
Kynurenine/Tryptophan Ratio as a Potential Blood-Based Biomarker in Non-Small Cell Lung Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patients Series
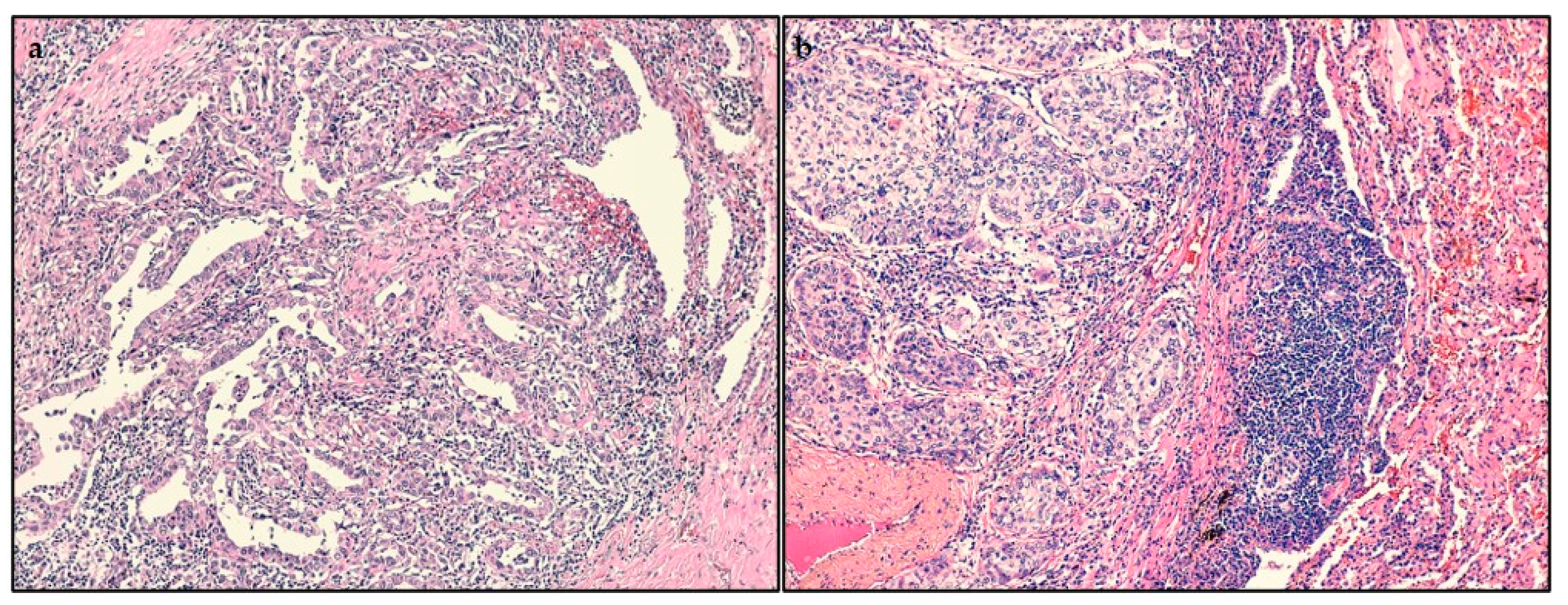
2.2. Histopathological Findings
2.3. Analysis of Tumor-Infiltrating Lymphocytes (TILs)
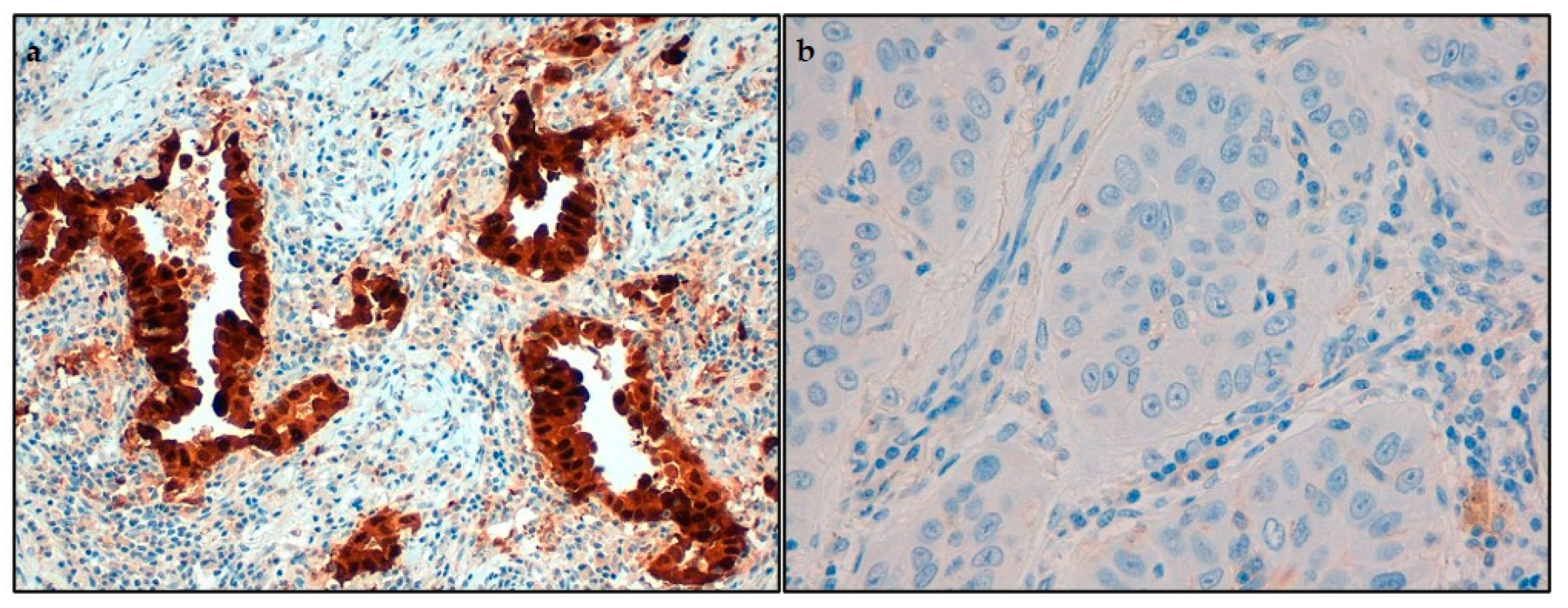
2.4. Immunohistochemical Analysis of IDO1 and Programmed Cell Death Ligand-1 (PD-L1)
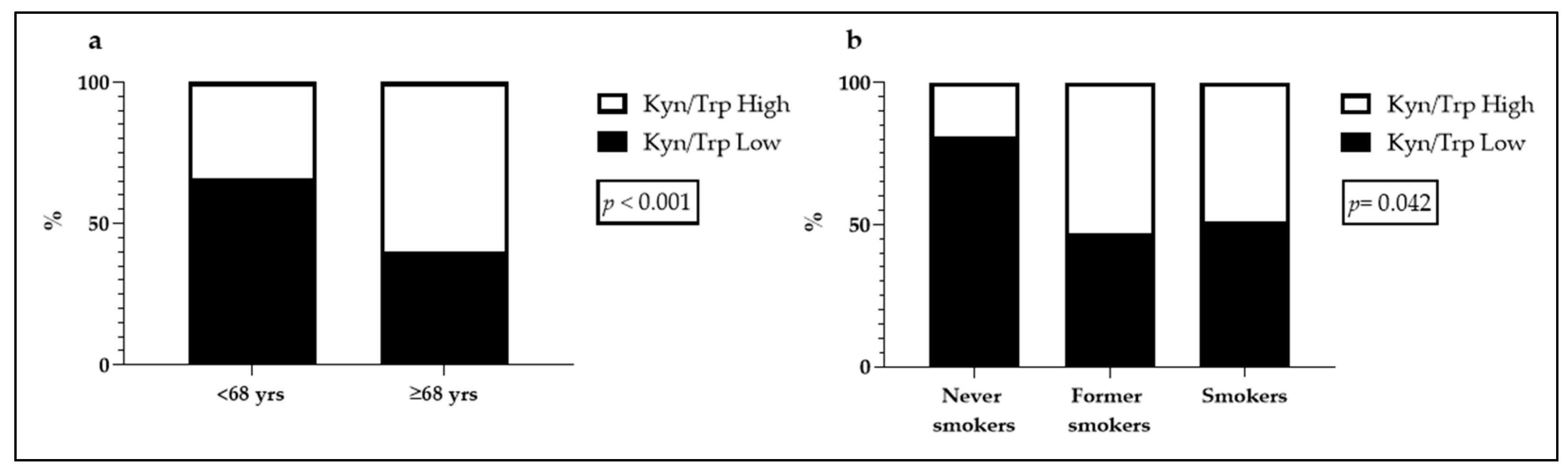
2.5. Kyn/Trp Ratio and Clinical Parameters Associations
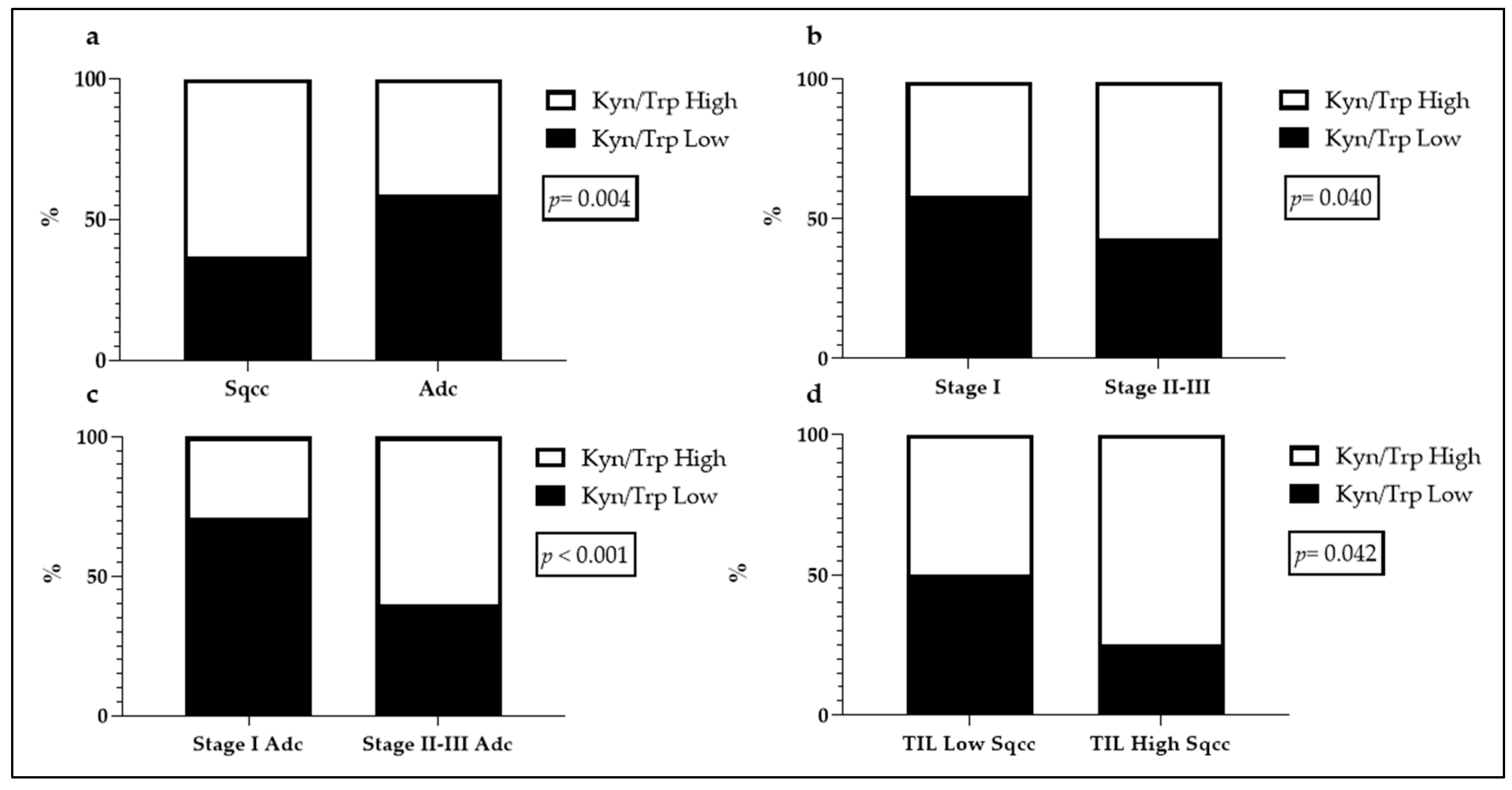
2.6. Kyn/Trp Ratio and Histopathological Findings Associations
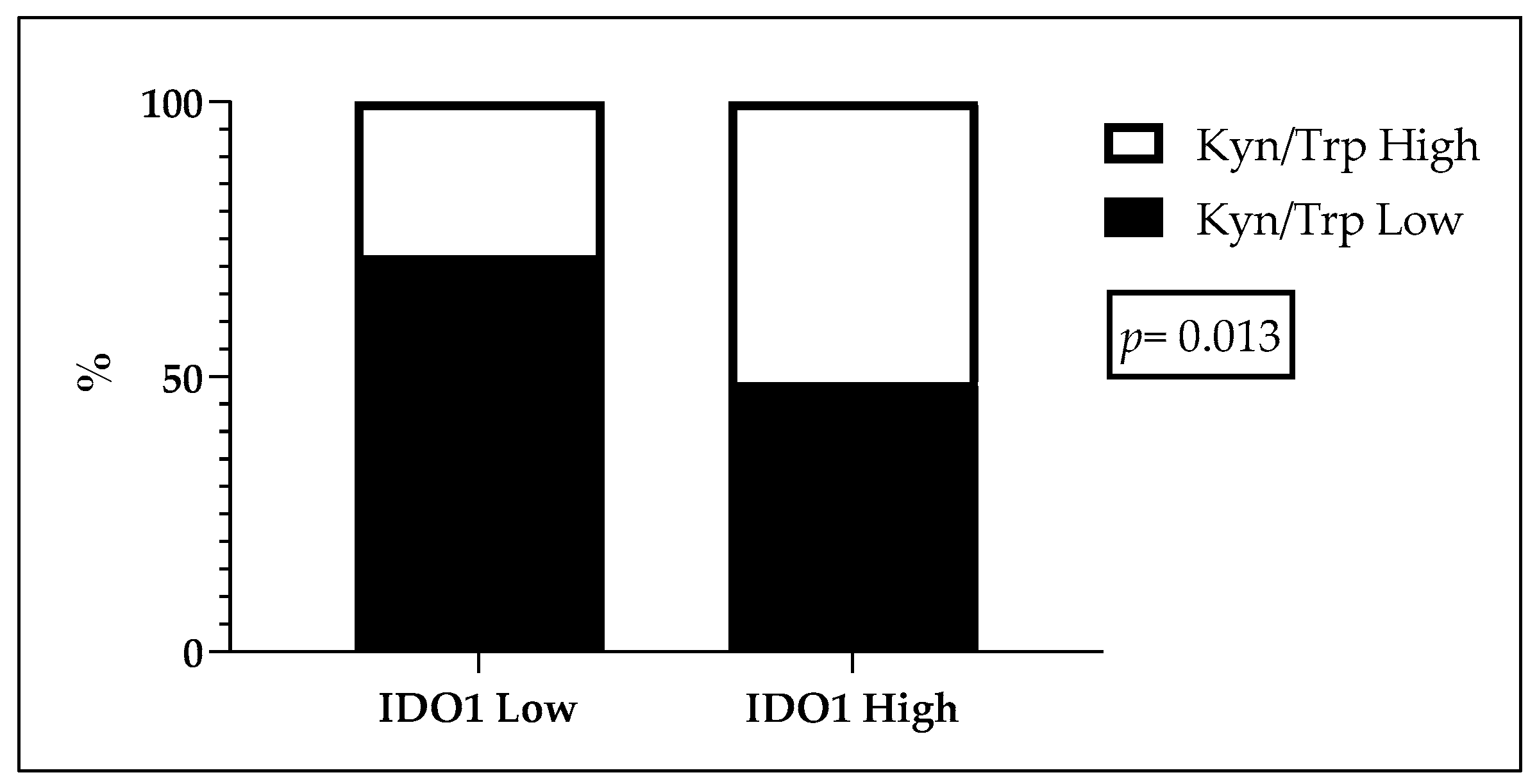
2.7. Kyn/Trp Ratio and Immunohistochemical Associations
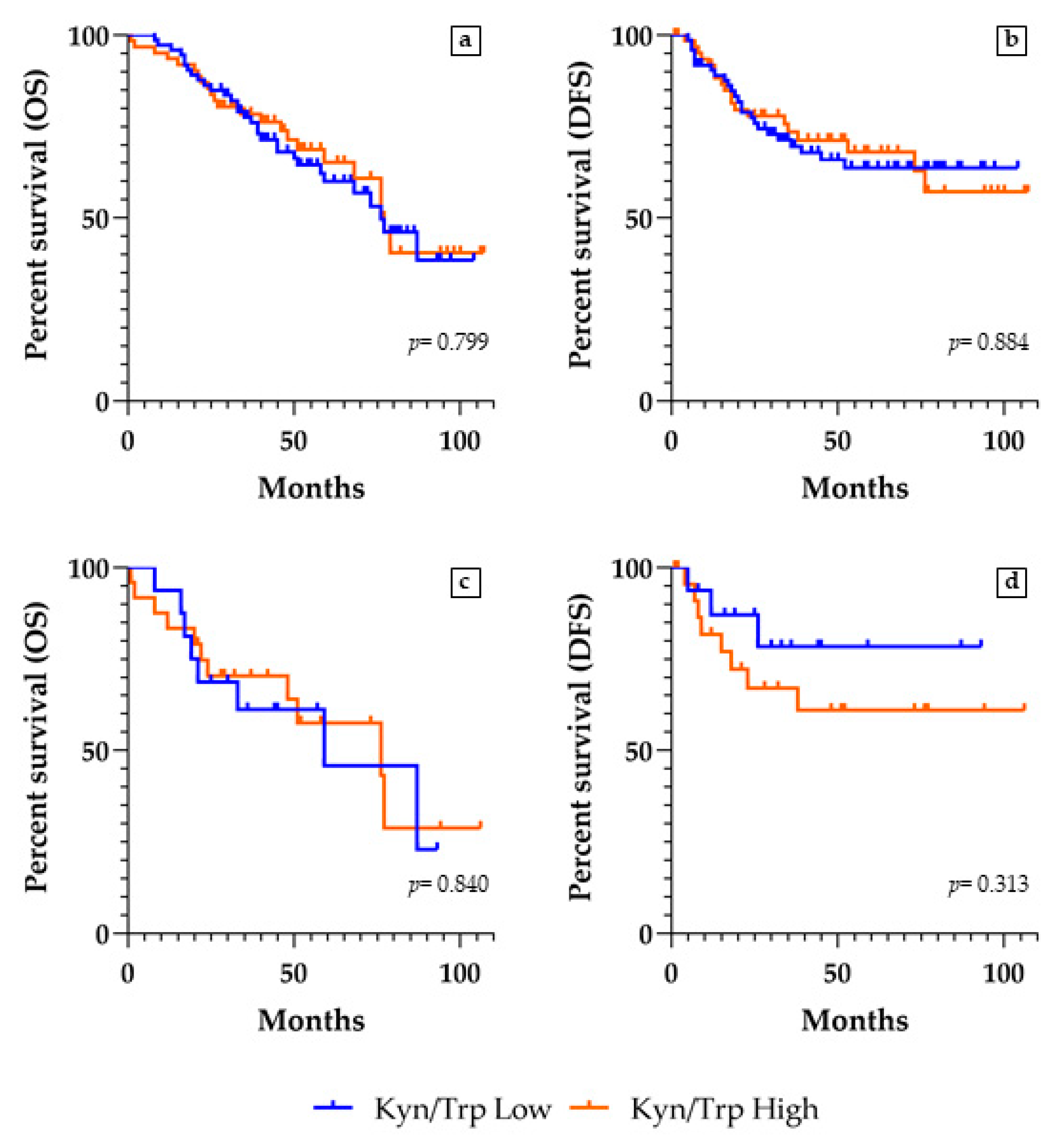
2.8. Kyn/Trp Ratio and Survivals Analyses
3. Discussion
4. Materials and Methods
4.1. Patients’ Recruitment
4.2. Histopathological and Immunohistochemical Determinations
4.3. Determination of Kyn and Trp Serum Concentration
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann. Glob. Health 2019, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. Cronin KA SEER Cancer Statistics Review, 1975–2017; National Cancer Institute: Bethesda, MD, USA, 2020.
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment With Targeted Tyrosine Kinase Inhibitors: Guideline From the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. Arch. Pathol. Lab. Med. 2018, 142, 321–346. [Google Scholar]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef]
- Blackhall, F.; Frese, K.K.; Simpson, K.; Kilgour, E.; Brady, G.; Dive, C. Will liquid biopsies improve outcomes for patients with small-cell lung cancer? Lancet Oncol. 2018, 19, e470–e481. [Google Scholar] [CrossRef]
- Prendergast, G.C. Immune escape as a fundamental trait of cancer: Focus on IDO. Oncogene 2008, 27, 3889–3900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Löb, S.; Königsrainer, A.; Rammensee, H.-G.; Opelz, G.; Terness, P. Inhibitors of indoleamine-2,3-dioxygenase for cancer therapy: Can we see the wood for the trees? Nat. Rev. Cancer 2009, 9, 445–452. [Google Scholar] [CrossRef]
- Munn, D.H.; Mellor, A.L. Indoleamine 2,3 dioxygenase and metabolic control of immune responses. Trends Immunol. 2013, 34, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Meireson, A.; Devos, M.; Brochez, L. IDO Expression in Cancer: Different Compartment, Different Functionality? Front. Immunol. 2020, 11, 531491. [Google Scholar] [CrossRef]
- Huang, J.Y.; Larose, T.L.; Luu, H.N.; Wang, R.; Fanidi, A.; Alcala, K.; Stevens, V.L.; Weinstein, S.J.; Albanes, D.; Caporaso, N.E.; et al. Circulating markers of cellular immune activation in prediagnostic blood sample and lung cancer risk in the Lung Cancer Cohort Consortium (LC3). Int. J. Cancer 2020, 146, 2394–2405. [Google Scholar] [CrossRef]
- Beatty, G.L.; Gladney, W.L. Immune escape mechanisms as a guide for cancer immunotherapy. Clin. Cancer Res. 2015, 21, 687–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timosenko, E.; Hadjinicolaou, A.V.; Cerundolo, V. Modulation of cancer-specific immune responses by amino acid degrading enzymes. Immunotherapy 2017, 9, 83–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallarino, F.; Grohmann, U.; Vacca, C.; Bianchi, R.; Orabona, C.; Spreca, A.; Fioretti, M.C.; Puccetti, P. T cell apoptosis by tryptophan catabolism. Cell Death Differ. 2002, 9, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Zaher, S.S.; Germain, C.; Fu, H.; Larkin, D.F.P.; George, A.J.T. 3-Hydroxykynurenine Suppresses CD4+ T-Cell Proliferation, Induces T-Regulatory-Cell Development, and Prolongs Corneal Allograft Survival. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2640–2648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hornyák, L.; Dobos, N.; Koncz, G.; Karányi, Z.; Páll, D.; Szabó, Z.; Halmos, G.; Székvölgyi, L. The Role of Indoleamine-2,3-Dioxygenase in Cancer Development, Diagnostics, and Therapy. Front. Immunol. 2018, 9, 151. [Google Scholar] [CrossRef]
- Yu, C.P.; Fu, S.F.; Chen, X.; Ye, J.; Ye, Y.; Kong, L.D.; Zhu, Z. The Clinicopathological and Prognostic Significance of IDO1 Expression in Human Solid Tumors: Evidence from a Systematic Review and Meta-Analysis. Cell Physiol. Biochem. 2018, 49, 134–143. [Google Scholar] [CrossRef]
- Lee, S.H.; Mahendran, R.; Tham, S.M.; Thamboo, T.P.; Chionh, B.J.; Lim, Y.X.; Tsang, W.C.; Wu, Q.H.; Chia, J.Y.; Tay, M.H.W.; et al. Tryptophan-kynurenine ratio as a biomarker of bladder cancer. BJU Int. 2021, 127, 445–453. [Google Scholar] [CrossRef]
- Li, H.; Bullock, K.; Gurjao, C.; Braun, D.; Shukla, S.A.; Bossé, D.; Lalani, A.A.; Gopal, S.; Jin, C.; Horak, C.; et al. Metabolomic adaptations and correlates of survival to immune checkpoint blockade. Nat. Commun. 2019, 10, 4346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, L.; Dey, M.; Lauing, K.L.; Gritsina, G.; Kaur, R.; Lukas, R.V.; Nicholas, M.K.; Rademaker, A.W.; Dostal, C.R.; McCusker, R.H.; et al. The kynurenine to tryptophan ratio as a prognostic tool for glioblastoma patients enrolling in immunotherapy. J. Clin. Neurosci. 2015, 22, 1964–1968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botticelli, A.; Mezi, S.; Pomati, G.; Cerbelli, B.; Cerbelli, E.; Roberto, M.; Giusti, R.; Cortellini, A.; Lionetto, L.; Scagnoli, S.; et al. Tryptophan Catabolism as Immune Mechanism of Primary Resistance to Anti-PD-1. Front. Immunol. 2020, 11, 1243. [Google Scholar] [CrossRef] [PubMed]
- Mandarano, M.; Bellezza, G.; Belladonna, M.L.; Van den Eynde, B.J.; Chiari, R.; Vannucci, J.; Mondanelli, G.; Ludovini, V.; Ferri, I.; Bianconi, F.; et al. Assessment of TILs, IDO-1, and PD-L1 in resected non-small cell lung cancer: An immunohistochemical study with clinicopathological and prognostic implications. Virchows Arch. 2019, 474, 159–168. [Google Scholar] [CrossRef]
- Ala, M. The footprint of kynurenine pathway in every cancer: A new target for chemotherapy. Eur. J. Pharmacol. 2021, 896, 173921. [Google Scholar] [CrossRef] [PubMed]
- Brochez, L.; Chevolet, I.; Kruse, V. The rationale of indoleamine 2,3-dioxygenase inhibition for cancer therapy. Eur. J. Cancer 2017, 76, 167–182. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Liang, H.; Fang, X.; Zhang, S.; Xing, Z.; Shi, L.; Kuang, C.; Seliger, B.; Yang, Q. What is the prospect of indoleamine 2,3-dioxygenase 1 inhibition in cancer? Extrapolation from the past. J. Exp. Clin. Cancer Res. 2021, 40, 60. [Google Scholar] [CrossRef] [PubMed]
- Beatty, G.L.; O’Dwyer, P.J.; Clark, J.; Shi, J.G.; Bowman, K.J.; Scherle, P.A.; Newton, R.C.; Schaub, R.; Maleski, J.; Leopold, L.; et al. First-in-Human Phase I Study of the Oral Inhibitor of Indoleamine 2,3-Dioxygenase-1 Epacadostat (INCB024360) in Patients with Advanced Solid Malignancies. Clin. Cancer Res. 2017, 23, 3269–3276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, Y.; Suda, T.; Furuhashi, K.; Suzuki, M.; Fujie, M.; Hahimoto, D.; Nakamura, Y.; Inui, N.; Nakamura, H.; Chida, K. Increased serum kynurenine/tryptophan ratio correlates with disease progression in lung cancer. Lung Cancer 2010, 67, 361–365. [Google Scholar] [CrossRef]
- Weinlich, G.; Murr, C.; Richardsen, L.; Winkler, C.; Fuchs, D. Decreased serum tryptophan concentration predicts poor prognosis in malignant melanoma patients. Dermatology 2007, 214, 8–14. [Google Scholar] [CrossRef]
- de Jong, R.A.; Nijman, H.W.; Boezen, H.M.; Volmer, M.; Ten Hoor, K.A.; Krijnen, J.; van der Zee, A.G.; Hollema, H.; Kema, I.P. Serum tryptophan and kynurenine concentrations as parameters for indoleamine 2,3-dioxygenase activity in patients with endometrial, ovarian, and vulvar cancer. Int. J. Gynecol. Cancer 2011, 21, 1320–1327. [Google Scholar] [CrossRef]
- Sorgdrager, F.J.H.; Naudé, P.J.W.; Kema, I.P.; Nollen, E.A.; Deyn, P.P. Tryptophan Metabolism in Inflammaging: From Biomarker to Therapeutic Target. Front. Immunol. 2019, 10, 2565. [Google Scholar] [CrossRef]
- Bürkle, A.; Moreno-Villanueva, M.; Bernhard, J.; Blasco, M.; Zondag, G.; Hoeijmakers, J.H.; Toussaint, O.; Grubeck-Loebenstein, B.; Mocchegiani, E.; Collino, S.; et al. MARK-AGE biomarkers of ageing. Mech. Ageing Dev. 2015, 151, 2–12. [Google Scholar] [CrossRef]
- Pertovaara, M.; Heliövaara, M.; Raitala, A.; Oja, S.S.; Knekt, P.; Hurme, M. The activity of the immunoregulatory enzyme indoleamine 2,3-dioxygenase is decreased in smokers. Clin. Exp. Immunol. 2006, 145, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Osoegawa, A.; Hiraishi, H.; Hashimoto, T.; Takumi, Y.; Abe, M.; Takeuchi, H.; Miyawaki, M.; Okamoto, T.; Sugio, K. The Positive Relationship Between γH2AX and PD-L1 Expression in Lung Squamous Cell Carcinoma. In Vivo 2018, 32, 171–177. [Google Scholar]
- Platten, M.; Wick, W.; Van den Eynde, B.J. Tryptophan catabolism in cancer: Beyond IDO and tryptophan depletion. Cancer Res. 2012, 72, 5435–5440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferns, D.M.; Kema, I.P.; Buist, M.R.; Nijman, H.W.; Kenter, G.G.; Jordanova, E.S. Indoleamine-2,3-dioxygenase (IDO) metabolic activity is detrimental for cervical cancer patient survival. Oncoimmunology 2015, 4, e981457. [Google Scholar] [CrossRef]
- Lenzen, A.; Zhai, L.; Lauing, K.L.; Gritsina, G.; Ladomersky, E.; Genet, M.; James, C.D.; Bloch, O.; Wainwright, D.A. The Kynurenine/Tryptophan Ratio and Glioblastoma Patients Treated with Hsppc-96 Vaccine. Immunotherapy 2016, 2, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Hu, G.F.; Wang, Z.H. The status of immunosuppression in patients with stage IIIB or IV non-small-cell lung cancer correlates with the clinical characteristics and response to chemotherapy. OncoTargets Ther. 2017, 10, 3557–3566. [Google Scholar] [CrossRef] [Green Version]
- Pradhan, M.; Chocry, M.; Gibbons, D.L.; Sepesi, B.; Cascone, T. Emerging biomarkers for neoadjuvant immune checkpoint inhibitors in operable non-small cell lung cancer. Transl. Lung Cancer Res. 2021, 10, 590–606. [Google Scholar] [CrossRef]
- Rocco, D.; Gravara, L.D.; Gridelli, C. The New Immunotherapy Combinations in the Treatment of Advanced Non-Small Cell Lung Cancer: Reality and Perspectives. Curr. Clin. Pharmacol. 2020, 15, 11–19. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Gettinger, S.; Chow, L.Q.M.; Gordon, M.; Awad, M.M.; Cha, E.; Gong, X.; Zhou, G.; Walker, C.; Leopold, L.; et al. Phase 1 study of epacadostat in combination with atezolizumab for patients with previously treated advanced nonsmall cell lung cancer. Int. J. Cancer 2020, 147, 1963–1969. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.H.; LoRusso, P.; Burris, H.; Gordon, M.; Bang, Y.J.; Hellmann, M.D.; Cervantes, A.; de Olza, M.O.; Marabelle, A.; Hodi, F.S.; et al. Phase I Study of the Indoleamine 2,3-Dioxygenase 1 (IDO1) Inhibitor Navoximod (GDC-0919) Administered with PD-L1 Inhibitor (Atezolizumab) in Advanced Solid Tumors. Clin. Cancer Res. 2019, 25, 3220–3228. [Google Scholar] [CrossRef] [Green Version]
- Murakami, S.; Shibaki, R.; Matsumoto, Y.; Yoshida, T.; Goto, Y.; Kanda, S.; Horinouchi, H.; Fujiwara, Y.; Yamamoto, N.; Ohe, Y. Association between serum level soluble programmed cell death ligand 1 and prognosis in patients with non-small cell lung cancer treated with anti-PD-1 antibody. Thorac. Cancer 2020, 11, 3585–3595. [Google Scholar] [CrossRef] [PubMed]
- Mildner, F.; Sopper, S.; Amann, A.; Pircher, A.; Pall, G.; Köck, S.; Naismith, E.; Wolf, D.; Gamerith, G. Systematic review: Soluble immunological biomarkers in advanced non-small-cell lung cancer (NSCLC). Crit. Rev. Oncol. Hematol. 2020, 153, 102948. [Google Scholar] [CrossRef] [PubMed]
- Théate, I.; van Baren, N.; Pilotte, L.; Moulin, P.; Larrieu, P.; Renauld, J.C.; Hervé, C.; Gutierrez-Roelens, I.; Marbaix, E.; Sempoux, C.; et al. Extensive profiling of the expression of the indoleamine 2,3-dioxygenase 1 protein in normal and tumoral human tissues. Cancer Immunol. Res. 2015, 3, 161–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Kyn/Trp Low | Kyn/Trp High | p Value | Total | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| 93 | 52 | 87 | 48 | 180 | 100 | ||
| Gender | |||||||
| Male | 62 | 49 | 65 | 51 | 0.237 | 127 | 71 |
| Female | 31 | 58 | 22 | 42 | 53 | 29 | |
| Age | |||||||
| <68 years | 54 | 66 | 28 | 34 | <0.001 | 82 | 46 |
| ≥68 years | 39 | 40 | 59 | 60 | 98 | 54 | |
| Smokers | |||||||
| Current | 38 | 57 | 37 | 49 | 0.042 | 75 | 42 |
| Former | 42 | 47 | 47 | 53 | 89 | 49 | |
| Never | 13 | 81 | 3 | 19 | 16 | 9 | |
| Parameter | Kyn/Trp Low | Kyn/Trp High | p Value | Total | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| 93 | 52 | 87 | 48 | 180 | 100 | ||
| Histotype | |||||||
| Adc 1 | 70 | 59 | 48 | 41 | 0.004 | 118 | 66 |
| Sqcc 2 | 23 | 37 | 39 | 63 | 62 | 34 | |
| Stage | |||||||
| I | 58 | 59 | 41 | 41 | 0.040 | 99 | 55 |
| II–III | 35 | 43 | 46 | 57 | 81 | 45 | |
| Adc 1 stage | 118 | 100 | |||||
| I | 52 | 71 | 21 | 29 | <0.001 | 73 | 62 |
| II–III | 18 | 40 | 27 | 60 | 45 | 38 | |
| Sqcc 2 stage | 62 | 100 | |||||
| I | 6 | 23 | 20 | 77 | 0.066 | 26 | 42 |
| II–III | 17 | 47 | 19 | 53 | 36 | 58 | |
| TILs Density | |||||||
| Low | 50 | 56 | 40 | 44 | 0.296 | 90 | 50 |
| High | 43 | 48 | 47 | 52 | 90 | 50 | |
| Adc 1 | 118 | 100 | |||||
| Low | 35 | 58 | 25 | 42 | 0.824 | 60 | 51 |
| High | 35 | 60 | 23 | 40 | 58 | 49 | |
| Sqcc 2 | 62 | 100 | |||||
| Low | 15 | 50 | 15 | 50 | 0.042 | 30 | 48 |
| High | 8 | 25 | 24 | 75 | 32 | 52 | |
| TILs Localization | |||||||
| Intratumoral | 45 | 54 | 58 | 46 | 0.418 | 83 | 46 |
| Peritumoral | 4 | 31 | 9 | 69 | 13 | 7 | |
| Mixed | 42 | 53 | 37 | 47 | 79 | 44 | |
| Absent | 2 | 40 | 3 | 60 | 5 | 3 | |
| Adc 1 | 118 | 100 | |||||
| Intratumoral | 37 | 59 | 26 | 41 | 0.446 | 63 | 53 |
| Peritumoral | 3 | 50 | 3 | 50 | 6 | 5 | |
| Mixed | 29 | 64 | 16 | 36 | 45 | 38 | |
| Absent | 1 | 25 | 3 | 75 | 4 | 4 | |
| Sqcc 2 | 62 | 100 | |||||
| Intratumoral | 8 | 40 | 12 | 60 | 0.341 | 20 | 32 |
| Peritumoral | 1 | 14 | 6 | 86 | 7 | 11 | |
| Mixed | 18 | 38 | 21 | 62 | 34 | 55 | |
| Absent | 1 | 100 | 0 | 0 | 1 | 2 | |
| Parameter | Kyn/Trp Low | Kyn/Trp High | p Value | Total | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| 93 | 52 | 87 | 48 | 180 | 100 | ||
| IDO1 | |||||||
| Low | 47 | 59 | 32 | 41 | 0.063 | 79 | 44 |
| High | 46 | 46 | 55 | 54 | 101 | 56 | |
| Adc 1 | 118 | 100 | |||||
| Low | 38 | 72 | 15 | 28 | 0.013 | 53 | 45 |
| High | 32 | 49 | 33 | 51 | 65 | 55 | |
| Sqcc 2 | 62 | 100 | |||||
| Low | 9 | 35 | 17 | 65 | 0.731 | 26 | 42 |
| High | 14 | 39 | 22 | 61 | 36 | 58 | |
| PD-L1 | |||||||
| Low | 73 | 53 | 66 | 47 | 0.674 | 139 | 77 |
| High | 20 | 49 | 21 | 51 | 41 | 23 | |
| Adc 1 | 118 | 100 | |||||
| Low | 60 | 62 | 37 | 38 | 0.229 | 97 | 82 |
| High | 10 | 48 | 11 | 52 | 21 | 18 | |
| Sqcc 2 | 62 | 100 | |||||
| Low | 13 | 31 | 29 | 69 | 0.147 | 42 | 68 |
| High | 10 | 50 | 10 | 50 | 20 | 32 | |
| Kyn/Trp | Exitus (%) | p Value | HR 1 (95% CI 2) | Relapse (%) | p Value | HR 1 (95% CI 2) | ||
|---|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | |||||
| NSCLCs | ||||||||
| Low | 39(51) | 54(52) | 0.941 | 1.02 (0.65–1.60) | 36(52) | 57(51) | 0.967 | 0.99 (0.62–1.59) |
| High | 37(49) | 50(48) | 33(48) | 5(49) | ||||
| Adenocarcinomas | ||||||||
| Low | 30(60) | 40(59) | 0.595 | 1.16 (0.65–2.07) | 31(58) | 39(60) | 0.701 | 1.11 (0.64–1.93) |
| High | 20(40) | 28(41) | 22(42) | 26(40) | ||||
| Squamous cell carcinomas | ||||||||
| Low | 9(35) | 14(39) | 0.837 | 0.92 (0.41–2.09) | 5(31) | 18(39) | 0.759 | 1.18 (0.42–3.29) |
| High | 17(65) | 22(61) | 11(69) | 28(61) | ||||
| Stage II–III | ||||||||
| Low | 16(41) | 19(45) | 0.873 | 1.05 (0.56–1.99) | 15(43) | 20(43) | 0.887 | 1.05 (0.54–2.05) |
| High | 23(59) | 23(55) | 20(57) | 26(57) | ||||
| Kyn/Trp | Exitus (%) | p Value | HR 1 (95% CI 2) | Relapse (%) | p Value | HR 1 (95% CI 2) | ||
|---|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | |||||
| NSCLCs | ||||||||
| Low | 31(57) | 42(52) | 0.799 | 0.93 (0.55–1.60) | 24(56) | 49(53) | 0.884 | 0.96 (0.52–1.74) |
| High | 23(43) | 39(48) | 19(44) | 43(47) | ||||
| Adenocarcinomas | ||||||||
| Low | 25(69) | 35(60) | 0.905 | 0.96 (0.47–1.94) | 23(64) | 37(64) | 0.859 | 1.06 (0.53–2.11) |
| High | 11(31) | 23(40) | 13(36) | 21(36) | ||||
| Squamous cell carcinomas | ||||||||
| Low | 6(33) | 7(30) | 0.657 | 0.80 (0.29–2.23) | 1(14) | 12(35) | 0.398 | 2.41 (0.47–12.39) |
| High | 12(66) | 16(70) | 6(86) | 22(65) | ||||
| Stage II–III | ||||||||
| Low | 8(43) | 8(38) | 0.840 | 0.91 (0.36–2.28) | 3(27) | 13(45) | 0.313 | 1.95 (0.59–6.46) |
| High | 11(58) | 13(62) | 8(73) | 16(55) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mandarano, M.; Orecchini, E.; Bellezza, G.; Vannucci, J.; Ludovini, V.; Baglivo, S.; Tofanetti, F.R.; Chiari, R.; Loreti, E.; Puma, F.; et al. Kynurenine/Tryptophan Ratio as a Potential Blood-Based Biomarker in Non-Small Cell Lung Cancer. Int. J. Mol. Sci. 2021, 22, 4403. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094403
Mandarano M, Orecchini E, Bellezza G, Vannucci J, Ludovini V, Baglivo S, Tofanetti FR, Chiari R, Loreti E, Puma F, et al. Kynurenine/Tryptophan Ratio as a Potential Blood-Based Biomarker in Non-Small Cell Lung Cancer. International Journal of Molecular Sciences. 2021; 22(9):4403. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094403
Chicago/Turabian StyleMandarano, Martina, Elena Orecchini, Guido Bellezza, Jacopo Vannucci, Vienna Ludovini, Sara Baglivo, Francesca Romana Tofanetti, Rita Chiari, Elisabetta Loreti, Francesco Puma, and et al. 2021. "Kynurenine/Tryptophan Ratio as a Potential Blood-Based Biomarker in Non-Small Cell Lung Cancer" International Journal of Molecular Sciences 22, no. 9: 4403. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094403