699–1.6408 | 0.9009 |
| TIM-3 rs10515746 CC genotype | 0.6981 | 0.5021–0.9706 | 0.0326 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mewes, C.; Alexander, T.; Büttner, B.; Hinz, J.; Alpert, A.; Popov, A.-F.; Ghadimi, M.; Beißbarth, T.; Tzvetkov, M.; Grade, M.; et al. TIM-3 Genetic Variants Are Associated with Altered Clinical Outcome and Susceptibility to Gram-Positive Infections in Patients with Sepsis. Int. J. Mol. Sci. 2020, 21, 8318. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21218318
Mewes C, Alexander T, Büttner B, Hinz J, Alpert A, Popov A-F, Ghadimi M, Beißbarth T, Tzvetkov M, Grade M, et al. TIM-3 Genetic Variants Are Associated with Altered Clinical Outcome and Susceptibility to Gram-Positive Infections in Patients with Sepsis. International Journal of Molecular Sciences. 2020; 21(21):8318. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21218318
Chicago/Turabian StyleMewes, Caspar, Tessa Alexander, Benedikt Büttner, José Hinz, Ayelet Alpert, Aron-F. Popov, Michael Ghadimi, Tim Beißbarth, Mladen Tzvetkov, Marian Grade, and et al. 2020. "TIM-3 Genetic Variants Are Associated with Altered Clinical Outcome and Susceptibility to Gram-Positive Infections in Patients with Sepsis" International Journal of Molecular Sciences 21, no. 21: 8318. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21218318