Platelet Features and Derivatives in Osteoporosis: A Rational and Systematic Review on the Best Evidence


Abstract
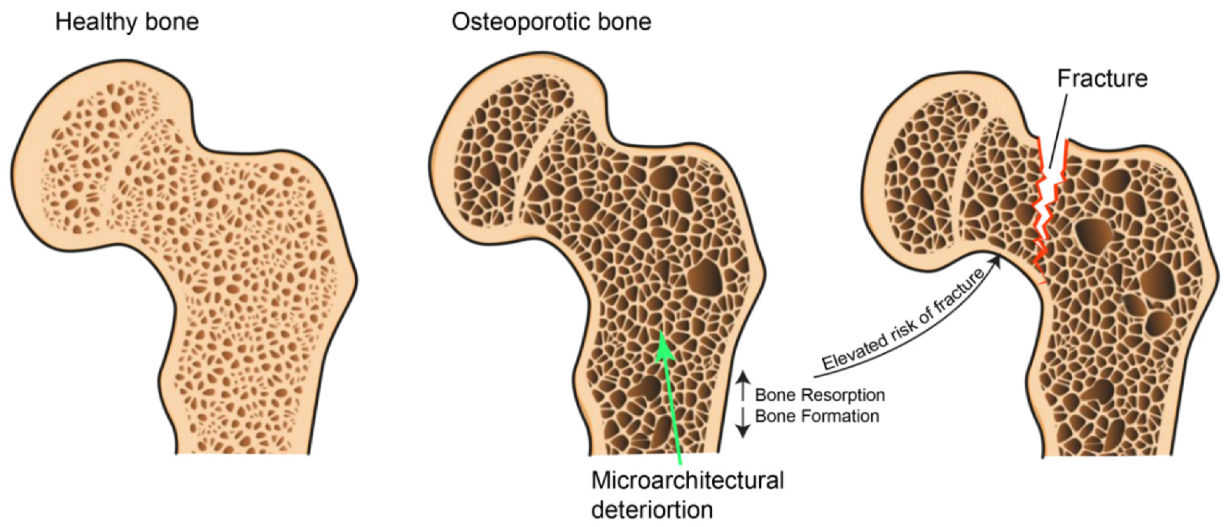
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information Source and Search Strategies
2.3. Study Selection and Data Extraction
2.4. Assessment of Methodological Quality
3. Results
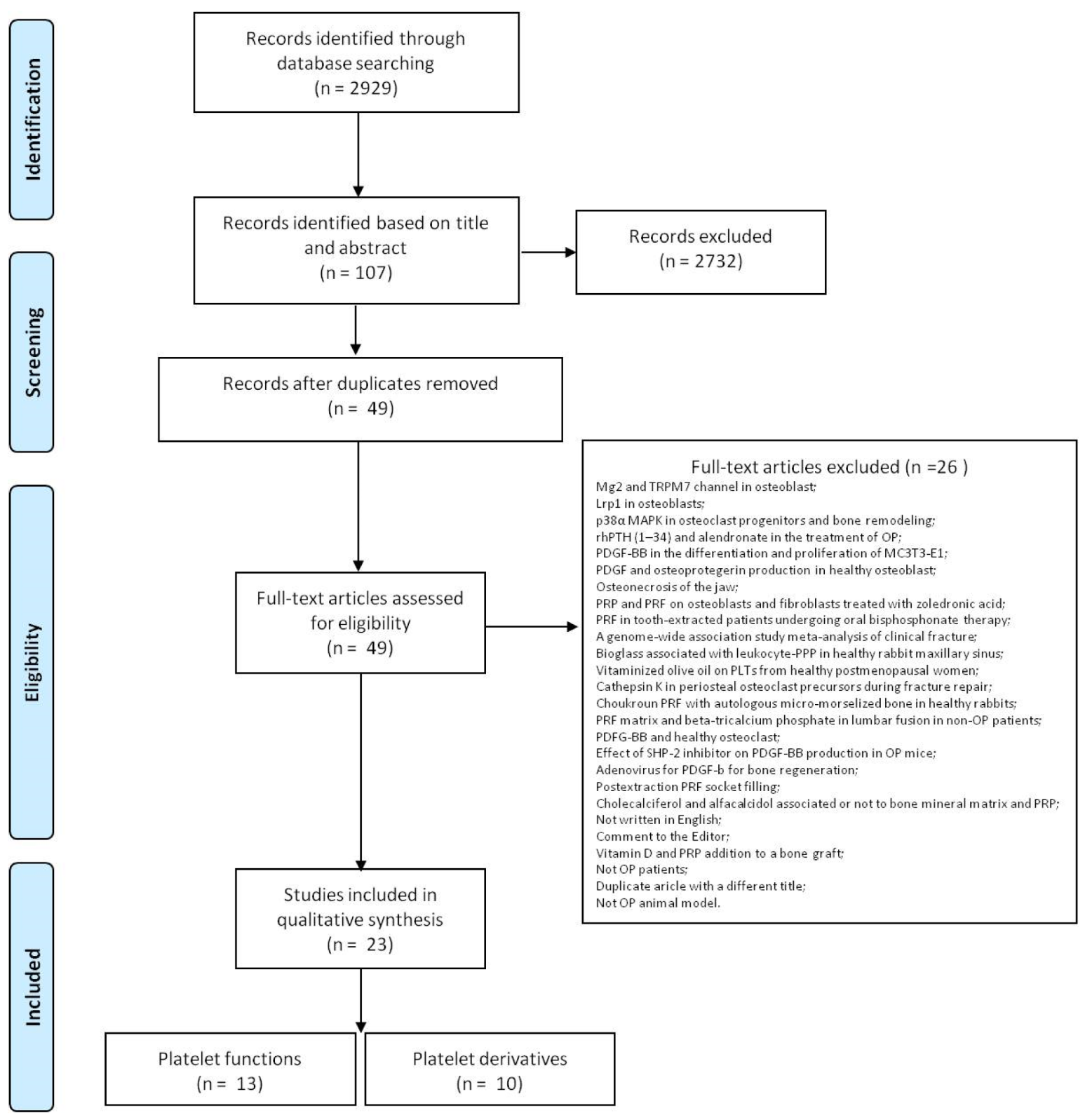
3.1. Study Selection and Characteristics
3.2. Assessment of Methodological Quality
4. Study Results
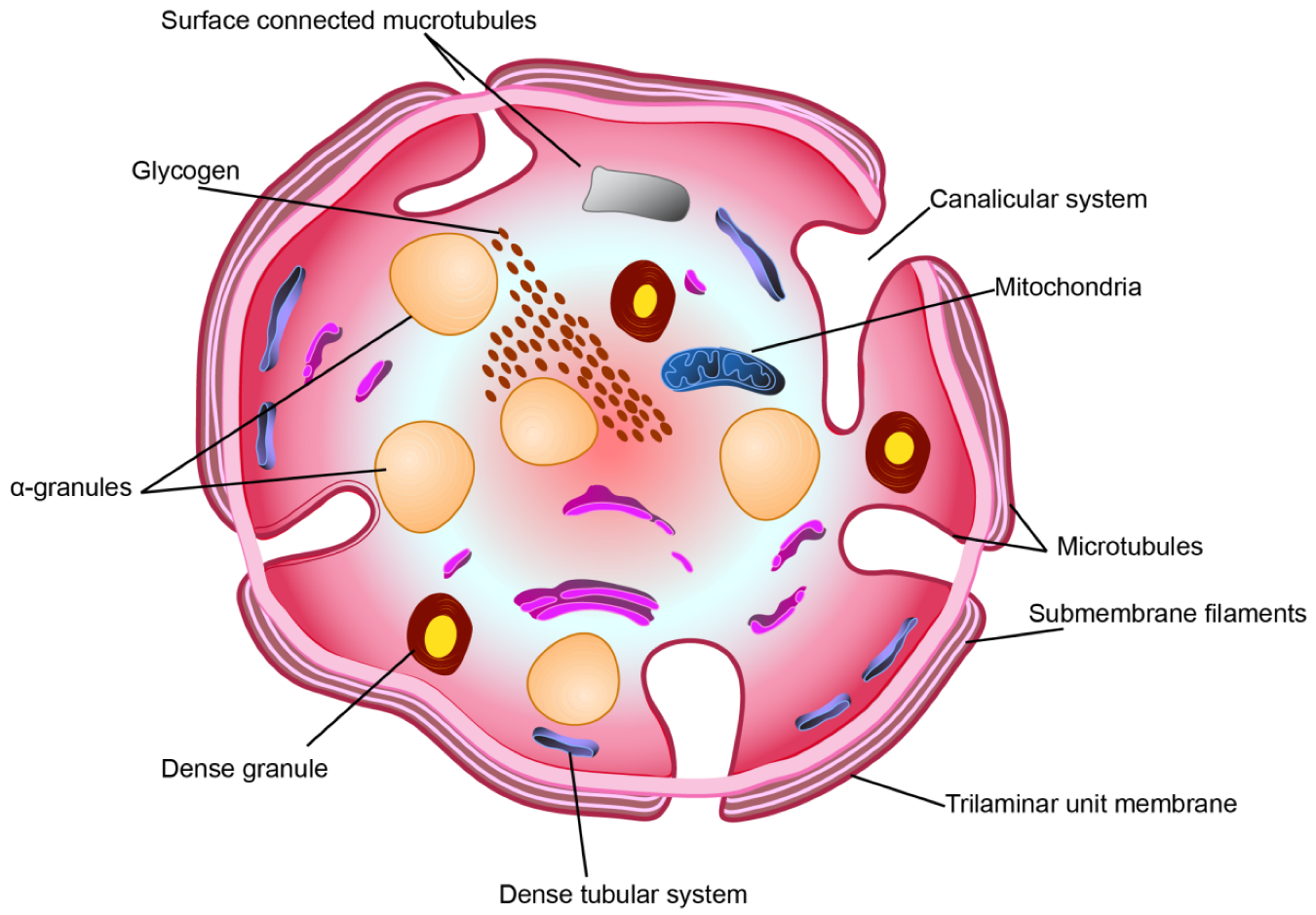
4.1. Platelet Functions/Features and Growth Factor in PLTs in Osteoporosis
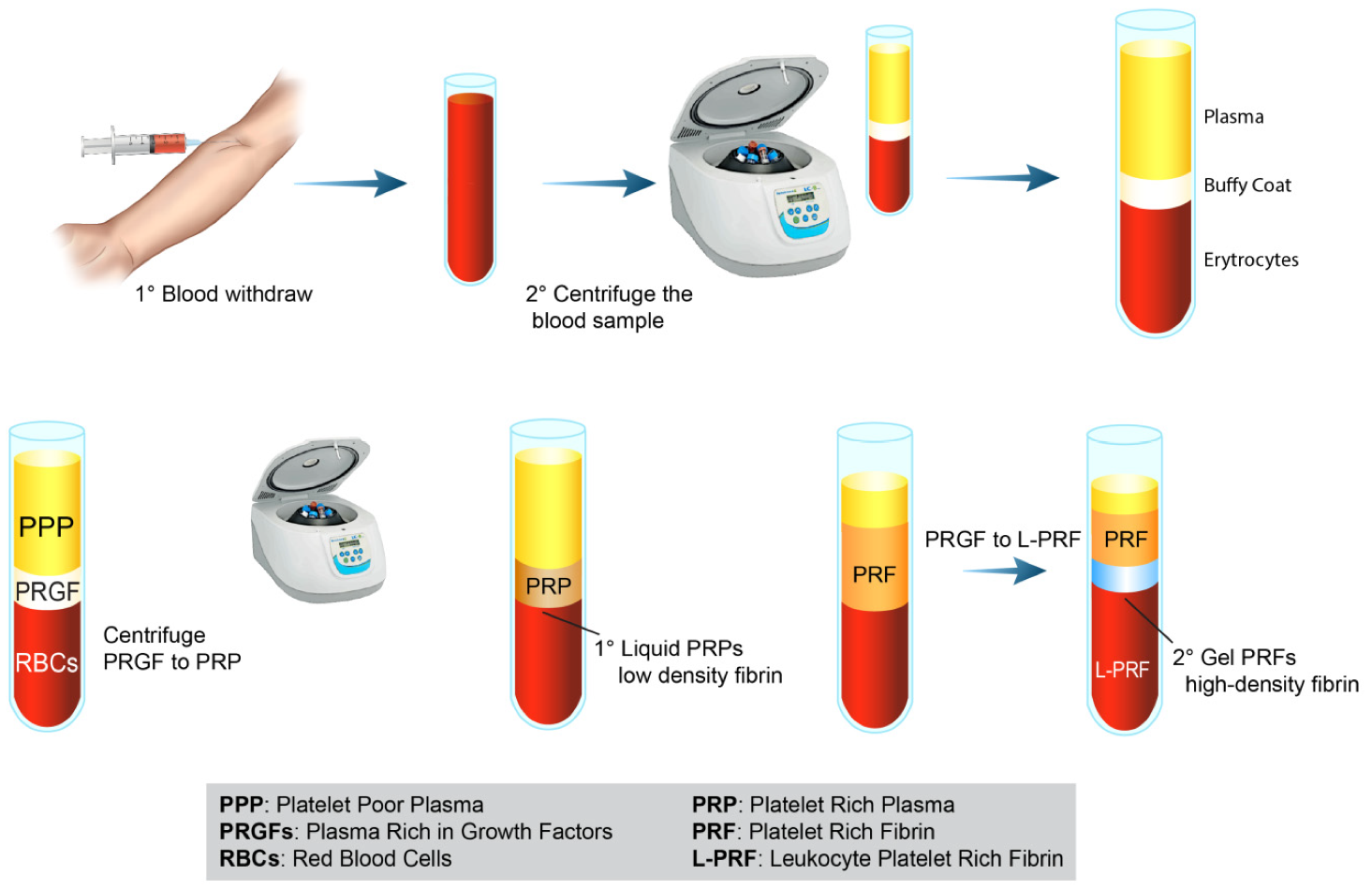
4.2. Platelet Derivatives in Osteoporosis
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Curtis, E.M.; Harvey, N.C.; Cooper, C. The burden of osteoporosis. In Osteoporosis: A Life Course Epidemiology Approach to Skeletal Health; Harvey, N.C., Cooper, C., Eds.; CRC Press: Boca Raton, FL, USA, 2018; pp. 1–20. [Google Scholar]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; Cooper, C.; Rizzoli, R.; Reginster, J.Y.; Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF). Executive summary of European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Aging Clin. Exp. Res. 2019, 31, 15–17. [Google Scholar] [CrossRef] [PubMed]
- Al Anouti, F.; Taha, Z.; Shamim, S.; Khalaf, K.; Al Kaabi, L.; Alsafar, H. An insight into the paradigms of osteoporosis: From genetics to biomechanics. Bone Rep. 2019, 11, 100216. [Google Scholar] [CrossRef] [PubMed]
- Black, D.M.; Rosen, C.J. Postmenopausal Osteoporosis. N. Engl. J. Med. 2016, 374, 2096–2097. [Google Scholar] [CrossRef] [PubMed]
- Bord, S.; Frith, E.; Ireland, D.C.; Scott, M.A.; Craig, J.I.; Compston, J.E. Megakaryocytes modulate osteoblast synthesis of type-l collagen, osteoprotegerin, and RANKL. Bone 2005, 36, 812–819. [Google Scholar] [CrossRef]
- Ciovacco, W.A.; Goldberg, C.G.; Taylor, A.F.; Lemieux, J.M.; Horowitz, M.C.; Donahue, H.J.; Kacena, M.A. The role of gap junctions in megakaryocyte-mediated osteoblast proliferation and differentiation. Bone 2009, 44, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Kacena, M.A.; Nelson, T.; Clough, M.E.; Lee, S.K.; Lorenzo, J.A.; Gundberg, C.M.; Horowitz, M.C. Megakaryocyte-mediated inhibition of osteoclast development. Bone 2006, 39, 991–999. [Google Scholar] [CrossRef]
- Maynard, D.M.; Heijnen, H.F.; Horne, M.K.; White, J.G.; Gahl, W.A. Proteomic analysis of platelet alpha-granules using mass spectrometry. J. Thromb. Haemost. 2007, 5, 1945–1955. [Google Scholar] [CrossRef]
- Singh, A.; Ali, S.; Srivastava, R.N. Platelet-rich plasma in osteoporotic fractures: A review of literature. J. Orthop. Traumatol. Rehabil. 2014, 7, 123–138. [Google Scholar] [CrossRef]
- Lieberman, J.R.; Daluiski, A.; Einhorn, T.A. The role of growth factors in the repair of bone. Biology and clinical applications. J. Bone Jt. Surg. Am. 2002, 84, 1032–1044. [Google Scholar] [CrossRef]
- Tabata, Y. Tissue regeneration based on growth factor release. Tissue Eng. 2003, 9 (Suppl. 1), 5–15. [Google Scholar] [CrossRef]
- Sharif, P.S.; Abdollahi, M. The role of platelets in bone remodeling. Inflamm. Allergy Drug Targets 2010, 9, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.A.; Parayaruthottam, P.; Roshan, G.; Menon, V.; Fidha, M.; Fernandes, A.K. Platelets and Their Pathways in Dentistry: Systematic Review. J. Int. Soc. Prev. Community Dent. 2017, 7 (Suppl. 2), 55–60. [Google Scholar] [CrossRef] [PubMed]
- Lang, S.; Loibl, M.; Herrmann, M. Platelet-Rich Plasma in Tissue Engineering: Hype and Hope. Eur. Surg. Res. 2018, 59, 265–275. [Google Scholar] [CrossRef]
- Oryan, A.; Alidadi, S.; Moshiri, A. Platelet-rich plasma for bone healing and regeneration. Expert Opin. Biol. Ther. 2016, 16, 213–232. [Google Scholar] [CrossRef] [PubMed]
- Salamanna, F.; Veronesi, F.; Maglio, M.; Della Bella, E.; Sartori, M.; Fini, M. New and emerging strategies in platelet-rich plasma application in musculoskeletal regenerative procedures: General overview on still open questions and outlook. Biomed Res. Int. 2015, 2015, 846045. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef]
- Camargo, P.M.; Lekovic, V.; Weinlaender, M.; Vasilic, N.; Madzarevic, M.; Kenney, E.B. Platelet-rich plasma and bovine porous bone mineral combined with guided tissue regeneration in the treatment of intrabony defects in humans. J. Periodontal. Res. 2002, 37, 300–306. [Google Scholar] [CrossRef]
- Uggeri, J.; Belletti, S.; Guizzardi, S.; Poli, T.; Cantarelli, S.; Scandroglio, R.; Gatti, R. Dose-dependent effects of platelet gel releasate on activities of human osteoblasts. J. Periodontol. 2007, 78, 1985–1991. [Google Scholar] [CrossRef]
- Man, Y.; Wang, P.; Guo, Y.; Xiang, L.; Yang, Y.; Qu, Y.; Gong, P.; Deng, L. Angiogenic and osteogenic potential of platelet-rich plasma and adipose-derived stem cell laden alginate microspheres. Biomaterials 2012, 33, 8802–8811. [Google Scholar] [CrossRef]
- Parsons, P.; Butcher, A.; Hesselden, K.; Ellis, K.; Maughan, J.; Milner, R.; Scott, M.; Alley, C.; Watson, J.T.; Horner, A. Platelet-rich concentrate supports human mesenchymal stem cell proliferation, bone morphogenetic protein-2 messenger RNA expression, alkaline phosphatase activity, and bone formation in vitro: A mode of action to enhance bone repair. J. Orthop. Trauma 2008, 22, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Mariano, R.; Messora, M.; de Morais, A.; Nagata, M.; Furlaneto, F.; Avelino, C.; Paula, F.; Ferreira, S.; Pinheiro, M.; de Sene, J.P. Bone healing in critical-size defects treated with platelet-rich plasma: A histologic and histometric study in the calvaria of diabetic rat. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2010, 109, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Simman, R.; Hoffmann, A.; Bohinc, R.J.; Peterson, W.C.; Russ, A.J. Role of platelet-rich plasma in acceleration of bone fracture healing. Ann. Plast. Surg. 2008, 61, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Tamimi, F.M.; Tresguerres, I.F.; Alkhraisat, M.H.; Khraisat, A.; Lopez-Cabarco, E.; Blanco, L. Effect of solely applied platelet-rich plasma on osseous regeneration compared to Bio-Oss: A morphometric and densitometric study on rabbit calvaria. Clin. Implant. Dent. Relat. Res. 2008, 10, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Giovanini, A.F.; Gonzaga, C.C.; Zielak, J.C.; Deliberador, T.M.; Kuczera, J.; Göringher, I.; de Oliveira Filho, M.A.; Baratto-Filho, F.; Urban, C.A. Platelet-rich plasma (PRP) impairs the craniofacial bone repair associated with its elevated TGF-β levels and modulates the co-expression between collagen III and α-smooth muscle actin. J. Orthop. Res. 2011, 29, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Lei, D.; Mao, T.; Yang, S.; Chen, F.; Wu, W. Repair of critical bone defects with injectable platelet rich plasma/bone marrow-derived stromal cells composite: Experimental study in rabbits. Ulus. Travma. Acil. Cerrahi. Derg. 2008, 14, 87–95. [Google Scholar]
- Célio-Mariano, R.; de Melo, W.M.; Carneiro-Avelino, C. Comparative radiographic evaluation of alveolar bone healing associated with autologous platelet-rich plasma after impacted mandibular third molar surgery. J. Oral. Maxillofac. Surg. 2012, 70, 19–24. [Google Scholar] [CrossRef]
- Poeschl, P.W.; Ziya-Ghazvini, F.; Schicho, K.; Buchta, C.; Moser, D.; Seemann, R.; Ewers, R.; Schopper, C. Application of platelet-rich plasma for enhanced bone regeneration in grafted sinus. J. Oral. Maxillofac. Surg. 2012, 70, 657–664. [Google Scholar] [CrossRef]
- Pappalardo, S.; Guarnieri, R. Efficacy of Platelet-Rich-Plasma (PRP) and Highly Purified Bovine Xenograft (Laddec®) Combination in Bone Regeneration after Cyst Enucleation: Radiological and Histological Evaluation. J. Oral. Maxillofac. Res. 2013, 4, 3. [Google Scholar] [CrossRef] [Green Version]
- Gupta, G. Clinical and radiographic evaluation of intra-bony defects in localized aggressive periodontitis patients with platelet rich plasma/hydroxyapatite graft: A comparative controlled clinical trial. Contemp. Clin. Dent. 2014, 5, 445–451. [Google Scholar] [CrossRef]
- Akbal, A.; Gökmen, F.; Gencer, M.; Inceer, B.S.; Kömürcü, E. Mean platelet volume and platelet distribution width can be related to bone mineralization. Osteoporos. Int. 2014, 25, 2291–2295. [Google Scholar] [CrossRef]
- Eroglu, S.; Karatas, G. Platelet/lymphocyte ratio is an independent predictor for osteoporosis. Saudi Med. J. 2019, 40, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, B.J.; Ahn, S.H.; Lee, S.H.; Koh, J.M. Higher plasma platelet-activating factor levels are associated with increased risk of vertebral fracture and lower bone mineral density in postmenopausal women. J. Bone Miner. Metab. 2015, 33, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayden, J.A.; Côté, P.; Bombardier, C. Evaluation of the quality of prognosis studies in systematic reviews. Ann. Intern. Med. 2006, 144, 427–437. [Google Scholar] [CrossRef]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef] [Green Version]
- Pountos, I.; Georgouli, T.; Henshaw, K.; Bird, H.; Jones, E.; Giannoudis, P.V. The effect of bone morphogenetic protein-2, bone morphogenetic protein-7, parathyroid hormone, and platelet-derived growth factor on the proliferation and osteogenic differentiation of mesenchymal stem cells derived from osteoporotic bone. J. Orthop. Trauma 2010, 24, 552–556. [Google Scholar] [CrossRef]
- Xie, H.; Cui, Z.; Wang, L.; Xia, Z.; Hu, Y.; Xian, L.; Li, C.; Xie, L.; Crane, J.; Wan, M.; et al. PDGF-BB secreted by preosteoclasts induces angiogenesis during coupling with osteogenesis. Nat. Med. 2014, 20, 1270–1278. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Jin, Y.; Qian, S.; Li, J.; Chang, Q.; Ye, D.; Pan, H.; Zhang, M.; Cao, H.; Liu, X.; et al. Vacuum extraction enhances rhPDGF-BB immobilization on nanotubes to improve implant osseointegration in ovariectomized rats. Nanomedicine 2014, 10, 1809–1818. [Google Scholar] [CrossRef]
- Tang, L.; Xia, Z.; Luo, Z.; Long, H.; Zhu, Y.; Zhao, S. Low plasma PDGF-BB levels are associated with estradiol in postmenopausal osteoporosis: PDGF-BB mediated by estradiol in women. J. Int. Med. Res. 2017, 45, 1332–1339. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.L.; Cho, H.Y.; Park, I.Y.; Choi, J.M.; Kim, M.; Jang, H.J.; Hwang, S.M. The positive association between peripheral blood cell counts and bone mineral density in postmenopausal women. Yonsei Med. J. 2011, 52, 739–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.S.; Zhang, J.R.; Meng, S.Y.; Li, Y.; Wang, R.T. Mean platelet volume is negatively associated with bone mineral density in postmenopausal women. J. Bone Miner. Metab. 2012, 30, 660–665. [Google Scholar] [CrossRef] [PubMed]
- D’Amelio, P.; Cristofaro, M.A.; De Vivo, E.; Ravazzoli, M.; Grosso, E.; Di Bella, S.; Aime, M.; Cotto, N.; Silvagno, F.; Isaia, G.C.; et al. Platelet vitamin D receptor is reduced in osteoporotic patients. Panminerva Med. 2012, 54, 225–231. [Google Scholar] [PubMed]
- Aypak, C.; Türedi, Ö.; Bircan, M.A.; Civelek, G.M.; Araz, M. Association between mean platelet volume and bone mineral density in postmenopausal women. J. Phys. Ther. Sci. 2016, 28, 1753–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vural, M.; Mert, M.; Erhan, B.; Gunduz, B.; Keles, B.Y.; Erdem, A.E.; Bozan, A.; Arslan, H. Is there any relationship between mean platelet volume, bone mineral density and vitamin d in postmenopausal women? Acta Med. Mediterr. 2017, 33, 443. [Google Scholar]
- Koseoglu, S.B. Bone loss & platelet-to-lymphocyte ratio. Biomark. Med. 2017, 11, 5–10. [Google Scholar]
- Lo, W.C.; Chiou, J.F.; Gelovani, J.G.; Cheong, M.L.; Lee, C.M.; Liu, H.Y.; Wu, C.H.; Wang, M.F.; Lin, C.T.; Deng, W.P. Transplantation of embryonic fibroblasts treated with platelet-rich plasma induces osteogenesis in SAMP8 mice monitored by molecular imaging. J. Nucl. Med. 2009, 50, 765–773. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.Y.; Wu, A.T.; Tsai, C.Y.; Chou, K.R.; Zeng, R.; Wang, M.F.; Chang, W.C.; Hwang, S.M.; Su, C.H.; Deng, W.P. The balance between adipogenesis and osteogenesis in bone regeneration by platelet-rich plasma for age-related osteoporosis. Biomaterials 2011, 32, 6773–6780. [Google Scholar] [CrossRef]
- Clafshenkel, W.P.; Rutkowski, J.L.; Palchesko, R.N.; Romeo, J.D.; McGowan, K.A.; Gawalt, E.S.; Witt-Enderby, P.A. A novel calcium aluminate-melatonin scaffold enhances bone regeneration within a calvarial defect. J. Pineal Res. 2012, 53, 206–218. [Google Scholar] [CrossRef]
- Chen, L.; Yang, X.; Huang, G.; Song, D.; Ye, X.S.; Xu, H.; Li, W. Platelet-rich plasma promotes healing of osteoporotic fractures. Orthopedics 2013, 36, 687–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, A.R.; Kim, H.K.; Kwon, J.Y.; Kim, T.K.; Choi, Y.M.; Kim, K.H. The incorporation of platelet-rich plasma into calcium phosphate cement enhances bone regeneration in osteoporosis. Pain Physician 2014, 17, 737–745. [Google Scholar]
- Jiang, N.; Du, P.; Qu, W.; Li, L.; Liu, Z.; Zhu, S. The synergistic effect of TiO2 nanoporous modification and platelet-rich plasma treatment on titanium-implant stability in ovariectomized rats. Int. J. Nanomed. 2016, 11, 4719–4733. [Google Scholar]
- Wei, B.; Huang, C.; Zhao, M.; Li, P.; Gao, X.; Kong, J.; Niu, Y.; Huang, R.; Quan, J.; Wei, J.; et al. Effect of Mesenchymal Stem Cells and Platelet-Rich Plasma on the Bone Healing of Ovariectomized Rats. Stem Cells Int. 2016, 2016, 9458396. [Google Scholar] [CrossRef] [PubMed]
- Rocha, M.A.C.; Silva, L.M.C.; Oliveira, W.A.; Bezerra, D.O.; Silva, G.C.D.; Silva, L.D.S.; Medeiros, B.L.D.N.; Baêta, S.A.F.; Carvalho, M.A.M.; Argôlo, N.M. Allogeneic mesenchymal stem cells and xenogenic platelet rich plasma, associated or not, in the repair of bone failures in rabbits with secondary osteoporosis. Acta Cir. Bras. 2017, 32, 767–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakata, M.; Tonomura, H.; Itsuji, T.; Ishibashi, H.; Takatori, R.; Mikami, Y.; Nagae, M.; Matsuda, K.I.; Tabata, Y.; Tanaka, M.; et al. Bone Regeneration of Osteoporotic Vertebral Body Defects Using Platelet-Rich Plasma and Gelatin β-Tricalcium Phosphate Sponges. Tissue Eng. Part A 2018, 24, 1001–1010. [Google Scholar] [CrossRef]
- Engler-Pinto, A.; Siéssere, S.; Calefi, A.; Oliveira, L.; Ervolino, E.; de Souza, S.; Furlaneto, F.; Messora, M.R. Effects of leukocyte- and platelet-rich fibrin associated or not with bovine bone graft on the healing of bone defects in rats with osteoporosis induced by ovariectomy. Clin. Oral. Implant. Res. 2019, 30, 962–976. [Google Scholar] [CrossRef]
- Goltzman, D. The Aging Skeleton. Adv. Exp. Med. Biol. 2019, 1164, 153–160. [Google Scholar]
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef]
- Dede, A.D.; Callan, M. Treatment of osteoporosis: Whom, how and for how long? Br. J. Hosp Med. (Lond.) 2018, 79, 259–264. [Google Scholar] [CrossRef]
- Caplan, A.I.; Correa, D. PDGF in bone formation and regeneration: New insights into a novel mechanism involving MSCs. J. Orthop. Res. 2011, 29, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Graham, S.; Leonidou, A.; Lester, M.; Heliotis, M.; Mantalaris, A.; Tsiridis, E. Investigating the role of PDGF as a potential drug therapy in bone formation and fracture healing. Expert Opin. Investig. Drugs 2009, 18, 1633–1654. [Google Scholar] [CrossRef] [PubMed]
- Varol, E. The relationship between platelet indices and postmenopausal osteoporosis. Osteoporos. Int. 2015, 26, 1871–1872. [Google Scholar] [CrossRef] [PubMed]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.S.; Brem, H.; Tomic-Canic, M. Growth factors and cytokines in wound healing. Wound Repair Regen. 2008, 16, 585–601. [Google Scholar] [CrossRef]
- Suzuki, S.; Morimoto, N.; Ikada, Y. Gelatin gel as a carrier of platelet-derived growth factors. J. Biomater. Appl. 2013, 28, 595–606. [Google Scholar] [CrossRef]
- Veronesi, F.; Pagani, S.; Torricelli, P.; Filardo, G.; Cavallo, C.; Grigolo, B.; Fini, M. PRP and MSCs on tenocytes artificial wound healing: An in vitro study comparing fresh and frozen PRP. Histol. Histopathol. 2018, 33, 1323–1334. [Google Scholar]
- Scully, D.; Naseem, K.M.; Matsakas, A. Platelet biology in regenerative medicine of skeletal muscle. Acta Physiol. (Oxf.) 2018, 223, 13071. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Items |
|---|---|
| PubMed | ((((((“blood platelets”[MeSH Terms] OR (“blood”[All Fields] AND “platelets”[All Fields]) OR “blood platelets”[All Fields] OR “platelet”[All Fields]) OR (“blood platelets”[MeSH Terms] OR (“blood”[All Fields] AND “platelets”[All Fields]) OR “blood platelets”[All Fields] OR “platelets”[All Fields])) OR ((“blood platelets”[MeSH Terms] OR (“blood”[All Fields] AND “platelets”[All Fields]) OR “blood platelets”[All Fields] OR “platelet”[All Fields]) AND functions[All Fields])) OR ((“blood platelets”[MeSH Terms] OR (“blood”[All Fields] AND “platelets”[All Fields]) OR “blood platelets”[All Fields] OR “platelet”[All Fields]) AND (“Changes”[Journal] OR “changes”[All Fields]))) OR ((“blood platelets”[MeSH Terms] OR (“blood”[All Fields] AND “platelets”[All Fields]) OR “blood platelets”[All Fields] OR “platelet”[All Fields]) AND (“Structure”[Journal] OR “structure”[All Fields]))) OR ((“blood platelets”[MeSH Terms] OR (“blood”[All Fields] AND “platelets”[All Fields]) OR “blood platelets”[All Fields] OR “platelet”[All Fields]) AND size[All Fields])) AND ((((((((“osteoporosis, postmenopausal”[MeSH Terms] OR (“osteoporosis”[All Fields] AND “postmenopausal”[All Fields]) OR “postmenopausal osteoporosis”[All Fields] OR “osteoporosis”[All Fields] OR “osteoporosis”[MeSH Terms]) OR (“bone demineralization, pathologic”[MeSH Terms] OR (“bone”[All Fields] AND “demineralization”[All Fields] AND “pathologic”[All Fields]) OR “pathologic bone demineralization”[All Fields] OR (“bone”[All Fields] AND “demineralization”[All Fields]) OR “bone demineralization”[All Fields])) OR (“bone density”[MeSH Terms] OR (“bone”[All Fields] AND “density”[All Fields]) OR “bone density”[All Fields])) OR (“osteoporotic fractures”[MeSH Terms] OR (“osteoporotic”[All Fields] AND “fractures”[All Fields]) OR “osteoporotic fractures”[All Fields])) OR (“bone diseases, metabolic”[MeSH Terms] OR (“bone”[All Fields] AND “diseases”[All Fields] AND “metabolic”[All Fields]) OR “metabolic bone diseases”[All Fields] OR “osteopenia”[All Fields])) OR (“bone diseases, metabolic”[MeSH Terms] OR (“bone”[All Fields] AND “diseases”[All Fields] AND “metabolic”[All Fields]) OR “metabolic bone diseases”[All Fields] OR (“bone”[All Fields] AND “loss”[All Fields]) OR “bone loss”[All Fields])) OR (“bone density”[MeSH Terms] OR (“bone”[All Fields] AND “density”[All Fields]) OR “bone density”[All Fields])) OR bmd[All Fields]) AND (“2009/07/27”[PDAT]: “2019/07/27”[PDAT]) |
| ProQuest | (platelet AND (bdl(1007527) AND pd(20090727-20190727))) AND (osteoporosis AND (bdl(1007527) AND pd(20090727-20190727))) Applied limits: Database: Biological Science Collection British Nursing Database Health Research Premium Collection Part of the search defined by the query is performed in these databases. Restricted based on: Database: Biological Science Collection; Health Research Premium Collection; Biological Science Index; MEDLINE®; TOXLINE |
| Web of Science Core Collection | (TS = platelet OR TS = platelets OR TS = platelet functions OR TS = platelet changes OR TS = platelet structure OR TS = platelet size) AND (TS = osteoporosis OR TS = bone demineralization OR TS = bone density OR TS = Osteoporotic Fractures OR TS = osteopenia OR TS = bone loss OR TS = bone density OR TS = bmd)—with Publication Year from 2009 to 2019 |
| Scopus | (TITLE-ABS-KEY (platelet) OR TITLE-ABS-KEY (platelets) OR TITLE-ABS-KEY (platelet AND functions) OR TITLE-ABS-KEY (platelet AND changes) OR TITLE-ABS-KEY (platelet AND structure) OR TITLE-ABS-KEY (platelet AND size) AND TITLE-ABS-KEY (osteoporosis) OR TITLE-ABS-KEY (bone AND demineralization) AND TITLE-ABS-KEY (bone AND density) OR TITLE-ABS-KEY (osteoporotic AND fractures) OR TITLE-ABS-KEY (osteopenia) OR TITLE-ABS-KEY (bone AND loss) OR TITLE-ABS-KEY (bone AND density) OR TITLE-ABS-KEY (bmd) OR TITLE-ABS-KEY (bone AND mass)) AND DOCTYPE (ar) AND PUBYEAR > 2008 |
| Cochrane Central Register of Controlled Trials | ((((((platelet) OR platelets) OR platelet functions) OR platelet changes) OR platelet structure) OR platelet size)) AND (((((((((osteoporosis) OR bone demineralization) OR bone density) OR Osteoporotic Fractures) OR osteopenia) OR bone loss) OR bone density) OR bmd) in All Text—with Publication Year from 2009 to 2019 |
| Reference | Aim | Study Design | Methodology | Platelet Function | Link Between Platelet and Osteoporosis | Main Results |
|---|---|---|---|---|---|---|
| In vitro studies | ||||||
| Pountos et al. 2010 [39] | Effect of BMP-2, BMP-7, PTH, and PDGF on proliferation and osteogenic differentiation of OP MSCs | MSCs isolated from trabecular bone of 10 OP patients (4 male and 6 female) treated with a 106 range of concentrations (0.001 to100 ng/mL) of PDGF-BB | Functional assays of proliferation and osteogenic differentiation | PDGF-BB | PDGF-BB have a positive effect on osteogenic differentiation of OP MSCs | MSC proliferation stimulated by BMP-7 and PDGF-BB |
| In vivo studies | ||||||
| Xie et al. 2014 [40] | Role of PDGF-BB in OVX mice | OVX C57BL/6 female mice injected with 1 μg PDGF-BB into the bone marrow cavity | Micro-CT, immunocytochemistry, immunofluorescence and histomorphometry. | PDGF-BB | Local PDGF-BB administration can temporally increase angiogenesis and spatially promote bone formation to couple angiogenesis with osteogenesis in bone modeling and remodeling | ↑PDGF-BB concentrations, VEGF concentrations, vessel volume, CD31hi Emcnhi cells, proliferation of endothelial cells in metaphysis, trabecular bone volume, thickness and number, cortical bone thickness, serum osteocalcin concentration in OVX mice treated with PDGF-BB |
| Zhang et al. 2014 [41] | Effect on osteointegration of nanotube arrays loaded with rhPDGF-BB | OVX rat femur implantation: - oxalic acid-etched titanium rods - titanium rods modified with TiO2 nanotube arrays - PDGF group (titanium rods immersed in 100 μg/mL rhPDGF-BB) - PDGF + Vacuum extraction (vacuum pump -PDGF + Vacuum group-for 10 min) | Static and dynamic histomorphometry and biomechanical test | PDGF-BB | Immobilization of rhPDGF-BB on nanotube arrays as implant surface modification strategy in orthopedic applications in osteoporotic patients | rhPDGF-BB immobilized on the nanotube surface ↑ new bone formation and osseointegration |
| Tang et al. 2017 [42] | Association between low plasma PDGF-BB levels and oestradiol | Sprague–Dawley rat: -Sham -OVX -OVX+oestradiol (100 mg/kg/d) -OVX+PDGF-BB (1mg/3 d/wk) | Plasma oestradiol and PDGF-BB levels measured using ELISA kits | PDGF-BB | Plasma PDGF-BB levels play a major role in OVX rats | ↓PDGF-BB levels in OVX rats than SHAM group. Oestradiol replacement ↑plasma PDGF-BB levels, while PDGF-BB systematic treatment not affect plasma estradiol levels |
| Clinical studies | ||||||
| Kim et al. 2011 [43] | Association between peripheral blood cell (PLT, WBC, RBC) counts BMD | Case-control study 17 OP patients 167 osteopenic patients 154 control subjects | DXA, biochemical parameters | PLTs count | Positive relationship between blood cell counts and BMD | WBC, RBC and PLT counts significantly associated with BMD |
| Li et al. 2012 [44] | Relationship between PLT count, MPV, and BMD | Case-control study 111 OP patients 171 osteopenic patients 128 control subjects | DXA, biochemical parameters | PLTs count and MPV | MPV negatively correlated with BMD | Negative correlation between MPV and the lumbar and femoral neck BMD. Univariate and multivariate analysis: MPV significantly associated with lumbar spine L2–L4 BMD and femoral neck BMD |
| D’Amelio et al. 2012 [45] | Correlation between PLTs vitamin D receptor expression and OP | Case-control study 77 postmenopausal OP patients 33 healthy control of childbearing age 49 healthy control men 11 healthy women matched with patients for age and postmenopausal period | DXA, markers of bone metabolism and vitamin D receptor levels | PLTs vitamin D receptor expression | Reduced level of PLT vitamin D receptor is correlate to OP | ↓PLTs vitamin D receptor expression in OP patients respect to healthy postmenopausal controls. PLTs vitamin D receptor not influenced by gender. PLTs vitamin D receptor predict 65% of the BMD variation. |
| Akbal et al. 2014 [32] | Correlation between BMD and MPV and PDW | Case-control study 30 OP patients 30 osteopenic patients 20 control subjects | DXA, full laboratory test | MPV PDW | Significant role of PDW and MPV in the postmenopausal OP development | ↓MPV and PDW in OP than the normal BMD patients. PDW positively correlated with FTT and L1–4T scores. Age and PDW independently related to FTT and LTT scores. |
| Kim et al. 2015 [34] | Association between plasma PAF, OP vertebral fracture and BMD | Case-control study 73 OP patients with vertebral fracture 73 OP patients without vertebral fracture | Radiography, DXA, biochemical parameters, plasma PAF concentration | PAF | Plasma PAF levels inversely correlated with BMD | 34.6% ↑ plasma PAF levels in postmenopausal women with vertebral fracture than subjects without vertebral fracture |
| Aypak et al. 2016 [46] | Correlation between BMD and MPV | Case-control study 126 OP patients 37 osteopenic patients 12 control subjects | DXA, laboratory tests including complete blood count (CBC), calcium, phosphorus, serum 25 hydroxyvitamin D (25OHD), and intact parathormone (iPTH) | MPV | MPV correlated with BMD in postmenopausal OP women. | MPV significantly associated with BMD in normal weight and overweight-obese OP patients. |
| Tang et al. 2017 [42] | Association between low plasma PDGF-BB levels and oestradiol in postmenopausal OP | Case-control study 28 postmenopausal OP patients 69 control young woman 24 age-matched women | DXA, plasma oestradiol and PDGF-BB levels | PDGF-BB | Plasma PDGF-BB levels maintained by oestrogen in normal young women and play a major role in postmenopausal OP | ↓plasma oestradiol and PDGF-BB levels in postmenopausal women, especially in OP patients. PDGF-BB levels were positively correlated with oestradiol levels and inversely correlated with age |
| Vural et al. 2017 [47] | Correlation between PLT functions, vitamin D and BMD | Case-control study 124 OP patients 151 osteopenic patients 87 control subjects | DXA, biochemical parameters | MPV | No correlation between MPV and OP. MPV considered a less important indicator in serum 25-hydroxyvitamin D levels and OP | No difference in MPV and PLT counts between groups. No correlation between MPV and serum 25-hydroxyvitamin D levels. Correlation between PLT count and lumbar spine (L1–4) T score |
| Koseoglu et al. 2017 [48] | Correlation between PLT/lymphocyte ratio and low BMD in postmenopausal woman | Case-control study 179 OP and osteopenic patients 32 control subjects | DXA, biochemical parameters | PLT/lymphocyte ratio | PLT/lymphocyte ratio as new inflammatory marker for bone loss and low BMD | ↑PLT/lymphocyte ratio in OP and osteopenic patients than in the control subjects. Negative correlation between lumbar and femur neck BMD and PLT/lymphocyte ratio |
| Eroglu et al. 2019 [33] | Correlation between PLT/lymphocyte and BMD | Case-control study 48 OP patients 112 osteopenic patients 92 control subjects | DXA, biochemical parameters | PLT/lymphocyte ratio | Negative correlation Between PLT/lymphocyte and BMD | ↑PLT/lymphocyte ratio in OP and osteopenic patients. |
| Reference | Aim | Study Type | Platelet Formulation | Platelets Concentration | White Blood Cells Content | Activation Method | Platelets Application | Experimental Design | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Lo et al. 2009 [49] | Transplantation of PRP/NIH3T3-G cells to induced bone regeneration in OP | in vitro and in vivo | Human PRP | NS | NS | Exogenous-bovine thrombin | NIH3T3-G alone, BMCs alone, and NIH3T3 G/BMC co-culture Bone marrow cavity of the tibia | OVX-SAMP8 mice treated with PRP/NIH3T3-G | PRP/NIH3T3-G treatment prevent OP development |
| Liu et al. 2011 [50] | Balance between adipogenesis and osteogenesis in bone regeneration by PRP for age-related OP | in vitro and in vivo | Human PRP | NS | NS | Exogenous-bovine thrombin | Mouse pre-adipocytes (3T3-L1) and osteoblast cell line (7F2) co-culture Bone marrow cavity of the hind femur | OVX-SAMP8 mice treated with PRP | PRP treatment exert its action promoting bone regeneration and suppressing adipogenesis within the marrow |
| Clafshenkel et al. 2012 [51] | Incorporation of melatonin and/or PRP into CA scaffolds to enhance bone regeneration in OP | in vivo | OVX rat PRP | NS | NS | NS | Calvaria critical-sized defect | OVX rats treated with CA scaffold with PRP and melatonin, associated or not | PRP not improves bone formation |
| Chen et al. 2013 [52] | PRP to promote healing of OP fractures | in vitro and in vivo | OVX rat PRP | High: 8.21 ± 0.4 × 109 Medium:2.65±0.2 × 109 Low: 0.85 ± 0.16x109 PPP:8 ± 0.5x106 (PLTs/mL) | NS | Exogenous-thrombin/CaCl2 | BMSCs culture Femoral fracture | OVX rats treated with high-, medium- and low-concentration PRP and with PPP | Medium-concentration of PRP is the more suitable in promoting fracture healing |
| Cho et al. 2014[53] | Incorporation of PRP into CPC to enhance bone regeneration in OP | in vivo | OVX rat PRP | 4.12 × 109 (PLTs/mL) | NS | NS | Vertebral body critical-size defects | OVX rats treated with CPC associated to PRP | PRP accelerates osteoconduction and improves trabecular bone microarchitecture and BMD |
| Jiang et al. 2016 [54] | PRP treatment and TiO2 nanoporous modification on the stability of titanium implants in OP | in vivo | Human PRP | 2 × 109 (PLTs/mL) | NS | Exogenous-calcium enriched batroxobin | Bone marrow cavity of the hind tibia | OVX rats treated with TiO2 associated to PRP | PRP treatment improves implant biomechanical stability |
| Wei et al. 2016 [55] | PRP in combination with BMSCs for the treatment of OP defect | in vivo | Rats PRP | NS | NS | Exogenous-thrombin | Tibia critical size defects defect | OVX rats treated with allogenic BMSC associated to PRP | PRP combined with BMSCs promotes bone defects healing |
| Rocha et al. 2017 [56] | PRP and MSCs, associated or not, in the repair of bone failures in secondary OP | in vivo | Equine PRP | 200 × 103 (PLTs/µL) | NS | NS | Tibia failures | Rabbits submitted to ovariosalpingohysterectomy and hypercortisolism treated with allogeneic BMSCs and PRP, associated or not | PRP contributes positively to the repair of bone failure, but less than the treatment with MSCs and similarly to the association of both |
| Sakata et al. 2018 [57] | Bone regeneration of OP defects by PRP and β-TCP | in vivo | Rats PRP | NS | NS | NS | Vertebral body critical-size defects | OVX rats treated with β-TCP associated to PRP | PRP associated to β-TCP sponge facilitates bone regeneration in OVX lumbar vertebral bone defect |
| Engler-Pinto et al. 2019 [58] | L-PRF associated or not with bovine bone graft on the healing of OP bone defects | in vivo | Rats L-PRF | NS | NS | NS | Calvaria critical size defects | OVX rats treated with bovine bone graft associated to PRP | L-PRF clot improves bone formation but less than the use of L-PRF associated to bovine bone graft |
| Study | QUIPS | |||||
|---|---|---|---|---|---|---|
| Study Participation | Study Attrition | Prognostic Factor Measurement | Outcome Measurement | Confounding Measurement and Account | Analysis | |
| PLT functions/features and growth factor in PLTs during osteoporosis | ||||||
| Kim et al.2011 [43] | Low | Low | Moderate | Moderate | Moderate | Low |
| Li et al. 2012 [44] | Low | Low | Low | Moderate | Low | Low |
| D’Amelio et al. 2012 [45] | Moderate | High | Moderate | High | Moderate | Moderate |
| Akbal et al. 2014 [32] | Low | Low | Low | Moderate | Low | Low |
| Kim et al. 2015 [34] | Low | Low | Low | Low | Low | Low |
| Aypak et al. 2016 [46] | Low | Low | Low | Moderate | Moderate | Moderate |
| Tang et al. 2017 [42] | Low | Moderate | Moderate | Moderate | Moderate | Moderate |
| Vural et al. 2017 [47] | Low | Low | Low | Moderate | Low | Moderate |
| Koseoglu et al. 2017 [48] | Low | Low | Low | Moderate | Moderate | Low |
| Eroglu et al. 2019 [33] | Low | Moderate | High | Moderate | Moderate | Low |
 low (good) indicator,
low (good) indicator,  moderate indicator,
moderate indicator,  high (bad) indicator.
high (bad) indicator.| SYRCLE | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | Selection Bias | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | Other | ||||
| Sequence Generation | Baseline Characteristics | Allocation Concealment | Random Housing | Blinding | Random Outcome Assessment | Blinding | Incomplete Outcome Data | Selective Outcome Reporting | Other Sources of Bias | |
| PLT functions/features and growth factor in PLTs during osteoporosis | ||||||||||
| Xie et al. 2014 [40] | Yes | Yes | Yes | Yes | No | Unclear | No | No | Yes | No |
| Zhang et al. 2014 [41] | No | Yes | Unclear | Unclear | Unclear | Yes | No | No | Yes | No |
| Tang et al. 2017 [42] | No | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | No | Yes | Yes |
| PLT derivatives in osteoporosis | ||||||||||
| Lo et al. 2009 [49] | No | Unclear | No | Unclear | Unclear | No | No | No | Yes | No |
| Liu et al. 2011 [50] | No | No | No | No | No | No | No | No | Unclear | No |
| Clafshenkel et al. [51] | No | Yes | No | No | No | No | No | Unclear | Yes | Unclear |
| Chen et al. 2013 [52] | No | Unclear | No | No | Yes | No | Yes | No | Yes | No |
| Cho et al. 2014 [53] | No | No | No | No | No | No | Unclear | Yes | Yes | Yes |
| Jiang et al. 2016 [54] | No | Yes | No | No | No | No | No | No | Yes | Unclear |
| Wei et al. 2016 [55] | Unclear | Yes | Unclear | No | No | No | No | No | Yes | No |
| Rocha et al. 2017 [56] | No | No | No | No | No | No | No | Unclear | Yes | Yes |
| Sakata et al. 2018 [57] | No | Yes | Unclear | No | No | No | No | No | Yes | No |
| Engler-Pinto et al. 2019 [58] | Yes | Yes | Yes | No | No | No | Unclear | No | Yes | No |
 positive (good) indicator,
positive (good) indicator,  unclear,
unclear,  negative (bad) indicator.
negative (bad) indicator.© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salamanna, F.; Maglio, M.; Sartori, M.; Tschon, M.; Fini, M. Platelet Features and Derivatives in Osteoporosis: A Rational and Systematic Review on the Best Evidence. Int. J. Mol. Sci. 2020, 21, 1762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21051762
Salamanna F, Maglio M, Sartori M, Tschon M, Fini M. Platelet Features and Derivatives in Osteoporosis: A Rational and Systematic Review on the Best Evidence. International Journal of Molecular Sciences. 2020; 21(5):1762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21051762
Chicago/Turabian StyleSalamanna, Francesca, Melania Maglio, Maria Sartori, Matilde Tschon, and Milena Fini. 2020. "Platelet Features and Derivatives in Osteoporosis: A Rational and Systematic Review on the Best Evidence" International Journal of Molecular Sciences 21, no. 5: 1762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21051762