Evaluating the Reliability and Validity of the Children’s Vitality-Relaxation Scale

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Translation and Cultural Adaptation Processes
2.3. Instruments
2.3.1. The Children’s Vitality-Relaxation Scale (CVRS)
2.3.2. Positive Affect and Negative Affect Schedule (PANAS)
2.3.3. Perceived Stress Scale (PSS)
2.3.4. Stress Response Inventory (SRI)
2.4. Data Collection
2.5. Data Analyses
2.6. Ethical Approval
3. Results
3.1. Characteristics of the Participants and Descriptive Data
3.2. Construct Validity
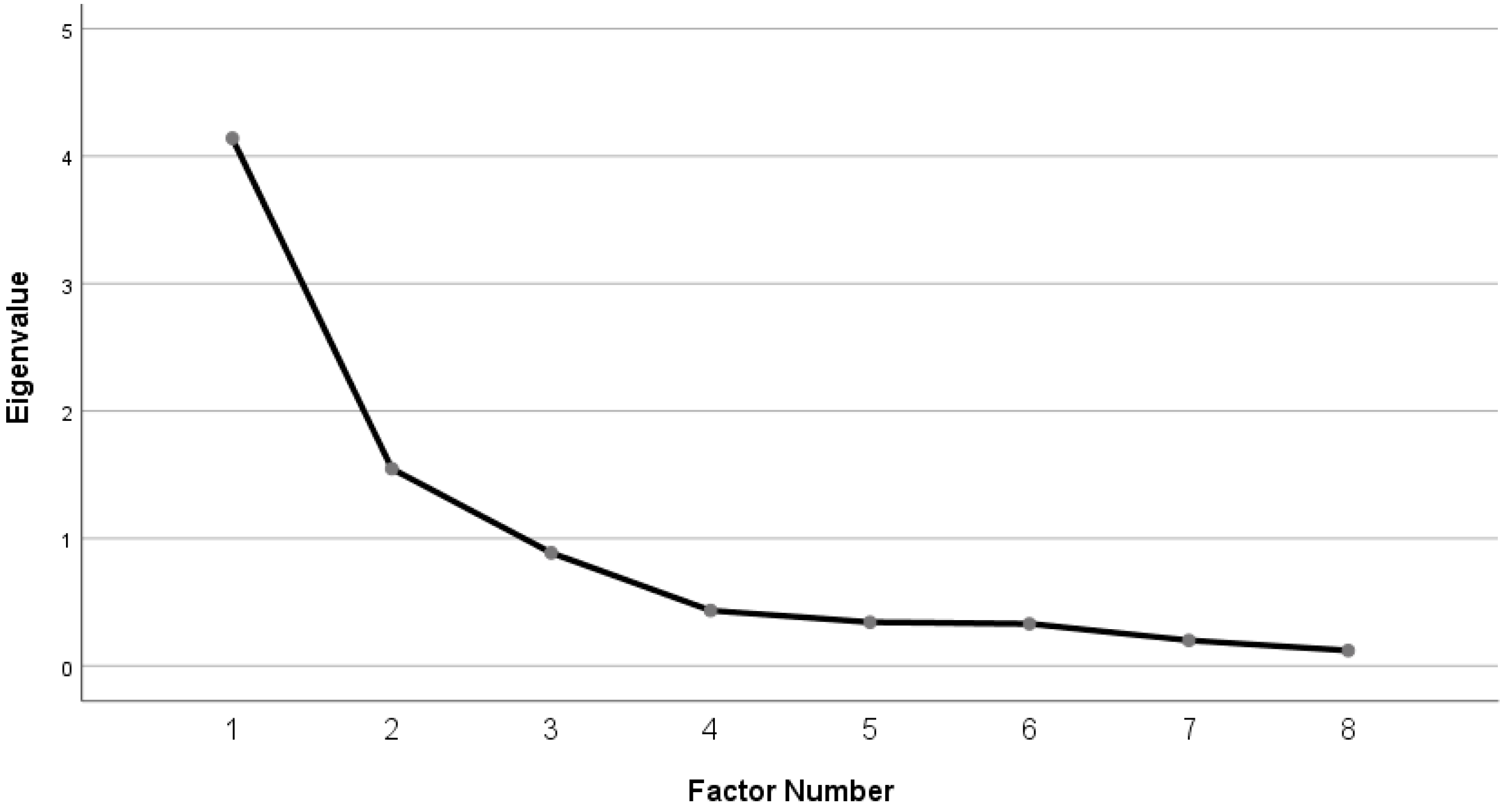
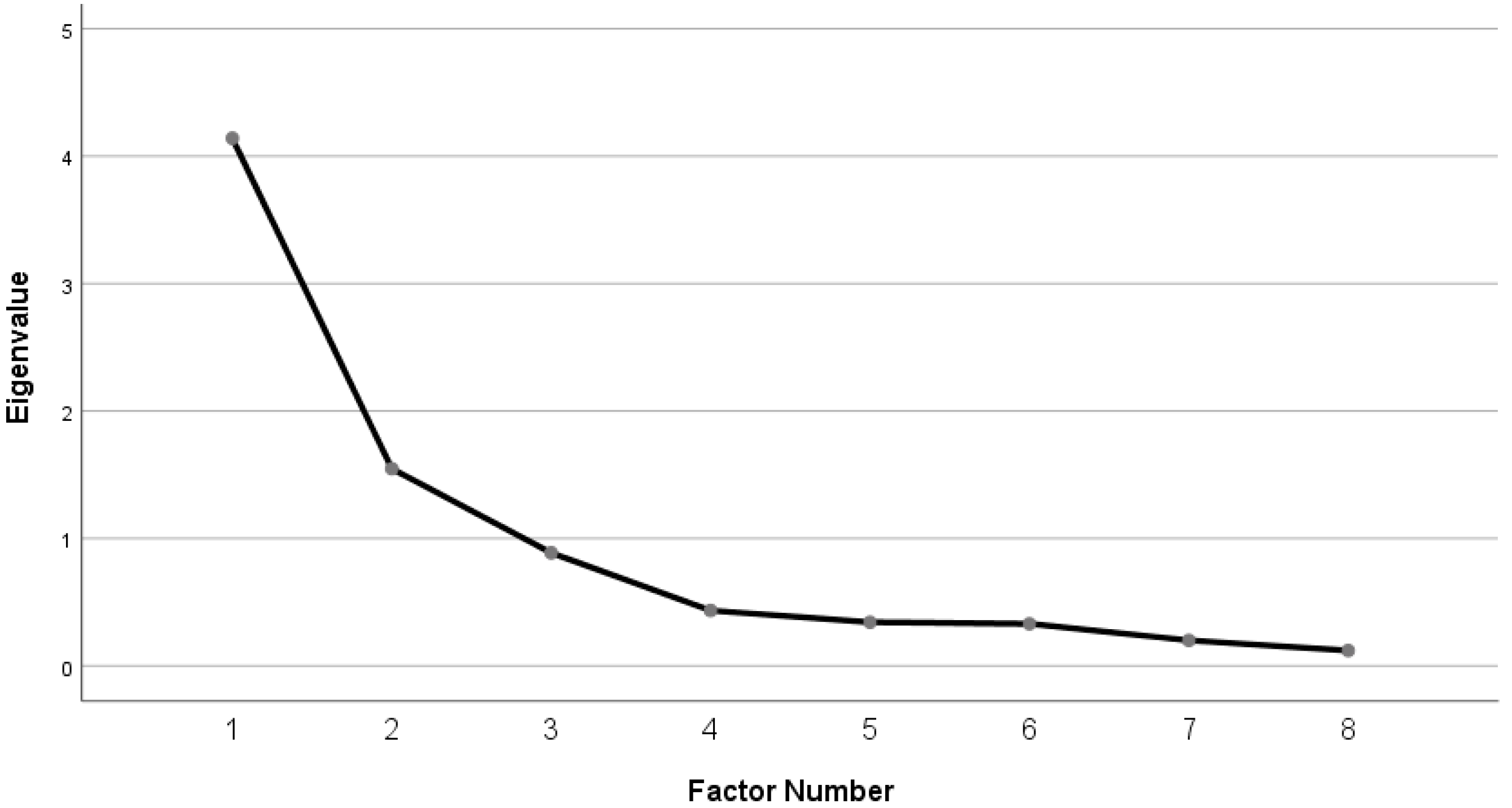
3.2.1. Factor Analysis
3.2.2. Known-Groups Validity
3.2.3. External construct Validity
3.3. Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Russell, J.A. Core affect and the psychological construction of emotion. Psychol. Rev. 2003, 110, 145–172. [Google Scholar] [CrossRef]
- Sheeran, P.; Webb, T.L.; Gollwitzer, P.M.; Oettingen, G.; Williams, D.; Rhodes, R.; Conner, M. Self-regulation of affect-health behavior relations. In Affective Determinants of Health Behavior; Williams, D.M., Rhodes, R.E., Conner, M.T., Eds.; Oxford University Press: New York, NY, USA, 2018; pp. 90–114. [Google Scholar]
- Watson, D.; Clark, L.A.; Carey, G. Positive and negative affectivity and their relation to anxiety and depressive disorders. J. Abnorm. Psychol. 1988, 97, 346–353. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Diener, E.; Wirtz, D.; Tov, W.; Kim-Prieto, C.; Choi, D.-W.; Oishi, S.; Biswas-Diener, R. New well-being measures: Short scales to assess flourishing and positive and negative feelings. Soc. Indic. Res. 2010, 97, 143–156. [Google Scholar] [CrossRef]
- Ramsawh, J.H.; Chavira, A.D. Association of childhood anxiety disorders and quality of life in a primary care sample. J. Dev. Behav. Pediatr. 2016, 37, 269–276. [Google Scholar] [CrossRef]
- Newman, L.; Sivaratnam, C.; Komiti, A. Attachment and early brain development–neuroprotective interventions in infant–caregiver therapy. Transl. Dev. Psychiatry 2015, 3, 28647. [Google Scholar] [CrossRef]
- Kim, J.W.; Lee, K.; Lee, Y.S.; Han, D.H.; Min, K.J.; Song, S.H.; Park, G.N.; Lee, J.Y.; Kim, J.O. Factors associated with group bullying and psychopathology in elementary school students using child-welfare facilities. Neuropsychiatr. Dis. Treat. 2015, 11, 991–998. [Google Scholar] [CrossRef] [Green Version]
- Jongenelis, M.; Pettigrew, S.; Lawrence, D.; Rikkers, W. Factors associated with poly drug use in adolescents. Prev. Sci. 2019, 20, 695–704. [Google Scholar] [CrossRef]
- Johnson, D.; Dupuis, G.; Piche, J.; Clayborne, Z.; Colman, I. Adult mental health outcomes of adolescent depression: A systematic review. Depress. Anxiety 2018, 35, 700–716. [Google Scholar] [CrossRef]
- Miller, A.L.; Gearhardt, A.N.; Retzloff, L.; Sturza, J.; Kaciroti, N.; Lumeng, J.C. Early childhood stress and child age predict longitudinal increases in obesogenic eating among low-income children. Acad. Pediatr. 2018, 18, 685–691. [Google Scholar] [CrossRef]
- Das, J.K.; Salam, R.A.; Lassi, Z.S.; Khan, M.N.; Mahmood, W.; Patel, V.; Bhutta, Z.A. Interventions for adolescent mental health: An overview of systematic reviews. J. Adolesc. Health 2016, 59, S49–S60. [Google Scholar] [CrossRef]
- Werner-Seidler, A.; Perry, Y.; Calear, A.L.; Newby, J.M.; Christensen, H. School-based depression and anxiety prevention programs for young people: A systematic review and meta-analysis. Clin. Psychol. Rev. 2017, 51, 30–47. [Google Scholar] [CrossRef] [Green Version]
- Weersing, V.R.; Jeffreys, M.; Do, M.-C.T.; Schwartz, K.T.G.; Bolano, C. Evidence base update of psychosocial treatments for child and adolescent depression. J. Clin. Child Adolesc. Psychol. 2017, 46, 11–43. [Google Scholar] [CrossRef]
- Higa-McMillan, C.K.; Francis, S.E.; Rith-Najarian, L.; Chorpita, B.F. Evidence base update: 50 years of research on treatment for child and adolescent anxiety. J. Clin. Child Adolesc. Psychol. 2016, 45, 91–113. [Google Scholar] [CrossRef]
- Ebesutani, C.; Korathu-Larson, P.; Nakamura, B.J.; Higa-McMillan, C.; Chorpita, B. The revised child anxiety and depression scale 25–parent version: Scale development and validation in a school-based and clinical sample. Assessment 2017, 24, 712–728. [Google Scholar] [CrossRef]
- Becker, S.P.; Schindler, D.N.; Holdaway, A.S.; Tamm, L.; Epstein, J.N.; Luebbe, A.M. The revised child anxiety and depression scales (RCADS): Psychometric evaluation in children evaluated for ADHD. J. Psychopathol. Behav. Assess. 2019, 41, 93–106. [Google Scholar] [CrossRef]
- Diener, E. Subjective well-being. Psychol. Bull. 1984, 95, 542–575. [Google Scholar] [CrossRef]
- Van Cappellen, P.; Rice, E.L.; Catalino, L.I.; Fredrickson, B.L. Positive affective processes underlie positive health behaviour change. Psychol. Health 2018, 33, 77–97. [Google Scholar] [CrossRef]
- Pressman, S.D.; Cohen, S. Does positive affect influence health? Psychol. Bull. 2005, 131, 925–971. [Google Scholar] [CrossRef]
- Ironson, G.; Banerjee, N.; Fitch, C.; Krause, N. Positive emotional well-being, health Behaviors, and inflammation measured by C-Reactive protein. Soc. Sci. Med. 2018, 197, 235–243. [Google Scholar] [CrossRef]
- Terry, P.C.; Lane, A.M.; Lane, H.J.; Keohane, L. Development and validation of a mood measure for adolescents. J. Sports Sci. 1999, 17, 861–872. [Google Scholar] [CrossRef] [Green Version]
- Laurent, J.; Catanzaro, S.J.; Joiner, T.E., Jr.; Rudolph, K.D.; Potter, K.I.; Lambert, S.; Osborne, L.; Gathright, T. A measure of positive and negative affect for children: Scale development and preliminary validation. Psychol. Assess. 1999, 11, 326–338. [Google Scholar] [CrossRef]
- Russell, J.A. A circumplex model of affect. J. Pers. Soc. Psychol. 1980, 39, 1161–1178. [Google Scholar] [CrossRef]
- Ekkekakis, P. Affect, mood, and emotion. In Measurement in Sport and Exercise Psychology; Tenenbaum, G., Eklund, R.C., Kamata, A., Eds.; Human Kinetics: Champaign, IL, USA, 2012; pp. 321–332. [Google Scholar]
- Okado, I.; Mueller, C.W.; Nakamura, B.J. Positive and negative affect in clinic-referred youth with ADHD. J. Atten. Disord. 2016, 20, 53–62. [Google Scholar] [CrossRef]
- Ramsey, M.A.; Gentzler, A.L. An upward spiral: Bidirectional associations between positive affect and positive aspects of close relationships across the life span. Dev. Rev. 2015, 36, 58–104. [Google Scholar] [CrossRef]
- Russell, J.A.; Weiss, A.; Mendelsohn, G.A. Affect grid: A single-item scale of pleasure and arousal. J. Pers. Soc. Psychol. 1989, 57, 493–502. [Google Scholar] [CrossRef]
- Killgore, W.D.S. The affect grid: A moderately valid, nonspecific measure of pleasure and arousal. Psychol. Rep. 1998, 83, 639–642. [Google Scholar] [CrossRef]
- Korpela, K.M.; Ylén, M.P. Effectiveness of favorite–place prescriptions: A field experiment. Am. J. Prev. Med. 2009, 36, 435–438. [Google Scholar] [CrossRef]
- Staats, H.; Kieviet, A.; Hartig, T. Where to recover from attentional fatigue: An expectancy-value analysis of environmental preference. J. Environ. Psychol. 2003, 23, 147–157. [Google Scholar] [CrossRef]
- Hartig, T.; Lindblom, K.; Ovefelt, K. The home and near-home area offer restoration opportunities differentiated by gender. Scand. Hous. Plan. Res. 1998, 15, 283–296. [Google Scholar] [CrossRef]
- Han, K.-T. A reliable and valid self-rating measure of the restorative quality of natural environments. Landsc. Urban Plan. 2003, 64, 209–232. [Google Scholar] [CrossRef]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989. [Google Scholar]
- Korpela, K.; Savonen, E.-M.; Anttila, S.; Pasanen, T.; Ratcliffe, E. Enhancing wellbeing with psychological tasks along forest trails. Urban For. Urban Green. 2017, 26, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Crombez, G.; Bijttebier, P.; Eccleston, C.; Mascagni, T.; Mertens, G.; Goubert, L.; Verstraeten, K. The child version of the pain catastrophizing scale (PCS-C): A preliminary validation. Pain 2003, 104, 639–646. [Google Scholar] [CrossRef]
- Hair, J.; Anderson, R.; Black, B.; Babin, B. Multivariate Data Analysis, 7th ed.; Pearson Education: Upper Saddle River, NJ, USA, 2016. [Google Scholar]
- Brislin, R.W.; Freimanis, C. Back-translation: A tool for cross-cultural research. In An Encyclopaedia of Translation: Chinese-English, English-Chinese; Chan, S.-W., David, E.P., Eds.; The Chinese University Press: Sha Tin, Hong Kong, 2001; pp. 22–40. [Google Scholar]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Korpela, K.M.; Ylén, M.; Tyrväinen, L.; Silvennoinen, H. Determinants of restorative experiences in everyday favorite places. Health Place 2008, 14, 636–652. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Kim, E.; Lee, M. A validation study of Korea positive and negative affect schedule: The PANAS scales. Kor. J. Clin. Psychol. 2003, 22, 935–946. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stres. J. Health Soc. Behav. 1983, 24, 386–396. [Google Scholar] [CrossRef]
- Lee, J.E. The Effects of Self-Complexity and Self-Efficacy on Depression and Perceived Stress. Master‘s thesis, Ajou University, Suwon, Korea, 2005. [Google Scholar]
- Ha, J.; Ahn, H. Multiple mediator effect of metacognition on the relation of perceived stress, anxiety and generalized problematic internet use. Korean J. Couns. Psychother. 2013, 25, 251–273. [Google Scholar]
- Choi, S.-M.; Kang, T.-Y.; Woo, J.-M. Development and validation of a modified form of the stress response inventory for workers. J. Korean Neuropsychiatr. Assoc. 2006, 45, 541–553. [Google Scholar]
- Choi, H.C. Statistical Method in Social Science, 3rd ed.; Nanam: Paju, Korea, 2007. [Google Scholar]
- Ryan, R.M.; Frederick, C. On energy, personality, and health: Subjective vitality as a dynamic reflection of well-being. J. Pers. 1997, 65, 529–565. [Google Scholar] [CrossRef]
- White, M.P.; Pahl, S.; Ashbullby, K.; Herbert, S.; Depledge, M.H. Feelings of restoration from recent nature visits. J. Environ. Psychol. 2013, 35, 40–51. [Google Scholar] [CrossRef]
- Sillanpää, E.; Häkkinen, K.; Holviala, J.; Häkkinen, A. Combined strength and endurance training improves health-related quality of life in healthy middle-aged and older adults. Int. J. Sports Med. 2012, 33, 981–986. [Google Scholar] [CrossRef]
- Kircanski, K.; Notthoff, N.; Shadel, D.; Mottola, G.R.; Carstensen, L.L.; Gotlib, I.H. Heightened emotional states increase susceptibility to fraud in older adults. SSRN Electron. J. 2016. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. Support of Community Children Center; Ministry of Health and Welfare: Sejong, South Korea, 2019.
- Gellci, K.; Marusak, H.A.; Peters, C.; Elrahal, F.; Iadipaolo, A.S.; Rabinak, C.A. Community and household-level socioeconomic disadvantage and functional organization of the salience and emotion network in children and adolescents. Neuroimage 2019, 184, 729–740. [Google Scholar] [CrossRef]
- Moon, S.-H.; Cho, H.H. Gender differences in self-competence, social anxiety and depression in upper level primary school children. Child Health Nurs. Res. 2010, 16, 230–238. [Google Scholar] [CrossRef]
- Park, S.; Jang, H.; Lee, E.-S. Major stressors among Korean adolescents according to gender, educational level, residential area, and socioeconomic status. Int. J. Env. Res. Public Health 2018, 15, 2080. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. Nursing Research: Generating and Assessing Evidence for Nursing Practice, 9th ed.; Sumunsa: Paju, South Korea, 2015. [Google Scholar]
- Lindeberg, S.I.; Eek, F.; Lindbladh, E.; Östergren, P.-O.; Hansen, Å.M.; Karlson, B. Exhaustion measured by the SF-36 vitality scale is associated with a flattened diurnal cortisol profile. Psychoneuroendocrinology 2008, 33, 471–477. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Variables | Categories | n (%) | CVRS | Vitality | Relaxation | |||
|---|---|---|---|---|---|---|---|---|
| M (SD) | t/F | M (SD) | Z/H | M (SD) | Z/H | |||
| (p) | (p) | (p) | ||||||
| Type of institution | School | 147 (81.2) | 38.44 (8.79) | 1.64 (0.102) | 21.05 (5.40) | −0.64 (0.523) | 17.39 (4.80) | −2.27 (0.023) |
| Community center | 34 (18.8) | 35.65 (9.43) | 20.32 (5.99) | 15.32 (4.86) | ||||
| Sub-total | 37.91 (8.95) | 20.91 (5.51) | 17.00 (4.87) | |||||
| Gender | Female | 84 (46.4) | 36.08 (9.17) | 2.60 (0.010) | 19.82 (5.63) | −2.53 (0.011) | 16.26 (5.09) | −2.21 (0.027) |
| Male | 97 (53.6) | 39.49 (8.50) | 21.86 (5.24) | 17.64 (4.60) | ||||
| Sub-total | 37.91 (8.95) | 20.91 (5.51) | 17.00 (4.87) | |||||
| Grade | 4th | 39 (21.5) | 41.79 (7.32) | 4.88 (0.009) | 23.64 (4.24) | 12.82 (0.002) | 18.15 (4.73) | 4.01 (0.135) |
| 5th | 77 (42.5) | 36.92 (9.46) | 20.49 (5.71) | 16.43 (5.21) | ||||
| 6th | 65 (35.9) | 36.75 (8.70) | 19.77 (5.50) | 16.98 (4.46) | ||||
| Sub-total | 37.91 (8.95) | 20.91 (5.51) | 17.00 (4.87) | |||||
| Family structure | With parent | 163 (90.1) | 38.21 (8.87) | −1.30 (0.194) | 21.07 (5.40) | −1.08 (0.279) | 17.13 (4.89) | −1.02 (0.308) |
| Without both parents | 18 (9.9) | 35.22 (9.53) | 19.44 (6.40) | 15.78 (4.60) | ||||
| Sub-total | 37.91 (8.95) | 20.91 (5.51) | 17.00 (4.87) | |||||
| Perceived economic status | High | 99 (54.7) | 40.10 (9.00) | −3.74 (<0.001) | 22.35 (5.25) | −4.04 (<0.001) | 17.75 (5.17) | −2.28 (0.023) |
| Middle and low | 82 (45.3) | 35.27 (8.20) | 19.17 (5.34) | 16.10 (4.33) | ||||
| Sub-total | 37.91 (8.95) | 20.91 (5.51) | 17.00 (4.87) | |||||
| Perceived academic status | High | 97 (53.6) | 41.34 (7.69) | 19.63 (<0.001) | 22.65 (4.65) | 20.01 (<0.001) | 18.69 (4.54) | 27.28 (<0.001) |
| Moderate | 68 (37.6) | 34.60 (8.51) | 18.99 (5.61) | 15.62 (4.29) | ||||
| Low | 16 (8.8) | 31.19 (9.27) | 18.56 (6.53) | 12.62 (4.77) | ||||
| Sub-total | 37.91 (8.95) | 20.91 (5.51) | 17.00 (4.87) | |||||
| Factor | Items | Communality | Factor Loading | M (SD) | Corrected Item-Total Correlation | Cronbach’s α If Item Deleted | Cronbach’s α | ||
|---|---|---|---|---|---|---|---|---|---|
| F1 | F2 | ||||||||
| F1 Vitality | 3 | I am enthusiastic and energetic. | 0.79 | 0.88 | 5.51 (1.49) | 0.75 | 0.821 | 0.867 | |
| 7 | I feel confident. | 0.66 | 0.76 | 4.93 (1.72) | 0.73 | 0.823 | |||
| 8 | I feel lively and vital. | 0.85 | 0.91 | 5.42 (1.64) | 0.79 | 0.801 | |||
| 9 | I am hopeful. | 0.69 | 0.61 | 5.06 (1.66) | 0.62 | 0.871 | |||
| F2 Relaxa-tion | 1 | I feel calm. | 0.43 | 0.64 | 3.74 (1.54) | 0.42 | 0.700 | 0.715 | |
| 2 | I can concentrate well. | 0.40 | 0.55 | 4.91 (1.47) | 0.47 | 0.675 | |||
| 4 | I am relaxed. | 0.72 | 0.74 | 4.66 (1.69) | 0.62 | 0.576 | |||
| 5 | I have no worries. | 0.44 | 0.60 | 3.69 (1.90) | 0.52 | 0.648 | |||
| Eigenvalue | 4.14 | 1.55 | |||||||
| Variance (%) | 36.3 | 25.5 | |||||||
| Cumulative variance (%) | 36.3 | 61.8 | |||||||
| Cronbach’s α for the total CVRS = 0.835 | |||||||||
| Variables | CVRS | |||
|---|---|---|---|---|
| Total | Vitality | Relaxation | ||
| r (p) | r (p) | r (p) | ||
| Vitality | 0.880 (<0.001) | |||
| Relaxation | 0.844 (<0.001) | 0.488 (<0.001) | ||
| PANAS | Positive | 0.543 (<0.001) | 0.624 (<0.001) | 0.293 (<0.001) |
| Negative | −0.337 (<0.001) | −0.187 (0.012) | −0.408 (<0.001) | |
| PSS | −0.583 (<0.001) | −0.431 (<0.001) | −0.584 (<0.001) | |
| SRI | −0.448 (<0.001) | −0.298 (<0.001) | −0.488 (<0.001) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bang, K.-S.; Kim, S.; Korpela, K.M.; Song, M.K.; Lee, G.; Jeong, Y. Evaluating the Reliability and Validity of the Children’s Vitality-Relaxation Scale. Int. J. Environ. Res. Public Health 2019, 16, 3369. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183369
Bang K-S, Kim S, Korpela KM, Song MK, Lee G, Jeong Y. Evaluating the Reliability and Validity of the Children’s Vitality-Relaxation Scale. International Journal of Environmental Research and Public Health. 2019; 16(18):3369. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183369
Chicago/Turabian StyleBang, Kyung-Sook, Sungjae Kim, Kalevi M. Korpela, Min Kyung Song, Gumhee Lee, and Yeseul Jeong. 2019. "Evaluating the Reliability and Validity of the Children’s Vitality-Relaxation Scale" International Journal of Environmental Research and Public Health 16, no. 18: 3369. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183369