
Comparison of Cerebellar Grey Matter Alterations in Bipolar and Cerebellar Patients: Evidence from Voxel-Based Analysis

 ,
,  ,
,
Abstract
:1. Introduction
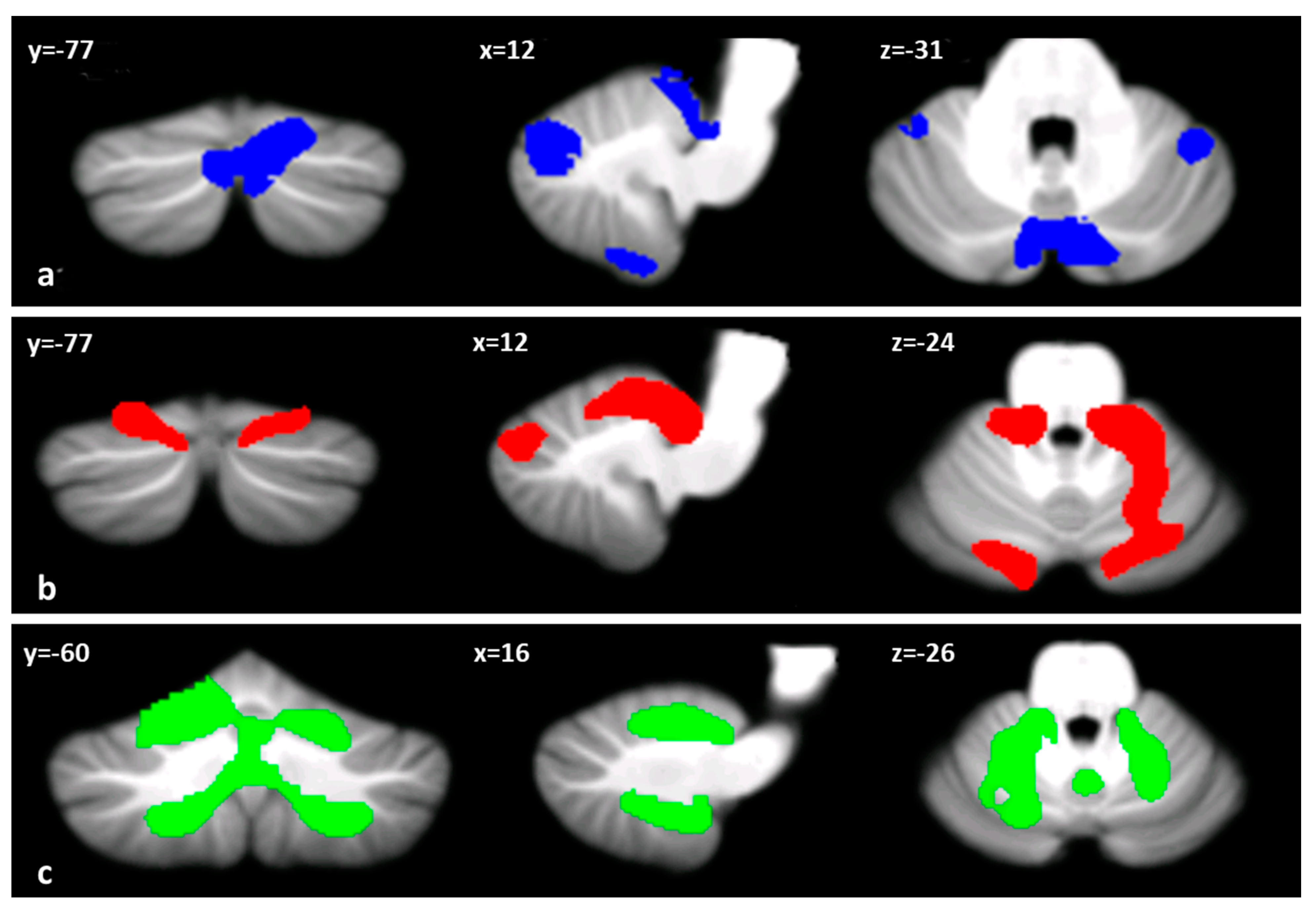
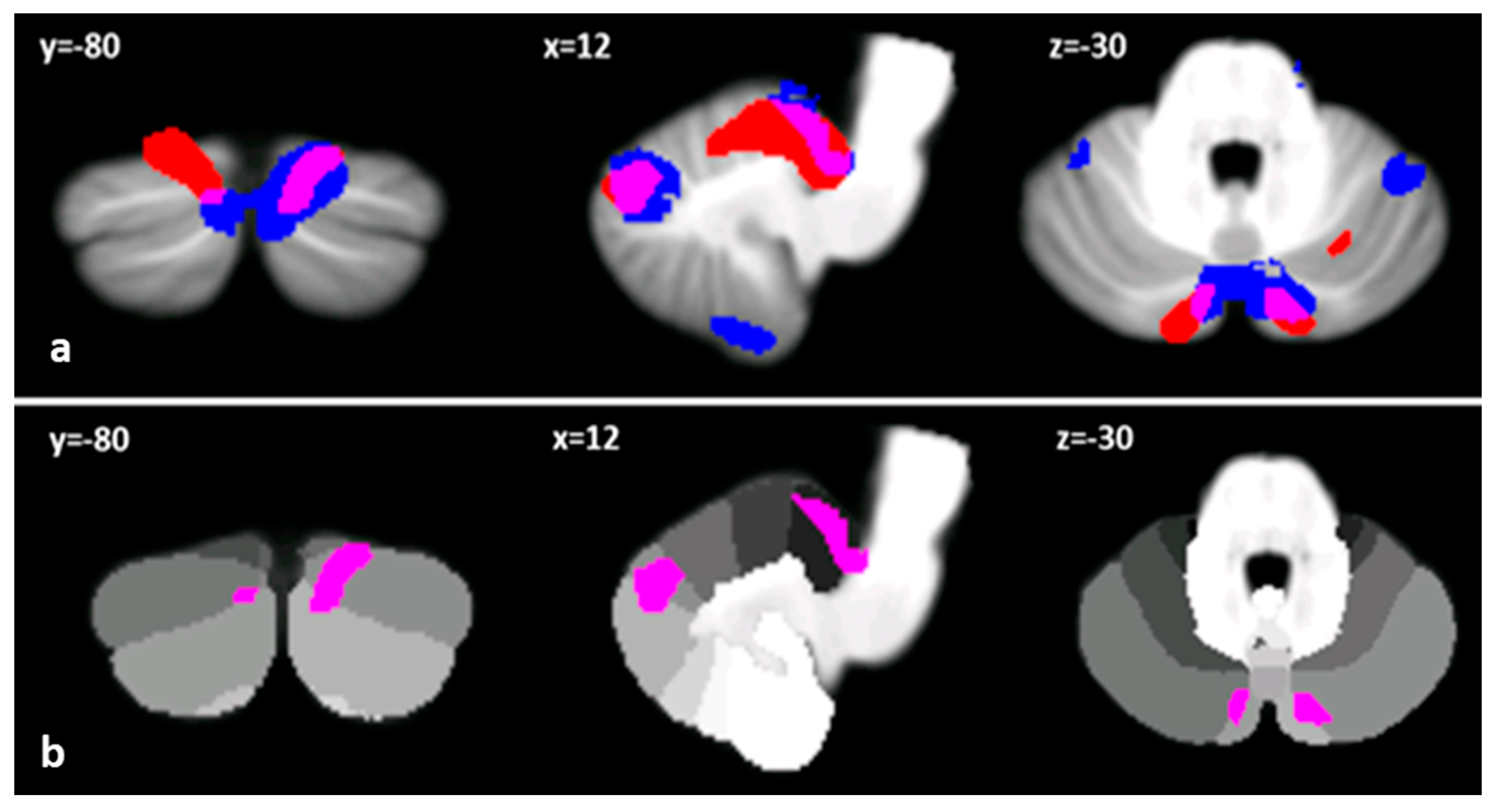
2. Results
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. MRI Acquisition Protocol
4.3. Image Processing and Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Merikangas, K.R.; Akiskal, H.S.; Angst, J.; Greenberg, P.E.; Hirschfeld, R.M.; Petukhova, M.; Kessler, R.C. Lifetime and 12-month prevalence of bipolar spectrum disorder in the National Comorbidity Survey replication. Arch. Gen. Psychiatry 2007, 64, 543–552. [Google Scholar] [CrossRef]
- Prieto, M.L.; Cuéllar-Barboza, A.B.; Bobo, W.V.; Roger, V.L.; Bellivier, F.; Leboyer, M.; West, C.P.; Frye, M.A. Risk of myocardial infarction and stroke in bipolar disorder: A systematic review and exploratory meta-analysis. Acta Psychiatr. Scand 2014, 130, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Dean, B.B.; Gerner, D.; Gerner, R.H. A systematic review evaluating health-related quality of life, work impairment, and healthcare costs and utilization in bipolar disorder. Curr. Med. Res. Opin. 2004, 20, 139–154. [Google Scholar] [CrossRef]
- Grande, I.; Goikolea, J.M.; de Dios, C.; González-Pinto, A.; Montes, J.M.; Saiz-Ruiz, J.; Prieto, E.; Vieta, E.; PREBIS group. Occupational disability in bipolar disorder: Analysis of predictors of being on severe disablement benefit (PREBIS study data). Acta Psychiatr. Scand 2013, 127, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Aran, A.; Vieta, E.; Torrent, C.; Sanchez-Moreno, J.; Goikolea, J.M.; Salamero, M.; Malhi, G.S.; Gonzalez-Pinto, A.; Daban, C.; Alvarez-Grandi, S.; et al. Functional outcome in bipolar disorder: The role of clinical and cognitive factors. Bipolar Disord. 2007, 9, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Palazzo, M.C.; Arici, C.; Cremaschi, L.; Cristoffanini, M.; Dobrea, C.; Dell’Osso, B.; Altamura, A.C. Cognitive Performance in Euthymic Patients with Bipolar Disorder vs Healthy Controls: A Neuropsychological Investigation. Clin. Pract. Epidemiol. Ment Health 2017, 13, 71–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparding, T.; Silander, K.; Pålsson, E.; Östlind, J.; Sellgren, C.; Ekman, C.J.; Joas, E.; Hansen, S.; Landén, M. Cognitive Functioning in Clinically Stable Patients With Bipolar Disorder I and II. PLoS ONE 2015, 10, e0115562. [Google Scholar] [CrossRef] [Green Version]
- Mann-Wrobel, M.C.; Carreno, J.T.; Dickinson, D. Meta-analysis of neuropsychological functioning in euthymic bipolar disorder: An update and investigation of moderate variables. Bipolar Disord. 2011, 13, 334–342. [Google Scholar] [CrossRef]
- Robinson, L.J.; Thompson, J.M.; Gallagher, P.; Goswami, U.; Young, A.H.; Ferrier, I.N.; Moore, P.B. A meta-analysis of cognitive deficits in euthymic patients with bipolar disorder. J. Affect. Disord. 2006, 93, 105–115. [Google Scholar] [CrossRef]
- Torres, I.J.; Boudreau, V.G.; Yatham, L.N. Neuropsychological functioning in euthymic bipolar disorder: A meta-analysis. Acta Psychiatr. Scand Suppl. 2007, 434, 17–26. [Google Scholar] [CrossRef]
- Adler, C.M.; Del Bello, M.P.; Jarvis, K.; Levine, A.; Adams, J.; Strakowski, S.M. Voxel-based study of structural changes in first-episode patients with bipolar disorder. Biol. Psychiatry 2007, 61, 776–781. [Google Scholar] [CrossRef]
- Lyoo, I.K.; Kim, M.J.; Stoll, A.L.; Demopulos, C.M.; Parow, A.M.; Dager, S.R.; Friedman, S.D.; Dunner, D.L.; Renshaw, P.F. Frontal lobe gray matter density decreases in bipolar I disorder. Biol. Psychiatry 2004, 55, 648–651. [Google Scholar] [CrossRef]
- Shaffer, J.J., Jr.; Johnson, C.P.; Fiedorowicz, J.G.; Christensen, G.E.; Wemmie, J.A.; Magnotta, V.A. Impaired Sensory Processing Measured by Functional MRI in Bipolar Disorder Manic and Depressed Mood States. Brain Imaging Behav. 2018, 12, 837–847. [Google Scholar] [CrossRef]
- Baumann, O.; Mattingley, J.B. Functional topography of primary emotion processing in the human cerebellum. Neuroimage 2012, 61, 805–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, D.; Luo, C.; Guell, X.; Wang, Y.; He, H.; Duan, M.; Eickhoff, S.B.; Yao, D. Compression of Cerebellar Functional Gradients in Schizophrenia. Schizophr. Bull. 2020. [Google Scholar] [CrossRef] [PubMed]
- Leggio, M.; Olivito, G. Topography of the cerebellum in relation to social brain regions and emotions. Handb. Clin. Neurol. 2018, 154, 71–84. [Google Scholar] [CrossRef]
- Sha, Z.; Edmiston, E.K.; Versace, A.; Fournier, J.C.; Graur, S.; Greenberg, T.; Lima Santos, J.P.; Chase, H.W.; Stiffler, R.S.; Bonar, L.; et al. Functional Disruption of Cerebello-thalamo-cortical Networks in Obsessive-Compulsive Disorder. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019, 5, 438–447. [Google Scholar] [CrossRef]
- Siciliano, L.; Clausi, S. Implicit vs. Explicit Emotion Processing in Autism Spectrum Disorders: An Opinion on the Role of the Cerebellum. Front. Psychol. 2020, 11, 96. [Google Scholar] [CrossRef] [PubMed]
- Stoodley, C.J.; Schmahmann, J.D. Functional topography in the human cerebellum: A meta-analysis of neuroimaging studies. Neuroimage 2009, 44, 489–501. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, B.; Li, K.; Wang, X.; Li, X.; Zhu, J.; Zhao, Q.; Yang, Y.; Lv, L.; Zhang, M.; et al. Altered Functional Connectivity Between the Cerebellum and the Cortico-Striato-Thalamo-Cortical Circuit in Obsessive-Compulsive Disorder. Front. Psychiatry 2019, 10, 522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhuo, C.; Wang, C.; Wang, L.; Guo, X.; Xu, Q.; Liu, Y.; Zhu, J. Altered resting-state functional connectivity of the cerebellum in schizophrenia. Brain Imaging Behav. 2018, 12, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Lupo, M.; Siciliano, L.; Leggio, M. From cerebellar alterations to mood disorders: A systematic review. Neurosci. Biobehav. Rev. 2019, 103, 21–28. [Google Scholar] [CrossRef]
- Sani, G.; Chiapponi, C.; Piras, F.; Ambrosi, E.; Simonetti, A.; Danese, E.; Janiri, D.; Brugnoli, R.; De Filippis, S.; Caltagirone, C.; et al. Gray and white matter trajectories in patients with bipolar disorder. Bipolar Disord. 2016, 18, 52–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldaçara, L.; Borgio, J.G.; Lacerda, A.L.; Jackowski, A.P. Cerebellum and psychiatric disorders. Braz. J. Psychiatry 2008, 30, 281–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Bello, M.P.; Strakowski, S.M.; Zimmermann, M.E.; Hawkins, J.M.; Sax, K.W. MRI analysis of the cerebellum in bipolar disorder: A pilot study. Neuropsychopharmacology 1999, 21, 63–68. [Google Scholar] [CrossRef]
- Kim, D.; Cho, H.B.; Dager, S.R.; Yurgelun-Todd, D.A.; Yoon, S.; Lee, J.H.; Lee, S.H.; Lee, S.; Renshaw, P.F.; Lyoo, I.K. Posterior Cerebellar Vermal Deficits in Bipolar Disorder. J. Affect. Disord. 2013, 150, 499–506. [Google Scholar] [CrossRef] [Green Version]
- Mills, N.P.; Del Bello, M.P.; Adler, C.M.; Strakowski, S.M. MRI analysis of cerebellar vermal abnormalities in bipolar disorder. Am. J. Psychiatry 2005, 162, 1530–1532. [Google Scholar] [CrossRef]
- Chen, G.; Zhao, L.; Jia, Y.; Zhong, S.; Chen, F.; Luo, X.; Qiu, S.; Lai, S.; Qi, Z.; Huang, L.; et al. Abnormal cerebellum-DMN Regions Connectivity in Unmedicated Bipolar II Disorder. J. Affect. Disord. 2019, 243, 441–447. [Google Scholar] [CrossRef]
- Johnson, C.P.; Christensen, G.E.; Fiedorowicz, J.G.; Mani, M.; Shaffer, J.J., Jr.; Magnotta, V.A.; Wemmie, J.A. Alterations of the cerebellum and basal ganglia in bipolar disorder mood states detected by quantitative T1ρ mapping. Bipolar Disord. 2018, 20, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Shinn, A.K.; Roh, Y.S.; Ravichandran, C.T.; Baker, J.T.; Öngür, D.; Cohen, B.M. Aberrant cerebellar connectivity in bipolar disorder with psychosis. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2017, 2, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Wang, Y.; Jia, Y.; Zhong, S.; Sun, Y.; Zhou, Z.; Zhang, Z.; Huang, L. Cerebellar microstructural abnormalities in bipolar depression and unipolar depression: A diffusion kurtosis and perfusion imaging study. J. Affect. Disord. 2016, 195, 21–31. [Google Scholar] [CrossRef]
- Zhao, L.; Luo, Z.; Qiu, S.; Jia, Y.; Zhong, S.; Chen, G.; Lai, S.; Qi, Z.; Luo, X.; Huang, G.; et al. Abnormalities of aquaporin-4 in the cerebellum in bipolar II disorder: An ultra-high b values diffusion weighted imaging study. J. Affect. Disord. 2020, 274, 136–143. [Google Scholar] [CrossRef]
- Deng, W.; Zhang, B.; Zou, W.; Zhang, X.; Cheng, X.; Guan, L.; Lin, Y.; Lao, G.; Ye, B.; Li, X.; et al. Abnormal Degree Centrality Associated With Cognitive Dysfunctions in Early Bipolar Disorder. Front. Psychiatry 2019, 10, 140. [Google Scholar] [CrossRef]
- Luo, X.; Chen, G.; Jia, Y.; Gong, J.; Qiu, S.; Zhong, S.; Zhao, L.; Chen, F.; Lai, S.; Qi, Z.; et al. Disrupted Cerebellar Connectivity With the Central Executive Network and the Default-Mode Network in Unmedicated Bipolar II Disorder. Front. Psychiatry 2018, 9, 705. [Google Scholar] [CrossRef]
- Clausi, S.; Iacobacci, C.; Lupo, M.; Olivito, G.; Molinari, M.; Leggio, M. The Role of the Cerebellum in Unconscious and Conscious Processing of Emotions: A Review. Appl. Sci. 2017, 7, 521. [Google Scholar] [CrossRef] [Green Version]
- Heath, R.G.; Dempesy, C.W.; Fontana, C.J.; Myers, W.A. Cerebellar stimulation: Effects on septal region, hippocampus, and amygdala of cats and rats. Biol. Psychiatry 1978, 13, 501–529. [Google Scholar]
- Lupo, M.; Troisi, E.; Chiricozzi, F.R.; Clausi, S.; Molinari, M.; Leggio, M. Inability to Process Negative Emotions in Cerebellar Damage: A Functional Transcranial Doppler Sonographic Study. Cerebellum 2015, 14, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Strata, P. The emotional cerebellum. Cerebellum 2015, 14, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, N.S.; Huitema, R.B.; Spikman, J.M.; Luijckx, G.J.; de Haan, E.H.F. Impairments in Emotion Recognition and Risk-Taking Behavior After Isolated, Cerebellar Stroke. Cerebellum 2020, 19, 419–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clausi, S.; Olivito, G.; Lupo, M.; Siciliano, L.; Bozzali, M.; Leggio, M. The Cerebellar Predictions for Social Interactions: Theory of Mind Abilities in Patients With Degenerative Cerebellar Atrophy. Front. Cell Neurosci. 2019, 12, 510. [Google Scholar] [CrossRef] [PubMed]
- Olivito, G.; Siciliano, L.; Clausi, S.; Lupo, M.; Romano, S.; Masciullo, M.; Molinari, M.; Cercignani, M.; Bozzali, M.; Leggio, M. Functional Changes of Mentalizing Network in SCA2 Patients: Novel Insights into Understanding the Social Cerebellum. Cerebellum 2020, 19, 235–242. [Google Scholar] [CrossRef]
- Koziol, L.F.; Budding, D.; Andreasen, N.; D’Arrigo, S.; Bulgheroni, S.; Imamizu, H.; Ito, M.; Manto, M.; Marvel, C.; Parker, K.; et al. Consensus paper: The cerebellum’s role in movement and cognition. Cerebellum 2014, 13, 151–177. [Google Scholar] [CrossRef]
- Leggio, M.G.; Chiricozzi, F.R.; Clausi, S.; Tedesco, A.M.; Molinari, M. The neuropsychological profile of cerebellar damage: The sequencing hypothesis. Cortex 2011, 47, 137–144. [Google Scholar] [CrossRef]
- Schmahmann, J.D. The cerebellum and cognition. Neurosci. Lett. 2019, 688, 62–75. [Google Scholar] [CrossRef]
- Tedesco, A.M.; Chiricozzi, F.R.; Clausi, S.; Lupo, M.; Molinari, M.; Leggio, M.G. The cerebellar cognitive profile. Brain 2011, 134, 3672–3686. [Google Scholar] [CrossRef] [PubMed]
- Clausi, S.; Lupo, M.; Olivito, G.; Siciliano, L.; Contento, M.P.; Aloise, F.; Pizzamiglio, L.; Molinari, M.; Leggio, M. Depression disorder in patients with cerebellar damage: Awareness of the mood state. J. Affect. Disord. 2019, 245, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Delle Chiaie, R.; Minichino, A.; Salviati, M.; Fiorentini, S.; Tonini, A.; Bersani, F.S.; De Michele, F.; Caredda, M.; Biondi, M. Bipolar spectrum disorders in patients with cerebellar lesions. A comparison with Parkinson’s Disease. J. Nerv. Ment. Dis. 2015, 203, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Lupo, M.; Olivito, G.; Siciliano, L.; Masciullo, M.; Bozzali, M.; Molinari, M.; Leggio, M. Development of a Psychiatric Disorder Linked to Cerebellar Lesions. Cerebellum 2018, 17, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Lupo, M.; Olivito, G.; Siciliano, L.; Masciullo, M.; Molinari, M.; Cercignani, M.; Bozzali, M.; Leggio, M. Evidence of Cerebellar Involvement in the Onset of a Manic State. Front. Neurol. 2018, 9, 774. [Google Scholar] [CrossRef]
- Schmahmann, J.D.; Sherman, J.C. The cerebellar cognitive affective syndrome. Brain 1998, 121, 561–579. [Google Scholar] [CrossRef]
- Diedrichsen, J.; Balsters, J.H.; Flavell, J.; Cussans, E.; Ramnani, N. A probabilistic MR atlas of the human cerebellum. Neuroimage 2009, 46, 39–46. [Google Scholar] [CrossRef]
- Buckner, R.L.; Krienen, F.M.; Castellanos, A.; Diaz, J.C.; Yeo, B.T. The organization of the human cerebellum estimated by intrinsic functional connectivity. J. Neurophysiol. 2011, 106, 2322–2345. [Google Scholar] [CrossRef]
- Habas, C.; Kamdar, N.; Nguyen, D.; Prater, K.; Beckmann, C.F.; Menon, V.; Greicius, M.D. Version 2. Distinct cerebellar contributions to intrinsic connectivity networks. J. Neurosci. 2009, 29, 8586–8594. [Google Scholar] [CrossRef]
- Lupo, M.; Olivito, G.; Clausi, S.; Siciliano, L.; Riso, V.; Bozzali, M.; Santorelli, F.M.; Silvestri, G.; Leggio, M. Cerebello-Cortical Alterations Linked to Cognitive and Social Problems in Patients With Spastic Paraplegia Type 7: A Preliminary Study. Front. Neurol. 2020, 11, 82. [Google Scholar] [CrossRef] [PubMed]
- Olivito, G.; Lupo, M.; Iacobacci, C.; Clausi, S.; Romano, S.; Masciullo, M.; Molinari, M.; Cercignani, M.; Bozzali, M.; Leggio, M. Structural cerebellar correlates of cognitive functions in spinocerebellar ataxia type 2. J. Neurol. 2018, 265, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Van Overwalle, F.; D’aes, T.; Mariën, P. Social cognition and the cerebellum: A meta-analytic connectivity analysis. Hum. Brain Mapp. 2015, 36, 5137–5154. [Google Scholar] [CrossRef]
- Kraepein, E. Manic-Depressive Insanity and Paranoia; Livingston: Edinburgh, UK, 1921. [Google Scholar]
- Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013.
- Toniolo, S.; Serra, L.; Olivito, G.; Marra, C.; Bozzali, M.; Cercignani, M. Patterns of cerebellar gray matter atrophy across Alzheimer’s disease progression. Front. Cell. Neurosci. 2018, 12, 430. [Google Scholar] [CrossRef] [PubMed]
- Bourne, C.; Aydemir, Ö.; Balanzá-Martínez, V.; Bora, E.; Brissos, S.; Cavanagh, J.T.; Clark, L.; Cubukcuoglu, Z.; Dias, V.V.; Dittmann, S.; et al. Neuropsychological testing of cognitive impairment in euthymic bipolar disorder: An individual patient data meta-analysis. Acta Psychiatr. Scand. 2013, 128, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, O.; Albayrak, Y.; Ekinci, A.E.; Caykoylu, A. Relationship of trait impulsivity with clinical presentation in euthymic bipolar disorder patients. Psychiatry Res. 2011, 190, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, P.; Gray, J.M.; Watson, S.; Young, A.H.; Ferrier, I.N. Neurocognitive functioning in bipolar depression: A component structure analysis. Psychol. Med. 2014, 44, 961–974. [Google Scholar] [CrossRef] [Green Version]
- O’Shea, R.; Poz, R.; Michael, A.; Berrios, G.E.; Evans, J.J.; Rubinsztein, J.S. Ecologically valid cognitive tests and everyday functioning in euthymic bipolar disorder patients. J. Affect. Disord. 2010, 125, 336–340. [Google Scholar] [CrossRef]
- Ambrosi, E.; Chiapponi, C.; Sani, G.; Manfredi, G.; Piras, F.; Caltagirone, C.; Spalletta, G. White matter microstructural characteristics in Bipolar I and Bipolar II Disorder: A diffusion tensor imaging study. J. Affect. Disord. 2016, 189, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Mahon, K.; Burdick, K.E.; Szeszko, P.R. A role for white matter abnormalities in the pathophysiology of bipolar disorder. Neurosci. Biobehav. Rev. 2010, 34, 533–554. [Google Scholar] [CrossRef] [Green Version]
- Narita, K.; Suda, M.; Takei, Y.; Aoyama, Y.; Majima, T.; Kameyama, M.; Kosaka, H.; Amanuma, M.; Fukuda, M.; Mikuni, M. Volume reduction of ventromedial prefrontal cortex in bipolar II patients with rapid cycling: A voxel-based morphometric study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Strakowski, S.M.; Eliassen, J.C.; Lamy, M.; Cerullo, M.A.; Allendorfer, J.B.; Madore, M.; Lee, J.H.; Welge, J.A.; Del Bello, M.P.; Fleck, D.E.; et al. Functional magnetic resonance imaging brain activation in bipolar mania: Evidence for disruption of the ventrolateral prefrontal-amygdala emotional pathway. Biol. Psychiatry 2011, 69, 381–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Zhong, S.; Jia, Y.; Zhou, Z.; Wang, B.; Pan, J.; Huang, L. Interhemispheric Resting State Functional Connectivity Abnormalities in Unipolar Depression and Bipolar Depression. Bipolar Disord. 2015, 17, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Olivito, G.; Cercignani, M.; Lupo, M.; Iacobacci, C.; Clausi, S.; Romano, S.; Masciullo, M.; Molinari, M.; Bozzali, M.; Leggio, M. Neural substrates of motor and cognitive dysfunctions in SCA2 patients: A network based statistics analysis. Neuroimage Clin. 2017, 14, 719–725. [Google Scholar] [CrossRef]
- Dayan, M.; Olivito, G.; Molinari, M.; Cercignani, M.; Bozzali, M.; Leggio, M. Impact of Cerebellar Atrophy on Cortical Gray Matter and Cerebellar Peduncles as Assessed by Voxel-Based Morphometry and High Angular Resolution Diffusion Imaging. Funct. Neurol. 2016, 31, 239–248. [Google Scholar] [CrossRef]
- Ginestroni, A.; Della Nave, R.; Tessa, C.; Giannelli, M.; De Grandis, D.; Plasmati, R.; Salvi, F.; Piacentini, S.; Mascalchi, M. Brain structural damage in spinocerebellar ataxia type 1: A VBM study. J. Neurol. 2008, 255, 1153–1158. [Google Scholar] [CrossRef]
- Stoodley, C.J.; MacMore, J.P.; Makris, N.; Sherman, J.C.; Schmahmann, J.D. Location of lesion determines motor vs. cognitive consequences in patients with cerebellar stroke. Neuroimage Clin. 2016, 12, 765–775. [Google Scholar] [CrossRef] [Green Version]
- Stoodley, C.J.; Limperopoulos, C. Structure-function Relationships in the Developing Cerebellum: Evidence From Early-Life Cerebellar Injury and Neurodevelopmental Disorders. Semin. Fetal. Neonatal Med. 2016, 21, 356–364. [Google Scholar] [CrossRef] [Green Version]
- Centorrino, F.; Fogarty, K.V.; Sani, G.; Salvatore, P.; Cincotta, S.L.; Hennen, J.; Guzzetta, F.; Talamo, A.; Saadeh, M.G.; Baldessarini, R.J. Use of combinations of antipsychotics: McLean Hospital inpatients, 2002. Hum. Psychopharmacol. 2005, 20, 485–492. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. SCID-5-CV. Intervista Clinica Strutturata per i Disturbi del DSM-5, Versione per il Clinico; Italiana a cura di Andrea Fossati e Serena Borroni; Raffaello Cortina Editore: Milano, Italy, 2017. [Google Scholar]
- Hamilton, M. Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A rating scale for mania: Reliability, validity and sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Trouillas, P.; Takayanagi, T.; Hallett, M.; Currier, R.D.; Subramony, S.H.; Wessel, K.; Bryer, A.; Diener, H.C.; Massaquoi, S.; Gomez, C.M.; et al. International Cooperative Ataxia Rating Scale for pharmacological assessment of the cerebellar syndrome. The Ataxia Neuropharmacology Committee of the World Federation of Neurology. J. Neurol. Sci. 1977, 145, 205–211. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Adult Intelligence Scale, 4th ed.; Psychological Corporation: San Antonio, TX, USA, 2008. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | BD (n = 29) | CD (n = 32) | HS (n = 37) |
|---|---|---|---|
| Age, years, mean ± SD | 42.69 ± 10.53 | 46.81 ± 11.48 | 45.75 ± 14.26 |
| Males/females | 13/16 | 18/14 | 15/22 |
| ICARS mean ± SD | 1.10 ± 2.06 | 25.78 ± 12.94 | − |
| Cluster Size (NoV) | Coordinates | Peak z-Score | Cerebellar Region | |||
|---|---|---|---|---|---|---|
| x | z | y | ||||
| BD < HS | 4667 | 7 | −78 | −33 | 5.35 | R-Crus II |
| 3358 | 17 | −42 | −12 | 6.86 | R-Lobule V | |
| 20 | −31 | −19 | 5.95 | R-Lobule V | ||
| 1024 | 45 | −46 | −27 | 4.36 | R-Crus I | |
| 892 | −44 | −47 | −45 | 4.38 | L-Crus II | |
| 223 | −41 | −43 | −28 | 4.37 | L-lobule VI | |
| CD < HS | 17246 | −8 | −37 | −19 | 5.99 | L-Lobule I−IV |
| 12 | −37 | −22 | 5.75 | R-Lobule I−IV | ||
| 13 | −48 | −16 | 5.21 | R-Lobule V | ||
| 2047 | −12 | −87 | −29 | 4.77 | L-Crus II | |
| −18 | −79 | −21 | 4.65 | L-Crus I | ||
| CD < BD | 28567 | 22 | −55 | −45 | 6.78 | R-Lobule VIIIb |
| −20 | −61 | −48 | 5.53 | L-Lobule VIIIa | ||
| −14 | −57 | −19 | 5.52 | L-Lobule VI | ||
| Medical Treatment | Mean ± SD | N° |
|---|---|---|
| HDRS | 1.82 ± 2.68 | 29 |
| YMRS | 1.61 ± 3.01 | 29 |
| Current pharmacotherapy | ||
| Antipsychotics | 13 | |
| Lithium | 14 | |
| Antiepileptics | 22 | |
| Antidepressants | 2 | |
| Anxiolytic | 3 | |
| Polypharmacy | 17 | |
| Diagnosis | N° |
|---|---|
| SCA type1 | 1 |
| SCA type 2 | 12 |
| SCA type 6 | 1 |
| SCA type 15 | 1 |
| SCA type 28 | 1 |
| SPG7 | 6 |
| FRDA | 2 |
| ICA | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lupo, M.; Olivito, G.; Gragnani, A.; Saettoni, M.; Siciliano, L.; Pancheri, C.; Panfili, M.; Bozzali, M.; Delle Chiaie, R.; Leggio, M. Comparison of Cerebellar Grey Matter Alterations in Bipolar and Cerebellar Patients: Evidence from Voxel-Based Analysis. Int. J. Mol. Sci. 2021, 22, 3511. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073511
Lupo M, Olivito G, Gragnani A, Saettoni M, Siciliano L, Pancheri C, Panfili M, Bozzali M, Delle Chiaie R, Leggio M. Comparison of Cerebellar Grey Matter Alterations in Bipolar and Cerebellar Patients: Evidence from Voxel-Based Analysis. International Journal of Molecular Sciences. 2021; 22(7):3511. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073511
Chicago/Turabian StyleLupo, Michela, Giusy Olivito, Andrea Gragnani, Marco Saettoni, Libera Siciliano, Corinna Pancheri, Matteo Panfili, Marco Bozzali, Roberto Delle Chiaie, and Maria Leggio. 2021. "Comparison of Cerebellar Grey Matter Alterations in Bipolar and Cerebellar Patients: Evidence from Voxel-Based Analysis" International Journal of Molecular Sciences 22, no. 7: 3511. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073511