
Tumor-Specific Immunoenhancing Effects after Local Cryoablation for Metastatic Bone Tumor in a Mouse Model

 , , ,
, , ,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
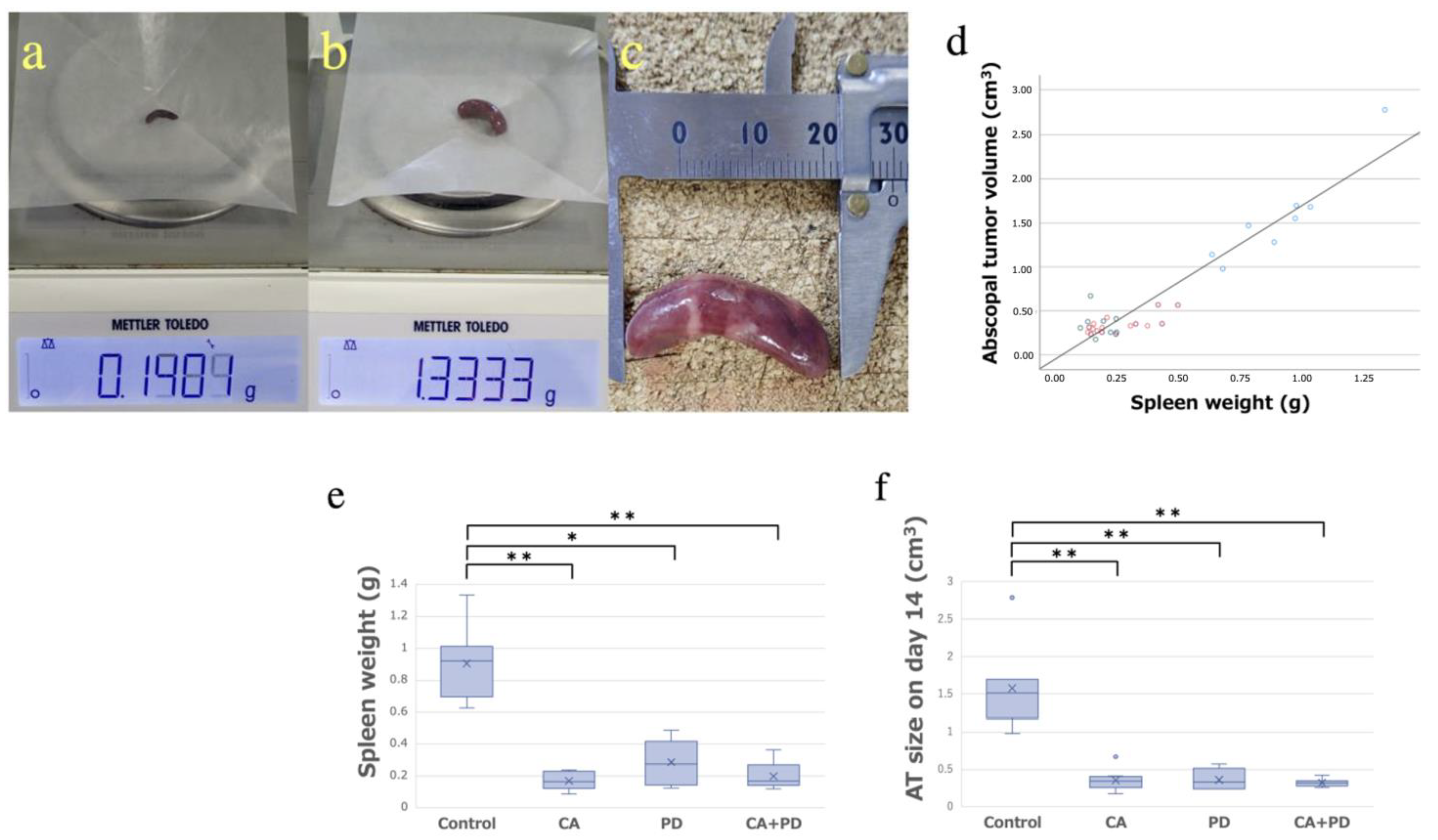
2.1. Abscopal Tumor Growth
2.2. Spleen Weight
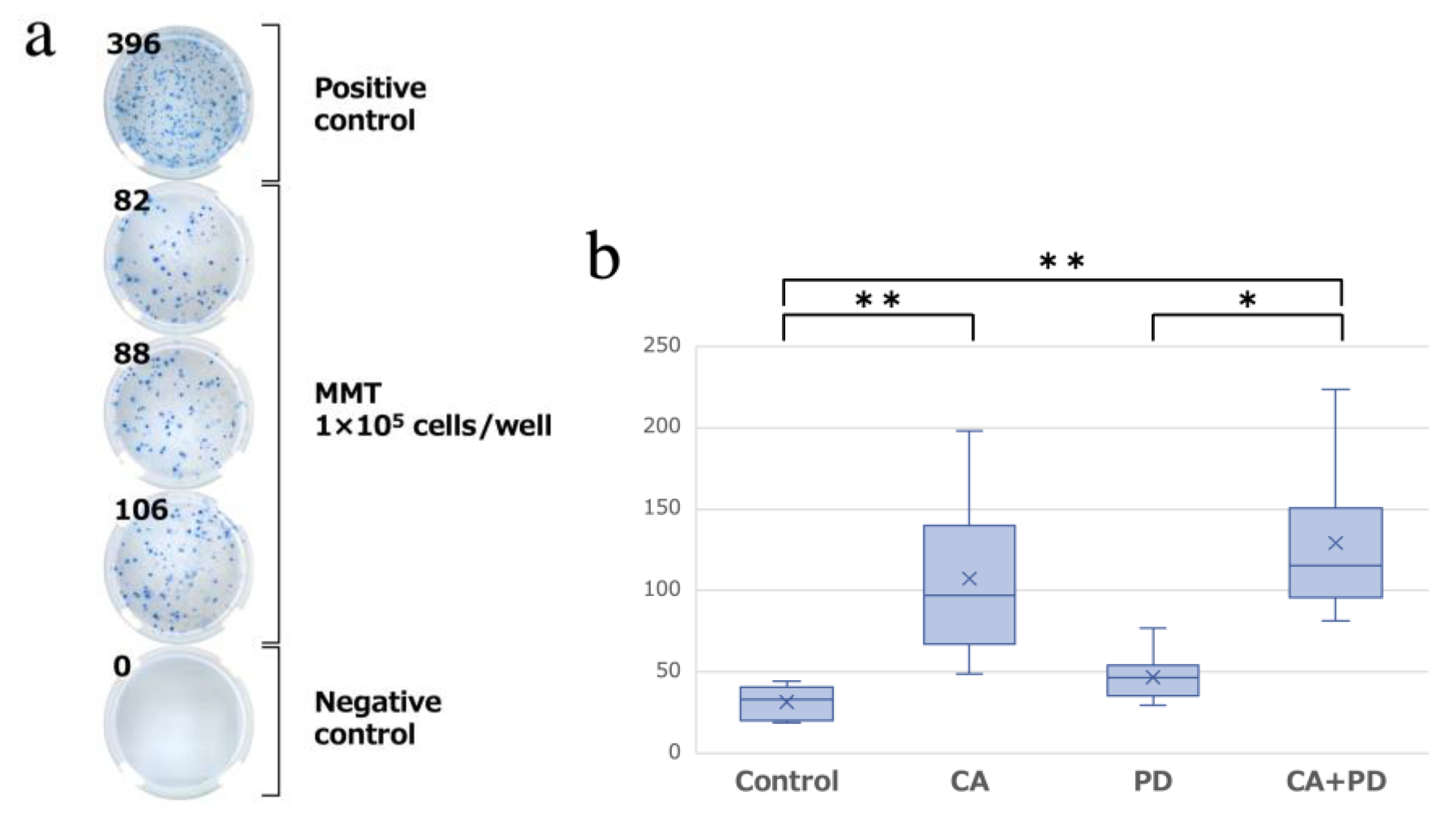
2.3. Enzyme-Linked Immunospot (ELISPOT) Assay
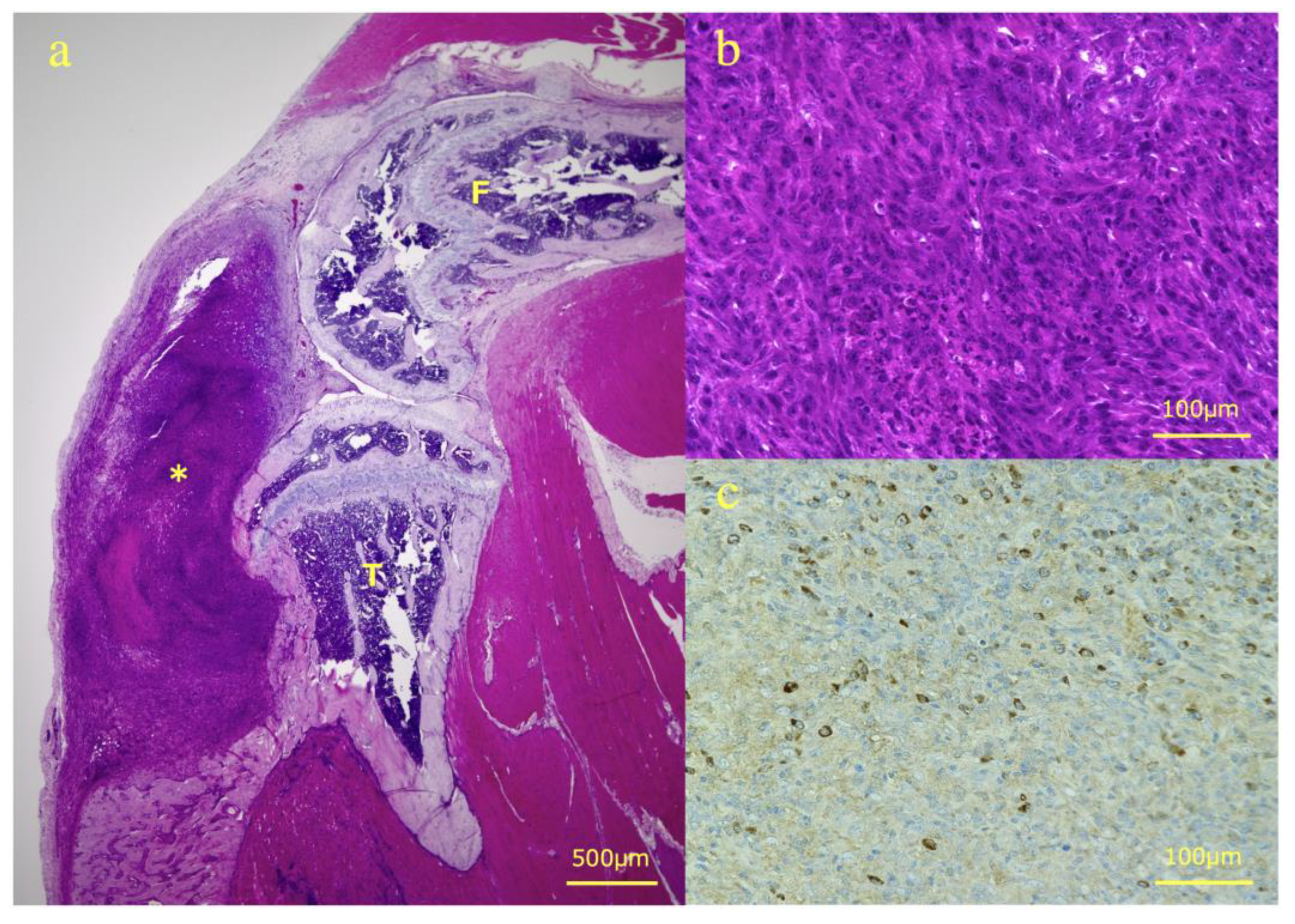
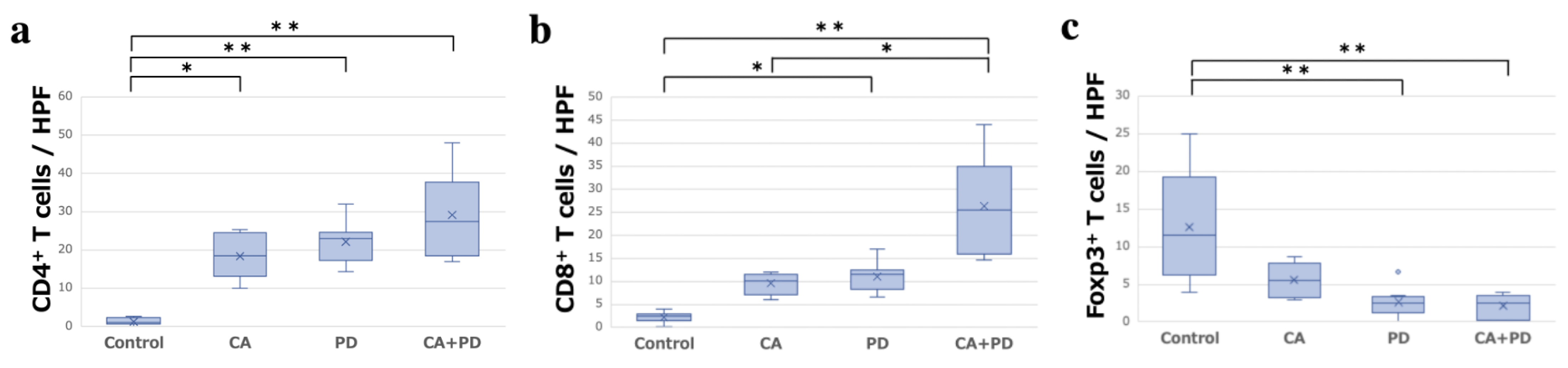
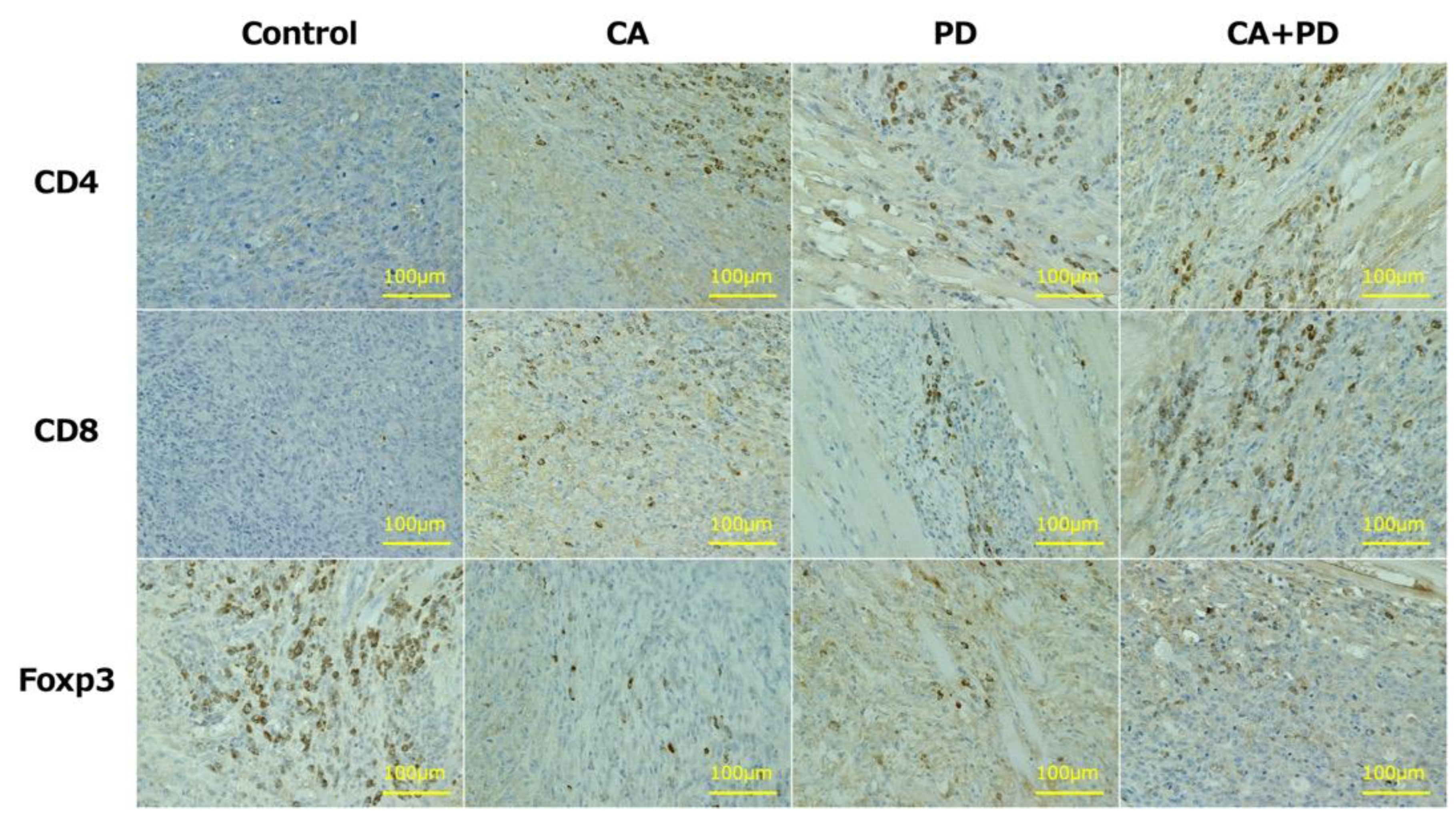
2.4. Immunohistochemistry
3. Discussion
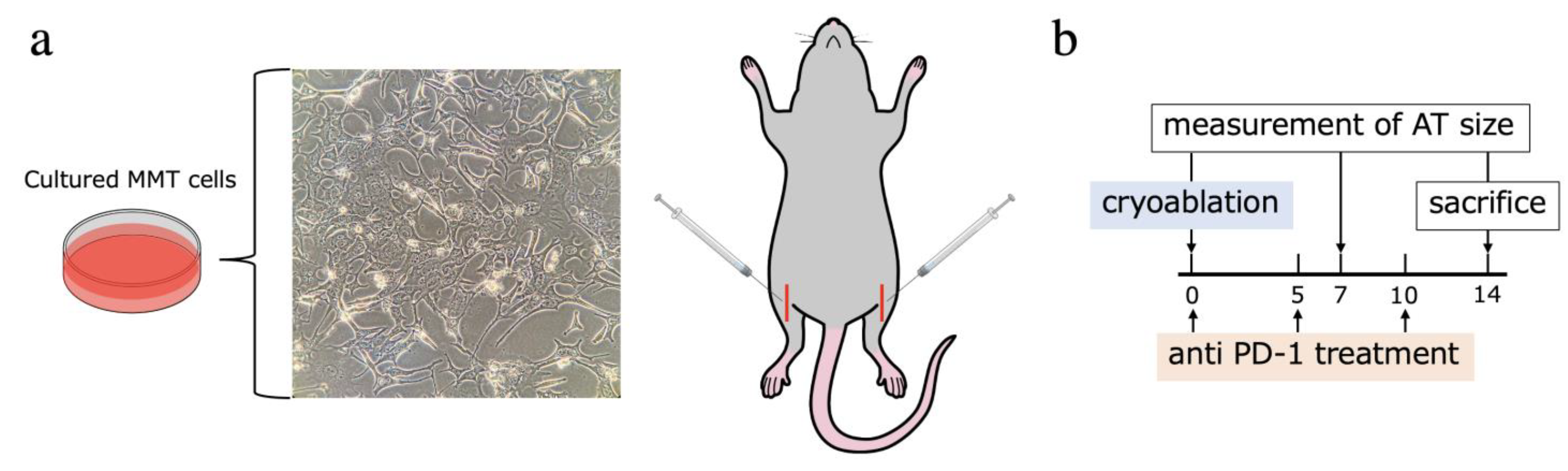
4. Materials and Methods
4.1. Animals
4.2. Tumors
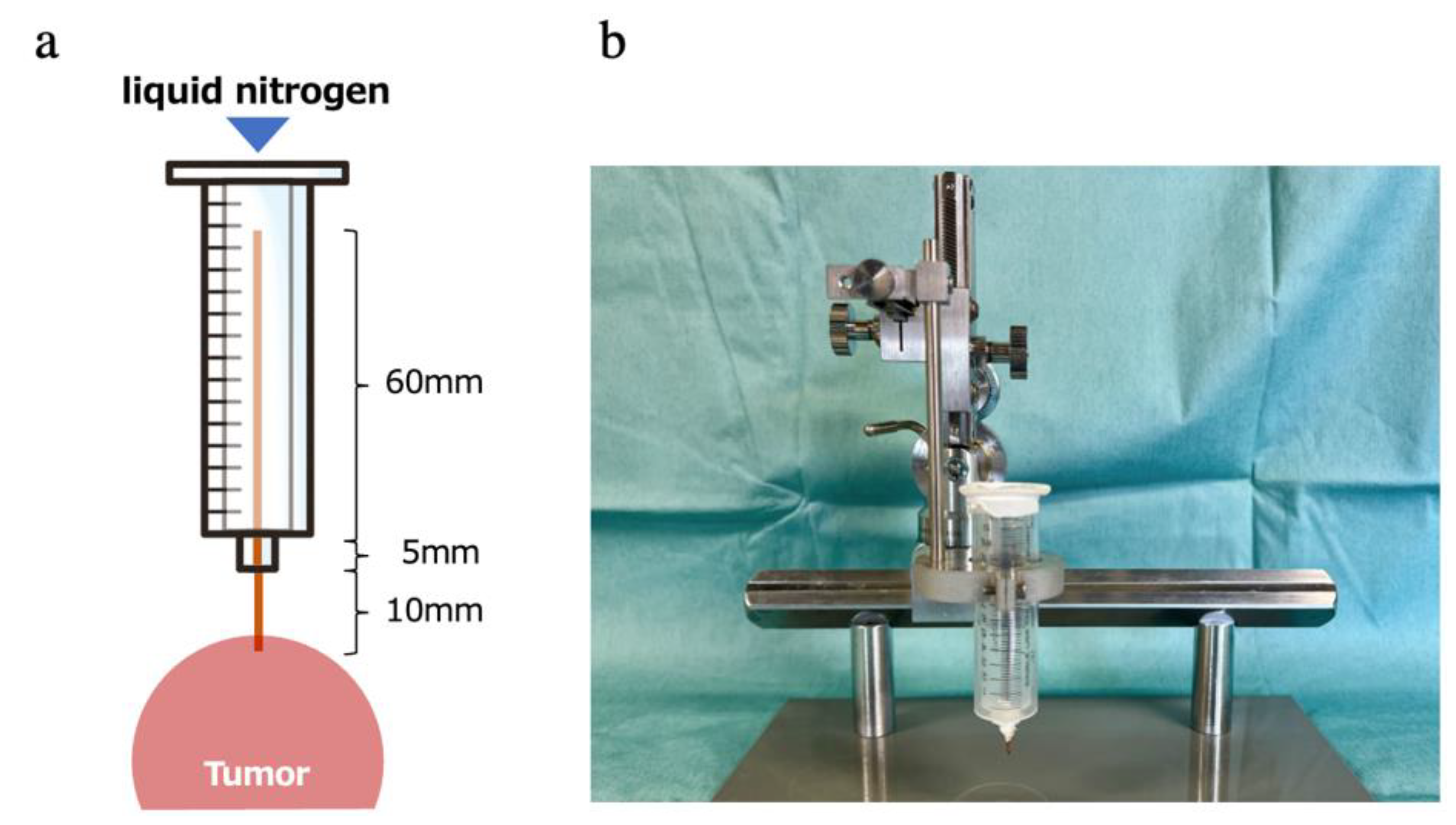
4.3. Freezing Device
4.4. Procedure
4.5. Immune Checkpoint Inhibitor for Adjuvant Treatment
4.6. Evaluation of the Spleen Weight
4.7. Tumor-Specific IFN-γ ELISPOT Assay
4.8. Evaluation of the Infiltration Intensity of Immune-Related Cells in the ATs
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aaron, A.D. The management of cancer metastatic to bone. JAMA 1994, 272, 1206–1209. [Google Scholar] [CrossRef] [PubMed]
- Desforges, J.F.; Byrne, T.N. Spinal Cord Compression from Epidural Metastases. N. Engl. J. Med. 1992, 327, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Bilsky, M.H.; Lis, E.; Raizer, J.; Lee, H.; Boland, P. The Diagnosis and Treatment of Metastatic Spinal Tumor. Oncologist 1999, 4, 459–469. [Google Scholar] [CrossRef] [Green Version]
- Orcutt, F.V. Surgical management of spinal metastases. West. J. Med. 1993, 159, 483–484. [Google Scholar] [PubMed]
- Cetin, K.; Christiansen, C.F.; Jacobsen, J.B.; Nørgaard, M.; Sørensen, H.T. Bone metastasis, skeletal-related events, and mortality in lung cancer patients: A Danish population-based cohort study. Lung Cancer 2014, 86, 247–254. [Google Scholar] [CrossRef]
- Farooki, A.; Leung, V.; Tala, H.; Tuttle, R.M. Skeletal-Related Events due to Bone Metastases from Differentiated Thyroid Cancer. J. Clin. Endocrinol. Metab. 2012, 97, 2433–2439. [Google Scholar] [CrossRef]
- Mole, R.H. Whole Body Irradiation—Radiobiology or Medicine? Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef]
- Aarts, B.M.; Klompenhouwer, E.G.; Rice, S.L.; Imani, F.; Baetens, T.; Bex, A.; Horenblas, S.; Kok, M.; Haanen, J.B.A.G.; Beets-Tan, R.G.H.; et al. Cryoablation and immunotherapy: An overview of evidence on its synergy. Insights Imaging 2019, 10, 53. [Google Scholar] [CrossRef]
- Craig, D.J.; Nanavaty, N.S.; Devanaboyina, M.; Stanbery, L.; Hamouda, D.; Edelman, G.; Dworkin, L.; Nemunaitis, J.J. The abscopal effect of radiation therapy. Futur. Oncol. 2021, 17, 1683–1694. [Google Scholar] [CrossRef]
- Mizukoshi, E.; Nakamoto, Y.; Arai, K.; Yamashita, T.; Mukaida, N.; Matsushima, K.; Matsui, O.; Kaneko, S. Enhancement of tumor-specific T-cell responses by transcatheter arterial embolization with dendritic cell infusion for hepatocellular carcinoma. Int. J. Cancer 2010, 126, 2164–2174. [Google Scholar] [CrossRef]
- Takaki, H.; Cornelis, F.; Kako, Y.; Kobayashi, K.; Kamikonya, N.; Yamakado, K. Thermal ablation and immunomodulation: From preclinical experiments to clinical trials. Diagn. Interv. Imaging 2017, 98, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Yakkala, C.; Chiang, C.L.-L.; Kandalaft, L.; Denys, A.; Duran, R. Cryoablation and Immunotherapy: An Enthralling Synergy to Confront the Tumors. Front. Immunol. 2019, 10, 2283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yonezawa, N.; Murakami, H.; Demura, S.; Kato, S.; Miwa, S.; Yoshioka, K.; Shinmura, K.; Yokogawa, N.; Shimizu, T.; Oku, N.; et al. Abscopal Effect of Frozen Autograft Reconstruction Combined with an Immune Checkpoint Inhibitor Analyzed Using a Metastatic Bone Tumor Model. Int. J. Mol. Sci. 2021, 22, 1973. [Google Scholar] [CrossRef] [PubMed]
- Caviezel, A.; Terraz, S.; Schmidlin, F.; Becker, C.; Iselin, C.E. Percutaneous cryoablation of small kidney tumours under magnetic resonance imaging guidance: Medium-term follow-up. Scand. J. Urol. Nephrol. 2008, 42, 412–416. [Google Scholar] [CrossRef]
- Baust, J.G.; Bischof, J.C.; Jiang-Hughes, S.; Polascik, T.J.; Rukstalis, D.B.; A Gage, A. Re-purposing cryoablation: A combinatorial ‘therapy’ for the destruction of tissue. Prostate Cancer Prostatic Dis. 2015, 18, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Kurup, A.N.; Morris, J.M.; Boon, A.J.; Strommen, J.A.; Schmit, G.D.; Atwell, T.D.; Carter, R.E.; Brown, M.J.; Wass, C.T.; Rose, P.S.; et al. Motor Evoked Potential Monitoring during Cryoablation of Musculoskeletal Tumors. J. Vasc. Interv. Radiol. 2014, 25, 1657–1664. [Google Scholar] [CrossRef]
- Hegg, R.M.; Kurup, A.N.; Schmit, G.D.; Weisbrod, A.J.; Atwell, T.D.; Olivier, K.R.; Moynihan, T.J.; Callstrom, M.R. Cryoablation of Sternal Metastases for Pain Palliation and Local Tumor Control. J. Vasc. Interv. Radiol. 2014, 25, 1665–1670. [Google Scholar] [CrossRef]
- Yasmin-Karim, S.; Ziberi, B.; Wirtz, J.; Bih, N.; Moreau, M.; Guthier, R.; Ainsworth, V.; Hesser, J.; Makrigiorgos, G.M.; Chuong, M.D.; et al. Boosting the Abscopal Effect Using Immunogenic Biomaterials with Varying Radiation Therapy Field Sizes. Int. J. Radiat. Oncol. 2021, 112, 475–486. [Google Scholar] [CrossRef]
- Hodgson, A.; Wier, E.M.; Fu, K.; Sun, X.; Wan, F. Ultrasound imaging of splenomegaly as a proxy to monitor colon tumor development in Apc min716/+ mice. Cancer Med. 2016, 5, 2469–2476. [Google Scholar] [CrossRef]
- Dolff, S.; Quandt, D.; Feldkamp, T.; Jun, C.; Mitchell, A.; Hua, F.; Specker, C.; Kribben, A.; Witzke, O.; Wilde, B. Increased percentages of PD-1 on CD4+T cells is associated with higher INF-γ production and altered IL-17 production in patients with systemic lupus erythematosus. Scand. J. Rheumatol. 2014, 43, 307–313. [Google Scholar] [CrossRef]
- Sabel, M.S. Cryo-immunology: A review of the literature and proposed mechanisms for stimulatory versus suppressive immune responses. Cryobiology 2009, 58, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.; Nielsen, T.K.; Lagerveld, B.; Garnon, J.; Breen, D.; King, A.; van Strijen, M.; Keeley, F.X. Renal cryoablation: Multidisciplinary, collaborative and perspective approach. Cryobiology 2018, 83, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Ablin, R.; Soanes, W.; Gonder, M. Prospects for cryo-immunotherapy in cases of metastasizing carcinoma of the prostate. Cryobiology 1971, 8, 271–279. [Google Scholar] [CrossRef]
- Soanes, W.A.; Ablin, R.; Gonder, M.J. Remission of Metastatic Lesions Following Cryosurgery in Prostatic Cancer: Immunologic Considerations. J. Urol. 1970, 104, 154–159. [Google Scholar] [CrossRef]
- Tanaka, S. Immunological aspects of cryosurgery in general surgery. Cryobiology 1982, 19, 247–262. [Google Scholar] [CrossRef]
- Kurachi, M. CD8+ T cell exhaustion. Semin. Immunopathol. 2019, 41, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Read, K.A.; Powell, M.D.; Sreekumar, B.K.; Oestreich, K.J. In Vitro Differentiation of Effector CD4+ T Helper Cell Subsets. In Methods in Molecular Biology; Humana Press: New York, NY, USA, 2019; Volume 1960, pp. 75–84. [Google Scholar]
- Choi, J.; Meilleur, C.E.; Haeryfar, S.M. Tailoring In Vivo Cytotoxicity Assays to Study Immunodominance in Tumor-specific CD8+ T Cell Responses. J. Vis. Exp. 2019, 2019, e59531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valdman, A.; Jaraj, S.J.; Compérat, E.; Charlotte, F.; Rouprêt, M.; Pisa, P.; Egevad, L. Distribution of Foxp3-, CD4- and CD8-positive lymphocytic cells in benign and malignant prostate tissue. APMIS 2010, 118, 360–365. [Google Scholar] [CrossRef]
- Ji, D.; Song, C.; Li, Y.; Xia, J.; Wu, Y.; Jia, J.; Cui, X.; Yu, S.; Gu, J. Combination of radiotherapy and suppression of Tregs enhances abscopal antitumor effect and inhibits metastasis in rectal cancer. J. Immunother. Cancer 2020, 8, e000826. [Google Scholar] [CrossRef]
- Mirjolet, C.; Truc, G. Abscopal effect: Myth or reality? Cancer Radiother. 2021, 25, 533–536. [Google Scholar] [CrossRef]
- Duan, X.; Wang, M.; Han, X.; Ren, J.; Huang, G.; Ju, S.; Zhang, Q. Combined use of microwave ablation and cell immunotherapy induces nonspecific immunity of hepatocellular carcinoma model mice. Cell Cycle 2020, 19, 3595–3607. [Google Scholar] [CrossRef]
- Shao, Q.; O’Flanagan, S.; Lam, T.; Roy, P.; Pelaez, F.; Burbach, B.J.; Azarin, S.M.; Shimizu, Y.; Bischof, J.C. Engineering T cell response to cancer antigens by choice of focal therapeutic conditions. Int. J. Hyperth. 2019, 36, 130–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, T.; Li, Q.; Chi, X.; Li, L.; Rao, J.; Hu, K. 0 °C is better?—Thawing temperature optimization study for cancer cryoablation in a mouse model with green fluorescent protein-labeled Lewis lung cancer. Cryobiology 2017, 75, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Lin, S.; Liang, J.; Zhu, Y. PD-1 blockade enhances the anti-tumor immune response induced by cryoablation in a murine model of renal cell carcinoma. Cryobiology 2019, 87, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Gaitanis, G.; Bassukas, I.D. Immunocryosurgery for non-superficial basal cell carcinomas ≤ 20 mm in maximal diameter: Five-year follow-up. J. Geriatr. Oncol. 2019, 10, 475–478. [Google Scholar] [CrossRef] [PubMed]
- Loewe, S.; Muischnek, H. Über Kombination Swirkungen. Arch. Exp. Pathol. 1926, 114, 313–326. [Google Scholar] [CrossRef]
- Gao, M.; Wang, T.; Ji, L.; Bai, S.; Tian, L.; Song, H. Therapy with Carboplatin and Anti-PD-1 Antibodies before Surgery Demonstrates Sustainable Anti-Tumor Effects for Secondary Cancers in Mice with Triple-Negative Breast Cancer. Front. Immunol. 2020, 11, 366. [Google Scholar] [CrossRef] [Green Version]
- Liang, Y.; Zhang, H.; Song, X.; Yang, Q. Metastatic heterogeneity of breast cancer: Molecular mechanism and potential therapeutic targets. Semin. Cancer Biol. 2020, 60, 14–27. [Google Scholar] [CrossRef]
- Takahashi, Y.; Izumi, Y.; Matsutani, N.; Dejima, H.; Nakayama, T.; Okamura, R.; Uehara, H.; Kawamura, M. Optimized magnitude of cryosurgery facilitating anti-tumor immunoreaction in a mouse model of Lewis lung cancer. Cancer Immunol. Immunother. 2016, 65, 973–982. [Google Scholar] [CrossRef]
- Akatsu, T.; Ono, K.; Katayama, Y.; Tamura, T.; Nishikawa, M.; Kugai, N.; Yamamoto, M.; Nagata, N. The Mouse Mammary Tumor Cell Line, MMT060562, Produces Prostaglandin E2 and Leukemia Inhibitory Factor and Supports Osteoclast Formation In Vitro Via a Stromal Cell-Dependent Pathway. J. Bone Miner. Res. 1998, 13, 400–408. [Google Scholar] [CrossRef]
- Ono, K.; Akatsu, T.; Murakami, T.; Wada, S.; Nishikawa, M.; Kugai, N.; Yamamoto, M.; Matsuura, N.; Nagata, N. Mouse Mammary Carcinoma Cell Line (BALB/c-MC) Stimulates Osteoclast Formation from Mouse Bone Marrow Cells Through Cell-to-Cell Contact. Bone 1998, 23, 27–32. [Google Scholar] [CrossRef]
- Steinbach, J.P.; Weissenberger, J.; Aguzzi, A. Distinct phases of cryogenic tissue damage in the cerebral cortex of wild-type and c-fos deficient mice. Neuropathol. Appl. Neurobiol. 1999, 25, 468–480. [Google Scholar] [CrossRef] [PubMed]
- Song, K.D. Percutaneous cryoablation for hepatocellular carcinoma. Clin. Mol. Hepatol. 2016, 22, 509–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Euhus, D.M.; Hudd, C.; Laregina, M.C.; Johnson, F.E. Tumor measurement in the nude mouse. J. Surg. Oncol. 1986, 31, 229–234. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Annen, R.; Kato, S.; Demura, S.; Miwa, S.; Yokka, A.; Shinmura, K.; Yokogawa, N.; Yonezawa, N.; Kobayashi, M.; Kurokawa, Y.; et al. Tumor-Specific Immunoenhancing Effects after Local Cryoablation for Metastatic Bone Tumor in a Mouse Model. Int. J. Mol. Sci. 2022, 23, 9445. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23169445
Annen R, Kato S, Demura S, Miwa S, Yokka A, Shinmura K, Yokogawa N, Yonezawa N, Kobayashi M, Kurokawa Y, et al. Tumor-Specific Immunoenhancing Effects after Local Cryoablation for Metastatic Bone Tumor in a Mouse Model. International Journal of Molecular Sciences. 2022; 23(16):9445. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23169445
Chicago/Turabian StyleAnnen, Ryohei, Satoshi Kato, Satoru Demura, Shinji Miwa, Akira Yokka, Kazuya Shinmura, Noriaki Yokogawa, Noritaka Yonezawa, Motoya Kobayashi, Yuki Kurokawa, and et al. 2022. "Tumor-Specific Immunoenhancing Effects after Local Cryoablation for Metastatic Bone Tumor in a Mouse Model" International Journal of Molecular Sciences 23, no. 16: 9445. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23169445