Quality of Life in Orthodontic Cancer Survivor Patients—A Prospective Case–Control Study


Abstract
:1. Introduction
2. Materials and Methods
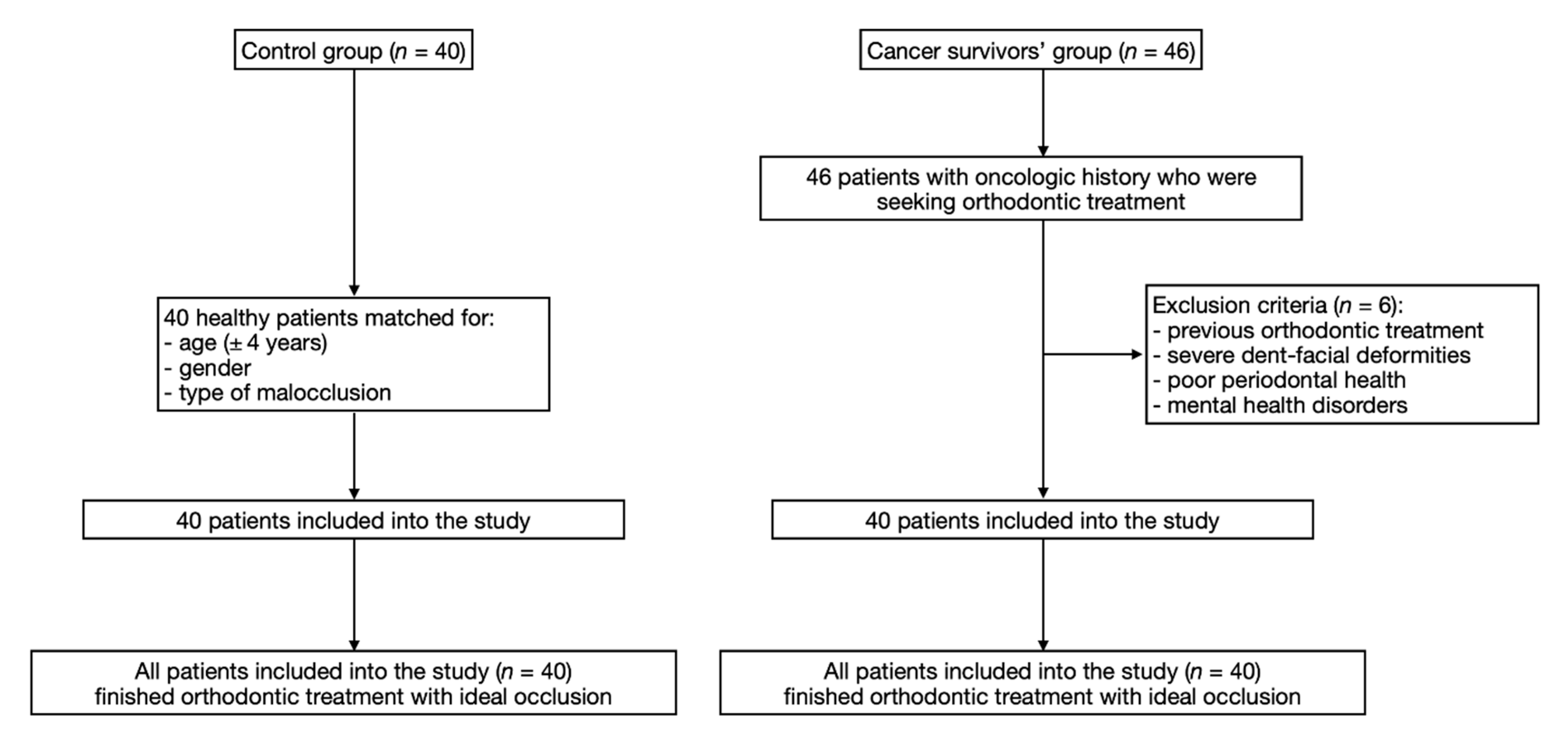
2.1. Study Population
2.2. Study Protocol
2.3. Statistical Analysis
3. Results
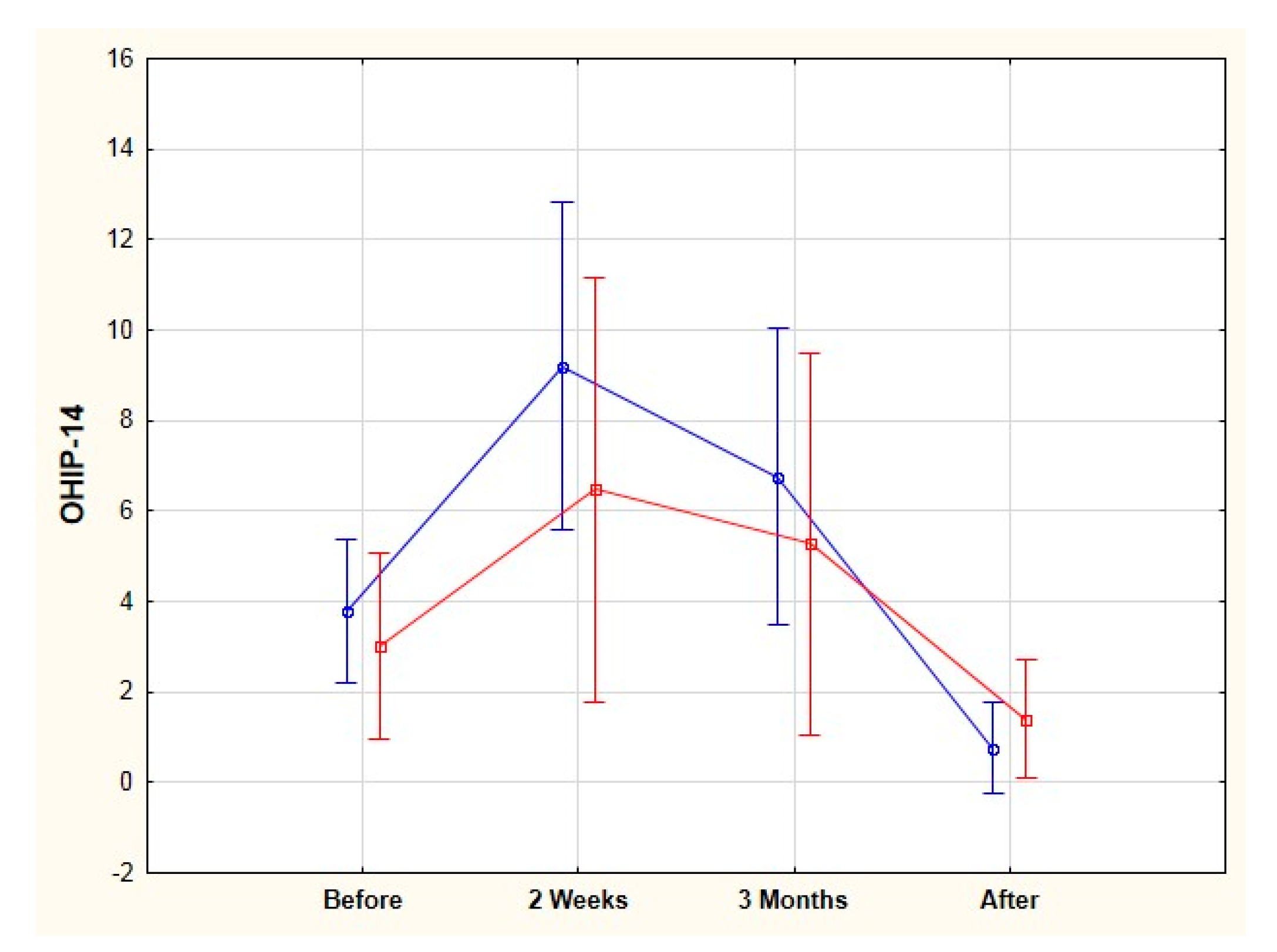
3.1. OHIP-14 Total Score
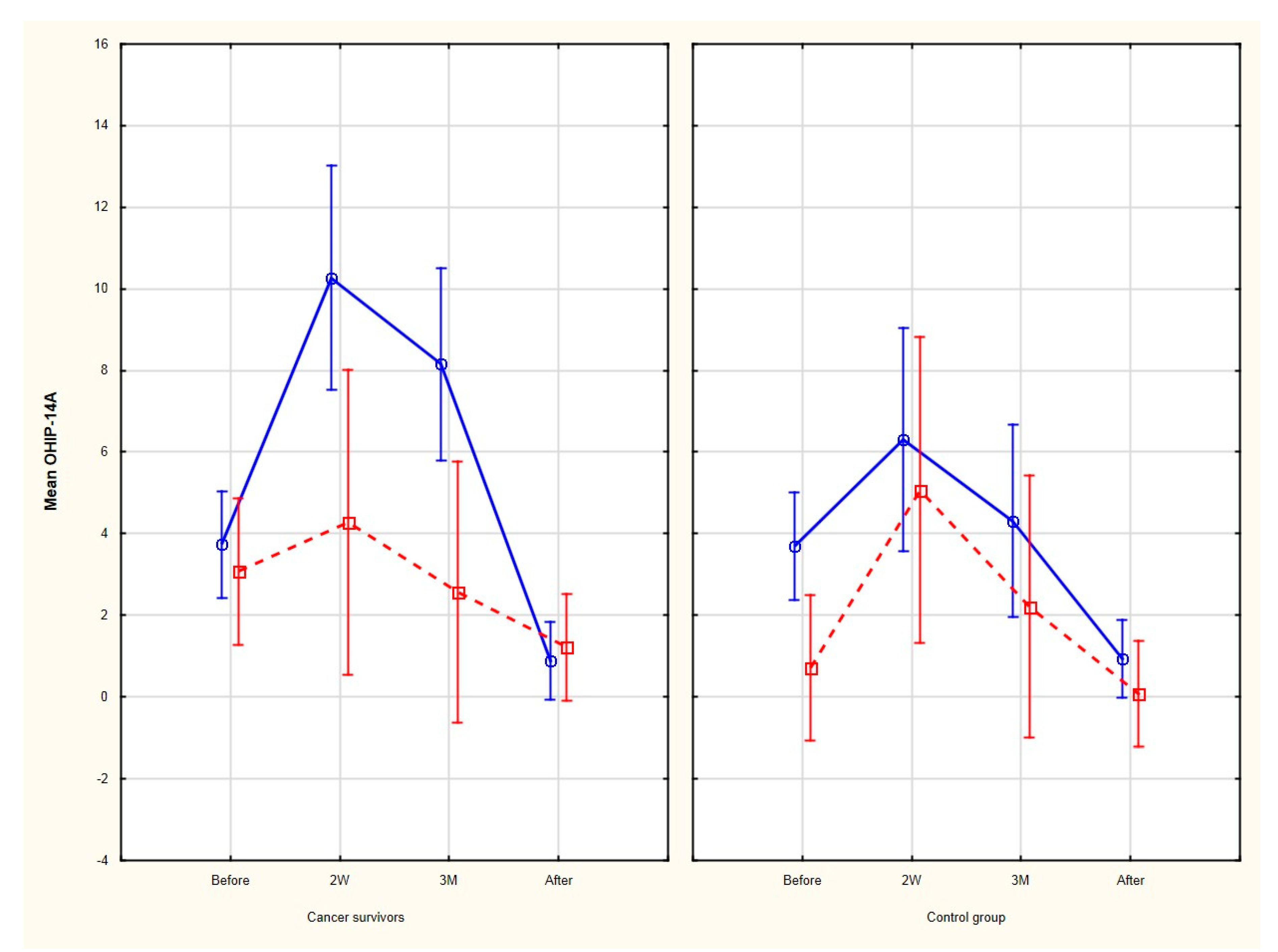
3.2. OHIP-14 Simple Count
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Steliarova-Foucher, E.; Colombet, M.; Ries, L.A.G.; Moreno, F.; Dolya, A.; Bray, F.; Heeseling, P.; Shin, H.Y.; Stiller, C.A.; Bouzbid, S.; et al. International incidence of childhood cancer, 2001–2010: A population-based registry study [published correction appears in Lancet Oncol. 2017 Jun; 18: e301]. Lancet. Oncol. 2017, 18, 719–731. [Google Scholar] [CrossRef]
- Filbin, M.; Monje, M. Developmental origins and emerging therapeutic opportunities for childhood cancer. Nat. Med. 2019, 25, 367–376. [Google Scholar] [CrossRef] [PubMed]
- WHO. Report on Cancer: Setting Priorities, Investing Wisely and Providing Care for All; World Health Organization: Geneva, Switzerland, 2020; Licence: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- Seth, R.; Singh, A. Leukemias in Children. Indian J. Pediatr. 2015, 82, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Howard, S.C.; Zaidi, A.; Cao, X.; Weil, O.; Bey, P.; Patte, C.; Samudio, A.; Haddad, L.; Lam, C.G.; Moreira, C.; et al. The My Child Matters programme: Effect of public-private partnerships on paediatric cancer care in low-income and middle-income countries. Lancet Oncol. 2018, 19, e252–e266. [Google Scholar] [CrossRef]
- Fung, A.; Horton, S.; Zabih, V.; Denburg, A.; Gupta, S. Cost and cost-effectiveness of childhood cancer treatment in low-income and middle-income countries: A systematic review. BMJ Glob. Health. 2019, 4, e001825. [Google Scholar] [CrossRef] [Green Version]
- Saletta, F.; Seng, M.S.; Lau, L. Advances in paediatric cancer treatment. Transl. Pediatr. 2014, 3, 156–182. [Google Scholar]
- Gawade, P.L.; Hudson, M.M.; Kaste, S.C.; Neglia, J.O.; Constine, L.S.; Robison, L.L.; Ness, K.K. A Systematic Review of Dental Late Effects in Survivors of Childhood Cancer. Pediatr. Blood Cancer 2014, 61, 407–416. [Google Scholar] [CrossRef] [Green Version]
- Mishra, S. Orthodontic Therapy for Paediatric Cancer Survivors: A Review. J. Clin. Diagn. Res. 2017, 11, ZE01–CZE04. [Google Scholar] [CrossRef]
- Mituś-Kenig, M.; Łoboda, M.; Marcinkowska-Mituś, A.; Durka-Zajac, M.; Pawłowska, E. Orthodontic treatment in oncological patients. Przegl. Lek. 2015, 72, 243–245. [Google Scholar]
- American Academy of Pediatric Dentistry (AAPD). Guideline on dental management of paediatric patients receiving chemotherapy, hematopoietic cell transplantation, and/or radiation. Pediatr. Dent. 2016, 6, 380–388. [Google Scholar]
- Dental Management of Pediatric Patients Receiving Chemotherapy, Hematopoietic Cell Transplantation, and/or Radiation Therapy. Pediatr. Dent. 2017, 39, 380–388.
- Hongxing, L.; List, T.; Nilsson, I.M.; Johansson, A.; Astrøm, A.N. Validity and reliability of OIDP and OHIP-14: A survey of Chinese high school students. BMC Oral Health 2014, 14, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sischo, L.; Broder, H.L. Oral health-related quality of life: What, why, how, and future implications. J. Dent. Res. 2011, 90, 1264–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andiappana, M.; Gaob, W.; Bernabé, E.; Kandalad, N.B.; Donaldson, A.N. Malocclusion, orthodontic treatment, and the Oral Health Impact Profile (OHIP-14): Systematic review and meta-analysis. Angle Orthod. 2015, 85, 493–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, L.F. The six keys to normal occlusion. Am. J. Orthod. 1972, 62, 296–309. [Google Scholar] [CrossRef]
- Husain, F.A.; Tatengkeng, F. Oral Health-Related Quality of Life Appraised by OHIP-14 Between Urban and Rural Areas in Kutai Kartanegara Regency, Indonesia: Pilot Pathfinder Survey. Open Dent. J. 2017, 11, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Deboni, A.L.; Giordani, A.J.; Lopes, N.N.; Dias, R.S.; Segreto, R.A.; Jensen, S.B.; Segreto, H.R.C. Long-term oral effects in patients treated with radiochemotherapy for head and neck cancer. Support Care Cancer 2012, 20, 555–568. [Google Scholar] [CrossRef]
- Aguiar, G.P.; Jham, B.C.; Magalhães, C.S.; Sensi, L.G.; Freire, A.R. A review of the biological and clinical aspects of radiation caries. J. Contemp. Dent. Pract. 2009, 10, 83–89. [Google Scholar] [CrossRef]
- Hong, C.H.; Fonseca, M. Consideration in the pediatric population with cancer. Dent. Clin. N. Am. 2008, 52, 155–181. [Google Scholar] [CrossRef]
- Kaste, S.C.; Goodman, P.; Leisenring, W.; Stovall, M.; Hayashi, R.J.; Yeazel, M.; Beiraghi, S.; Hudson, M.W.; Sklar, C.A.; Robison, L.L.; et al. Impact of radiation and chemotherapy on the risk of dental abnormalities. Cancer 2009, 115, 5817–5827. [Google Scholar] [CrossRef]
- Sonis, S.T. Oral mucositis. Anticancer Drugs 2011, 22, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Montero-Martín, J.; Bravo-Pérez, M.; Albaladejo-Martínez, A.; Hernández- Martín, L.A.; Rosel-Gallardo, E.M. Validation the Oral Health Impact Profile (OHIP-14sp) for adults in Spain. J. Clin. Exp. Dent. 2009, 1, e1–e7. [Google Scholar]
- Rourke, M.T.; Stuber, M.L.; Hobbie, W.L.; Kazak, A.E. Posttraumatic stress disorder: Understanding the psychosocial impact of surviving childhood cancer into young adulthood. J. Pediatr. Oncol. Nurs. 1999, 16, 126–135. [Google Scholar] [PubMed]
- Bruce, M. A systematic and conceptual review of posttraumatic stress in childhood cancer survivors and their parents. Clin. Psychol. Rev. 2006, 26, 233–256. [Google Scholar] [CrossRef] [PubMed]
- Johal, A.; Alyaqoobi, I.; Patel, R.; Cox, S. The impact of orthodontic treatment on quality of life and self-esteem in adult patients. Eur. J. Orthod. 2015, 37, 233–237. [Google Scholar] [CrossRef]
- Feu, D.; Miguel, J.A.; Celeste, R.K.; Oliveira, B.H. Effect of orthodontic treatment on oral health-related quality of life. Angle Orthod. 2013, 83, 892–898. [Google Scholar] [CrossRef]
- Javidi, H.; Benson, P. The impact of malocclusion and its treatment on the oral health related quality of life of adults, assessed using the Oral Health Impact Profile (OHIP-14). Evid. Based Dent. 2015, 16, 57–58. [Google Scholar] [CrossRef]
- Ni, J.; Song, S.; Zhou, N. Impact of surgical orthodontic treatment on quality of life in Chinese young adults with class III malocclusion: A longitudinal study. BMC Oral Health 2019, 19, 109. [Google Scholar] [CrossRef] [Green Version]
- Rezaei, F.; Masalehi, H.; Golshah, A.; Imani, M.M. Oral health related quality of life of patients with class III skeletal malocclusion before and after orthognathic surgery. BMC Oral Health 2019, 19, 289. [Google Scholar] [CrossRef]
- Zheng, D.H.; Wang, X.X.; Su, Y.R.; Zhao, S.Y.; Xu, C.; Kong, C.; Zhang, J. Assessing changes in quality of life using the Oral Health Impact Profile (OHIP) in patients with different classifications of malocclusion during comprehensive orthodontic treatment. BMC Oral Health 2015, 15, 148. [Google Scholar] [CrossRef] [Green Version]
- Demirovic, K.; Habibovic, J.; Dzemidzic, V.; Tiro, A.; Nakas, E. Comparison of Oral Health-Related Quality of Life in Treated and Non-Treated Orthodontic Patients. Med. Arch. 2019, 73, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Jamilian, A.; Kiaee, B.; Sanayei, S.; Khosravi, S.; Perillo, L. Orthodontic Treatment of Malocclusion and its Impact on Oral Health-Related Quality of Life. Open Dent. J. 2016, 10, 236–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, J.M.; Kang, K.H. Effect of malocclusion or orthodontic treatment on oral health-related quality of life in adults. Korean J. Orthod. 2014, 44, 304–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Factor | Cancer Survivors’ Group | Control Group | p-Value a |
|---|---|---|---|
| Number of patients (n) (female/male ratio) | 40 (26/14) | 40 (26/14) | 1.000 |
| Median age (range) (years) | 19.4 (14–28) | 19.2 (14–28) | 0.889 |
| Orthodontic assessment (the same for both groups) | Skeletal class II: 26 patients each group Skeletal class I: 9 patients each group Skeletal class III: 5 patients each group | 1.000 | |
| Diagnosis | No of Cases | Mean Age at Diagnosis | Follow-up Time | Treatment Modality | |
|---|---|---|---|---|---|
| Chemotherapy | Radiotherapy | ||||
| Leukemia | 22 | 3.8 ± 1.3 | 9.5 ± 4.6 | 28 | 0 |
| Neuroblastoma | 3 | 0.7 ± 0.4 | 5.3 ± 1.1 | 4 | 0 |
| Soft tissue sarcoma | 3 | 2.2 ± 1.76 | 7.2 ± 2.0 | 4 | 1 |
| Non-Hodgkin’s lymphoma | 6 | 4.7 ± 2.1 | 8.0 ± 4.2 | 8 | 1 |
| Wilms tumor | 6 | 3.8 ± 2.2 | 6.1 ± 3.3 | 8 | 0 |
| The List of Questions in the OHIP-14 Questionnaire |
|---|
| Functional Limitation |
|
| Physical Pain |
|
| Psychological Discomfort |
|
| Physical Disability |
|
| Psychological Disability |
|
| Social Disability |
|
| Handicap |
|
| Time of Orthodontic Treatment (TX) | Cancer Survivors’ Group | Control Group | p-Value a |
|---|---|---|---|
| (mean ± SD) (Range) | (mean ± SD) (Range) | ||
| Before TX | 3.5 ± 3.9 1,2,3 | 3.7 ± 3.0 4,5,6 | 0.278 |
| (0–14) | (0–9) | ||
| 2 weeks after the onset of TX | 8.2 ± 8.9 1 | 8 ± 5.0 4 | 0.159 |
| (0–32) | (0–20) | ||
| 3 months after the onset of TX | 6.2 ± 7.9 2 | 6.2 ± 3.9 5 | 0.213 |
| (0–28) | (0–15) | ||
| After TX | 1.0 ± 2.5 3 | 0.6 ± 2.3 6 | 0.126 |
| (0–14) | (0–12) |
| OHIP-14 Domains | Functional Limitation | Physical Pain | Psychological Discomfort | Physical Disability | Psychological Disability | Social Disability | Handicap |
|---|---|---|---|---|---|---|---|
| Before (cancer survivors vs. control) | 0.3 ± 0.5 0.3 ± 0.6 | 0.1 ± 0.3 0.1 ± 0.3 | 0.4 ± 0.7 0.2 ± 0.5 | 0.9 ± 0.9 0.6 ± 0.9 | 0.7 ± 1.3 0.5 ± 0.8 | 0.4 ± 0.7 0.3 ± 0.6 | 0.8 ± 1.1 0.6 ± 0.9 |
| 2 weeks (cancer survivors vs. control) | 0.8 ± 0.9 0.9 ± 1.2 | 2.2 ± 2.7 1.6 ± 1.2 | 1.3 ± 2.0 1 0.3 ± 0.6 1 | 1.7 ± 1.6 1.2 ± 1.0 | 1.2 ± 1.6 1.0 ± 1.3 | 0.4 ± 0.8 0.4 ± 0.7 | 0.7 ± 1.3 0.5 ± 0.8 |
| 3 months (cancer survivors vs. control) | 0.4 ± 0.8 0.6 ± 0.9 | 1.6 ± 2.1 0.9 ± 0.9 | 1.0 ± 1.6 2 0.2 ± 0.9 2 | 1.4 ± 1.7 0.8 ± 1.0 | 1.0 ± 1.5 0.7 ± 0.9 | 0.4 ± 0.8 0.2 ± 0.5 | 0.5 ± 1.2 0.4 ± 0.6 |
| After (cancer survivors vs. control) | 0.1 ± 0.3 0.1 ± 1.4 | 0.2 ± 0.5 0.1 ± 0.3 | 0.2 ± 0.6 0.1 ± 0.3 | 0.3 ± 0.6 0.1 ± 0.4 | 0.1 ± 0.5 0.1 ± 0.3 | 0.1 ± 0.4 0.1 ± 0.4 | 0.1 ± 0.3 0.1 ± 0.4 |
| OHIP-14 Domains | Functional Limitation | Physical Pain | Psychological Discomfort | Physical Disability | Psychological Disability | Social Disability | Handicap |
|---|---|---|---|---|---|---|---|
| Before vs. after | <0.001 <0.001 | <0.001 <0.001 | <0.001 0.652 | <0.001 <0.001 | <0.001 0.004 | 0.156 0.342 | <0.001 <0.001 |
| Before vs. 2 weeks | <0.001 <0.001 | <0.001 <0.001 | <0.001 0.020 | <0.001 0.225 | <0.001 0.025 | 0.656 0.421 | 0.034 0.041 |
| Before vs. 3 months | <0.001 <0.001 | <0.001 <0.001 | <0.001 0.030 | <0.001 0.225 | 0.041 0.287 | 1 0.987 | 0.019 0.012 |
| OHIP-14 DOMAINS | Functional Limitation | Physical Pain | Psychological Discomfort | Physical Disability | Psychological Disability | Social Disability | Handicap |
|---|---|---|---|---|---|---|---|
| Before (cancer survivors vs. control) | 1 3 | 0 0 | 4 1 | 12 10 | 8 6 | 6 2 | 8 7 |
| 2 weeks (cancer survivors vs. control) | 6 11 | 16 17 | 13 1 2 1 | 22 19 | 13 11 | 5 4 | 6 3 |
| 3 months (cancer survivors vs. control) | 2 7 | 14 7 | 11 2 2 2 | 16 12 | 12 6 | 5 3 | 5 3 |
| After (cancer survivors vs. control) | 1 1 | 2 1 | 3 1 | 2 1 | 2 1 | 2 2 | 1 2 |
| Time of Orthodontic Treatment (TX) | Cancer Survivors’ Group | Control Group | p-Value |
|---|---|---|---|
| (Chi-Square Test) | |||
| Before | 6 (15.0%) | 3 (7.5%) | 0.289 |
| 2 weeks | 13 (32.5%) | 11 (27.5%) | 0.716 |
| 3 months | 11 (27.5%) | 6 (15.0%) | 0.172 |
| After the treatment | 2 (5.0%) | 1 (2.5%) | 0.556 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitus-Kenig, M.; Derwich, M.; Czochrowska, E.; Pawlowska, E. Quality of Life in Orthodontic Cancer Survivor Patients—A Prospective Case–Control Study. Int. J. Environ. Res. Public Health 2020, 17, 5824. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165824
Mitus-Kenig M, Derwich M, Czochrowska E, Pawlowska E. Quality of Life in Orthodontic Cancer Survivor Patients—A Prospective Case–Control Study. International Journal of Environmental Research and Public Health. 2020; 17(16):5824. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165824
Chicago/Turabian StyleMitus-Kenig, Maria, Marcin Derwich, Ewa Czochrowska, and Elzbieta Pawlowska. 2020. "Quality of Life in Orthodontic Cancer Survivor Patients—A Prospective Case–Control Study" International Journal of Environmental Research and Public Health 17, no. 16: 5824. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165824