
User Experience during an Immersive Virtual Reality-Based Cognitive Task: A Comparison between Estonian and Italian Older Adults with MCI

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Previous Work
3. Aims
- 1.
- To assess the user experience of an immersive VR-based application in a group of Estonian older adults with MCI, in order to evaluate whether it could be used, in the clinical practice, as a tool for the assessment and the training of visuospatial abilities;
- 2.
- To compare the Estonian older adults’ user experience, both at subjective (i.e., via standard questionnaires) and objective (i.e., performance) levels, to Italian older adults’ UX, obtained in a previous study [42]. Such a comparison could be meaningful to verify whether a different social, cultural, and economic background could (i) impact UX in general and (ii) assess which factors are mainly influenced.
4. Materials and Methods
4.1. Participants
4.2. Equipment
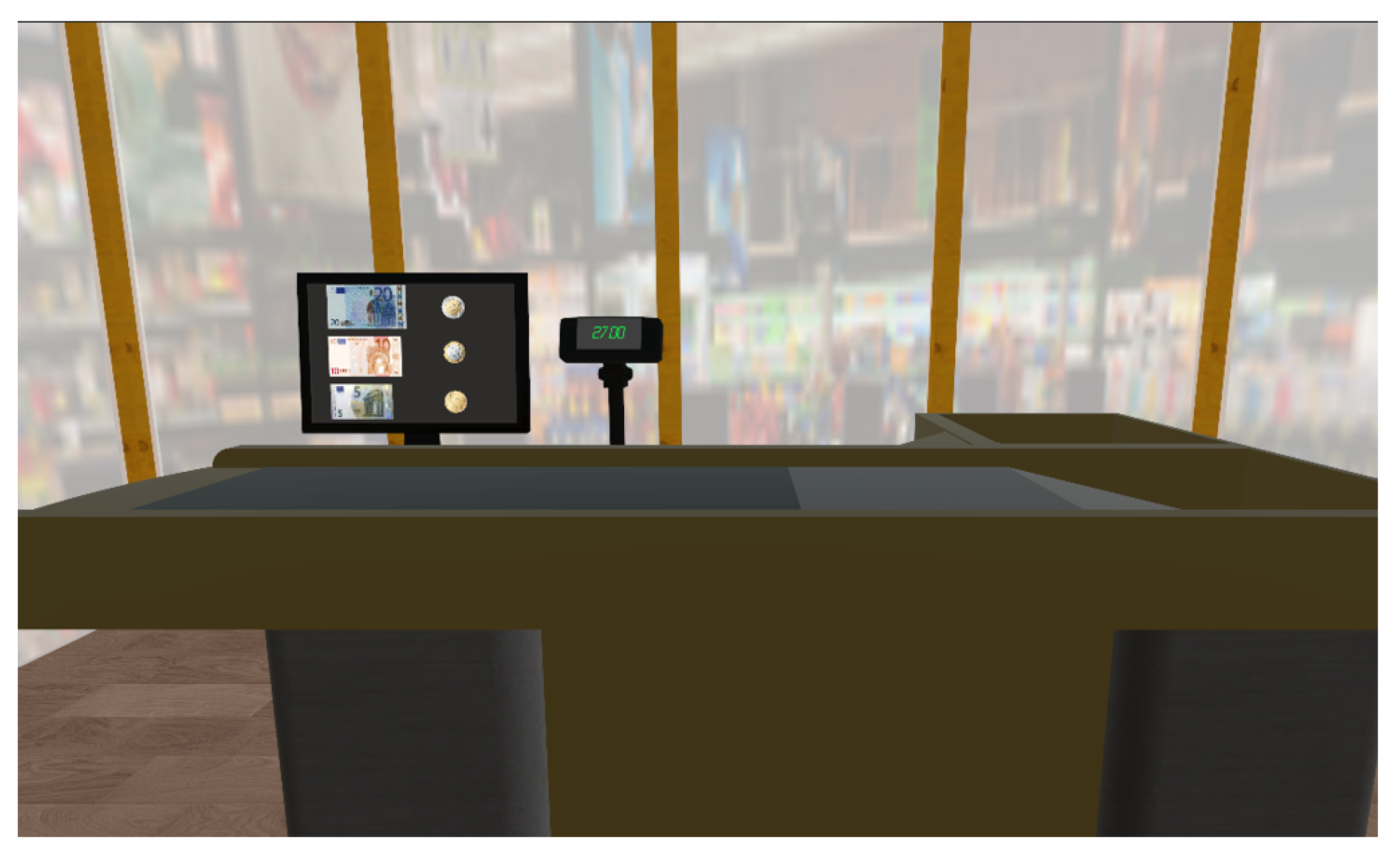
4.2.1. The Virtual Supermarket
4.2.2. Hardware
4.3. Study Protocol
4.4. Measures
4.4.1. Baseline Assessment
4.4.2. User Experience Evaluation
- Perceived ease of use (PEOU), i.e., the degree to which a person believes that the use of a system is easy (4 items),
- Computer anxiety (CANX), i.e., the individual apprehension that is perceived towards technology (4 items),
- Perceived enjoyment (ENJ), i.e., the extent to which the activity of using a system is perceived as enjoyable, regardless of the performance of the system itself (3 items),
- Behavioral intention (BI) (3 items), as before the experience.
4.4.3. Performance Variables
4.5. Statistical Analysis
5. Results
5.1. Subjective and Objective Variables’ Characteristics
5.2. Pre- and Post-Experience Differences
5.3. Correlation between Subjective Variables
5.4. Correlation between Subjective Variables and Performance
5.5. Spontaneous Comments and Clinicians’ Observations
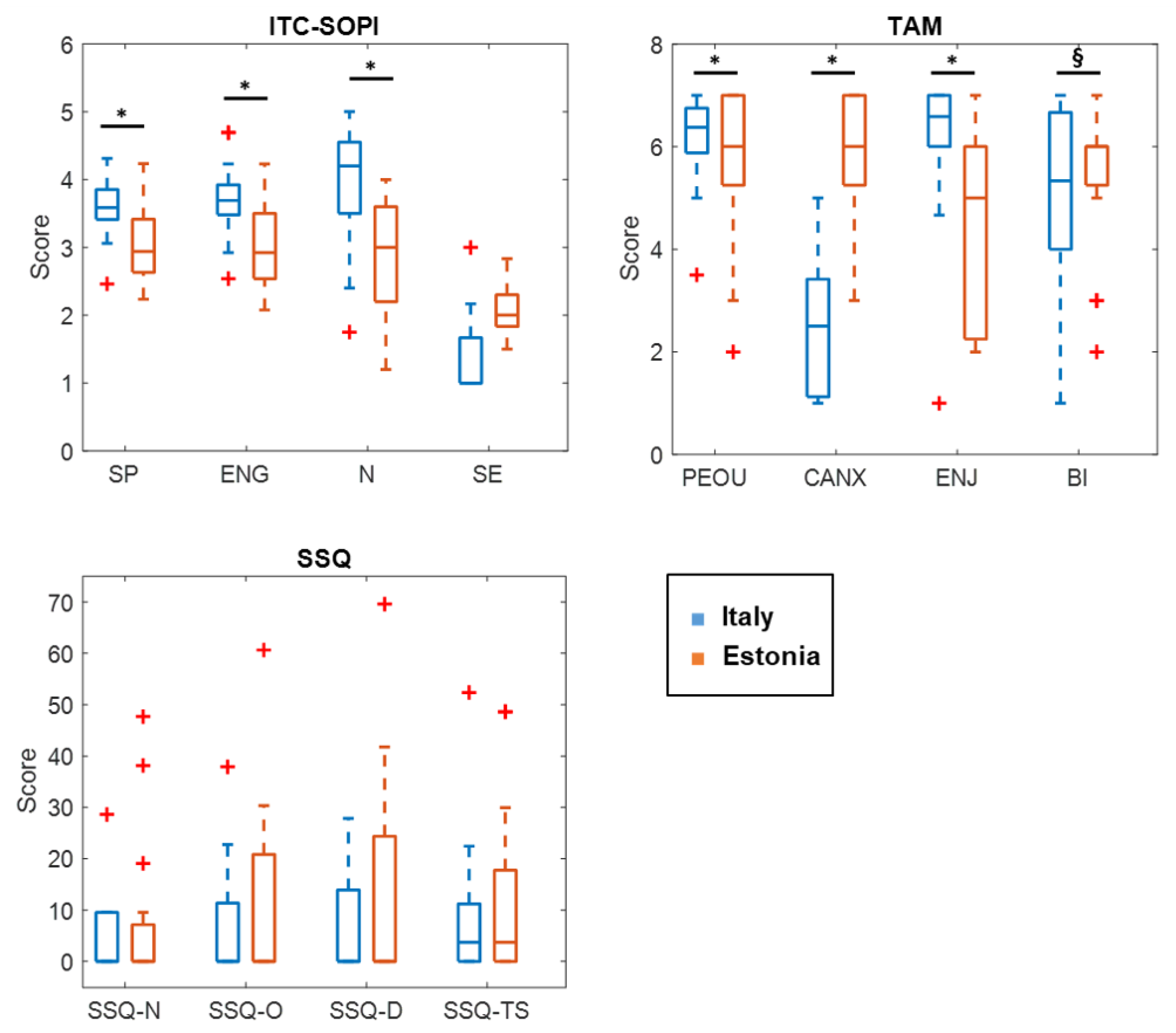
5.6. Differences with the Italian Participants
6. Discussion
7. Limitations
8. Conclusions and Future Work
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Orgeta, V.; Mukadam, N.; Sommerlad, A.; Livingston, G. The lancet commission on dementia prevention, intervention, and care: A call for action. Ir. J. Psychol. Med. 2019, 36, 85–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaz, M.; Silvestre, S. Alzheimer’s disease: Recent treatment strategies. Eur. J. Pharmacol. 2020, 887, 173554. [Google Scholar] [CrossRef] [PubMed]
- Golomb, J.; Kluger, A.; Ferris, S.H. Mild cognitive impairment: Historical development and summary of research. Dialogues Clin. Neurosci. 2022, 6, 351–367. [Google Scholar] [CrossRef]
- Lynch, C. World Alzheimer Report 2019: Attitudes to dementia, a global survey: Public health: Engaging people in ADRD research. Alzheimer’s Dement. 2020, 16, e038255. [Google Scholar] [CrossRef]
- Petersen, R.C.; Kokmen, E.; Smith, G.E.; Waring, S.C.; Kurland, L.T.; Ivnik, R.J.; Tangalos, E.G.; Schaid, D.J.; Thibodeau, S.N. Apolipoprotein E Status as a Predictor of the Development of Alzheimer’s Disease in Memory-Impaired Individuals. JAMA 1995, 273, 1274–1278. [Google Scholar] [CrossRef]
- Rivas-Vazquez, R.A.; Mendez, C.; Rey, G.J.; Carrazana, E.J. Mild cognitive impairment: New neuropsychological and pharmacological target. Arch. Clin. Neuropsychol. 2004, 19, 11–27. [Google Scholar] [CrossRef]
- Prince, M.; Knapp, M.; Guerchet, M.; McCrone, P.; Prina, M.; Comas-Herrera, A.; Wittenberg, R.; Adelaja, B.; Hu, B.; King, D.; et al. Dementia UK; Kings College London: London, UK, 2014. [Google Scholar]
- Standen, P.J.; Brown, D.J. Virtual reality in the rehabilitation of people with intellectual disabilities: Review. Cyberpsychol. Behav. Impact Internet Multimed. Virtual Real. Behav. Soc. 2005, 8, 272–282. [Google Scholar] [CrossRef]
- Sabbagh, M.N.; Boada, M.; Borson, S.; Chilukuri, M.; Dubois, B.; Ingram, J.; Iwata, A.; Porsteinsson, A.; Possin, K.; Rabinovici, G.; et al. Early detection of mild cognitive impairment (MCI) in primary care. J. Prev. Alzheimer’s Dis. 2020, 7, 165–170. [Google Scholar] [CrossRef]
- Lissek, V.; Suchan, B. Preventing dementia? Interventional approaches in mild cognitive impairment. Neurosci. Biobehav. Rev. 2021, 122, 143–164. [Google Scholar] [CrossRef]
- Rauschnabel, P.A.; Felix, R.; Hinsch, C.; Shahab, H.; Alt, F. What is XR? Towards a framework for augmented and virtual reality. Comput. Hum. Behav. 2022, 133, 107289. [Google Scholar] [CrossRef]
- Mann, S.; Furness, T.; Yuan, Y.; Iorio, J.; Wang, Z. All reality: Virtual, augmented, mixed (x), mediated (x, y), and multimediated reality. arXiv 2018, arXiv:1804.08386. [Google Scholar]
- Navarro, M.D.; Lloréns, R.; Noé, E.; Ferri, J.; Alcañiz, M. Validation of a low-cost virtual reality system for training street-crossing. A comparative study in healthy, neglected and non-neglected stroke individuals. Neuropsychol. Rehabil. 2013, 23, 597–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouellet, E.; Boller, B.; Corriveau-Lecavalier, B.; Cloutier, S.; Belleville, S. The Virtual Shop: A new immersive virtual reality environment and scenario for the assessment of everyday memory. J. Neurosci. Methods 2018, 303, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Tanis, E.S.; Palmer, S.B.; Wehmeyer, M.L.; Davies, D.; Stock, S.; Bishop, B. A Self-Report Computer-Based Survey of Technology Use by People with Intellectual and Developmental Disabilities Kathy Lobb, and Self-Advocate Coalition of Kansas. Intellect Dev. Disabil. 2012, 50, 53–68. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Wiederhold, B.K.; Wiederhold, M.D.; Kim, S.I.; Ku, J.; Cho, W.; Hahn, W.Y.; Kim, I.Y.; Lee, S.M.; Kang, Y.; et al. A virtual reality system for the assessment and rehabilitation of the activities of daily living. Cyberpsychol. Behav. Impact Internet Multimed. Virtual Real. Behav. Soc. 2003, 6, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Faria, A.L.; Andrade, A.; Soares, L.; I Badia, S.B. Benefits of virtual reality based cognitive rehabilitation through simulated activities of daily living: A randomized controlled trial with stroke patients. J. Neuroeng. Rehabil. 2016, 13, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2017, 2017, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharples, S.; Cobb, S.; Moody, A.; Wilson, J.R. Virtual reality induced symptoms and effects (VRISE): Comparison of head mounted display (HMD), desktop and projection display systems. Displays 2008, 29, 58–69. [Google Scholar] [CrossRef]
- Weech, S.; Kenny, S.; Barnett-Cowan, M. Presence and cybersickness in virtual reality are negatively related: A review. Front. Psychol. 2019, 10, 158. [Google Scholar] [CrossRef] [Green Version]
- Coldham, G.; Cook, D.M. VR usability from elderly cohorts: Preparatory challenges in overcoming technology rejection. In Proceedings of the 2017 National Information Technology Conference (NITC), Colombo, Sri Lanka, 13–15 September 2017; pp. 131–135. [Google Scholar] [CrossRef]
- Sagnier, C.; Loup-Escande, E.; Lourdeaux, D.; Thouvenin, I.; Valléry, G. User Acceptance of Virtual Reality: An Extended Technology Acceptance Model. Int. J. Hum. Comput. Interact. 2020, 36, 993–1007. [Google Scholar] [CrossRef]
- Helkama, K.; Verkasalo, M.; Myyry, L.; Silfver, M.; Niit, T.; Manganelli, A.M.; Andreeva, G.; Stefanenko, T.; Dubovskaya, E.; Tikhomandritskaya, O.; et al. Honor as a value in Finland, Estonia, Italy, Russia, and Switzerland. Group Process. Intergroup Relations 2013, 16, 279–297. [Google Scholar] [CrossRef]
- Smooha, S. How do western democracies cope with the challenge of societal diversity? Nations Natl. 2018, 24, 215–236. [Google Scholar] [CrossRef]
- Kreyenfeld, M.; Andersson, G.; Pailhé, A. Economic uncertainty and family dynamics in Europe: Introduction. Demogr. Res. 2012, 27, 835–852. [Google Scholar] [CrossRef] [Green Version]
- Trechsel, A.H.; Kies, R.; Mendez, F.; Schmitter, P.C. Evaluation of the Use of New Technologies in Order to Facilitate Democracy in Europe; C2D-Research and Documentation Centre on Direct Democracy: Aarau, Switzerland, 2003. [Google Scholar]
- Hasebrink, U.; Livingstone, S.; Haddon, L.; Olafsson, K. Comparing Children’s Online Opportunities and Risks Across Europe: Cross-National Comparisons for EU Kids Online; EU Kids Online: London, UK, 2009. [Google Scholar]
- Arlati, S.; Borghetti, D. XR and Neurorehabilitation. Roadmapping Extended Reality: Fundamentals and Applications; Wiley: Hoboken, NJ, USA, 2022; pp. 257–282. [Google Scholar]
- Mrakic-Sposta, S.; Di Santo, S.G.; Franchini, F.; Arlati, S.; Zangiacomi, A.; Greci, L.; Moretti, S.; Jesuthasan, N.; Marzorati, M.; Rizzo, G.; et al. Effects of combined physical and cognitive virtual reality-based training on cognitive impairment and oxidative stress in MCI patients: A pilot study. Front. Aging Neurosci. 2018, 10, 282. [Google Scholar] [CrossRef] [Green Version]
- Clay, F.; Howett, D.; FitzGerald, J.; Fletcher, P.; Chan, D.; Price, A. Use of Immersive Virtual Reality in the Assessment and Treatment of Alzheimer’s Disease: A Systematic Review. J. Alzheimer’s Dis. JAD 2020, 75, 23–43. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.C.; Yang, Y.H. The Long-term Effects of Immersive Virtual Reality Reminiscence in People With Dementia: Longitudinal Observational Study. JMIR Serious Games 2022, 10, e36720. [Google Scholar] [CrossRef]
- Boletsis, C.; McCallum, S. Augmented reality cubes for cognitive gaming: Preliminary usability and game experience testing. Int. J. Serious Games 2016, 3, 3–18. [Google Scholar] [CrossRef] [Green Version]
- Andrade Ferreira, L.D.; Cavaco, S.; Bermúdez i Badia, S. Feasibility Study of an Augmented Reality System for People with Dementia. In Proceedings of the ICAT-EGVE 2018—International Conference on Artificial Reality and Telexistence and Eurographics Symposium on Virtual Environments, Limassol, Cyprus, 7–9 November 2018; Bruder, G., Yoshimoto, S., Cobb, S., Eds.; The Eurographics Association: Goslar, Germany, 2018. [Google Scholar] [CrossRef]
- Sonntag, D. Kognit: Intelligent cognitive enhancement technology by cognitive models and mixed reality for dementia patients. In Proceedings of the 2015 AAAI Fall Symposium Series, Arlington, VA, USA, 12–14 November 2015. [Google Scholar]
- Aruanno, B.; Garzotto, F.; Rodriguez, M.C. Hololens-based mixed reality experiences for subjects with alzheimer’s disease. In Proceedings of the 12th Biannual Conference on Italian SIGCHI Chapter, Cagliari, Italy, 18–20 September 2017; pp. 1–9. [Google Scholar]
- Desai, S.; Ong, J.; Fels, D.; Astell, A. Sound Mixed Reality Prompts for People with Dementia: A Familiar and Meaningful Experience. In Designing Interactions for Music and Sound; Focal Press: Waltham, MA, USA, 2022; pp. 151–176. [Google Scholar]
- Hill, N.T.; Mowszowski, L.; Naismith, S.L.; Chadwick, V.L.; Valenzuela, M.; Lampit, A. Computerized Cognitive Training in Older Adults With Mild Cognitive Impairment or Dementia: A Systematic Review and Meta-Analysis. Am. J. Psychiatry 2017, 174, 329–340. [Google Scholar] [CrossRef] [Green Version]
- Arlati, S.; Greci, L.; Mondellini, M.; Zangiacomi, A.; Santo, S.G.D.; Franchini, F.; Marzorati, M.; Mrakic-Sposta, S.; Vezzoli, A. A virtual reality-based physical and cognitive training system aimed at preventing symptoms of dementia. In Proceedings of the International Conference on Wireless Mobile Communication and Healthcare, Vienna, Austria, 14–15 September 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 117–125. [Google Scholar]
- Zygouris, S.; Giakoumis, D.; Votis, K.; Doumpoulakis, S.; Ntovas, K.; Segkouli, S.; Karagiannidis, C.; Tzovaras, D.; Tsolaki, M. Can a virtual reality cognitive training application fulfill a dual role? Using the virtual supermarket cognitive training application as a screening tool for mild cognitive impairment. J. Alzheimer’S Dis. 2015, 44, 1333–1347. [Google Scholar] [CrossRef]
- Maeng, S.; Hong, J.P.; Kim, W.H.; Kim, H.; Cho, S.E.; Kang, J.M.; Na, K.S.; Oh, S.H.; Park, J.W.; Bae, J.N.; et al. Effects of Virtual Reality-Based Cognitive Training in the Elderly with and without Mild Cognitive Impairment. Psychiatry Investig. 2021, 18, 619. [Google Scholar] [CrossRef]
- Mondellini, M.; Arlati, S.; Pizzagalli, S.; Greci, L.; Sacco, M.; Ferrigno, G. Assessment of the usability of an immersive virtual supermarket for the cognitive rehabilitation of elderly patients: A pilot study on young adults. In Proceedings of the 2018 IEEE 6th International Conference on Serious Games and Applications for Health, SeGAH 2018, Vienna, Austria, 16–18 May 2018; p. 49556579. [Google Scholar] [CrossRef]
- Arlati, S.; Di Santo, S.G.; Franchini, F.; Mondellini, M.; Filiputti, B.; Luchi, M.; Ratto, F.; Ferrigno, G.; Sacco, M.; Greci, L. Acceptance and Usability of Immersive Virtual Reality in Older Adults with Objective and Subjective Cognitive Decline. J. Alzheimer’s Dis. JAD 2021, 80, 1025–1038. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, A.R.; Thongpapanl, N.; Auh, S. The application of the technology acceptance model under different cultural contexts: The case of online shopping adoption. J. Int. Mark. 2014, 22, 68–93. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator sickness questionnaire: An enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Rebenitsch, L.; Owen, C. Review on cybersickness in applications and visual displays. Virtual Real. 2016, 20, 101–125. [Google Scholar] [CrossRef]
- Bouchard, S.; Robillard, G.; Renaud, P. Revising the factor structure of the Simulator Sickness Questionnaire. Annu. Rev. CyberTherapy Telemed. 2007, 5, 128–137. [Google Scholar]
- Venkatesh, V.; Bala, H. Technology Acceptance Model 3 and a Research Agenda on Interventions. Decis. Sci. 2008, 39, 273–315. [Google Scholar] [CrossRef] [Green Version]
- Lessiter, J.; Freeman, J.; Keogh, E.; Davidoff, J. A cross-media presence questionnaire: The ITC-sense of presence inventory. Presence Teleoperators Virtual Environ. 2001, 10, 282–297. [Google Scholar] [CrossRef] [Green Version]
- SPSS Statistics | IBM. Available online: https://www.ibm.com/it-it/spss (accessed on 24 October 2022).
- Dorić, D.; Nikolić-Dorić, E.; Jevremović, V.; Mališić, J. On measuring skewness and kurtosis. Qual. Quant. 2007, 43, 481–493. [Google Scholar] [CrossRef]
- Wilcoxon, F. Individual Comparisons by Ranking Methods. Biom. Bull. 1945, 1, 80–83. [Google Scholar] [CrossRef]
- Trzepacz, P.T.; Hochstetler, H.; Wang, S.; Walker, B.; Saykin, A.J. Relationship between the Montreal Cognitive Assessment and Mini-mental State Examination for assessment of mild cognitive impairment in older adults. BMC Geriatr. 2015, 15, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergeron, D.; Flynn, K.; Verret, L.; Poulin, S.; Bouchard, R.W.; Bocti, C.; Fülöp, T.; Lacombe, G.; Gauthier, S.; Nasreddine, Z.; et al. Multicenter validation of an MMSE-Mo CA conversion table. J. Am. Geriatr. Soc. 2017, 65, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, J.; Schmitz, P.; Calero Valdez, A.; Kobbelt, L.; Ziefle, M. Get well soon! human factors’ influence on cybersickness after redirected walking exposure in virtual reality. In Proceedings of the Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), Las Vegas, NV, USA, 15–20 July 2018; Springer: Berlin/Heidelberg, Gremany, 2018; Volume 10909 LNCS, pp. 82–101. [Google Scholar]
- Yildirim, C. Cybersickness during VR gaming undermines game enjoyment: A mediation model. Displays 2019, 59, 35–43. [Google Scholar] [CrossRef]
- Schepers, J.; Wetzels, M. A meta-analysis of the technology acceptance model: Investigating subjective norm and moderation effects. Inf. Manag. 2007, 44, 90–103. [Google Scholar] [CrossRef]
- Venkatesh, V. Determinants of Perceived Ease of Use: Integrating Control, Intrinsic Motivation, and Emotion into the Technology Acceptance Model. Inf. Syst. Res. 2000, 11, 342–365. [Google Scholar] [CrossRef] [Green Version]
- Lau, S.Y.J.; Agius, H. A framework and immersive serious game for mild cognitive impairment. Multimed. Tools Appl. 2021, 80, 31183–31237. [Google Scholar] [CrossRef]
- Mittelstaedt, J.M.; Wacker, J.; Stelling, D. VR aftereffect and the relation of cybersickness and cognitive performance. Virtual Real. 2019, 23, 143–154. [Google Scholar] [CrossRef]
- Edmans, J.A.; Gladman, J.R.; Cobb, S.; Sunderland, A.; Pridmore, T.; Hilton, D.; Walker, M.F. Validity of a virtual environment for stroke rehabilitation. Stroke 2006, 37, 2770–2775. [Google Scholar] [CrossRef] [Green Version]
- Mondellini, M.; Arlati, S.; Greci, L.; Ferrigno, G.; Sacco, M. Sense of presence and cybersickness while cycling in virtual environments: Their contribution to subjective experience. In Proceedings of the International Conference on Augmented Reality, Virtual Reality and Computer Graphics, Otranto, Italy, 24–27 June 2018; Springer: Berlin/Heidelberg, Germany, 2018; pp. 3–20. [Google Scholar]
- Leppiman, A.; Riivits-Arkonsuo, I.; Pohjola, A. Old-Age Digital Exclusion as a Policy Challenge in Estonia and Finland. In Social Exclusion in Later Life; Springer: Cham, Switzerlnad, 2021; pp. 409–419. [Google Scholar]
- Arlati, S.; Spoladore, D.; Baldassini, D.; Sacco, M.; Greci, L. VirtualCruiseTour: An AR/VR application to promote shore excursions on cruise ships. In Proceedings of the International Conference on Augmented Reality, Virtual Reality and Computer Graphics, Lecce, Italy, 7–10 September 2018; Springer: Berlin/Heidelberg, Germany, 2018; pp. 133–147. [Google Scholar]
- Faulkner, L. Beyond the five-user assumption: Benefits of increased sample sizes in usability testing. Behav. Res. Methods Instrum. Comput. 2003, 35, 379–383. [Google Scholar] [CrossRef] [Green Version]
- Grassini, S.; Laumann, K. Are modern head-mounted displays sexist? A systematic review on gender differences in HMD-mediated virtual reality. Front. Psychol. 2020, 11, 1604. [Google Scholar] [CrossRef]
- Stanney, K.; Fidopiastis, C.; Foster, L. Virtual reality is sexist: But it does not have to be. Front. Robot. AI 2020, 7, 4. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technology | Definition | Applications |
|---|---|---|
| Virtual reality | an artificial, virtual and viewer-centered experience that blocks out the physical world | physical activity [29], cognitive training [30], reminescence therapy [31] |
| Augmented reality | a hybrid experience consisting of context-specific virtual content merged into a user’s perception of the physical environment | cognitive training [32], assistance in daily life (e.g., home assistance [33] and reminders [34]) |
| Mixed reality | an AR experience characterized by high local presence in which virtual holograms are totally blended with the real world | cognitive training [35], assistance in daily life (e.g., promotion of social engagement [36]) |
| Variable | Min | Max | Mean | Std. Dev. |
|---|---|---|---|---|
| Time Aisle (min) | 1.23 | 40.00 | 15.50 | 13.56 |
| Time Payment (min) | 0.5 | 17.46 | 5.09 | 5.70 |
| Error: dropped item | 0 | 3 | 0.93 | 1.10 |
| Error: wrong item | 0 | 1 | 0.21 | 0.43 |
| Error: dropped and collected | 0 | 1 | 0.31 | 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mondellini, M.; Arlati, S.; Gapeyeva, H.; Lees, K.; Märitz, I.; Pizzagalli, S.L.; Otto, T.; Sacco, M.; Teder-Braschinsky, A. User Experience during an Immersive Virtual Reality-Based Cognitive Task: A Comparison between Estonian and Italian Older Adults with MCI. Sensors 2022, 22, 8249. https://0-doi-org.brum.beds.ac.uk/10.3390/s22218249
Mondellini M, Arlati S, Gapeyeva H, Lees K, Märitz I, Pizzagalli SL, Otto T, Sacco M, Teder-Braschinsky A. User Experience during an Immersive Virtual Reality-Based Cognitive Task: A Comparison between Estonian and Italian Older Adults with MCI. Sensors. 2022; 22(21):8249. https://0-doi-org.brum.beds.ac.uk/10.3390/s22218249
Chicago/Turabian StyleMondellini, Marta, Sara Arlati, Helena Gapeyeva, Kairi Lees, Ingrid Märitz, Simone Luca Pizzagalli, Tauno Otto, Marco Sacco, and Anneli Teder-Braschinsky. 2022. "User Experience during an Immersive Virtual Reality-Based Cognitive Task: A Comparison between Estonian and Italian Older Adults with MCI" Sensors 22, no. 21: 8249. https://0-doi-org.brum.beds.ac.uk/10.3390/s22218249