Short and Long-Term Trainability in Older Adults: Training and Detraining Following Two Years of Multicomponent Cognitive—Physical Exercise Training

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
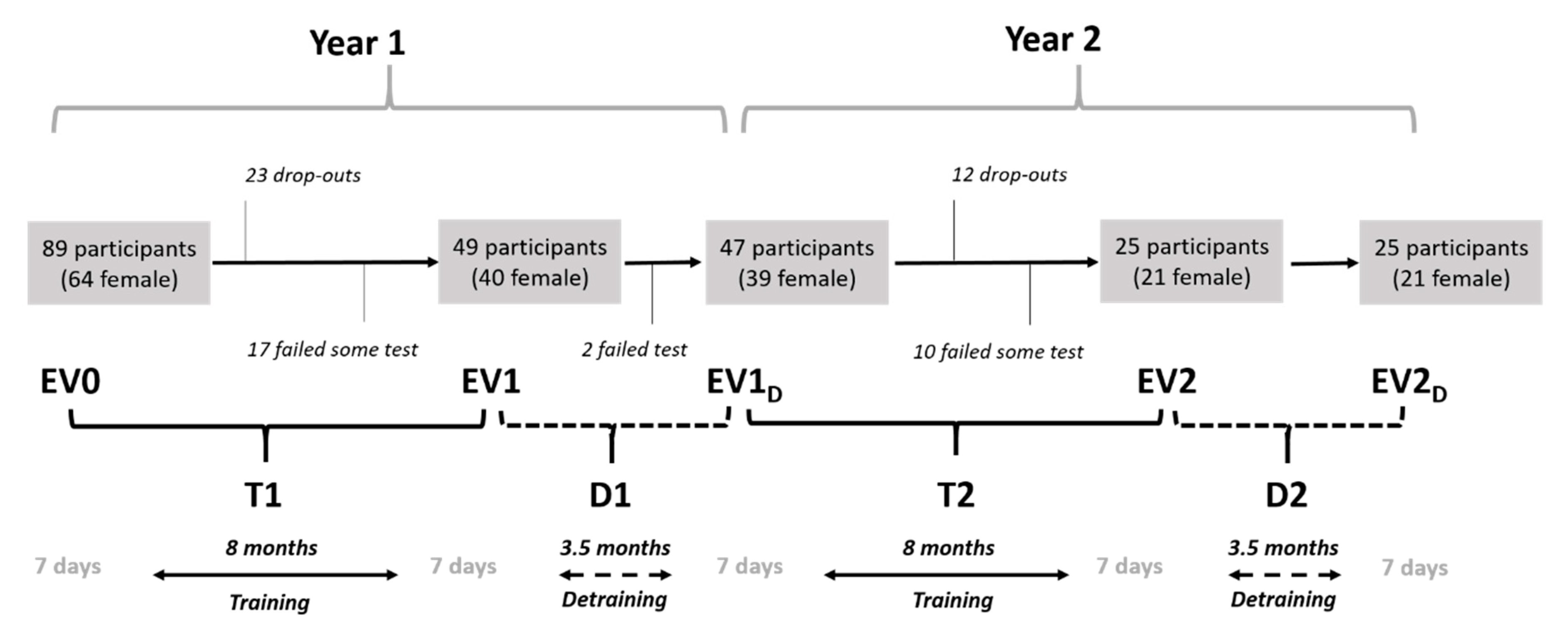
2.1. Experimental Approach
2.2. Participants
2.3. Procedures and Performance Outcomes
2.4. MCcogTP Intervention
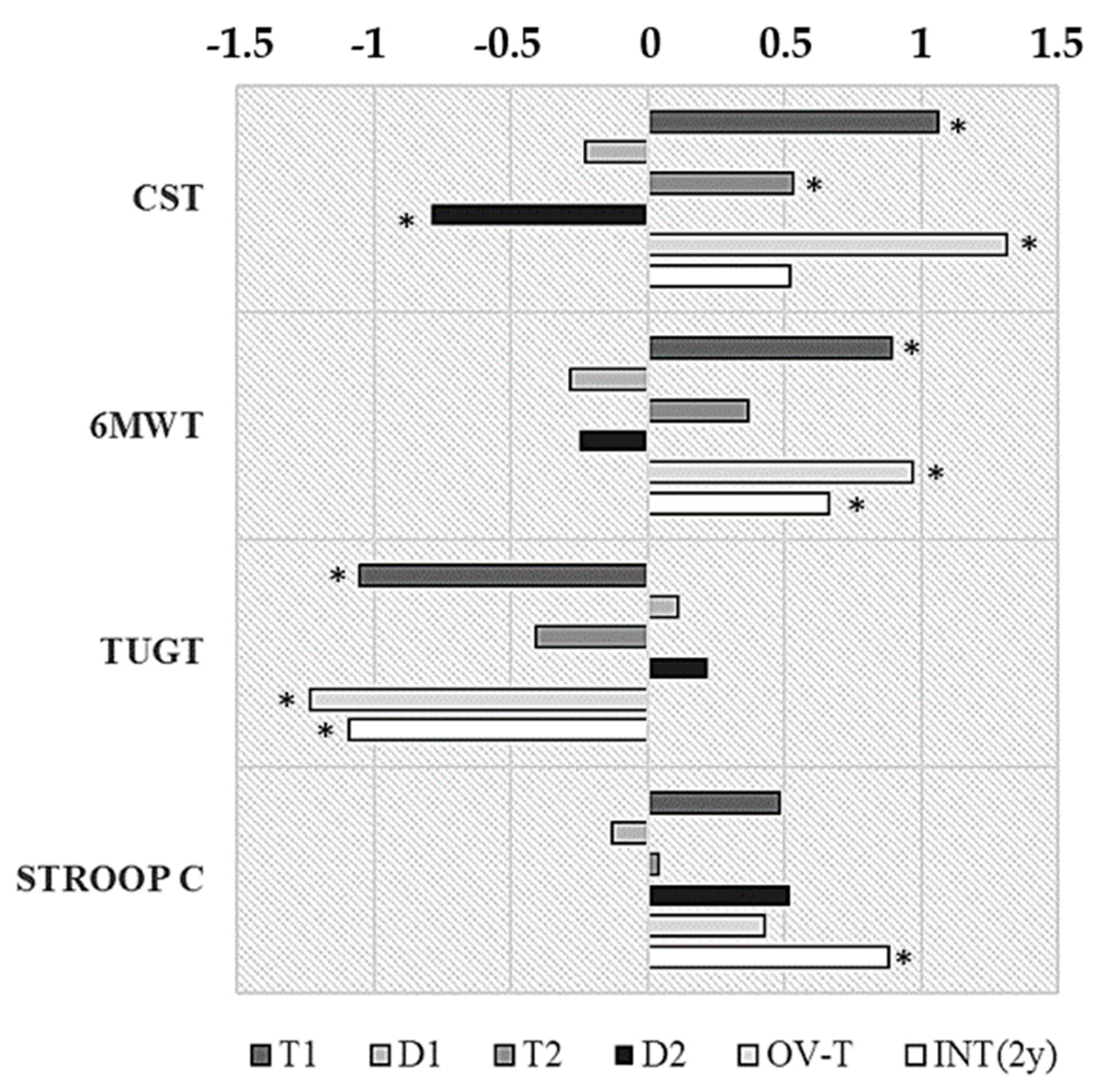
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blasco-Lafarga, C.; Martínez-Navarro, I.; Sisamón, M.E.; Caus, N.; Yangüez, E.; Llorens-Soriano, P. Linear and nonlinear heart rate dynamics in elderly inpatients. Relations with comorbidity and depression. Medicina 2010, 46, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, B.K.; Berger, S.L.; Brunet, A.; Campisi, J.; Cuervo, A.M.; Epel, E.S.; Franceschi, C.; Lithgow, G.J.; Morimoto, R.I.; Pessin, J.E.; et al. Geroscience: Linking aging to chronic disease. Mol. Cell 2014, 159, 709–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avers, D.; Brown, M.; Chui, K.; Wong, R.A.; Lusardi, M.M. Use of the Term “Elderly”. J. Geriatr. Phys. Ther. 2011, 34, 2. [Google Scholar] [CrossRef] [PubMed]
- Blasco-Lafarga, C. Fundamentación teórica del Entrenamiento Funcional en los Adultos Mayores; Fundamentals of training in older adults (neurophysiology and integrative responses to physical exercise). In El Entrenamiento Funcional en los Adultos Mayores II, Jornadas; [CD-ROM]; Blasco-Lafarga, C., Ed.; UIRFIDE/GIEFAM (Physical Education and Sports Department) University of Valencia: Valencia, Spain, 2013; p. 44. [Google Scholar]
- Yashin, A.I.; Arbeev, K.G.; Arbeeva, L.S.; Wu, D.; Akushevich, I.; Kovtun, M.; Yashkin, A.; Kulminski, A.; Culminskaya, I.; Stallard, E.; et al. How the effects of aging and stresses of life are integrated in mortality rates: Insights for genetic studies of human health and longevity. Biogerontology 2016, 17, 89–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fajemiroye, J.O.; Da Cunha, L.C.; Saavedra-Rodríguez, R.; Rodrigues, K.L.; Naves, L.M.; Mourão, A.A.; Da Silva, E.F.; Williams, N.E.E.; Martins, J.L.R.; Sousa, R.B.; et al. Aging-induced biological changes and cardiovascular diseases. BioMed Res. Int. 2018, 2018, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haigis, M.C.; Yankner, B.A. The aging stress response. Mol. Cell 2010, 40, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Frontera, W.R. Physiologic Changes of the Musculoskeletal System with Aging: A Brief Review. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 705–711. [Google Scholar] [CrossRef]
- Lazarus, N.R.; Lord, J.M.; Harridge, S.D. The relationships and interactions between age, exercise and physiological function. J. Phys. 2019, 597, 1299–1309. [Google Scholar] [CrossRef] [Green Version]
- Boros, K.; Freemont, T. Physiology of ageing of the musculoskeletal system. Best Pract. Res. Clin. Rheumatol. 2017, 31, 203–217. [Google Scholar] [CrossRef]
- Zullo, A.; Fleckenstein, J.; Schleip, R.; Hoppe, K.; Wearing, S. Structural and functional changes in the coupling of fascial tissue, skeletal muscle, and nerves during aging. Front. Phys. 2020, 11, 592. [Google Scholar] [CrossRef]
- Laranjo, S.; Geraldes, V.; Oliveira, M.; Rocha, I. Insights into the background of autonomic medicine. Rev. Port. Cardiol. 2017, 36, 757–771. [Google Scholar] [CrossRef] [PubMed]
- Aiello, A.; Farzaneh, F.; Candore, G.; Caruso, C.; Davinelli, S.; Gambino, C.M.; Ligotti, M.E.; Zareian, N.; Accardi, G. The immunosenescence and its hallmarks: How to oppose ageing strategically? A review of potential options for therapeutic intervention. Front. Immunol. 2019, 10, 2247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauman, A.; Merom, D.; Bull, F.; Buchner, D.; Fiatarone Singh, M. Updating the Evidence for Physical Activity: Summative Reviews of the Epidemiological Evidence, Prevalence, and Interventions to Promote “Active Aging”. Gerontologist 2016, 56, S268–S280. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, N.R.; Izquierdo, M.; Higginson, I.J.; Harridge, S.D. Exercise deficiency diseases of ageing: The primacy of exercise and muscle strengthening as first-line therapeutic agents to combat frailty. J. Am. Med. Dir. Assoc. 2018, 19, 741–743. [Google Scholar] [CrossRef] [PubMed]
- Sellami, M.; Gasmi, M.; Denham, J.; Hayes, L.D.; Stratton, D.; Padulo, J.; Bragazzi, N. Effects of acute and chronic exercise on immunological parameters in the elderly aged: Can physical activity counteract the effects of aging? Front. Immunol. 2018, 9, 2187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garatachea, N.; Pareja-Galeano, H.; Sanchis-Gomar, F.; Santos-Lozano, A.; Fiuza-Luces, C.; Morán, M.; Emanuele, E.; Joyner, M.J.; Lucia, A. Exercise attenuates the major hallmarks of aging. Rejuvenation Res. 2015, 18, 57–89. [Google Scholar] [CrossRef] [Green Version]
- Valenzuela, P.L.; Morales, J.S.; Pareja-Galeano, H.; Izquierdo, M.; Emanuele, E.; de la Villa, P.; Lucia, A. Physical strategies to prevent disuse-induced functional decline in the elderly. Ageing Res. Rev. 2018, 47, 80–88. [Google Scholar] [CrossRef]
- Forte, R.; Boreham, C.; Costa-Leite, J.; De Vito, G.; Brennan, L.; Gibney, E.; Pesce, C. Enhancing cognitive functioning in the elderly: Multicomponent vs resistance training. Clin. Interv. Aging 2013, 8, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Falck, R.S.; Davis, J.C.; Best, J.R.; Crockett, R.A.; Liu-Ambrose, T. Impact of exercise training on physical and cognitive function among older adults: A systematic review and meta-analysis. Neurobiol. Aging 2019, 79, 119–130. [Google Scholar] [CrossRef]
- Langlois, F.; Minh Vu, T.; Chassé, K.; Dupuis, G.; Kergoat, M.; Bherer, L. Benefits of Physical Exercise Training on Cognition and Quality of Life in Frail Older Adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2012, 68, 400–404. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hortobágyi, T.; Lesinski, M.; Gäbler, M.; VanSwearingen, J.; Malatesta, D.; Granacher, U. Effects of Three Types of Exercise Interventions on Healthy Old Adults’ Gait Speed: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1627–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, L.; Hortobagyi, T.; la Bastide-van Gemert, S.; van der Zee, E.; van Heuvelen, M. Dose-response relationship between exercise and cognitive function in older adults with and without cognitive impairment: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0210036. [Google Scholar] [CrossRef] [PubMed]
- Farrance, C.; Tsofliu, F.; Clark, C. Adherence to community based group exercise interventions for older people: A mixed-methods systematic review. Prev. Med. 2016, 87, 155–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamada, M.; Shiroma, E.; Buring, J.; Miyachi, M.; Lee, I. Strength Training and All-Cause, Cardiovascular Disease, and Cancer Mortality in Older Women: A Cohort Study. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef] [Green Version]
- Bouaziz, W.; Lang, P.; Schmitt, E.; Kaltenbach, K.; Geny, B.; Vogel, T. Health benefits of multicomponent training programmes in seniors: A systematic review. Int. J. Clin. Pract. 2016, 70, 520–536. [Google Scholar] [CrossRef]
- Fragala, M.; Cadore, E.; Dorgo, S.; Izquierdo, M.; Kraemer, W.; Peterson, M.; Ryan, E. Resistance training for older adults: Position statement from the National strength and conditioning association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Levin, O.; Netz, Y.; Ziv, G. The beneficial effects of different types of exercise interventions on motor and cognitive functions in older age: A systematic review. Eur. Rev. Aging Phys. Act. 2017, 14, 1–23. [Google Scholar] [CrossRef]
- Eggenberger, P.; Theill, N.; Holenstein, S.; Schumacher, V.; de Bruin, E.D. Multicomponent physical exercise with simultaneous cognitive training to enhance dual-task walking of older adults: A secondary analysis of a 6-month randomized controlled trial with 1-year follow-up. Clin. Interv. Aging 2015, 10, 1711–1732. [Google Scholar] [CrossRef] [Green Version]
- Larsen, L.; Schou, L.; Lund, H.; Langberg, H. The Physical Effect of Exergames in Healthy Elderly—A Systematic Review. Games Health J. 2013, 2, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Fang, Q.; Ghanouni, P.; Anderson, S.E.; Touchett, H.; Shirley, R.; Fang, F.; Fang, C. Effects of exergaming on balance of healthy older adults: A systematic review and meta-analysis of randomized controlled trials. Games Health J. 2020, 9, 11–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, R.; Santa-Marinha, C.; Leão, R.; Monteiro, D.; Bento, T.; Santos Rocha, R.; Brito, J. Exercise training programs and detraining in older women. J. Hum. Sport Exerc. 2017, 12, 142–155. [Google Scholar] [CrossRef] [Green Version]
- Leitão, L.; Brito, J.; Leitão, A.; Pereira, A.; Conceição, A.; Silva, A.; Louro, H. Functional capacity retention in older women after multicomponent exercise cessation: 3-year longitudinal study. Motricidade 2015, 11, 81–91. [Google Scholar] [CrossRef] [Green Version]
- de Lemos Muller, C.H.; de Matos, J.R.; Grigolo, G.B.; Schroeder, H.T.; Rodrigues-Krause, J.; Krause, M. Exercise Training for the Elderly: Inflammaging and the Central Role for HSP70. J. Sci. Sport Exerc. 2019, 1, 97–115. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, G.; Hardman, R.J.; Macpherson, H.; Scholey, A.B.; Pipingas, A. How does exercise reduce the rate of age-associated cognitive decline? A review of potential mechanisms. J. Alzheimer’s Dis. 2017, 55, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Stillman, C.M.; Donofry, S.D.; Erickson, K.I. Exercise, fitness and the aging brain: A review of functional connectivity in aging. Arch. Psychol. 2019, 3. [Google Scholar] [CrossRef]
- Delshad, M.; Ghanbarian, A.; Mehrabi, Y.; Sarvghadi, F.; Ebrahim, K. Effect of Strength Training and Short-term Detraining on Muscle Mass in Women Aged Over 50 Years Old. Int. J. Prev. Med. 2013, 4, 1386. [Google Scholar]
- Blasco-Lafarga, C.; Martinez-Navarro, I.; Cordellat, A.; Roldán, A.; Monteagudo, P.; Sanchis-Soler, G.; Sanchis-Sanchis, R. Método de Entrenamiento Funcional Cognitivo Neuromotor; Propiedad Intelectual nº156069; Universitat de València: Valencia, Spain, 2016. [Google Scholar]
- Blasco-Lafarga, C.; Monteagudo, P.; Roldán, A.; Cordellat, A.; Pesce, C. Strategies to change body composition in older adults: Do type of exercise and dose distribution matter? J. Sports Med. Phys. Fit. 2020, 60, 552. [Google Scholar]
- Blasco-Lafarga, C.; Sanchis-Sanchis, R.; Sanchis-Soler, G.; San Inocencio-Cuenca, D.; Llorens-Soriano, P. Entrenamiento Neuromotor en pacientes ancianos pluripatológicos en las Unidades de Hospitalización a Domicilio: Estudio piloto. Cuadernos de Psicología del Deporte 2019, 19, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Monteagudo, P.; Cordellat, A.; Roldán, A.; Gómez-Cabrera, M.; Blasco-Lafarga, C. Effects of multicomponent exercise on metabolic health parameters in elderly. MOJ Sports Med. 2019, 3, 70–74. [Google Scholar]
- Roldán, A.; Cordellat, A.; Monteagudo, P.; García-Lucerga, C.; Blasco-Lafarga, N.M.; Gomez-Cabrera, M.C.; Blasco-Lafarga, C. Beneficial Effects of Inspiratory Muscle Training Combined With Multicomponent Training in Elderly Active Women. Res. Q. Exerc. Sport 2019, 90, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Sanchis, R.; Blasco-Lafarga, C.; Camacho-García, A.; Encarnación-Martínez, A.; Pérez-Soriano, P. Evaluation of impact-shock on gait after the implementation of two different training programs in older adults. Clin. Biomech. 2020, 80, 105131. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Sanchis, R.; Blasco-Lafarga, C.; Encarnación-Martínez, A.; Pérez-Soriano, P. Changes in plantar pressure and spatiotemporal parameters during gait in older adults after two different training programs. Gait Posture 2020, 77, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Blasco-Lafarga, C.; Monteagudo, P.; Blasco-Lafarga, N.; Cordellat, A.; Roldán, A. Función ejecutiva, capacidad cardiovascular y calidad de vida en mayores del entorno rural: Impacto de un programa multidisciplinar. Comunidad 2016, 18, 1–6. [Google Scholar]
- Sanchis-Soler, G.; San Inocencio-Cuenca, D.; Llorens-Soriano, P.; Blasco-Lafarga, C. Reducción de la sobrecarga del cuidador tras entrenamiento supervisado en ancianos pluripatológicos y paliativos. Cuadernos de Psicología del Deporte 2021, CPD1(2021). in press. [Google Scholar]
- Patil, R.; Uusi-Rasi, K.; Tokola, K.; Karinkanta, S.; Kannus, P.; Sievänen, H. Effects of a Multimodal Exercise Program on Physical Function, Falls, and Injuries in Older Women: A 2-Year Community-Based, Randomized Controlled Trial. J. Am. Geriatr. Soc. 2015, 63, 1306–1313. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and validation of a functional fitness test for community-residing older adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Comalli, P., Jr.; Wapner, S.; Werner, H. Interference Effects of Stroop Color-Word Test in Childhood, Adulthood, and Aging. J. Genet. Psychol. 1962, 100, 47–53. [Google Scholar] [CrossRef]
- Platonov, V. Teoría General Del Entrenamiento Deportivo Olímpico; Paidotribo: Barcelona, Spain, 2001. [Google Scholar]
- Martínez-Navarro, I. Efectos De Un Programa De Entrenamiento Funcional Sobre La Variablidad De La Frecuencia Cardíaca, La Función Ejecutiva Y La Capacidad Condicional En Los Adultos Mayores. Ph.D. Thesis, Universitat de València, Valencia, Spain, 2014. [Google Scholar]
- Cordellat, A.; Roldán, A.; Monteagudo, P.; Daltell, A.; Blasco-Lafarga, C. Pruebas T vs análisis categorial: Evolución de la agilidad en los adultos mayores tras dos años de entrenamiento (T test vs categorical analysis: Evolution of agility in older adults following two years of training). Retos 2020, 39. [Google Scholar] [CrossRef]
- Magistro, D.; Candela, F.; Brustio, P.R.; Liubicich, M.E.; Rabaglietti, E. A Longitudinal Study on the Relationship Between Aerobic Endurance and Lower Body Strength in Italian Sedentary Older Adults. J. Aging Phys. Act. 2015, 23, 444–451. [Google Scholar] [CrossRef] [Green Version]
- Bouaziz, W.; Vogel, T.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Lang, P. Health benefits of aerobic training programs in adults aged 70 and over: A systematic review. Arch. Gerontol. Geriatr. 2017, 69, 110–127. [Google Scholar] [CrossRef] [PubMed]
- Coetsee, C.; Terblanche, E. The time course of changes induced by resistance training and detraining on muscular and physical function in older adults. Eur. Rev. Aging Phys. Act. 2015, 12, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Rikli, R.E.; Jones, C.J. Development and Validation of Criterion-Referenced Clinically Relevant Fitness Standards for Maintaining Physical Independence in Later Years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Leitão, L.; Pereira, A.; Mazini, M.; Venturini, G.; Campos, Y.; Vieira, J.; Novaes, J.; Vianna, J.; da Silva, S.; Louro, H. Effects of Three Months of Detraining on the Health Profile of Older Women after a Multicomponent Exercise Program. Int. J. Environ. Res. Public Health 2019, 16, 3881. [Google Scholar] [CrossRef] [Green Version]
- Donath, L.; van Dieën, J.; Faude, O. Exercise-Based Fall Prevention in the Elderly: What About Agility? Sports Med. 2016, 46, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geirsdottir, O.; Arnarson, A.; Ramel, A.; Briem, K.; Jonsson, P.; Thorsdottir, I. Muscular strength and physical function in elderly adults 6–18 months after a 12-week resistance exercise program. Scand. J. Public Health 2015, 43, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.; Loughrey, D.; Lawlor, B.; Robertson, I.; Walsh, C.; Brennan, S. The impact of exercise on the cognitive functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2014, 16, 12–31. [Google Scholar] [CrossRef]
- Morita, E.; Yokoyama, H.; Imai, D.; Takeda, R.; Ota, A.; Kawai, E.; Suzuki, Y.; Okazaki, K. Effects of 2-Year Cognitive–Motor Dual-Task Training on Cognitive Function and Motor Ability in Healthy Elderly People: A Pilot Study. Brain Sci. 2018, 8, 86. [Google Scholar] [CrossRef] [Green Version]
- Martin, M.; Clare, L.; Altgassen, A.; Cameron, M.; Zehnder, F. Cognition-based interventions for healthy older people and people with mild cognitive impairment. Cochrane Database Syst. Rev. 2011, 11, cd006220. [Google Scholar] [CrossRef]
- Northey, J.; Cherbuin, N.; Pumpa, K.; Smee, D.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef]
- López-Sáez de Asteasu, M.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, A.; Izquierdo, M. Role of physical exercise on cognitive function in healthy older adults: A systematic review of randomized clinical trials. Ageing Res. Rev. 2017, 37, 117–134. [Google Scholar] [CrossRef] [PubMed]
- Best, J.; Nagamatsu, L.; Liu-Ambrose, T. Improvements to executive function during exercise training predict maintenance of physical activity over the following year. Front. Aging Neurosci. 2014, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho Júnior, H.; Rodrigues, B.; Gonçalves, I.; Uchida, M. Effects of a short-term detraining period on muscle functionality and cognition of strength-trained older women: A preliminary report. J. Exerc. Rehabil. 2017, 3, 559–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frändin, K.; Grönstedt, H.; Helbostad, J.; Bergland, A.; Andresen, M.; Puggaard, L.; Harms-Ringdahl, K.; Granbo, R.; Hellström, K. Long-Term Effects of Individually Tailored Physical Training and Activity on Physical Function, Well-Being and Cognition in Scandinavian Nursing Home Residents: A Randomized Controlled Trial. Gerontology 2016, 62, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Toraman, N.F. Short term and long term detraining: Is there any difference between young-old and old people? Br. J. Sports Med. 2005, 39, 561–564. [Google Scholar] [CrossRef]
- Nordgren, B.; Fridén, C.; Demmelmaier, I.; Bergström, G.; Lundberg, I.; Nessen, T.; Dufour, A.; Opava, C. An Outsourced Health-enhancing Physical Activity Program for People with Rheumatoid Arthritis: Study of the Maintenance Phase. J. Rheumatol. 2018, 45, 1093–1100. [Google Scholar] [CrossRef]
- 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; ODPHP, Ed.; US Department of Health and Human Services: Washington, DC, USA, 2018; p. 779. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | EV0 | CV (%) | EV2D | CV (%) | p | d |
|---|---|---|---|---|---|---|
| Weight (kg) | 66.02 (10.03) | 15.19 | 65.09 (9.15) | 14.06 | 0.20 | −0.10 |
| Height (m) | 1.56 (0.07) | 4.49 | 1.55 (0.07) | 4.52 | 0.30 | −0.14 |
| Lean Body Mass (kg) | 40.67 (7.11) | 17.48 | 41.08 (7.35) | 17.9 | 0.52 | 0.06 |
| Fat Mass (kg) | 34.97 (5.80) | 16.59 | 32.85 (5.56) | 16.93 | 0.02 | −0.37 |
| SBP (mmHg) | 133.75 (25.11) | 18.77 | 123.14 (12.21) | 9.92 | 0.04 | −0.54 |
| DBP (mmHg) | 75.79 (11.40) | 15.04 | 71.43 (8.34) | 11.68 | 0.02 | −0.44 |
| Tests of Within-Subjects Effects | |||||||
|---|---|---|---|---|---|---|---|
| Intervention | Variables | Type III Sum of Squares | Df | Mean Square | F | p | Partial eta Square |
| 6MWT | 56,455.07 | 4 | 14,113.77 | 14.33 | 0.001 | 0.46 | |
| CST | 279.62 | 4 | 67.65 | 14.2 | 0.001 | 0.44 | |
| TUGT | 29.01 | 4 | 7.25 | 16.45 | 0.001 | 0.46 | |
| STROOPT | 644.43 | 4 | 161.11 | 5.27 | 0.001 | 0.32 | |
| Sampling Conditions | CST (rep) | CV (%) | TUGT (s) | CV (%) | 6MWT (m) | CV (%) | STROOPT (a.u) | CV (%) |
|---|---|---|---|---|---|---|---|---|
| EV0 | 15.47 (3.13) a,b,c | 20.23 | 6.9 (1.54) a,b,c,d | 22.32 | 507.61 (73.8) a,b,c,d | 14.54 | 28.92 (9.22) d | 31.88 |
| EV1 | 19.13 (3.75) | 19.6 | 5.60 (0.83) | 14.82 | 571.86 (70.6) | 12.35 | 34.17 (12.5) | 36.58 |
| ∆T1 | 23.65% | −18.84% | 12.65% | 18.15% | ||||
| EV1D | 18.26 (3.71) c | 20.32 | 5.68 (0.54) | 9.51 | 551.67 (74.5) | 13.5 | 32.58 (12.32) | 37.81 |
| ∆D1 | −4.54% | 1.43% | −3.53% | −4.65% | ||||
| EV2 | 20.45 (4.43) d | 21.66 | 5.42 (0.72) | 13.28 | 579.17 (74.13) | 12.8 | 33 (9.81) | 29.73 |
| ∆T2 | 11.99% | −4.58% | 4.98% | 1.29% | ||||
| EV2D | 17.24 (3.61) | 20.94 | 5.58 (0.74) | 13.26 | 559.17 (83.2) | 14.88 | 39.08 (13.43) | 34.37 |
| ∆D2 | −15.7% | 2.95% | −3.45% | 18.42% | ||||
| ∆ OV-T | 32.19% | −21.45% | 14.08% | 14.11% | ||||
| ∆ Int-2y | 11.44% | −19.13% | 10.16% | 35.13% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blasco-Lafarga, C.; Cordellat, A.; Forte, A.; Roldán, A.; Monteagudo, P. Short and Long-Term Trainability in Older Adults: Training and Detraining Following Two Years of Multicomponent Cognitive—Physical Exercise Training. Int. J. Environ. Res. Public Health 2020, 17, 5984. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165984
Blasco-Lafarga C, Cordellat A, Forte A, Roldán A, Monteagudo P. Short and Long-Term Trainability in Older Adults: Training and Detraining Following Two Years of Multicomponent Cognitive—Physical Exercise Training. International Journal of Environmental Research and Public Health. 2020; 17(16):5984. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165984
Chicago/Turabian StyleBlasco-Lafarga, Cristina, Ana Cordellat, Anabel Forte, Ainoa Roldán, and Pablo Monteagudo. 2020. "Short and Long-Term Trainability in Older Adults: Training and Detraining Following Two Years of Multicomponent Cognitive—Physical Exercise Training" International Journal of Environmental Research and Public Health 17, no. 16: 5984. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165984