
Current and Emerging Approaches for Spine Tumor Treatment

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Spine Tumors
2.1. Primary Spinal Tumors
2.2. Spinal Metastases
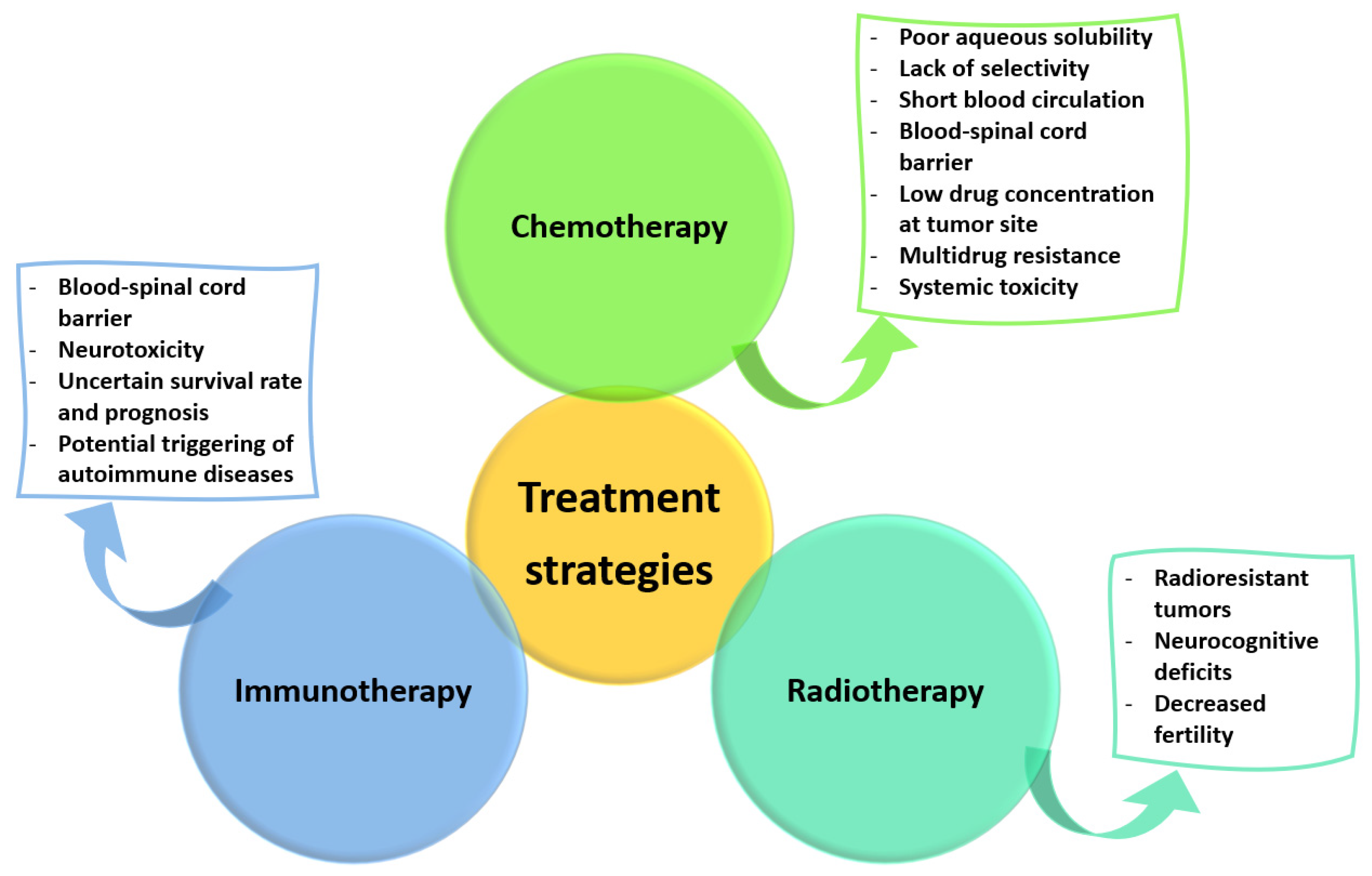
3. Current Treatment Strategies and Their Limitations
3.1. Surgical Treatment
3.2. Non-Surgical Treatment
4. Emerging Treatment Strategies
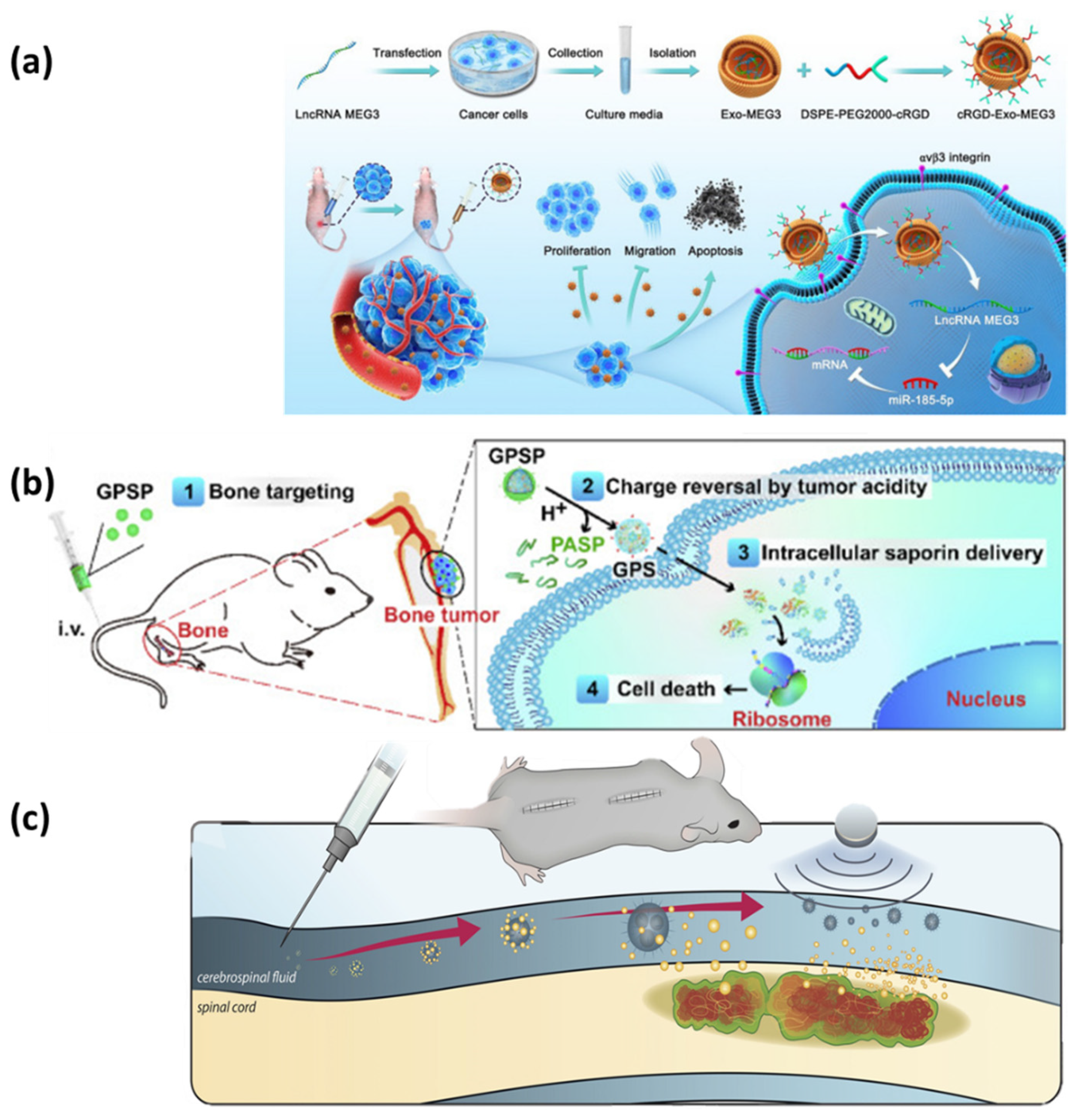
4.1. Tumor-Targeted Therapies

4.2. Custom-Made Vertebral Body Implants
4.3. Surgical Novelties
4.4. Clinical Trials
5. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frost, B.A.; Camarero-Espinosa, S.; Foster, E.J. Materials for the Spine: Anatomy, Problems, and Solutions. Materials 2019, 12, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grijalvo, S.; Nieto-Díaz, M.; Maza, R.M.; Eritja, R.; Díaz, D.D. Alginate Hydrogels as Scaffolds and Delivery Systems to Repair the Damaged Spinal Cord. Biotechnol. J. 2019, 14, 1900275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smit, T.H.; Helder, M.N. 20—In vivo models of regenerative medicine in the spine. In Biomaterials for Spinal Surgery; Ambrosio, L., Tanner, E., Eds.; Woodhead Publishing: Sawston, UK, 2012; pp. 582–607. [Google Scholar]
- Ge, L.; Arul, K.; Mesfin, A. Spinal Cord Injury From Spinal Tumors: Prevalence, Management, and Outcomes. World Neurosurg. 2019, 122, e1551–e1556. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.S.; Koffie, R.M.; Rattani, A.; Dewan, M.C.; Baticulon, R.E.; Qureshi, M.M.; Wahjoepramono, E.J.; Rosseau, G.; Park, K.; Nahed, B.V. Global incidence of brain and spinal tumors by geographic region and income level based on cancer registry data. J. Clin. Neurosci. 2019, 66, 121–127. [Google Scholar] [CrossRef]
- Porras, J.L.; Pennington, Z.; Hung, B.; Hersh, A.; Schilling, A.; Goodwin, C.R.; Sciubba, D.M. Radiotherapy and Surgical Advances in the Treatment of Metastatic Spine Tumors: A Narrative Review. World Neurosurg. 2021, 151, 147–154. [Google Scholar] [CrossRef]
- Khadka, B.; Lee, J.-Y.; Kim, K.-T.; Bae, J.-S. Recent progress in therapeutic drug delivery systems for treatment of traumatic CNS injuries. Future Med. Chem. 2020, 12, 1759–1778. [Google Scholar] [CrossRef]
- Sayyadi, M.; Moradabadi, A.; Noroozi-Aghideh, A.; Yazdanian, M. Effect of Gaillardin on Proliferation and Apoptosis of Acute Promyelocytic Leukemia Cell Lines, NB4 as Cancer Treatment. Biointerface Res. Appl. Chem. 2021, 11, 7445–7452. [Google Scholar] [CrossRef]
- Zhou, Z.; Li, D.; Fan, X.; Lin, S.; Yuan, Y.; Zhuang, P.; Hu, H.; Ge, M.; Chen, S.; Mei, X. Gold nanoclusters for optimizing the general efficacies of herbal medicines on nerve repair after spinal cord injury. Mater. Des. 2022, 215, 110465. [Google Scholar] [CrossRef]
- Hong, Q.; Song, H.; Lan Chi, N.T.; Brindhadevi, K. Numerous nanoparticles as drug delivery system to control secondary immune response and promote spinal cord injury regeneration. Process Biochem. 2022, 112, 145–153. [Google Scholar] [CrossRef]
- Mauri, E.; Masi, M. Chapter 8—Nanomaterials for spinal cord injury (SCI) regeneration. In Spinal Cord Injury (SCI) Repair Strategies; Perale, G., Rossi, F., Eds.; Woodhead Publishing: Amsterdam, The Netherlands, 2020; pp. 129–155. [Google Scholar]
- Gounden, S.; Daniels, A.; Singh, M. Chitosan-Modified Silver Nanoparticles Enhance Cisplatin Activity in Breast Cancer Cells. Biointerface Res. Appl. Chem. 2021, 11, 10572–10584. [Google Scholar] [CrossRef]
- Grewal, I.K.; Singh, S.; Arora, S.; Sharma, N. Polymeric Nanoparticles for Breast Cancer Therapy: A Comprehensive Review. Biointerface Res. Appl. Chem. 2021, 11, 11151–11171. [Google Scholar] [CrossRef]
- Kumari, R.; Saini, A.K.; Chhillar, A.K.; Saini, V.; Saini, R.V. Antitumor Effect of Bio-Fabricated Silver Nanoparticles Towards Ehrlich Ascites Carcinoma. Biointerface Res. Appl. Chem. 2021, 11, 12958–12972. [Google Scholar] [CrossRef]
- Bollen, L.; Dijkstra, S.P.D.; Bartels, R.H.M.A.; de Graeff, A.; Poelma, D.L.H.; Brouwer, T.; Algra, P.R.; Kuijlen, J.M.A.; Minnema, M.C.; Nijboer, C.; et al. Clinical management of spinal metastases—The Dutch national guideline. Eur. J. Cancer 2018, 104, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Sumdani, H.; Aguilar-Salinas, P.; Avila, M.J.; Barber, S.R.; Dumont, T. Utility of Augmented Reality and Virtual Reality in Spine Surgery: A Systematic Review of the Literature. World Neurosurg. 2022, 161, e8–e17. [Google Scholar] [CrossRef] [PubMed]
- Lador, R.; Regev, G.; Salame, K.; Khashan, M.; Lidar, Z. Use of 3-Dimensional Printing Technology in Complex Spine Surgeries. World Neurosurg. 2020, 133, e327–e341. [Google Scholar] [CrossRef] [PubMed]
- Horst, J.D.; De Andrade, P.P.; Duvoisin, C.A.; Vieira, R.D. Fabrication of Conductive Filaments for 3D-printing: Polymer Nanocomposites. Biointerface Res. Appl. Chem. 2020, 10, 6577–6586. [Google Scholar] [CrossRef]
- Ngadiman, N.H.A.; Abidin, R.Z.; Murizan, N.I.S.; Yusof, N.M.; Idris, A.; Kadir, A.Z.A. Optimization of Materials Composition and UV-VIS Light Wavelength Towards Curing Time Performance on Development of Tissue Engineering Scaffold. Biointerface Res. Appl. Chem. 2021, 11, 8740–8750. [Google Scholar] [CrossRef]
- Laufer, I.; Bilsky, M.H. Advances in the treatment of metastatic spine tumors: The future is not what it used to be. J. Neurosurg. Spine 2019, 30, 299–307. [Google Scholar] [CrossRef]
- Li, J.; Wei, W.; Xu, F.; Wang, Y.; Liu, Y.; Fu, C. Clinical Therapy of Metastatic Spinal Tumors. Front. Surg. 2021, 8, 626873. [Google Scholar] [CrossRef]
- Ahangar, P.; Aziz, M.; Rosenzweig, D.H.; Weber, M.H. Advances in personalized treatment of metastatic spine disease. Ann. Transl. Med. 2019, 7, 223. [Google Scholar] [CrossRef]
- Anwar, M.A.; El-Baba, C.; Elnaggar, M.H.; Elkholy, Y.O.; Mottawea, M.; Johar, D.; Al Shehabi, T.S.; Kobeissy, F.; Moussalem, C.; Massaad, E.; et al. Novel therapeutic strategies for spinal osteosarcomas. Semin. Cancer Biol. 2020, 64, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Sheha, E.D.; Gandhi, S.D.; Colman, M.W. 3D printing in spine surgery. Ann. Transl. Med. 2019, 7, S164. [Google Scholar] [CrossRef] [PubMed]
- Ottenhausen, M.; Ntoulias, G.; Bodhinayake, I.; Ruppert, F.-H.; Schreiber, S.; Förschler, A.; Boockvar, J.A.; Jödicke, A. Intradural spinal tumors in adults—Update on management and outcome. Neurosurg. Rev. 2019, 42, 371–388. [Google Scholar] [CrossRef] [PubMed]
- Das, J.M.; Hoang, S.; Mesfin, F.B. Intramedullary spinal cord tumors. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Walha, S.; Fairbanks, S.L. Spinal Cord Tumor Surgery. Anesthesiol. Clin. 2021, 39, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Mary S., S.C.; Sasikala, S. An expert system of MRI spinal cord tumor types using glcm features for classification techniques. MATTER Int. J. Sci. Technol. 2019, 5, 20–34. [Google Scholar] [CrossRef]
- Rauschenbach, L. Spinal Cord Tumor Microenvironment. In Tumor Microenvironments in Organs: From the Brain to the Skin—Part A; Birbrair, A., Ed.; Springer International Publishing: Cham, Switzerland, 2020; pp. 97–109. [Google Scholar]
- Grady, C.; Melnick, K.; Porche, K.; Dastmalchi, F.; Hoh, D.J.; Rahman, M.; Ghiaseddin, A. Glioma immunotherapy: Advances and challenges for spinal cord gliomas. Neurospine 2022, 19, 13. [Google Scholar] [CrossRef] [PubMed]
- Missenard, G.; Bouthors, C.; Fadel, E.; Court, C. Surgical strategies for primary malignant tumors of the thoracic and lumbar spine. Orthop. Traumatol. Surg. Res. 2020, 106, S53–S62. [Google Scholar] [CrossRef] [PubMed]
- Kerr, D.L.; Dial, B.L.; Lazarides, A.L.; Catanzano, A.A.; Lane, W.O.; Blazer, D.G.; Brigman, B.E.; Mendoza-Lattes, S.; Eward, W.C.; Erickson, M.E. Epidemiologic and survival trends in adult primary bone tumors of the spine. Spine J. 2019, 19, 1941–1949. [Google Scholar] [CrossRef]
- Vuong, H.G.; Dunn, I.F. Chondrosarcoma and Chordoma of the Skull Base and Spine: Implication of Tumor Location on Patient Survival. World Neurosurg. 2022, 162, e635–e639. [Google Scholar] [CrossRef]
- Baig Mirza, A.; Bartram, J.; Okasha, M.; Al Banna, Q.; Vastani, A.; Maratos, E.; Gullan, R.; Thomas, N. Surgical Management of Spinal Chordoma: A Systematic Review and Single-Center Experience. World Neurosurg. 2021, 156, e111–e129. [Google Scholar] [CrossRef]
- Court, C.; Briand, S.; Mir, O.; Le Péchoux, C.; Lazure, T.; Missenard, G.; Bouthors, C. Management of chordoma of the sacrum and mobile spine. Orthop. Traumatol. Surg. Res. 2022, 108, 103169. [Google Scholar] [CrossRef] [PubMed]
- Elmajee, M.; Osman, K.; Dermanis, A.; Duffaydar, H.; Soon, W.C.; czyz, M. A literature Review: The genomic landscape of spinal chondrosarcoma and potential diagnostic, prognostic & therapeutic implications. Interdiscip. Neurosurg. 2022, 30, 101651. [Google Scholar] [CrossRef]
- Berger, G.K.; Nisson, P.L.; James, W.S.; Kaiser, K.N.; Hurlbert, R.J. Outcomes in different age groups with primary Ewing sarcoma of the spine: A systematic review of the literature. J. Neurosurg. Spine 2019, 30, 664–673. [Google Scholar] [CrossRef]
- Lu, V.M.; Goyal, A.; Alvi, M.A.; Kerezoudis, P.; Haddock, M.G.; Bydon, M. Primary intradural Ewing’s sarcoma of the spine: A systematic review of the literature. Clin. Neurol. Neurosurg. 2019, 177, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Hesla, A.C.; Bruland, Ø.S.; Jebsen, N.; Styring, E.; Eriksson, S.; Tsagozis, P. Ewing sarcoma of the mobile spine; predictive factors for survival, neurological function and local control. A Scandinavian sarcoma group study with a mean follow-up of 12 years. J. Bone Oncol. 2019, 14, 100216. [Google Scholar] [CrossRef]
- Zhang, J.; Huang, Y.; Lu, J.; He, A.; Zhou, Y.; Hu, H.; Shen, Z.; Sun, Y.; Yao, Y. Impact of first-line treatment on outcomes of Ewing sarcoma of the spine. Am. J. Cancer Res. 2018, 8, 1262. [Google Scholar]
- Ahangar, P.; Akoury, E.; Ramirez Garcia Luna, A.S.; Nour, A.; Weber, M.H.; Rosenzweig, D.H. Nanoporous 3D-Printed Scaffolds for Local Doxorubicin Delivery in Bone Metastases Secondary to Prostate Cancer. Materials 2018, 11, 1485. [Google Scholar] [CrossRef] [Green Version]
- Kuah, T.; Vellayappan, B.A.; Makmur, A.; Nair, S.; Song, J.; Tan, J.H.; Kumar, N.; Quek, S.T.; Hallinan, J.T.P.D. State-of-the-Art Imaging Techniques in Metastatic Spinal Cord Compression. Cancers 2022, 14, 3289. [Google Scholar] [CrossRef]
- Meyer, H.S.; Wagner, A.; Raufer, A.; Joerger, A.-K.; Gempt, J.; Meyer, B. Surgery in Acute Metastatic Spinal Cord Compression: Timing and Functional Outcome. Cancers 2022, 14, 2249. [Google Scholar] [CrossRef]
- Berardi, R.; Morgese, F.; Rinaldi, S.; Torniai, M.; Mentrasti, G.; Scortichini, L.; Giampieri, R. Benefits and Limitations of a Multidisciplinary Approach in Cancer Patient Management. Cancer Manag. Res. 2020, 12, 9363–9374. [Google Scholar] [CrossRef]
- Barzilai, O.; Robin, A.M.; O’Toole, J.E.; Laufer, I. Minimally Invasive Surgery Strategies: Changing the Treatment of Spine Tumors. Neurosurg. Clin. N. Am. 2020, 31, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, S.T.; Kirkegaard, A.O.; Carreon, L.; Rousing, R.; Andersen, M.Ø. Vertebroplasty or kyphoplasty as palliative treatment for cancer-related vertebral compression fractures: A systematic review. Spine J. 2019, 19, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- Barber, S.M.; Fridley, J.S.; Konakondla, S.; Nakhla, J.; Oyelese, A.A.; Telfeian, A.E.; Gokaslan, Z.L. Cerebrospinal fluid leaks after spine tumor resection: Avoidance, recognition and management. Ann. Transl. Med. 2019, 7, 217. [Google Scholar] [CrossRef] [PubMed]
- Igoumenou, V.G.; Mavrogenis, A.F.; Angelini, A.; Baracco, R.; Benzakour, A.; Benzakour, T.; Bork, M.; Vazifehdan, F.; Nena, U.; Ruggieri, P. Complications of spine surgery for metastasis. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 37–56. [Google Scholar] [CrossRef] [PubMed]
- Amjad, M.T.; Chidharla, A.; Kasi, A. Cancer chemotherapy. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Chidambaram, M.; Manavalan, R.; Kathiresan, K. Nanotherapeutics to overcome conventional cancer chemotherapy limitations. J. Pharm. Pharm. Sci. 2011, 14, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Wo, J.Y.; Viswanathan, A.N. Impact of Radiotherapy on Fertility, Pregnancy, and Neonatal Outcomes in Female Cancer Patients. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1304–1312. [Google Scholar] [CrossRef] [Green Version]
- Monje, M.; Dietrich, J. Cognitive side effects of cancer therapy demonstrate a functional role for adult neurogenesis. Behav. Brain Res. 2012, 227, 376–379. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.; Liu, T.; Han, B.; Tan, S.; Guo, H.; Xin, Y. Immunotherapy: A potential approach for high-grade spinal cord astrocytomas. Front. Immunol. 2021, 11, 582828. [Google Scholar] [CrossRef]
- Tan, S.; Li, D.; Zhu, X. Cancer immunotherapy: Pros, cons and beyond. Biomed. Pharmacother. 2020, 124, 109821. [Google Scholar] [CrossRef]
- Varghese, R.; Salvi, S.; Sood, P.; Kulkarni, B.; Kumar, D. Cubosomes in cancer drug delivery: A review. Colloid Interface Sci. Commun. 2022, 46, 100561. [Google Scholar] [CrossRef]
- Mansoori, B.; Mohammadi, A.; Davudian, S.; Shirjang, S.; Baradaran, B. The different mechanisms of cancer drug resistance: A brief review. Adv. Pharm. Bull. 2017, 7, 339. [Google Scholar] [CrossRef] [PubMed]
- Saleem, J.; Wang, L.M.; Chen, C.Y. Carbon-Based Nanomaterials for Cancer Therapy via Targeting Tumor Microenvironment. Adv. Healthc. Mater. 2018, 7, 1800525. [Google Scholar] [CrossRef] [PubMed]
- Belfiore, L.; Saunders, D.N.; Ranson, M.; Thurecht, K.J.; Storm, G.; Vine, K.L. Towards clinical translation of ligand-functionalized liposomes in targeted cancer therapy: Challenges and opportunities. J. Control. Release 2018, 277, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, G.; Esposito, M.; Kang, Y. Bone metastasis and the metastatic niche. J. Mol. Med. 2015, 93, 1203–1212. [Google Scholar] [CrossRef] [Green Version]
- Guise, T. Examining the Metastatic Niche: Targeting the Microenvironment. Semin. Oncol. 2010, 37, S2–S14. [Google Scholar] [CrossRef]
- Yan, Y.; Zhou, L.; Sun, Z.; Song, D.; Cheng, Y. Targeted and intracellular delivery of protein therapeutics by a boronated polymer for the treatment of bone tumors. Bioact. Mater. 2022, 7, 333–340. [Google Scholar] [CrossRef]
- Wu, H.; Luo, Y.; Xu, D.; Ke, X.; Ci, T. Low molecular weight heparin modified bone targeting liposomes for orthotopic osteosarcoma and breast cancer bone metastatic tumors. Int. J. Biol. Macromol. 2020, 164, 2583–2597. [Google Scholar] [CrossRef]
- Ahmadi, D.; Zarei, M.; Rahimi, M.; Khazaie, M.; Asemi, Z.; Mir, S.M.; Sadeghpour, A.; Karimian, A.; Alemi, F.; Rahmati-Yamchi, M.; et al. Preparation and in-vitro evaluation of pH-responsive cationic cyclodextrin coated magnetic nanoparticles for delivery of methotrexate to the Saos-2 bone cancer cells. J. Drug Deliv. Sci. Technol. 2020, 57, 101584. [Google Scholar] [CrossRef]
- Khelghati, N.; Rasmi, Y.; Farahmandan, N.; Sadeghpour, A.; Mir, S.M.; Karimian, A.; Yousefi, B. Hyperbranched polyglycerol β-cyclodextrin as magnetic platform for optimization of doxorubicin cytotoxic effects on Saos-2 bone cancerous cell line. J. Drug Deliv. Sci. Technol. 2020, 57, 101741. [Google Scholar] [CrossRef]
- Plesselova, S.; Garcia-Cerezo, P.; Blanco, V.; Reche-Perez, F.J.; Hernandez-Mateo, F.; Santoyo-Gonzalez, F.; Giron-Gonzalez, M.D.; Salto-Gonzalez, R. Polyethylenimine–Bisphosphonate–Cyclodextrin Ternary Conjugates: Supramolecular Systems for the Delivery of Antineoplastic Drugs. J. Med. Chem. 2021, 64, 12245–12260. [Google Scholar] [CrossRef]
- Huang, X.; Wu, W.; Jing, D.; Yang, L.; Guo, H.; Wang, L.; Zhang, W.; Pu, F.; Shao, Z. Engineered exosome as targeted lncRNA MEG3 delivery vehicles for osteosarcoma therapy. J. Control. Release 2022, 343, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.; Huang, Y.; Huang, S.; Zhuang, J.; Chen, P.; Wang, Y.; Zhang, L. Targeted delivery of cancer drug paclitaxel to chordomas tumor cells via an RNA nanoparticle harboring an EGFR aptamer. Colloids Surf. B Biointerfaces 2022, 212, 112366. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhao, Z.; Xie, C.; Zhao, Y. Dual-targeting liposome modified by glutamic hexapeptide and folic acid for bone metastatic breast cancer. Chem. Phys. Lipids 2020, 228, 104882. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.T.; Nguyen, H.T.; Phung, C.D.; Pathak, S.; Regmi, S.; Ha, D.-H.; Kim, J.O.; Yong, C.S.; Kim, S.K.; Choi, J.-E.; et al. Targeted delivery of doxorubicin for the treatment of bone metastasis from breast cancer using alendronate-functionalized graphene oxide nanosheets. J. Ind. Eng. Chem. 2019, 76, 310–317. [Google Scholar] [CrossRef]
- Kheirkhah, P.; Denyer, S.; Bhimani, A.D.; Arnone, G.D.; Esfahani, D.R.; Aguilar, T.; Zakrzewski, J.; Venugopal, I.; Habib, N.; Gallia, G.L.; et al. Magnetic Drug Targeting: A Novel Treatment for Intramedullary Spinal Cord Tumors. Sci. Rep. 2018, 8, 11417. [Google Scholar] [CrossRef] [Green Version]
- Costanzo, R.; Ferini, G.; Brunasso, L.; Bonosi, L.; Porzio, M.; Benigno, U.E.; Musso, S.; Gerardi, R.M.; Giammalva, G.R.; Paolini, F.; et al. The Role of D. Printed Custom-Made Vertebral Body Implants in the Treatment of Spinal Tumors A. Systematic Review. Life 2022, 12, 489. [Google Scholar] [CrossRef]
- Chatain, G.P.; Finn, M. Compassionate use of a custom 3D-printed sacral implant for revision of failing sacrectomy: Case report. J. Neurosurg. Spine SPI 2020, 33, 513–518. [Google Scholar] [CrossRef]
- Leary, O.P.; Crozier, J.; Liu, D.D.; Niu, T.; Pertsch, N.J.; Camara-Quintana, J.Q.; Svokos, K.A.; Syed, S.; Telfeian, A.E.; Oyelese, A.A.; et al. Three-Dimensional Printed Anatomic Modeling for Surgical Planning and Real-Time Operative Guidance in Complex Primary Spinal Column Tumors: Single-Center Experience and Case Series. World Neurosurg. 2021, 145, e116–e126. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Choy, W.J.; Wilson, P.; McEvoy, A.; Phan, K.; Parr, W.C.H. L5 En-Bloc Vertebrectomy with Customized Reconstructive Implant: Comparison of Patient-Specific Versus Off-the-Shelf Implant. World Neurosurg. 2018, 112, 94–100. [Google Scholar] [CrossRef]
- Xu, N.; Wei, F.; Liu, X.; Jiang, L.; Cai, H.; Li, Z.; Yu, M.; Wu, F.; Liu, Z. Reconstruction of the upper cervical spine using a personalized 3D-printed vertebral body in an adolescent with Ewing sarcoma. Spine 2016, 41, E50–E54. [Google Scholar] [CrossRef]
- Parr, W.C.H.; Burnard, J.L.; Singh, T.; McEvoy, A.; Walsh, W.R.; Mobbs, R.J. C3-C5 Chordoma Resection and Reconstruction with a Three-Dimensional Printed Titanium Patient-Specific Implant. World Neurosurg. 2020, 136, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.; Li, Z.; Liu, Z.; Liu, X.; Jiang, L.; Yu, M.; Xu, N.; Wu, F.; Dang, L.; Zhou, H.; et al. Upper cervical spine reconstruction using customized 3D-printed vertebral body in 9 patients with primary tumors involving C2. J Ann. Transl. Med. 2020, 8, 332. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, X.; Zhang, Y.; Zhang, H.; Sun, H.; Hao, D.; Wang, B. One-stage posterior en-bloc spondylectomy following reconstruction with individualized 3D printed artificial vertebrae for multi-segment thoracolumbar metastases: Case report and literature review. Am. J. Transl. Res. 2021, 13, 115–123. [Google Scholar] [PubMed]
- Kim, D.; Lim, J.-Y.; Shim, K.-W.; Han, J.W.; Yi, S.; Yoon, D.H.; Kim, K.N.; Ha, Y.; Ji, G.Y.; Shin, D.A. Sacral Reconstruction with a 3D-Printed Implant after Hemisacrectomy in a Patient with Sacral Osteosarcoma: 1-Year Follow-Up Result. YMJ 2017, 58, 453–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Ma, Z.; Yuan, K.; Ji, T. Using scaffolds as drug delivery systems to treat bone tumor. Nanotechnology 2022, 33, 212002. [Google Scholar] [CrossRef] [PubMed]
- Ghaednia, H.; Fourman, M.S.; Lans, A.; Detels, K.; Dijkstra, H.; Lloyd, S.; Sweeney, A.; Oosterhoff, J.H.F.; Schwab, J.H. Augmented and virtual reality in spine surgery, current applications and future potentials. Spine J. 2021, 21, 1617–1625. [Google Scholar] [CrossRef]
- Eliahu, K.; Liounakos, J.; Wang, M.Y. Applications for Augmented and Virtual Reality in Robot-Assisted Spine Surgery. Curr. Robot. Rep. 2022, 3, 33–37. [Google Scholar] [CrossRef]
- Morimoto, T.; Kobayashi, T.; Hirata, H.; Otani, K.; Sugimoto, M.; Tsukamoto, M.; Yoshihara, T.; Ueno, M.; Mawatari, M. XR (Extended Reality: Virtual Reality, Augmented Reality, Mixed Reality) Technology in Spine Medicine: Status Quo and Quo Vadis. J. Clin. Med. 2022, 11, 470. [Google Scholar] [CrossRef]
- Auloge, P.; Cazzato, R.L.; Ramamurthy, N.; de Marini, P.; Rousseau, C.; Garnon, J.; Charles, Y.P.; Steib, J.-P.; Gangi, A. Augmented reality and artificial intelligence-based navigation during percutaneous vertebroplasty: A pilot randomised clinical trial. Eur. Spine J. 2020, 29, 1580–1589. [Google Scholar] [CrossRef]
- Elmi-Terander, A.; Burström, G.; Nachabé, R.; Fagerlund, M.; Ståhl, F.; Charalampidis, A.; Edström, E.; Gerdhem, P. Augmented reality navigation with intraoperative 3D imaging vs fluoroscopy-assisted free-hand surgery for spine fixation surgery: A matched-control study comparing accuracy. Sci. Rep. 2020, 10, 707. [Google Scholar] [CrossRef] [Green Version]
- Gu, Y.; Yao, Q.; Xu, Y.; Zhang, H.; Wei, P.; Wang, L. A clinical application study of mixed reality technology assisted lumbar pedicle screws implantation. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e924982-1. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.-H.; Chiang, C.-C.; Wang, M.-L.; Wu, N.-Y.; Lee, P.-Y. Clinical feasibility of the augmented reality computer-assisted spine surgery system for percutaneous vertebroplasty. Eur. Spine J. 2020, 29, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Wei, P.; Yao, Q.; Xu, Y.; Zhang, H.; Gu, Y.; Wang, L. Percutaneous kyphoplasty assisted with/without mixed reality technology in treatment of OVCF with IVC: A prospective study. J. Orthop. Surg. Res. 2019, 14, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, C.; Li, J.; Zeng, G.; Ye, W.; Sun, J.; Hong, J.; Li, C. Development of a virtual reality preoperative planning system for postlateral endoscopic lumbar discectomy surgery and its clinical application. World Neurosurg. 2019, 123, e1–e8. [Google Scholar] [CrossRef]
- Carl, B.; Bopp, M.; Saß, B.; Voellger, B.; Nimsky, C. Implementation of augmented reality support in spine surgery. Eur. Spine J. 2019, 28, 1697–1711. [Google Scholar] [CrossRef]
- Carl, B.; Bopp, M.; Saß, B.; Pojskic, M.; Gjorgjevski, M.; Voellger, B.; Nimsky, C. Reliable navigation registration in cranial and spine surgery based on intraoperative computed tomography. Neurosurg. Focus 2019, 47, E11. [Google Scholar] [CrossRef] [Green Version]
- Rasouli, J.J.; Shao, J.; Neifert, S.; Gibbs, W.N.; Habboub, G.; Steinmetz, M.P.; Benzel, E.; Mroz, T.E. Artificial Intelligence and Robotics in Spine Surgery. Glob. Spine J. 2020, 11, 556–564. [Google Scholar] [CrossRef] [Green Version]
- Gumbs, A.A.; Perretta, S.; d’Allemagne, B.; Chouillard, E. What is artificial intelligence surgery? Artif. Intell. Surg. 2021, 1, 1–10. [Google Scholar] [CrossRef]
- Benzakour, A.; Altsitzioglou, P.; Lemée, J.M.; Ahmad, A.; Mavrogenis, A.F.; Benzakour, T. Artificial intelligence in spine surgery. Int. Orthop. 2022, 1–9. [Google Scholar] [CrossRef]
- Hopkins, B.S.; Mazmudar, A.; Driscoll, C.; Svet, M.; Goergen, J.; Kelsten, M.; Shlobin, N.A.; Kesavabhotla, K.; Smith, Z.A.; Dahdaleh, N.S. Using artificial intelligence (AI) to predict postoperative surgical site infection: A retrospective cohort of 4046 posterior spinal fusions. Clin. Neurol. Neurosurg. 2020, 192, 105718. [Google Scholar] [CrossRef]
- Washington University School of Medicine. Stereotactic Radiosurgery (SRS) for Spine Metastases (SRS). Available online: https://clinicaltrials.gov/ct2/show/NCT00593320 (accessed on 5 September 2022).
- Mahadevan, A. Randomized Study of Stereotactic Body Radiotherapy vs. Conventional Radiation for Spine Metastasis. Available online: https://clinicaltrials.gov/ct2/show/NCT01525745 (accessed on 5 September 2022).
- Rizzoli, I.O. Custom Pack in Spine Surgery (Kit). Available online: https://clinicaltrials.gov/ct2/show/NCT03050203 (accessed on 5 September 2022).
- McGarry, R. Conformal High Dose Intensity Modulated Radiation Therapy for Disease to Thoracic and Lumbar Spine. Available online: https://clinicaltrials.gov/ct2/show/NCT01654068 (accessed on 5 September 2022).
- Memorial Sloan Kettering Cancer Center. Image-Guided Navigation for High Dose Rate Temporary Interstitial Brachytherapy in the Palliative Management of Previously Treated Tumors of the Spine and Pelvis. Available online: https://clinicaltrials.gov/ct2/show/NCT01757717 (accessed on 5 September 2022).
- Mai, J. Stereotactic Body Radiotherapy for Spine Tumors. Available online: https://clinicaltrials.gov/ct2/show/NCT01347307 (accessed on 5 September 2022).
- Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins. Radiotherapy for Solid Tumor Spine Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT01752036 (accessed on 5 September 2022).
- Radiation Therapy Oncology Group. Image-Guided Radiosurgery or Stereotactic Body Radiation Therapy in Treating Patients with Localized Spine Metastasis. Available online: https://clinicaltrials.gov/ct2/show/NCT00922974 (accessed on 5 September 2022).
- MedtronicNeuro. OsteoCool Tumor Ablation Post-Market Study (OPuS One). Available online: https://clinicaltrials.gov/ct2/show/NCT03249584 (accessed on 5 September 2022).
- Timmerman, R. Stereotactic Body Radiation Therapy and Vertebroplasty in Treating Patients with Localized Spinal Metastasis. Available online: https://clinicaltrials.gov/ct2/show/NCT00855803 (accessed on 5 September 2022).
- Lee, T.C. Image-guided Cryoablation of Head, Neck and Spine Tumors. Available online: https://clinicaltrials.gov/ct2/show/NCT02085941 (accessed on 5 September 2022).
- Redmond, K.J.; Sciubba, D.; Khan, M.; Gui, C.; Lo, S.L.; Gokaslan, Z.L.; Leaf, B.; Kleinberg, L.; Grimm, J.; Ye, X.; et al. A Phase 2 Study of Post-Operative Stereotactic Body Radiation Therapy (SBRT) for Solid Tumor Spine Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.; Pugh, S.L.; Gerszten, P.C.; Yin, F.-F.; Timmerman, R.D.; Hitchcock, Y.J.; Movsas, B.; Kanner, A.A.; Berk, L.B.; Followill, D.S.; et al. RTOG 0631 phase 2/3 study of image guided stereotactic radiosurgery for localized (1-3) spine metastases: Phase 2 results. Pract. Radiat. Oncol. 2014, 4, 76–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, J.; Hopkins, T.; Morris, J.; Tran, N.D.; David, E.; Massari, F.; Farid, H.; Vogel, A.; O’Connell, W.G.; Sunenshine, P.; et al. Radiofrequency Ablation for the Palliative Treatment of Bone Metastases: Outcomes from the Multicenter OsteoCool Tumor Ablation Post-Market Study (OPuS One Study) in 100 Patients. J. Vasc. Interv. Radiol. 2020, 31, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Taipei Veterans General Hospital, Taiwan. Study to Evaluate the Safety and Clinical Outcome of Using Navigation System in Pedicle Screw Placement in Spine Surgery. Available online: https://clinicaltrials.gov/ct2/show/NCT04578691 (accessed on 5 September 2022).
- M.D. Anderson Cancer Center. Evaluation of a Novel CT-On-Rails or Trilogy Stereotactic Spine Radiotherapy System (SSRS). Available online: https://clinicaltrials.gov/ct2/show/NCT00508443 (accessed on 5 September 2022).
- Ghaly, M. Kypho-Intra Operative Radiation Therapy (IORT) for Localized Spine Metastasis, Phase I/II Study (Kypho-IORT). Available online: https://clinicaltrials.gov/ct2/show/NCT02987153 (accessed on 5 September 2022).
- M.D. Anderson Cancer Center. Cement Augmentation in Preventing Vertebral Body Compression Fracture Following Spine Stereotactic Radiosurgery in Patients with Solid Tumors and Spinal Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT02387905 (accessed on 5 September 2022).
- M.D. Anderson Cancer Center. 18F-FDG PET-MRI for Planning and Follow-Up of Patients with Spine Tumors Treated with Spine Stereotactic Radiosurgery. Available online: https://clinicaltrials.gov/ct2/show/NCT05174026 (accessed on 5 September 2022).
- M.D. Anderson Cancer Center. Standard and Delayed FDG PET/CT After Chemoradiation Therapy in Assessing Patients with Metastatic Head and Neck Squamous Cell Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03575949 (accessed on 5 September 2022).
- M.D. Anderson Cancer Center. Single Versus Multifraction Salvage Spine Stereotactic Radiosurgery for Previously Irradiated Spinal Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT03028337 (accessed on 5 September 2022).
- Wong, J. Ablation and Cementoplasty for Painful Bone Lesions. Available online: https://clinicaltrials.gov/ct2/show/NCT04635137 (accessed on 5 September 2022).
- Wake Forest University Health Sciences. Study of Combined Decompressive Spine Radiosurgery and Pembrolizumab. Available online: https://clinicaltrials.gov/ct2/show/NCT05204290 (accessed on 5 September 2022).
- Zetagen Therapeutics, Inc. ZetaFuse™ Bone Graft in the Repair of Bone Defects From Metastatic Breast Cancer in the Spinal Vertebral Body (ZGMBC). Available online: https://clinicaltrials.gov/ct2/show/NCT05280067 (accessed on 5 September 2022).
- Children’s Cancer Hospital Egypt 57357. Dexmedetomidine Infusion on Intraoperative Propofol, Fentanyl Requirements in Spine Surgery for Pediatric Cancer Patients. Available online: https://clinicaltrials.gov/ct2/show/NCT05493228 (accessed on 5 September 2022).
- Axon srl. SPINERY™ A Novel Radio-Frequency Tumor Ablation Device Study (SPARTA). Available online: https://clinicaltrials.gov/ct2/show/NCT05467540 (accessed on 5 September 2022).
- Case Comprehensive Cancer Center. Single- vs. Two-Fraction Spine Stereotactic Radiosurgery for the Treatment of Vertebral Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT04218617 (accessed on 5 September 2022).
- National Taiwan University Hospital. ERAS Anesthetic Care for Metastatic Spine Cancer Resection. Available online: https://clinicaltrials.gov/ct2/show/NCT05427825 (accessed on 5 September 2022).
- National Taiwan University Hospital. Involved Versus Elective Target SSRS for Spinal Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT04033536 (accessed on 5 September 2022).
- Baptist Health South Florida. Radiation Therapy Alone Versus Radiation Therapy Plus Radiofrequency Ablation (RFA)/Vertebral Augmentation. Available online: https://clinicaltrials.gov/ct2/show/NCT04375891 (accessed on 5 September 2022).
- Lee, I. Laser Interstitial Thermal Ablation and Stereotactic Radiosurgery for Patients with Spine Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT05023772 (accessed on 5 September 2022).
- National Taiwan University Hospital. A Prospective Study of the Safety and Efficacy of 3D-printed Non-Rigid Biomimetic Implant in Cervical and Thoracolumbar Spine. Available online: https://clinicaltrials.gov/ct2/show/NCT05396222 (accessed on 5 September 2022).
- Freire, V. Increased Early Pain Relief by Adding Vertebroplasty to SBRT. Available online: https://clinicaltrials.gov/ct2/show/NCT05317026 (accessed on 5 September 2022).
- Baptist Health South Florida. Dose-Escalated Spine SbRT for Localized Metastasis to the Spinal Column (DESSRT). Available online: https://clinicaltrials.gov/ct2/show/NCT04802603 (accessed on 5 September 2022).
- National Taiwan University Hospital. Post Operative RT for Limited Spine Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT05495399 (accessed on 5 September 2022).
- Saravi, B.; Hassel, F.; Ülkümen, S.; Zink, A.; Shavlokhova, V.; Couillard-Despres, S.; Boeker, M.; Obid, P.; Lang, G.M. Artificial Intelligence-Driven Prediction Modeling and Decision Making in Spine Surgery Using Hybrid Machine Learning Models. J. Pers. Med. 2022, 12, 509. [Google Scholar] [CrossRef]
- Massaad, E.; Fatima, N.; Hadzipasic, M.; Alvarez-Breckenridge, C.; Shankar, G.M.; Shin, J.H. Predictive Analytics in Spine Oncology Research: First Steps, Limitations, and Future Directions. Neurospine 2019, 16, 669–677. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Nanocarrier | Chemotherapeutic | Mechanism(s) of Action | Tumor Type | Reference |
|---|---|---|---|---|
| Boronated polymer coated with anionics poly(aspartic acid) | Saporin |
| Osteosarcoma | [61] |
| Liposomes modified with alendronate and low molecular weight heparin | Doxorubicin |
| Osteosarcoma Breast cancer bone metastasis | [62] |
| Magnetic nanoparticles coated with cationic cyclodextrin | Methotrexate |
| Osteosarcoma | [63] |
| Magnetic hyperbranched β-cyclodextrin | Doxorubicin |
| Osteosarcoma | [64] |
| Polyethyleneimine–bisphosphonate (BP)–cyclodextrin ternary conjugates | Doxorubicin |
| Osteosarcoma Breast cancer bone metastasis | [65] |
| c(RGDyK)-modified exosomes | lncRNA MEG3 |
| Osteosarcoma | [66] |
| 3-way junction nanoparticle functionalized with EGFR aptamer | Paclitaxel |
| Chordoma | [67] |
| Liposome modified with glutamic hexapeptide-folic acid | Paclitaxel |
| Breast cancer bone metastasis | [68] |
| Alendronate-functionalized graphene oxide nanosheets | Doxorubicin |
| Breast cancer bone metastasis | [69] |
| Magnetic nanoparticles | Doxorubicin |
| High-grade intramedullary spinal cord tumors | [70] |
| Implant Material | Implant Site | Tumor Type | Postoperative Observations | Reference |
|---|---|---|---|---|
| Titanium alloy | Upper cervical spine (between C1 and C3) | Ewing sarcoma | Uneventful recovery The patient began to ambulate on postoperative day 7 and started adjuvant treatment 3 weeks after surgery Tumor-free at the 1-year follow-up | [75] |
| Titanium alloy | Cervical spine (between C2 and C6) | Chordoma | No postoperative complications The patient was mobilized 48 h after the anterior intervention, was discharged after 10 days, and was required to wear a neck brace for 10 days No change in implant position, no evidence of hardware failure, and no significant adverse effects at 14 months follow-up Tumor-free at the 15 months follow-up | [76] |
| Titanium alloy | Upper cervical spine | Primary osseous spinal tumors | No sign of displacement or subsidence During a mean follow-up of 28.6 months, 1 patient died of systemic metastasis, and 1 had local tumor recurrence, while the other 7 patients were alive and functional in their daily living | [77] |
| Titanium alloy | Thoracolumbar spine (between T10 and L2) | Breast cancer metastasis | The patient was stable 3 days after the operation, and after 6 days, the back pain was significantly alleviated; the patient could walk normally independently with a thoracolumbar brace Tumor-free at the 2 years follow-up | [78] |
| Titanium alloy | Lumbar spine (between L4 and S1) | Renal cell metastasis | No intraoperative complications The patient was mobilized on postoperative day 4 and discharged on day 15 At the 3-month follow-up, the surgical and low back pain settled considerably, but the functional motion range of the lumbar spine remained limited | [74] |
| Porous titanium mesh | Sacrum | Chordoma | Tumor-free at the 18-month follow-up The patient could walk short distances with assistance | [72] |
| Porous titanium mesh | Sacrum | Osteosarcoma | The patient could walk 2 weeks after surgery Due to the resection of the left S1 nerve root, there occurred a left foot drop and neuropathic pain in the left leg The patient underwent 3 cycles of adjuvant chemotherapy up to 12 months after the surgery | [79] |
| ClinicalTrials.gov Identifier | Official Title | Intervention/Treatment | Phase | Actual Study Completion Date | Reference |
|---|---|---|---|---|---|
| NCT00593320 | Stereotactic Radiosurgery (SRS) for One or Two Localized Spine Metastases | Radiation: Stereotactic Radiosurgery | Not Applicable | March 2010 | [96] |
| NCT01525745 | Randomized Ph II Study of Stereotactic Body Radiotherapy (SBRT) Versus Conventional Radiation for Spine Metastasis | Radiation: Radiosurgery/SBRT Radiation: External Beam Radiation Therapy | Phase 2 | January 2014 | [97] |
| NCT03050203 | Surgical Field Custom Pack’s Efficacy on Soft Tissue Dissecting Time Reduction, on Relative Risks and Materials Wasted, in Patients Undergoing Spine Surgery: Randomized Controlled Trial | Other: custom pack Other: standard care | Not Applicable | 30 July 2016 | [98] |
| NCT01654068 | Conformal High Dose Intensity Modulated Radiation Therapy for Asymptomatic Metastatic Disease to the Thoracic and Lumbar Spine | Radiation: Conformal High Dose Intensity Modulated Radiation Therapy | Not Applicable | 8 September 2016 | [99] |
| NCT01757717 | A Pilot Study of Image-Guided Navigation for High Dose Rate Temporary Interstitial Brachytherapy in the Palliative Management of Previously Treated Tumors of the Spine and Pelvis | Radiation: Ir-192 high dose rate (HDR) | Not Applicable | July 2017 | [100] |
| NCT01347307 | Phase IV Trial Evaluating the Use of Stereotactic Body Radiotherapy for the Treatment of Spine Metastases and Primary Spine Tumors | Radiation: SBRT for Benign Extradural Spine Tumors Radiation: SBRT for Vertebral/Paraspinal Metastases | Not Applicable | September 2017 | [101] |
| NCT01752036 | Phase II Study of Postoperative Stereotactic Radiosurgery for Solid Tumor Spine Metastases | Radiation: Postoperative, SBRT | Phase 2 | 27 July 2018 | [102] |
| NCT00922974 | Phase II/III Study of Image-Guided Radiosurgery/SBRT for Localized Spine Metastasis | Radiation: External beam radiation therapy Radiation: Radiosurgery/SBRT | Phase 2 Phase 3 | 6 April 2020 | [103] |
| NCT03249584 | OsteoCool Tumor Ablation Post-Market Study (OPuS One) | Device: OsteoCool™ RF Ablation | Not Applicable | 17 July 2020 | [104] |
| NCT00855803 | Phase II Study of Stereotactic Body Radiation Therapy and Vertebroplasty for Localized Spinal Metastasis (SBRT Spine) | Radiation: radiation | Phase 2 | 20 January 2021 | [105] |
| NCT02085941 | Image-guided Cryoablation of Head, Neck and Spine Tumors | Device: Cryoablation Device: Biopsy | Not Applicable | July 2021 | [106] |
| ClinicalTrials.gov Identifier | Official Title | Intervention/Treatment | Phase | Estimated Study Completion Date | Reference |
|---|---|---|---|---|---|
| NCT04578691 | A Two-arm, Single Center, Randomised Study to Evaluate the Safety and Clinical Outcome of Using Navigation System in Pedicle Screw Placement in Spine Surgery | Device: “Anatase” Spine Surgery Navigation System Device: Medtronic Stealthstation S7 Treatment Guidance System | Not Applicable | 31 December 2021 | [110] |
| NCT00508443 | Phase I/II Evaluation of a Novel CT-On-Rails or Trilogy Stereotactic Spine Radiotherapy System (SSRS) for the Treatment of Metastatic Spine Disease | Radiation: Radiation Therapy | Phase 1 Phase 2 | 31 October 2022 | [111] |
| NCT02987153 | Kypho-Intra Operative Radiation Therapy (IORT) for Localized Spine Metastasis, Phase I/II Study | Radiation: Kypho-IORT | Not Applicable | November 2022 | [112] |
| NCT02387905 | Prophylactic Cement Augmentation for Patients at High Risk for Developing Vertebral Body Compression Fracture Following Spine Stereotactic Radiosurgery: A Randomized Phase II Clinical Trial | Procedure: Management of Therapy Complications Other: Quality-of-Life Assessment Other: Questionnaire Administration Radiation: Stereotactic Radiosurgery | Phase 2 | 30 November 2022 | [113] |
| NCT05174026 | A Pilot Study on the Efficacy of Advanced 18F-FDG PET-MRI in Spine Stereotactic Radiosurgery | Other: Fludeoxyglucose F-18 Procedure: Magnetic Resonance Imaging Procedure: Positron Emission Tomography | Not Applicable | 31 December 2022 | [114] |
| NCT03575949 | Dual-Time Point (DTP) FDG PET CT for the Post-Treatment Assessment of Head and Neck Tumors Following Definitive Chemoradiation Therapy | Procedure: Computed Tomography Other: Fludeoxyglucose F-18 Procedure: Positron Emission Tomography | Not Applicable | 31 December 2022 | [115] |
| NCT03028337 | Single Versus Multifraction Salvage Spine Stereotactic Radiosurgery for Previously Irradiated Spinal Metastases: A Randomized Phase II Clinical Trial | Radiation: Spine Radiosurgery Behavioral: Questionnaires | Phase 2 | 18 January 2023 | [116] |
| NCT04635137 | Percutaneous Ablation and Cementoplasty for Painful Bone Lesions: A Canadian Single-Centre Experience | Procedure: Ablation and Cementoplasty | Not Applicable | March 2023 | [117] |
| NCT05204290 | A Pilot Study of Combined Decompressive Spine Radiosurgery and Pembrolizumab in Patients with High-Grade Epidural Disease | Drug: Pembrolizumab Radiation: Stereotactic Body Radiation Therapy Other: Blood draws | Early Phase 1 | September 2023 | [118] |
| NCT05280067 | Feasibility Study of ZetaFuse™ Bone Graft in the Repair of Bone Defects from Metastatic Breast Cancer in the Spinal Vertebral Body | Device: ZetaFuse™ Bone Graft | Not Applicable | September 2023 | [119] |
| NCT05493228 | The Role of Dexmedetomidine (Precedex) Infusion on Intraoperative Propofol & Fentanyl Requirements in Spine Surgery for Pediatric Cancer Patients | Drug: Precedex Injectable Product Drug: Saline | Phase 3 | 30 October 2023 | [120] |
| NCT05467540 | Clinical Study of SPINERY™ A Novel Radio-Frequency Tumor Ablation Device for Spine Metastatic Tumors | Device: SPINERY | Not Applicable | 30 November 2023 | [121] |
| NCT04218617 | Single- vs. Two-Fraction Spine Stereotactic Radiosurgery for the Treatment of Vertebral Metastases | Device: Diagnostic MRI Device: Planning MRI Other: Simulation CT Other: QOL assessment Other: Brief pain inventory (BPI) Radiation: sSRS in 1 fraction Radiation: sSRS in 2 fraction | Phase 2 | 1 January 2024 | [122] |
| NCT05427825 | Anesthetic Protocols for Enhance Recovery After Metastatic Spine Tumor Resection Surgery: A Randomized Controlled Trial | Other: ERAS anesthetic care Other: Standard anesthetic care | Not Applicable | January 2024 | [123] |
| NCT04033536 | A Prospective Randomized Trial of Involved Versus Elective Target Definition in Stereotactic Spine Radiosurgery for Spinal Metastases | Radiation: Involved Target Stereotactic Spine Radiosurgery Radiation: Elective Target Stereotactic Spine Radiosurgery | Not Applicable | June 2024 | [124] |
| NCT04375891 | Randomized Phase II Study of Radiation Therapy Alone Versus Radiation Therapy Plus Radiofrequency Ablation (RFA)/Vertebral Augmentation for Localized Spine Metastasis | Radiation: Radiation Therapy Radiation: Radiofrequency Ablation (RFA) | Not Applicable | 1 September 2024 | [125] |
| NCT05023772 | A Clinical Trial Evaluating the Efficacy of Combining Laser Interstitial Thermal Ablation with and Without Spine Stereotactic Radiosurgery for Patients with Spine Metastases | Procedure: Stereotactic Laser Ablation Radiation: Stereotactic Radiosurgery Diagnostic Test: MRI guided laser ablation | Not Applicable | September 2024 | [126] |
| NCT05396222 | A Prospective Study of the Safety and Efficacy of 3D-printed Custom-made Non-rigid Biomimetic Implant for Anterior Column Reconstruction in Cervical and Thoracolumbar Spine | Device: 3D-printed custom-made non-rigid biomimetic implant | Not Applicable | 4 February 2025 | [127] |
| NCT05317026 | Pre-irradiation Vertebroplasty in Patients with Spine Metastases Candidates for SBRT vs. SBRT Alone: Increased Early Pain Relief | Procedure: Vertebroplasty Procedure: Stereotactic Body Radiation Therapy only | Not Applicable | 31 December 2025 | [128] |
| NCT04802603 | Dose-Escalated Spine SbRT (DESSRT) for Localized Metastasis to the Spinal Column | Radiation: Spine stereotactic body radiotherapy | Not Applicable | 31 December 2026 | [129] |
| NCT05495399 | Surgery for Limited Spine Metastases Followed by Conventional Radiotherapy or Stereotactic Body Radiation Therapy | Procedure: Spondylectomy Radiation: SBRT | Not Applicable | July 2027 | [130] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costăchescu, B.; Niculescu, A.-G.; Iliescu, B.F.; Dabija, M.G.; Grumezescu, A.M.; Rotariu, D. Current and Emerging Approaches for Spine Tumor Treatment. Int. J. Mol. Sci. 2022, 23, 15680. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms232415680
Costăchescu B, Niculescu A-G, Iliescu BF, Dabija MG, Grumezescu AM, Rotariu D. Current and Emerging Approaches for Spine Tumor Treatment. International Journal of Molecular Sciences. 2022; 23(24):15680. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms232415680
Chicago/Turabian StyleCostăchescu, Bogdan, Adelina-Gabriela Niculescu, Bogdan Florin Iliescu, Marius Gabriel Dabija, Alexandru Mihai Grumezescu, and Daniel Rotariu. 2022. "Current and Emerging Approaches for Spine Tumor Treatment" International Journal of Molecular Sciences 23, no. 24: 15680. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms232415680