
The Role of Vitamin D in Sleep Disorders of Children and Adolescents: A Systematic Review


Abstract
:1. Introduction
1.1. Vitamin D and the Serotonergic System
1.2. Vitamin D and the Dopaminergic System
2. Materials and Methods
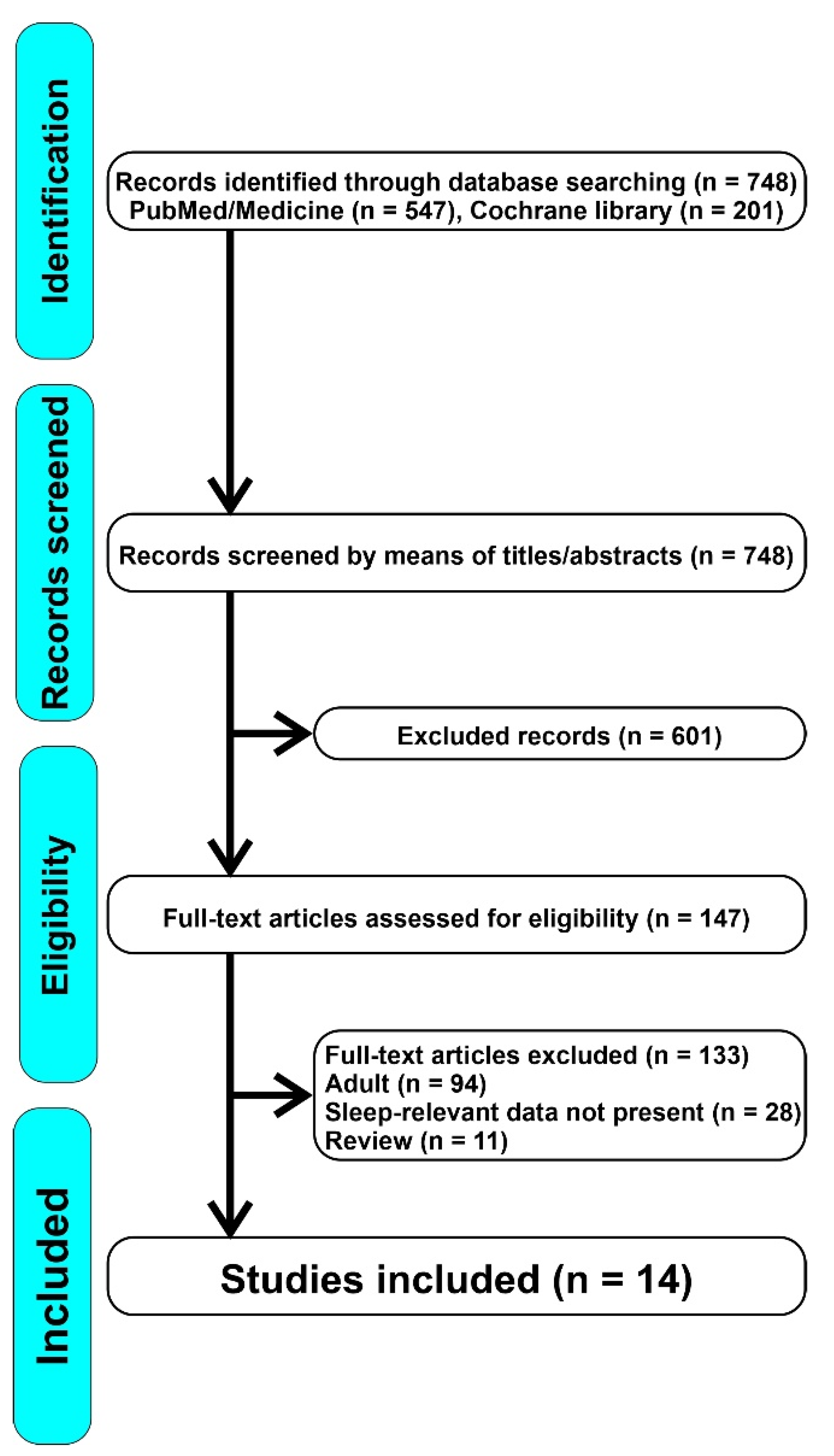
2.1. Search Strategies and Selection of the Studies
2.2. Data Extraction and Quality Assessment
3. Results and Discussion
3.1. Vitamin D and Sleep Duration and Quality of Sleep
3.1.1. Association between Sleep Duration and Plasma Vitamin D Levels in Children
3.1.2. Correlation between Cord Blood Vit D Levels and Sleep Features of Preschool Children
3.2. Vitamin D and OSA
3.3. Other Studies on Specific Diseases
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.M.; DePeter, K.C.; Feldman, H.A.; Grace, E.; Emans, S.J. Prevalence of Vitamin D Deficiency Among Healthy Adolescents. Arch. Pediatr. Adolesc. Med. 2004, 158, 531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulie, T.; Groff, A.; Redmer, J.; Hounshell, J.; Schrager, S. Vitamin D: An Evidence-Based Review. J. Am. Board Fam. Med. 2009, 22, 698–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evatt, M.L. Vitamin D Associations and Sleep Physiology—Promising Rays of Information. Sleep 2015, 38, 171–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gominak, S.C.; Stumpf, W.E. The world epidemic of sleep disorders is linked to vitamin D deficiency. Med. Hypotheses 2012, 79, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Archontogeorgis, K.; Nena, E.; Steiropoulos, P. Linking Vitamin D and Sleep. In Neurological Modulation of Sleep; Elsevier: Amsterdam, The Netherlands, 2020; pp. 385–399. ISBN 978-0-12-816658-1. [Google Scholar]
- Muscogiuri, G.; Barrea, L.; Scannapieco, M.; Di Somma, C.; Scacchi, M.; Aimaretti, G.; Savastano, S.; Colao, A.; Marzullo, P. The lullaby of the sun: The role of vitamin D in sleep disturbance. Sleep Med. 2019, 54, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, W.E.; O’Brien, L.P. 1,25(OH)2 vitamin D3 sites of action in the brain: An autoradiographic study. Histochemistry 1987, 87, 393–406. [Google Scholar] [CrossRef]
- Eyles, D.W.; Smith, S.; Kinobe, R.; Hewison, M.; McGrath, J.J. Distribution of the Vitamin D receptor and 1α-hydroxylase in human brain. J. Chem. Neuroanat. 2005, 29, 21–30. [Google Scholar] [CrossRef]
- Muzur, A.; Pace-Schott, E.F.; Hobson, J.A. The prefrontal cortex in sleep. Trends Cogn. Sci. 2002, 6, 475–481. [Google Scholar] [CrossRef]
- Macey, P.M.; Henderson, L.A.; Macey, K.E.; Alger, J.R.; Frysinger, R.C.; Woo, M.A.; Harper, R.K.; Yan-Go, F.L.; Harper, R.M. Brain Morphology Associated with Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2002, 166, 1382–1387. [Google Scholar] [CrossRef] [PubMed]
- Cameron, H.A.; Mckay, R.D.G. Adult neurogenesis produces a large pool of new granule cells in the dentate gyrus. J. Comp. Neurol. 2001, 435, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Guzmán-Marín, R.; Suntsova, N.; Stewart, D.R.; Gong, H.; Szymusiak, R.; McGinty, D. Sleep Deprivation Reduces Proliferation of Cells in the Dentate Gyrus of the Hippocampus in Rats. J. Physiol. 2003, 549, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Stoffers, D.; Altena, E.; van der Werf, Y.D.; Sanz-Arigita, E.J.; Voorn, T.A.; Astill, R.G.; Strijers, R.L.M.; Waterman, D.; Van Someren, E.J.W. The caudate: A key node in the neuronal network imbalance of insomnia? Brain 2014, 137, 610–620. [Google Scholar] [CrossRef] [Green Version]
- Marks, G.A.; Roffwarg, H.P.; Shaffery, J.P. Neuronal activity in the lateral geniculate nucleus associated with ponto-geniculo-occipital waves lacks lamina specificity. Brain Res. 1999, 815, 21–28. [Google Scholar] [CrossRef]
- Lima, M.M.S.; Andersen, M.L.; Reksidler, A.B.; Vital, M.A.B.F.; Tufik, S. The Role of the Substantia Nigra Pars Compacta in Regulating Sleep Patterns in Rats. PLoS ONE 2007, 2, e513. [Google Scholar] [CrossRef] [Green Version]
- Bivona, G.; Gambino, C.M.; Iacolino, G.; Ciaccio, M. Vitamin D and the nervous system. Neurol. Res. 2019, 41, 827–835. [Google Scholar] [CrossRef]
- Brown, A.J.; Slatopolsky, E. Vitamin D analogs: Therapeutic applications and mechanisms for selectivity. Mol. Aspects Med. 2008, 29, 433–452. [Google Scholar] [CrossRef]
- Cohen-Lahav, M.; Shany, S.; Tobvin, D.; Chaimovitz, C.; Douvdevani, A. Vitamin D decreases NFκB activity by increasing IκBα levels. Nephrol. Dial. Transplant. 2006, 21, 889–897. [Google Scholar] [CrossRef] [Green Version]
- Dong, X.; Craig, T.; Xing, N.; Bachman, L.A.; Paya, C.V.; Weih, F.; McKean, D.J.; Kumar, R.; Griffin, M.D. Direct Transcriptional Regulation of RelB by 1α,25-Dihydroxyvitamin D3 and Its Analogs. J. Biol. Chem. 2003, 278, 49378–49385. [Google Scholar] [CrossRef] [Green Version]
- McCarty, D.E.; Chesson, A.L.; Jain, S.K.; Marino, A.A. The link between vitamin D metabolism and sleep medicine. Sleep Med. Rev. 2014, 18, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Ryan, S.; McNicholas, W.T.; Taylor, C.T. A critical role for p38 map kinase in NF-κB signaling during intermittent hypoxia/reoxygenation. Biochem. Biophys. Res. Commun. 2007, 355, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Aranow, C. Vitamin D and the Immune System. J. Investig. Med. 2011, 59, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besedovsky, L.; Lange, T.; Haack, M. The Sleep-Immune Crosstalk in Health and Disease. Physiol. Rev. 2019, 99, 1325–1380. [Google Scholar] [CrossRef] [Green Version]
- Sochal, M.; Małecka-Panas, E.; Gabryelska, A.; Talar-Wojnarowska, R.; Szmyd, B.; Krzywdzińska, M.; Białasiewicz, P. Determinants of Sleep Quality in Inflammatory Bowel Diseases. J. Clin. Med. 2020, 9, 2921. [Google Scholar] [CrossRef]
- Golan, D.; Staun-Ram, E.; Glass-Marmor, L.; Lavi, I.; Rozenberg, O.; Dishon, S.; Barak, M.; Ish-Shalom, S.; Miller, A. The influence of vitamin D supplementation on melatonin status in patients with multiple sclerosis. Brain. Behav. Immun. 2013, 32, 180–185. [Google Scholar] [CrossRef]
- Basoli, V.; Santaniello, S.; Cruciani, S.; Ginesu, G.; Cossu, M.; Delitala, A.; Serra, P.; Ventura, C.; Maioli, M. Melatonin and Vitamin D Interfere with the Adipogenic Fate of Adipose-Derived Stem Cells. Int. J. Mol. Sci. 2017, 18, 981. [Google Scholar] [CrossRef] [Green Version]
- Maria, S.; Witt-Enderby, P.A. Melatonin effects on bone: Potential use for the prevention and treatment for osteopenia, osteoporosis, and periodontal disease and for use in bone-grafting procedures. J. Pineal Res. 2014, 56, 115–125. [Google Scholar] [CrossRef]
- Costello, R.B.; Lentino, C.V.; Boyd, C.C.; O’Connell, M.L.; Crawford, C.C.; Sprengel, M.L.; Deuster, P.A. The effectiveness of melatonin for promoting healthy sleep: A rapid evidence assessment of the literature. Nutr. J. 2014, 13, 106. [Google Scholar] [CrossRef] [Green Version]
- Galano, A.; Tan, D.-X.; Reiter, R. Melatonin: A Versatile Protector against Oxidative DNA Damage. Molecules 2018, 23, 530. [Google Scholar] [CrossRef] [Green Version]
- Galano, A.; Tan, D.X.; Reiter, R.J. On the free radical scavenging activities of melatonin’s metabolites, AFMK and AMK. J. Pineal Res. 2013, 54, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Rastegar Moghaddam Mansouri, M.; Abbasian, S.; Khazaie, M. Melatonin and Exercise: Their Effects on Malondialdehyde and Lipid Peroxidation. In Melatonin-Molecular Biology, Clinical and Pharmaceutical Approaches; Manuela Drăgoi, C., Crenguţa Nicolae, A., Eds.; IntechOpen: London, UK, 2018. [Google Scholar]
- Favero, G.; Franceschetti, L.; Bonomini, F.; Rodella, L.F.; Rezzani, R. Melatonin as an Anti-Inflammatory Agent Modulating Inflammasome Activation. Int. J. Endocrinol. 2017, 2017, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, J.-X.; Lee, S.; Taweechaipaisankul, A.; Kim, G.A.; Lee, B.C. Melatonin regulates lipid metabolism in porcine oocytes. J. Pineal Res. 2017, 62, e12388. [Google Scholar] [CrossRef] [PubMed]
- Garaulet, M.; Qian, J.; Florez, J.C.; Arendt, J.; Saxena, R.; Scheer, F.A.J.L. Melatonin Effects on Glucose Metabolism: Time To Unlock the Controversy. Trends Endocrinol. Metab. 2020, 31, 192–204. [Google Scholar] [CrossRef] [PubMed]
- Owino, S.; Buonfiglio, D.D.C.; Tchio, C.; Tosini, G. Melatonin Signaling a Key Regulator of Glucose Homeostasis and Energy Metabolism. Front. Endocrinol. 2019, 10, 488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekmekcioglu, C. Melatonin receptors in humans: Biological role and clinical relevance. Biomed. Pharmacother. 2006, 60, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Tordjman, S.; Chokron, S.; Delorme, R.; Charrier, A.; Bellissant, E.; Jaafari, N.; Fougerou, C. Melatonin: Pharmacology, Functions and Therapeutic Benefits. Curr. Neuropharmacol. 2017, 15, 434–443. [Google Scholar] [CrossRef]
- Slominski, R.M.; Reiter, R.J.; Schlabritz-Loutsevitch, N.; Ostrom, R.S.; Slominski, A.T. Melatonin membrane receptors in peripheral tissues: Distribution and functions. Mol. Cell. Endocrinol. 2012, 351, 152–166. [Google Scholar] [CrossRef] [Green Version]
- Häfner, R.; Truckenbrodt, H.; Spamer, M. 10 Rehabilitation in children with juvenile chronic arthritis. Baillières Clin. Rheumatol. 1998, 12, 329–361. [Google Scholar] [CrossRef]
- Liu, X.I.; Dallmann, A.; Wang, Y.-M.; Green, D.J.; Burnham, J.M.; Chiang, B.; Wu, P.; Sheng, M.; Lu, K.; van den Anker, J.N.; et al. Monoclonal Antibodies and Fc-Fusion Proteins for Pediatric Use: Dosing, Immunogenicity, and Modeling and Simulation in Data Submitted to the US Food and Drug Administration. J. Clin. Pharmacol. 2019, 59, 1130–1143. [Google Scholar] [CrossRef] [Green Version]
- Monti, J.M. Serotonin control of sleep-wake behavior. Sleep Med. Rev. 2011, 15, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y. Tryptophan metabolism in animals important roles in nutrition and health. Front. Biosci. 2011, S3, 286–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarris, J.; Byrne, G.J. A systematic review of insomnia and complementary medicine. Sleep Med. Rev. 2011, 15, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Paredes, S.D.; Barriga, C.; Reiter, R.J.; Rodríguez, A.B. Assessment of the Potential Role of Tryptophan as the Precursor of Serotonin and Melatonin for the Aged Sleep-wake Cycle and Immune Function: Streptopelia Risoria as a Model. Int. J. Tryptophan Res. 2009, 2, 23–36. [Google Scholar] [CrossRef] [Green Version]
- Garau, C.; Aparicio, S.; Rial, R.; Nicolau, M.; Esteban, S. Age-related changes in circadian rhythm of serotonin synthesis in ring doves: Effects of increased tryptophan ingestion. Exp. Gerontol. 2006, 41, 40–48. [Google Scholar] [CrossRef] [PubMed]
- González, S.; Moreno-Delgado, D.; Moreno, E.; Pérez-Capote, K.; Franco, R.; Mallol, J.; Cortés, A.; Casadó, V.; Lluís, C.; Ortiz, J.; et al. Circadian-Related Heteromerization of Adrenergic and Dopamine D4 Receptors Modulates Melatonin Synthesis and Release in the Pineal Gland. PLoS Biol. 2012, 10, e1001347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penckofer, S.; Byrn, M.; Adams, W.; Emanuele, M.A.; Mumby, P.; Kouba, J.; Wallis, D.E. Vitamin D Supplementation Improves Mood in Women with Type 2 Diabetes. J. Diabetes Res. 2017, 2017, 1–11. [Google Scholar] [CrossRef]
- Patrick, R.P.; Ames, B.N. Vitamin D and the omega-3 fatty acids control serotonin synthesis and action, part 2: Relevance for ADHD, bipolar disorder, schizophrenia, and impulsive behavior. FASEB J. 2015, 29, 2207–2222. [Google Scholar] [CrossRef] [Green Version]
- Huiberts, L.M.; Smolders, K.C.H.J. Effects of vitamin D on mood and sleep in the healthy population: Interpretations from the serotonergic pathway. Sleep Med. Rev. 2021, 55, 101379. [Google Scholar] [CrossRef]
- Bertone-Johnson, E.R. Vitamin D and the occurrence of depression: Causal association or circumstantial evidence? Nutr. Rev. 2009, 67, 481–492. [Google Scholar] [CrossRef]
- Patrick, R.P.; Ames, B.N. Vitamin D hormone regulates serotonin synthesis. Part 1: Relevance for autism. FASEB J. 2014, 28, 2398–2413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutknecht, L.; Kriegebaum, C.; Waider, J.; Schmitt, A.; Lesch, K.-P. Spatio-temporal expression of tryptophan hydroxylase isoforms in murine and human brain: Convergent data from Tph2 knockout mice. Eur. Neuropsychopharmacol. 2009, 19, 266–282. [Google Scholar] [CrossRef] [PubMed]
- Crockett, M.J. The Neurochemistry of Fairness: Clarifying the Link between Serotonin and Prosocial Behavior. Ann. N. Y. Acad. Sci. 2009, 1167, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Austin, M.C.; O’Donnell, S.M. Regional Distribution and Cellular Expression of Tryptophan Hydroxylase Messenger RNA in Postmortem Human Brainstem and Pineal Gland. J. Neurochem. 2008, 72, 2065–2073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, P.D.; Pontrello, C.; Burke, S. Robust and tissue-specific expression of TPH2 versus TPH1 in rat raphe and pineal gland. Biol. Psychiatry 2004, 55, 428–433. [Google Scholar] [CrossRef]
- Cajochen, C. Alerting effects of light. Sleep Med. Rev. 2007, 11, 453–464. [Google Scholar] [CrossRef]
- Kaneko, I.; Sabir, M.S.; Dussik, C.M.; Whitfield, G.K.; Karrys, A.; Hsieh, J.-C.; Haussler, M.R.; Meyer, M.B.; Pike, J.W.; Jurutka, P.W. 1,25-Dihydroxyvitamin D regulates expression of the tryptophan hydroxylase 2 and leptin genes: Implication for behavioral influences of vitamin D. FASEB J. 2015, 29, 4023–4035. [Google Scholar] [CrossRef]
- Wrzosek, M.; Łukaszkiewicz, J.; Wrzosek, M.; Jakubczyk, A.; Matsumoto, H.; Piątkiewicz, P.; Radziwoń-Zaleska, M.; Wojnar, M.; Nowicka, G. Vitamin D and the central nervous system. Pharmacol. Rep. 2013, 65, 271–278. [Google Scholar] [CrossRef]
- Cui, X.; Pelekanos, M.; Liu, P.-Y.; Burne, T.H.J.; McGrath, J.J.; Eyles, D.W. The vitamin D receptor in dopamine neurons; its presence in human substantia nigra and its ontogenesis in rat midbrain. Neuroscience 2013, 236, 77–87. [Google Scholar] [CrossRef]
- Oran, M.; Albayrak, Y.; Tulubas, F.; Oguz, K.; Avci, O.; Turgut, N.; Alp, R.; Unsal, C.; Gurel, A. Possible association between vitamin D deficiency and restless legs syndrome. Neuropsychiatr. Dis. Treat. 2014, 10, 953. [Google Scholar] [CrossRef] [Green Version]
- Shinpo, K.; Kikuchi, S.; Sasaki, H.; Moriwaka, F.; Tashiro, K. Effect of 1,25-dihydroxyvitamin D3 on cultured mesencephalic dopaminergic neurons to the combined toxicity caused by L-buthionine sulfoximine and 1-methyl-4-phenylpyridine. J. Neurosci. Res. 2000, 62, 374–382. [Google Scholar] [CrossRef]
- Ibi, M.; Sawada, H.; Nakanishi, M.; Kume, T.; Katsuki, H.; Kaneko, S.; Shimohama, S.; Akaike, A. Protective effects of 1α,25-(OH)2D3 against the neurotoxicity of glutamate and reactive oxygen species in mesencephalic culture. Neuropharmacology 2001, 40, 761–771. [Google Scholar] [CrossRef]
- Evatt, M.L.; DeLong, M.R.; Khazai, N.; Rosen, A.; Triche, S.; Tangpricha, V. Prevalence of Vitamin D Insufficiency in Patients With Parkinson Disease and Alzheimer Disease. Arch. Neurol. 2008, 65, 1348–1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, K.; Wang, W.; Kang, U.J. The Role of Glutathione in Dopaminergic Neuronal Survival. J. Neurochem. 2002, 69, 1850–1858. [Google Scholar] [CrossRef] [PubMed]
- Ibi, M.; Sawada, H.; Kume, T.; Katsuki, H.; Kaneko, S.; Shimohama, S.; Akaike, A. Depletion of Intracellular Glutathione Increases Susceptibility to Nitric Oxide in Mesencephalic Dopaminergic Neurons. J. Neurochem. 2002, 73, 1696–1703. [Google Scholar] [CrossRef] [Green Version]
- Garcion, E.; Sindji, L.; Leblondel, G.; Brachet, P.; Darcy, F. 1,25-Dihydroxyvitamin D3 Regulates the Synthesis of γ-Glutamyl Transpeptidase and Glutathione Levels in Rat Primary Astrocytes. J. Neurochem. 2002, 73, 859–866. [Google Scholar] [CrossRef]
- Jenner, P.; Olanow, C.W. Oxidative stress and the pathogenesis of Parkinson’s disease. Neurology 1996, 47, 161S–170S. [Google Scholar] [CrossRef]
- Bollu, P.C.; Yelam, A.; Thakkar, M.M. Sleep Medicine: Restless Legs Syndrome. Mo. Med. 2018, 115, 380. [Google Scholar]
- Çakır, T.; Doğan, G.; Subaşı, V.; Filiz, M.B.; Ülker, N.; Doğan, Ş.K.; Toraman, N.F. An evaluation of sleep quality and the prevalence of restless leg syndrome in vitamin D deficiency. Acta Neurol. Belg. 2015, 115, 623–627. [Google Scholar] [CrossRef]
- Balaban, H.; Yıldız, Ö.K.; Çil, G.; Şentürk, İ.A.; Erselcan, T.; Bolayır, E.; Topaktaş, S. Serum 25-hydroxyvitamin D levels in restless legs syndrome patients. Sleep Med. 2012, 13, 953–957. [Google Scholar] [CrossRef]
- Yoon, J.W.; Kim, S.W.; Yoo, E.G.; Kim, M.K. Prevalence and risk factors for vitamin D deficiency in children with iron deficiency anemia. Korean J. Pediatr. 2012, 55, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kheirandish-Gozal, L.; Peris, E.; Gozal, D. Vitamin D levels and obstructive sleep apnoea in children. Sleep Med. 2014, 15, 459–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Shawwa, B.; Ehsan, Z.; Ingram, D.G. Vitamin D and sleep in children. J. Clin. Sleep Med. 2020, 16, 5. [Google Scholar] [CrossRef] [PubMed]
- Gong, Q.-H.; Li, S.-X.; Li, H.; Chen, Q.; Li, X.-Y.; Xu, G.-Z. 25-Hydroxyvitamin D Status and Its Association with Sleep Duration in Chinese Schoolchildren. Nutrients 2018, 10, 1013. [Google Scholar] [CrossRef] [Green Version]
- Sung, M.; Rhie, S.; Kim, J.H.; Lee, S.W.; Ha, E.K.; Jee, H.M.; Yoo, E.-G.; Chae, K.Y.; Han, M.Y. Assessment of vitamin D, exercise, and lipid profile associated with excessive daytime sleepiness in school children. Sleep Med. 2021, 77, 51–57. [Google Scholar] [CrossRef]
- Valtuena, J.; Gonzalez-Gross, M.; Huybrechts, I.; Breidenassel, C.; Ferrari, M.; Mouratidou, T.; Gottrand, F.; Dallongeville, J.; Azzini, E.; Sioen, I.; et al. Factors Associated with Vitamin D Deficiency in European Adolescents: The HELENA Study. J. Nutr. Sci. Vitaminol. 2013, 59, 161–171. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Qin, R.; Hong, H.; Lv, H.; Ye, K.; Wei, Y.; Zheng, W.; Qi, H.; Ni, Y.; Zhang, L.; et al. Vitamin D status and its dietary and lifestyle factors in children during the first 5 years of life: A cross-sectional multicentre Jiangsu bone study. J. Hum. Nutr. Diet. 2021, 34, 792–806. [Google Scholar] [CrossRef]
- Yong, C.Y.; Reynaud, E.; Forhan, A.; Dargent-Molina, P.; Heude, B.; Charles, M.-A.; Plancoulaine, S.; Annesi-Maesano, I.; Bernard, J.Y.; Botton, J.; et al. Cord-blood vitamin D level and night sleep duration in preschoolers in the EDEN mother-child birth cohort. Sleep Med. 2019, 53, 70–74. [Google Scholar] [CrossRef] [Green Version]
- Deng, Y.; Wang, G.; Ye, X.; Jiang, Y.; Lin, Q.; Dong, S.; Song, Y.; Zhu, L.; Meng, M.; Li, W.; et al. The association between 25-hydroxyvitamin D levels and children’s sleep-wake patterns: A prospective cohort study. Sleep Med. 2020, 67, 207–214. [Google Scholar] [CrossRef]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Sheldon, S.H.; Spruyt, K.; Ward, S.D.; et al. Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome. Pediatrics 2012, 130, 576–584. [Google Scholar] [CrossRef] [Green Version]
- Marcus, C.L.; Greene, M.G.; Carroll, J.L. Blood Pressure in Children with Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 1998, 157, 1098–1103. [Google Scholar] [CrossRef] [PubMed]
- Beebe, D.W.; Ris, M.D.; Kramer, M.E.; Long, E.; Amin, R. The Association Between Sleep Disordered Breathing, Academic Grades, and Cognitive and Behavioral Functioning Among Overweight Subjects During Middle to Late Childhood. Sleep 2010, 33, 1447–1456. [Google Scholar] [CrossRef] [Green Version]
- Ozgurhan, G.; Vehapoglu, A.; Vermezoglu, O.; Temiz, R.N.; Guney, A.; Hacihamdioglu, B. Risk assessment of obstructive sleep apnea syndrome in pediatric patients with vitamin D deficiency: A questionnaire-based study. Medicine 2016, 95, e4632. [Google Scholar] [CrossRef] [PubMed]
- Hewison, M. Vitamin D and immune function: An overview. Proc. Nutr. Soc. 2012, 71, 50–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zicari, A.M.; Occasi, F.; Di Mauro, F.; Lollobrigida, V.; Di Fraia, M.; Savastano, V.; Loffredo, L.; Nicita, F.; Spalice, A.; Duse, M. Mean Platelet Volume, Vitamin D and C Reactive Protein Levels in Normal Weight Children with Primary Snoring and Obstructive Sleep Apnea Syndrome. PLoS ONE 2016, 11, e0152497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tauman, R.; Ivanenko, A.; O’Brien, L.M.; Gozal, D. Plasma C-Reactive Protein Levels Among Children With Sleep-Disordered Breathing. Pediatrics 2004, 113, e564–e569. [Google Scholar] [CrossRef] [Green Version]
- Gozal, D.; Crabtree, V.M.; Sans Capdevila, O.; Witcher, L.A.; Kheirandish-Gozal, L. C-reactive Protein, Obstructive Sleep Apnea, and Cognitive Dysfunction in School-aged Children. Am. J. Respir. Crit. Care Med. 2007, 176, 188–193. [Google Scholar] [CrossRef] [Green Version]
- Cui, P.; Ge, L.; Li, J. Study on the Improvement of Behavioral and Cognitive Dysfunction of Children with OSAHS by Vitamin D. BioMed Res. Int. 2021, 2021, 1–6. [Google Scholar] [CrossRef]
- Rosenzweig, I.; Glasser, M.; Crum, W.R.; Kempton, M.J.; Milosevic, M.; McMillan, A.; Leschziner, G.D.; Kumari, V.; Goadsby, P.; Simonds, A.K.; et al. Changes in Neurocognitive Architecture in Patients with Obstructive Sleep Apnea Treated with Continuous Positive Airway Pressure. EBioMedicine 2016, 7, 221–229. [Google Scholar] [CrossRef] [Green Version]
- Barceló, A.; Morell-Garcia, D.; Ribot, C.; De la Peña, M.; Peña-Zarza, J.A.; Alonso-Fernández, A.; Giménez, P.; Piérola, J. Vitamin D as a biomarker of health in snoring children: A familial aggregation study. Pediatr. Res. 2021. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.R.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Işıkay, S.; Işıkay, N.; Per, H.; Çarman, K.B.; Kocamaz, H. Restless leg syndrome in children with celiac disease. Turk. J. Pediatr. 2018, 60, 70. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, R.M.K.; Balci, S.; Serbes, M.; Dogruel, D.; Altintas, D.U.; Yilmaz, M. Decreased serum vitamin B12 and vitamin D levels affect sleep quality in children with familial Mediterranean fever. Rheumatol. Int. 2018, 38, 83–87. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Objective | Design | Population | Methods | Results |
|---|---|---|---|---|---|
| Al-Shawwa et al. 2020 | Relationship between sleep architecture and vitD status. | Retrospective cohort study. | 39 children | PSG and pediatric sleep questionnaires. | 51 with vitD deficiency (25(OH)D < 30 ng/mL). Children with vitD deficiency: decreased TST and sleep efficiency, and later weekday and weekend bedtimes. |
| Deng et al., 2020 | Association between vit D in cord or venous blood and sleep–wake patterns at two years of age. | Prospective cohort study. | 29 children | 25(OH)D assessed in cord blood and venous blood at two years of age. Sleep–wake patterns measured with BISQ and Acti-Watch. | Venous but not cord blood 25(OH)D level at two years age positively associated with sleep duration. |
| Gong et al., 2018 | Association between 25(OH)D levels and sleep duration. | School-based prospective study. | 800 Chinese adolescents (8–14 years) | Anthropometric measured by trained research staff. Serum 25(OH)D and lipids measured in the laboratory. Sleep habits and health-related behaviors assessed by questionnaire. | 25(OH)D levels positively correlated with sleep duration. Insufficiency/deficiency of vitD (25(OH)D < 20 ng/mL) significantly associated with increased probability of short sleep. |
| Yong et al., 2019 | Association between cord-blood vitD levels at birth and night-sleep duration trajectories between 2 and 5–6 years old. | Cohort study. | 264 children | Cord-blood 25OHD determined by radio-immunoassay at birth, and night-sleep trajectories between 2 and 5–6 years obtained by group-based trajectory modeling method. Associations assessed by multinomial logistic regression adjusted for maternal and child characteristics. | Trajectories short sleep (<10.5 h) was found in 5%, medium–low sleep (10.5–11.0 h) in 46%, medium–high sleep (≈11.5 h) in 37%, long sleep (≥11.5 h) in 4% and changing sleep (decreased from ≥11.5 to 10.5–11.0 h) in 8%, respectively. The mean 25OHD level was 19, 12, 19, 14, and 16, respectively. On adjusted analysis, decrease in 25OHD level correlated with the odds of belonging to the shorter sleep trajectories. |
| Kheirandish-Gozal et al., 2014 | Association between OSA and plasma 25(OH)D and risk of metabolic dysfunction and systemic inflammation. | Observational cross-sectional study. | 176 obese and non-obese children with and without OSA | PSG and fasting blood draw the morning after. Lipid profile, homeostatic model of insulin resistance and high-sensitivity C-reactive protein assays and plasma 25(OH)D assessed. | 25(OH)D levels reduced in pediatric OSA (also in Afro American and in obese children); possible role in modulating the degree of insulin resistance and systemic inflammation. |
| Shin et al., 2018 | Relationship between vitD and associated factors in children ATH. | Retrospective cross-sectional study. | 88 children with sleep-disordered breathing | Four groups based on adenoidal and/or tonsillar hypertrophy. Demographic data, the sizes of tonsils and adenoids, serum 25(OH)D level, BMI, and allergen sensitization patterns. | Children with ATH had decreased 25(OH)D). Children with vitD deficiencies higher frequency of ATH. Inverse correlation between serum 25(OH)D levels and age, tonsil and adenoid size, and height. Tonsil and adenoid size, and BMI-z score associated with 25(OH)D levels, after controlling for age, sex, height, and mite sensitization. |
| Ekinci et al., 2017 | Serum vitB12 and vitD correlation with self-reported sleep quality of pediatric FMF patients. | Case-control study. | 63 children with FMF | Self-administered PSQI. The patients divided into subgroups depending on vitD concentrations (≥20 and <20 ng/mL) or to vitB12 concentration (≥200, <200 pg/mL). | vitB12 levels not correlated with PSQI scores. Significant correlation between vitD and total PSQI scores and daytime sleepiness. Total PSQI score, sleep disorders and daytime sleepiness sub-scores higher in patients with vitD < 20 ng/mL. vitD possibly protective against sleep disorders and poor sleep. |
| Zhao et al., 2021 | vitD status by demographic and lifestyle factors including dietary supplementation and physical activity. | Population based, cross-sectional, multicenter study. | 5289 children aged 0–5 years | Stratified cluster random-sampling method in 12 Children’s Health Care Centers from 10 cities in Jiangsu Province, China. | Prevalence of vitD deficiency 30.1%. Higher risk of vitD deficiency associated with: older age, girls, survey conducted in spring, location in southern Jiangsu province, residence in urban, outdoor activity < 2 h/day. Lower risk associated with: parity ≥ 2 times, vitD supplementation from birth to 6 months, vitD supplementation starting ≤ 1 month after birth, vitD and calcium supplementation in the last 3 months, and dose of vitD supplementation > 400 IU/day. Higher risk of vitD deficiency with preference for sweets, meat consumption > 150.0 g/day1, milk consumption < 250 mL/day, sleeping < 10 h/day. |
| Ozgurhan et al., 2016 | Risk of OSA in subjects with vitD deficiency. | Prospective and comparative study. | 176 obese and non-obese children with and without OSA | Two groups based on 25(OH)D levels: low level (<20 ng/mL) group (n = 120) and control (>20 ng/mL) group (n = 120). Risk of developing OSA assessed by Berlin Questionnaire. | No statistically significant differences between the low level and control groups in terms of gender, age, and BMI z-score distributions. 24 subjects with high risk of developing OSA (17 subjects in the low-level group and 7 subjects in the control group). Risk of developing OSA significantly higher in the low-level group. BMI z-score significantly higher in high-risk groups than low-risk groups. |
| Cui et al., 2021 | vitD in the treatment of children with OSA. | Case-control study. | 50 children: 30 with OSA, 20 controls | In all subjects: sex, age, triglyceride, total cholesterol, HDL, LDL, serum 25-OHD levels, and Conners’ parental scale were measured. In children with OSA: BMI, AHI, and minimum oxygen saturation. Children with OSA treated with Rocaltrol (0.25 g/QD) for 4 weeks and reanalyzing their triglycerides, total cholesterol, HDL, LDL, serum 25(OH)D levels, sleep AHI, minimum oxygen saturation, and Conners’ parental scale. | Children with OSA frequently obese, with dyslipidemia, and vitD deficiency, with behavioral and cognitive dysfunction. No significant changes in BMI, triglycerides, total cholesterol, HDL, LDL, sleep AHI, and minimum oxygen saturation after vitD treatment, but the serum 25-OHD level significantly improved, as well as conduct problems, learning problems, and hyperactivity index decreased. |
| Sung et al., 2020 | Factors associated with EDS and vitD level. | Case-control study. | 618 children: 111 with EDS and 507 healthy controls | Physical examination, acoustic rhinometry, and blood sampling. Parent-filled questionnaires. Korean version of Pediatric Daytime Sleepiness Scale (PDSS). | Children with low 25(OH)D3 (<20 ng/mL) and HDL-C (<40 mg/dL) levels with increased risk of EDS. 25(OH)D3 level, exercise, and BMI were over three. High levels of 25(OH)D3 and HDL cholesterol and performing regular exercise associated with decreased risk of EDS. |
| Valtuena et al., 2013 | Environmental, individual, and genetic factors associated with 25(OH)D levels. | Multi-center cross-sectional study. | 1006 children | Measures of body composition, biochemical markers, socioeconomic status, dietary intake, physical activity, fitness, sleep time, and vitamin D genetic polymorphism (rs1544410). | In males, 25(OH)D levels independently influenced by winter season, higher latitudes, BMI z-score and retinol concentration. In females, 25(OH)D levels independently influenced by winter season, sleep time, supplement intake, flexibility, body fat %, BMI z-score, higher latitudes, and handgrip strength. Season, latitude, fitness, adiposity, sleep time, and micronutrient supplementation were highly related to 25(OH)D concentrations. |
| Işıkay et al., 2018 | Prevalence and associated factors of RLS in children with CD. | Cross-sectional study: case-control study. | 494 children: 226 with CD and 268 controls | Demographic data, educational status and routine laboratory data of children including complete blood count, ferritin, vitB12, folate and 25(OH)D levels. RLS prevalence and associated symptoms by a 30-item questionnaire. | Prevalence of RLS not increased in children with CD. Age at onset of RLS symptoms significantly younger and more severe in CD. |
| Barceló et al., 2021 | Inter-relationship between serum 25(OH)D levels and metabolic profiles, sleep parameters, and paternal and maternal vitD status. | Familial longitudinal study. | 137 Caucasian families (children and their parents) | Measurement of serum 25(OH)D levels, serum glucose, lipids, liver enzymes, parathyroid hormone, insulin, and glycated hemoglobin and evaluation of overnight PSG. | VitD insufficiency (<30 ng/mL) and deficiency (<20 ng/mL) in 40.9% and 17.5%, respectively. Risk of vitD insufficiency increased by both paternal and maternal insufficiency. Serum 25(OH)D concentration associated with AHI and respiratory arousal index. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prono, F.; Bernardi, K.; Ferri, R.; Bruni, O. The Role of Vitamin D in Sleep Disorders of Children and Adolescents: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 1430. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23031430
Prono F, Bernardi K, Ferri R, Bruni O. The Role of Vitamin D in Sleep Disorders of Children and Adolescents: A Systematic Review. International Journal of Molecular Sciences. 2022; 23(3):1430. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23031430
Chicago/Turabian StyleProno, Federica, Katerina Bernardi, Raffaele Ferri, and Oliviero Bruni. 2022. "The Role of Vitamin D in Sleep Disorders of Children and Adolescents: A Systematic Review" International Journal of Molecular Sciences 23, no. 3: 1430. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23031430