The Association of Peer Smoking Behavior and Social Support with Quit Success in Employees Who Participated in a Smoking Cessation Intervention at the Workplace

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Setting and Participants
2.3. Measurements
2.4. Variables
2.5. Statistical Analyses
3. Results
3.1. Participants
3.2. Loss to Follow-Up
3.3. Short-Term and Long-Term Abstinence of Participants
3.4. Associations of Social Support with Quit Success
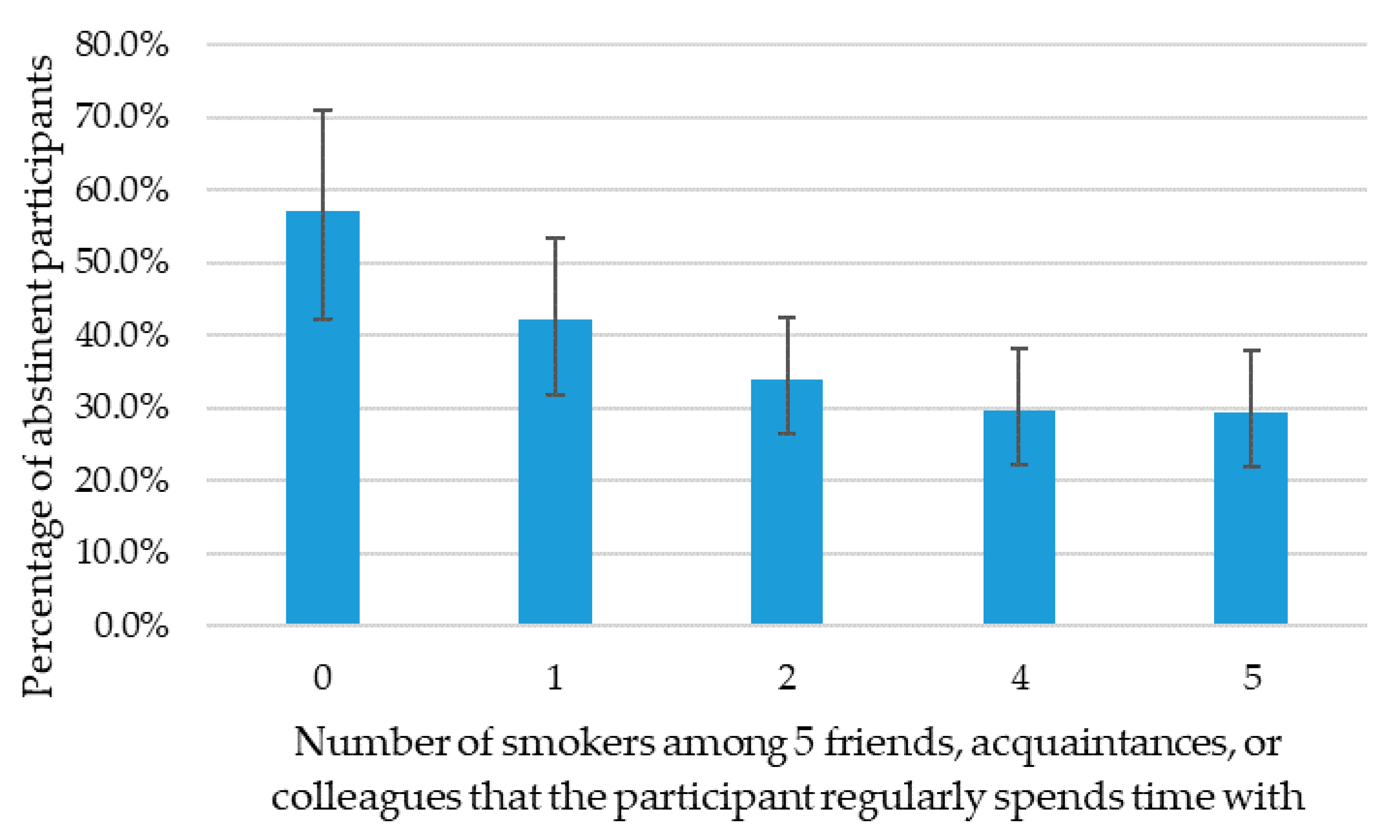
3.5. Associations of Smoking Behavior of Persons in the Social Environment with Quit Success
3.6. Sensitivity Analyses
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Variable | Multiple Imputation | Complete Case Analysis | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p Value | Odds Ratio | 95% CI | p Value | |
| Number of smokers in close circle (0–5) | 0.79 | 0.69–0.89 | <0.001 * | 0.80 | 0.70–0.92 | 0.002 |
| Partner smoking status | ||||||
| Never smoked (ref.) | 1 | 1 | ||||
| Continued smoking | 0.36 | 0.22–0.59 | <0.001 * | 0.43 | 0.25–0.73 | 0.002 * |
| Stopped | 0.47 | 0.26–0.84 | 0.012 * | 0.53 | 0.27–1.02 | 0.059 |
| No partner | 0.39 | 0.23–0.65 | <0.001 * | 0.37 | 0.21–0.66 | <0.001 * |
| Other | 0.08 | 0.02–0.33 | <0.001 * | 0.04 | 0.01–0.31 | 0.002 * |
| Group training colleague support | ||||||
| Not very supportive (ref.) | 1 | 1 | ||||
| Very supportive | 1.94 | 1.22–3.10 | 0.006 * | 1.25 | 0.75–2.07 | 0.392 |
| Other colleague support | ||||||
| Not very supportive (ref.) | 1 | 1 | ||||
| Very supportive | 0.83 | 0.56–1.21 | 0.328 | 0.74 | 0.48–1.14 | 0.172 |
| Friends and family support | ||||||
| Not very supportive (ref.) | 1 | 1 | ||||
| Very supportive | 1.11 | 0.77–1.61 | 0.566 | 1.02 | 0.68–1.54 | 0.915 |
| Partner support | ||||||
| Not very supportive or no partner (ref.) | 1 | 1 | ||||
| Very supportive | 1.88 | 1.30–2.70 | >0.001 * | 1.66 | 1.10–2.51 | 0.016 * |
Appendix B
| Variable | Directly after Smoking Cessation Program A | 12 Months after Smoking Cessation Program B | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p Value | Odds Ratio | 95% Confidence Interval | p Value | |
| Number of smokers in close circle (0–5) | 0.93 | 0.79–1.10 | 0.390 | 0.81 | 0.69–0.94 | 0.006* |
| Partner smoking status | ||||||
| Never smoked (ref.) | 1 | 1 | ||||
| Continued smoking | 1.09 | 0.50–2.37 | 0.828 | 0.49 | 0.28–0.86 | 0.013 * |
| Stopped | 1.35 | 0.48–3.83 | 0.573 | 0.58 | 0.29–1.17 | 0.127 |
| No partner | 0.46 | 0.24–0.89 | 0.022* | 0.46 | 0.23–0.91 | 0.027 * |
| Other | 0.39 | 0.13–1.16 | 0.090 | 0.05 | 0.01–0.38 | 0.004 * |
| Group training colleague support | ||||||
| Not very supportive (ref.) | 1 | 1 | ||||
| Very supportive | 3.53 | 1.94–6.42 | <0.001 * | 1.24 | 0.73–2.11 | 0.422 |
| Other colleague support | ||||||
| Not very supportive (ref.) | 1 | |||||
| Very supportive | 0.98 | 0.55–1.73 | 0.936 | n.s. | n.s. | n.s. |
| Friends and family support | ||||||
| Not very supportive (ref.) | 1 | |||||
| Very supportive | 1.26 | 0.72–2.20 | 0.412 | n.s. | n.s. | n.s. |
| Partner support | ||||||
| Not very supportive or no partner (ref.) | 1 | 1 | ||||
| Very supportive | 2.07 | 1.17–3.66 | 0.012 * | 1.11 | 0.66–1.87 | 0.700 |
References
- Christakis, N.A.; Fowler, J.H. The collective dynamics of smoking in a large social network. N. Engl. J. Med. 2008, 358, 2249–2258. [Google Scholar] [CrossRef] [PubMed]
- Hitchman, S.C.; Fong, G.T.; Zanna, M.P.; Thrasher, J.F.; Laux, F.L. The relation between number of smoking friends, and quit intentions, attempts, and success: Findings from the International Tobacco Control (ITC) Four Country Survey. Psychol. Addict. Behav. 2014, 28, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Holahan, C.K.; Holahan, C.J.; Li, X.; Jung, S.J. Social influences on smoking in American workers: The role of the presence of smokers in the workplace and in the home. Am. J. Health Promot. 2013, 28, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Stead, L.F.; Carroll, A.J.; Lancaster, T. Group behaviour therapy programmes for smoking cessation. CDSR 2017. [Google Scholar] [CrossRef] [PubMed]
- Lawhon, D.; Humfleet, G.L.; Hall, S.M.; Munoz, R.F.; Reus, V.I. Longitudinal analysis of abstinence-specific social support and smoking cessation. Health Psychol. 2009, 28, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Margolis, R.; Wright, L. Better off alone than with a smoker: the influence of partner’s smoking behavior in later life. J Gerontol B Pscyhol Sci Soc Sci 2016, 74, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Homish, G.G.; Leonard, K.E. Spousal influence on smoking behaviors in a US community sample of newly married couples. Soc. Sci. Med. 2005, 61, 2557–2567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandola, T.; Head, J.; Bartley, M.J. Socio-demographic predictors of quitting smoking: How important are household factors? Addiction 2004, 99, 770–777. [Google Scholar] [CrossRef]
- Ferguson, J.; Bauld, L.; Chesterman, J.; Judge, K. The English smoking treatment services: One-year outcomes. Addiction 2005, 100, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Hyland, A.; Li, Q.; Bauer, J.E.; Giovino, G.A.; Steger, C.; Cummings, K.M.J. Predictors of cessation in a cohort of current and former smokers followed over 13 years. Nicotine Tob. Res. 2004, 6, S363–S369. [Google Scholar] [CrossRef]
- Biener, L.; Hamilton, W.L.; Siegel, M.; Sullivan, E.M. Individual, social-normative and policy predictors of smoking cessation: A multilevel longitudinal analysis. Am. J. Public Health 2010, 100, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Baha, M.; Le Faou, A.L. Smokers’ reasons for quitting in an anti-smoking social context. Public Health 2010, 124, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Westmaas, J.L.; Bontemps-Jones, J.; Bauer, J.E. Social support in smoking cessation: Reconciling theory and evidence. Nicotine Tob. Res. 2010, 12, 695–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dellen, M.R.; Boyd, S.M.; Ranby, K.W.; MacKillop, J.; Lipkus, I.M.J. Willingness to provide support for a quit attempt: A study of partners of smokers. J. Health Psychol. 2016, 21, 1840–1849. [Google Scholar] [CrossRef] [PubMed]
- Shiffmann, S. Dynamic influences on smoking relapse process. J. Pers. 2005, 73, 1715–1748. [Google Scholar] [CrossRef] [PubMed]
- Quist, H.G.; Christensen, U.; Carneiro, I.G.; Hansen, J.V.; Bjorner, J.B. Do colleagues influence our lifestyle: The matter of smoking, body mass index and leisure-time physical activity? Prev. Med. 2014, 67, 166–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yong, L.C.; Luckhaupt, S.E.; Li, J.; Calvert, G.M. Quit interest, quit attempt and recent cigarette smoking cessation in the US working population, 2010. Occup. Environ. Med. 2014, 71, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Van den Brand, F.A.; Dohmen, L.M.E.; Van Schayck, C.P.; Nagelhout, G.E. ’Secretly, it’s a competition‘: A qualitative study investigating what helped employees quit smoking during a workplace smoking cessation group training programme with incentives. BMC Open 2018. [Google Scholar] [CrossRef]
- Roski, J.; Schmid, L.A.; Lando, H.A. Long-term associations of helpful and harmful spousal behaviors with smoking cessation. Addict. Behav. 1996, 21, 173–185. [Google Scholar] [CrossRef]
- Mermelstein, R.; Cohen, S.; Lichtenstein, E.; Baer, J.S.; Kamarck, T. Social support and smoking cessation and maintenance. J. Consult. Clin. Psychol. 1986, 54, 447–453. [Google Scholar] [CrossRef]
- Van den Brand, F.A.; Nagelhout, G.E.; Winkens, B.; Evers, S.M.; Kotz, D.; Chavannes, N.H.; Van Schayck, C.P. The effect of financial incentives on top of behavioral support on quit rates in tobacco smoking employees: Study protocol of a cluster-randomized trial. BMC Public Health 2016, 16, 1056. [Google Scholar] [CrossRef] [PubMed]
- Van den Brand, F.A.; Nagelhout, G.E.; Winkens, B.; Chavannes, N.H.; Van Schayck, O.C.P. Effect of a workplace-based group training programme combined with financial incentives on smoking cessation: A cluster-randomised controlled trial. Lancet Public health 2018, 3, e536–e544. [Google Scholar] [CrossRef]
- West, R.P.L.J. Outcome criteria in smoking cessation trials: Proposal for a common standard. Addiction 2005, 100, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.-O. The Fagerström Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Fagerström, K.; Furberg, H. A comparison of the Fagerström Test for Nicotine Dependence and smoking prevalence across countries. Addiction 2008, 103, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Herd, N.; Borland, R.; Hyland, A. Predictors of smoking relapse by duration of abstinence: Findings from the International Tobacco Control (ITC) Four Country Survey. Addiction 2009, 104, 2088–2099. [Google Scholar] [CrossRef] [PubMed]
- Dollar, K.M.; Homish, G.G.; Kozlowski, L.T.; Leonard, K.E. Spousal and alcohol-related predictors of smoking cessation: A longitudinal study in a community sample of married couples. Am. J. Public Health 2009, 99, 231–233. [Google Scholar] [CrossRef] [PubMed]

| Characteristic | Participants |
|---|---|
| Age (n = 599) | |
| Mean (standard deviation (SD)) | 45.1 (10.2) |
| Sex (n = 604) | |
| Women | 381 (37%) |
| Men | 223 (63%) |
| Educational level (n = 579) | |
| Low | 159 (27%) |
| Moderate | 255 (44%) |
| High | 165 (29%) |
| Income level (n = 535) | |
| Low | 179 (33%) |
| Moderate | 175 (33%) |
| High | 181 (34%) |
| Nicotine dependence (Fagerström score 0–10) (n = 573) | |
| Mean (SD) | 4.4 (2.0) |
| Minimally dependent (<4) | 184 (32.1%) |
| Moderately dependent (4–6) | 305 (53.2%) |
| Highly dependent (7–10) | 84 (14.7%) |
| Number of smokers within five friends, acquaintances or colleagues (n = 579) | |
| Mean (SD) | 3.8 (1.5) |
| 0 | 42 (7%) |
| 1 | 76 (12%) |
| 2 | 130 (22%) |
| 3 | 124 (21%) |
| 4 | 125 (21%) |
| 5 | 82 (14%) |
| Characteristic | Participants |
|---|---|
| Participant smoking status A | |
| Abstinent after smoking cessation program completion (n = 604) | |
| Yes | 482 (80%) |
| No | 122 (20%) |
| Abstinent 12 months after smoking cessation program completion (n = 603) B | |
| Yes | 206 (34%) |
| No | 397 (66%) |
| Partner smoking status (n = 508) | |
| Never smoked | 237 (47%) |
| Continued smoking | 108 (21%) |
| Stopped | 63 (12%) |
| No partner | 96 (19%) |
| Other | 4 (1%) |
| Group training colleague support (n = 503) | |
| Not very supportive | 112 (22%) |
| Very supportive | 391 (78%) |
| Other colleague support (n = 500) | |
| Not very supportive | 304 (61%) |
| Very supportive | 196 (39%) |
| Friends and family support (n = 509) | |
| Not very supportive | 247 (49%) |
| Very supportive | 262 (51%) |
| Partner support (n = 516) | |
| Not very supportive | 133 (26%) |
| No partner | 106 (20%) |
| Very supportive | 277 (54%) |
| Variable | Smoking Abstinence Directly after the Smoking Cessation Program A | Smoking Abstinence 12 Months after the Smoking Cessation Program B | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p Value | Odds Ratio | 95% Confidence Interval | p Value | |
| Number of smokers in close circle (0–5) | 0.93 | 0.80–1.08 | 0.346 | 0.81 | 0.71–0.92 | 0.002 * |
| Partner smoking status | ||||||
| Never smoked (ref.) | 1 | 1 | ||||
| Continued smoking | 0.62 | 0.33–1.17 | 0.140 | 0.40 | 0.24–0.66 | <0.001 * |
| Stopped | 0.87 | 0.36–2.06 | 0.745 | 0.47 | 0.26–0.86 | 0.014 * |
| No partner | 0.46 | 0.25–0.85 | 0.014 * | 0.48 | 0.26–0.88 | 0.019 * |
| Other | 0.23 | 0.09–0.57 | 0.002 * | 0.09 | 0.02–0.35 | <0.001 * |
| Group training colleague support | ||||||
| Not very supportive (ref.) | 1 | 1 | ||||
| Very supportive | 3.63 | 2.07–6.37 | <0.001 * | 1.85 | 1.14–3.00 | 0.013 * |
| Other colleague support | ||||||
| Not very supportive (ref.) | 1 | |||||
| Very supportive | 0.95 | 0.57–1.58 | 0.850 | n.s. C | n.s. C | n.s. C |
| Friends and family support | ||||||
| Not very supportive (ref.) | 1 | |||||
| Very supportive | 1.23 | 0.76–1.99 | 0.398 | n.s.C | n.s. C | n.s. C |
| Partner support | ||||||
| Not very supportive or no | ||||||
| partner (ref.) | 1 | 1 | ||||
| Very supportive | 2.01 | 1.23–3.30 | 0.006 * | 1.19 | 0.75–1.88 | 0.465 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van den Brand, F.A.; Nagtzaam, P.; Nagelhout, G.E.; Winkens, B.; van Schayck, C.P. The Association of Peer Smoking Behavior and Social Support with Quit Success in Employees Who Participated in a Smoking Cessation Intervention at the Workplace. Int. J. Environ. Res. Public Health 2019, 16, 2831. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162831
van den Brand FA, Nagtzaam P, Nagelhout GE, Winkens B, van Schayck CP. The Association of Peer Smoking Behavior and Social Support with Quit Success in Employees Who Participated in a Smoking Cessation Intervention at the Workplace. International Journal of Environmental Research and Public Health. 2019; 16(16):2831. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162831
Chicago/Turabian Stylevan den Brand, Floor A., Puck Nagtzaam, Gera E. Nagelhout, Bjorn Winkens, and Constant P. van Schayck. 2019. "The Association of Peer Smoking Behavior and Social Support with Quit Success in Employees Who Participated in a Smoking Cessation Intervention at the Workplace" International Journal of Environmental Research and Public Health 16, no. 16: 2831. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162831