Perception of Gingival Bleeding by People and Healthcare Professionals: A Multicentre Study in an Adult French Population

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants, Settings, and Administration of the Questionnaire
- North region, with the city of Paris, the French capital (2,206,000 inhabitants, the first French city)
- South region, with the city of Montpellier (278,000 inhabitants, the seventh French city)
- West region, with the city of Rennes (215,000 inhabitants, the eleventh French city)
- East region, with the city of Nancy (105,000 inhabitants, the forty-second French city)
2.3. Survey Instrument
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Participants
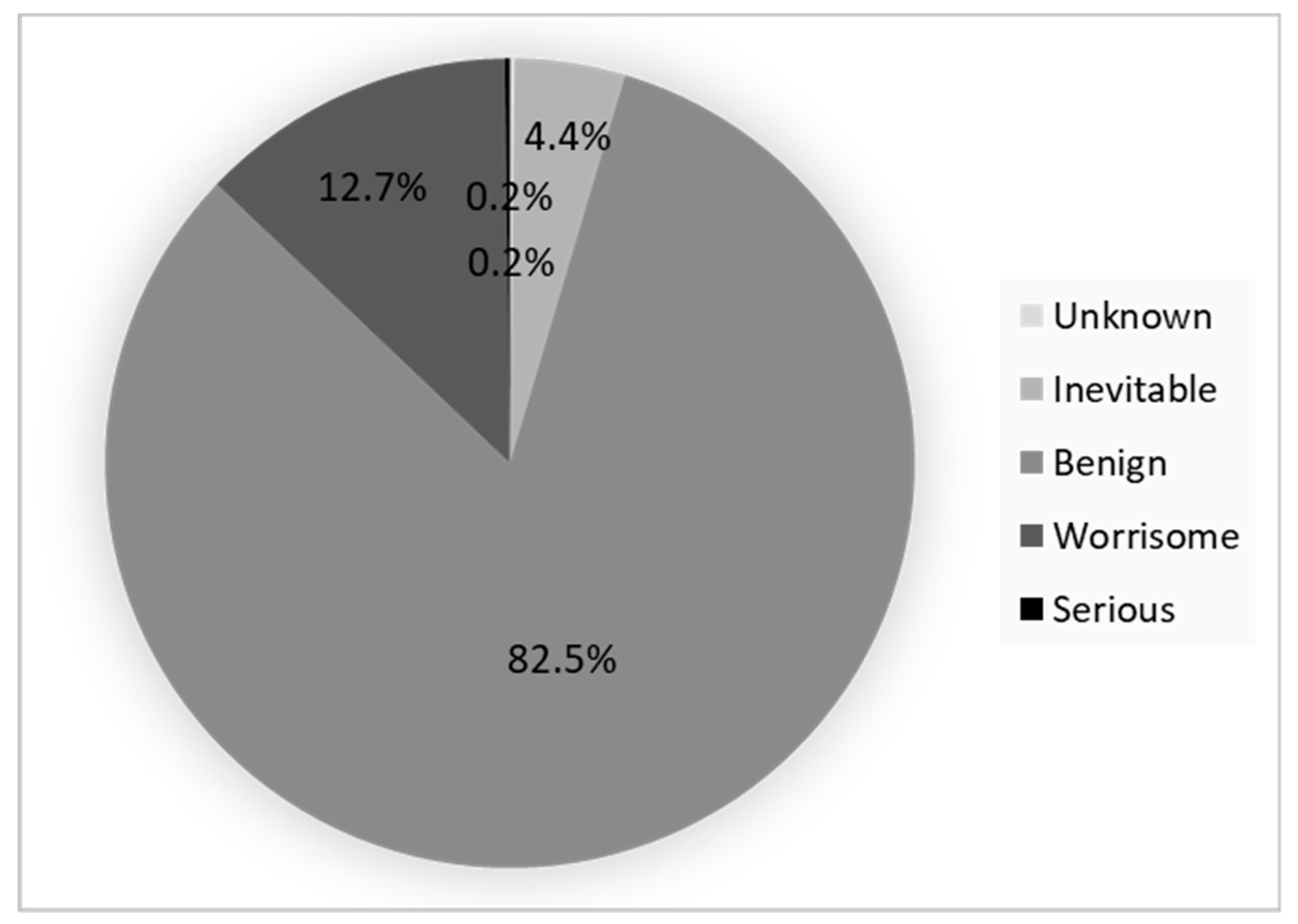
3.2. Perception and Responses to the GB among Population GB Positive
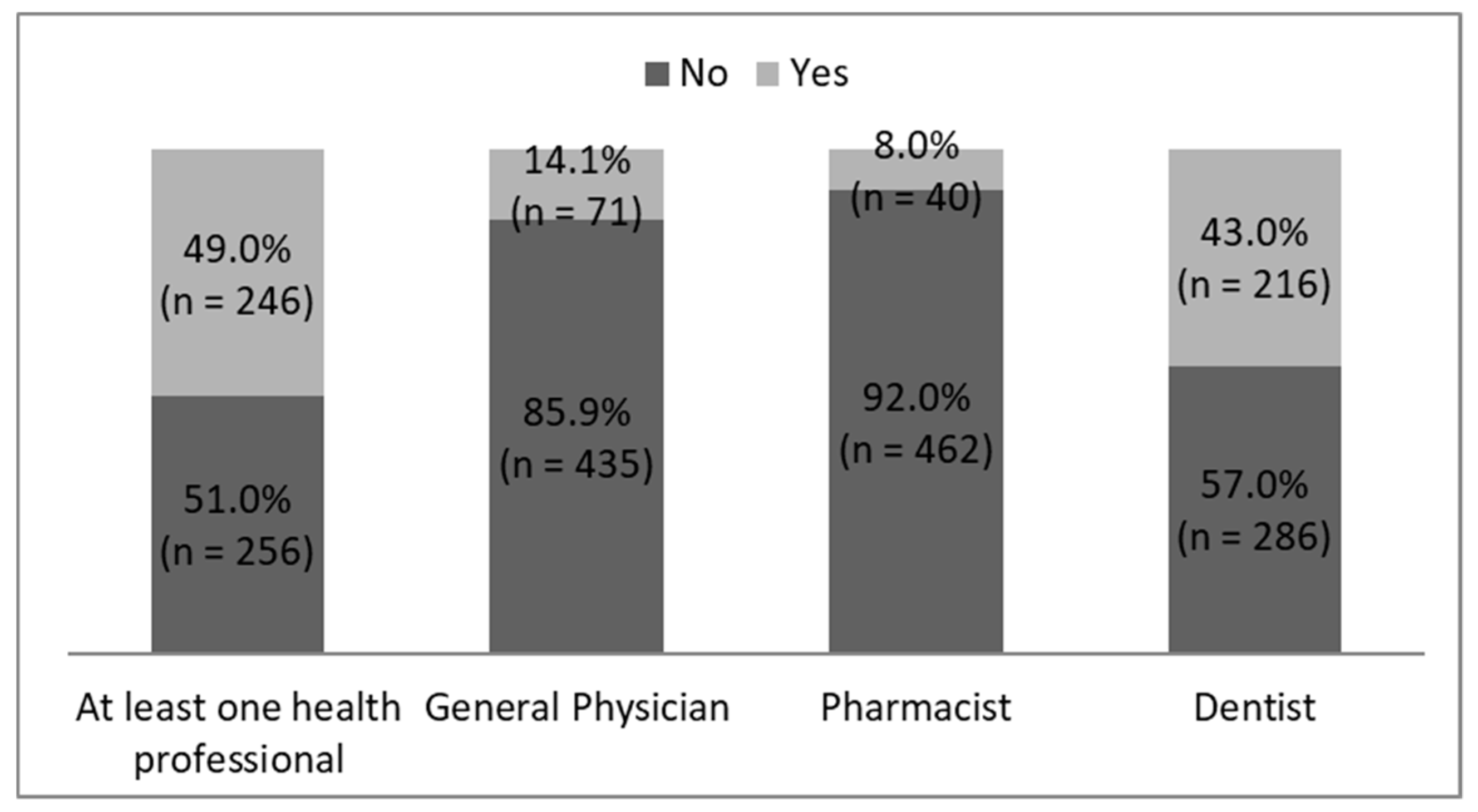
3.3. Healthcare Professionals Responses to the GB Reported by Their Patient
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marcenes, W.; Kassebaum, N.J.; Bernabé, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.J. Global burden of oral conditions in 1990–2010: A systematic analysis. J. Dent. Res. 2013, 92, 592–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourgeois, D.; Bouchard, P.; Mattout, C. Epidemiology of periodontal status in dentate adults in France, 2002–2003. J. Periodont. Res. 2007, 42, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.; Yu, W.H.; Lakshmanan, A.; Wade, W.G. The Human Oral Microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef] [Green Version]
- Verma, D.; Garg, P.K.; Dubey, A.K. Insights into the human oral microbiome. Arch. Microbiol. 2018, 4, 525–540. [Google Scholar] [CrossRef]
- Vieira Colombo, A.P.; Magalhães, C.B.; Hartenbach, F.A.; Martins do Souto, R.; Maciel da Silva-Boghossian, C. Periodontal-disease-associated biofilm: A reservoir for pathogens of medical importance. Microb. Pathog. 2016, 94, 27–34. [Google Scholar] [CrossRef]
- Arimatsu, K.; Yamada, H.; Miyazawa, H.; Minagawa, T.; Nakajima, M.; Ryder, M.; Gotoh, K.; Motooka, D.; Nakamura, S.; Iida, T.; et al. Oral pathobiont induces systemic inflammation and metabolic changes associated with alteration of gut microbiota. Sci. Rep. 2014, 4, 4828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Dominy, S.S.; Lynch, C.; Ermini, F.; Benedyk, M.; Marczyk, A.; Konradi, A.; Nguyen, M.; Haditsch, U.; Raha, D.; Griffin, C.; et al. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Sci. Adv. 2019, 5, eaau3333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, L.A.; Demerath, E.; Bittner-Eddy, P.; Costalonga, M. Placental colonization with periodontal pathogens: The potential missing link. Am. J. Obstet. Gynecol. 2019, 5, 383–392. [Google Scholar] [CrossRef]
- Joshi, C.; Bapat, R.; Anderson, W.; Dawson, D.; Hijazi, K.; Cherukara, G. Detection of periodontal microorganisms in coronary atheromatous plaque specimens of myocardial infarction patients: A systematic review and meta-analysis. Trends Cardiovasc. Med. 2019. [Google Scholar] [CrossRef]
- Araújo, V.M.; Melo, I.M.; Lima, V. Relationship between Periodontitis and Rheumatoid Arthritis: Review of the Literature. Mediat. Inflamm. 2015, 2015, 259074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal Pathogens as Risk Factors of Cardiovascular Diseases, Diabetes, Rheumatoid Arthritis, Cancer, and Chronic Obstructive Pulmonary Disease—Is There Cause for Consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Aiuto, F.; Gkranias, N.; Bhowruth, D.; Khan, T.; Orlandi, M.; Suvan, J.; Masi, S.; Tsakos, G.; Hurel, S.; Hingorani, A.D.; et al. Systemic effects of periodontitis treatment in patients with type 2 diabetes: A 12 month, single-centre, investigator-masked, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 954–965. [Google Scholar] [CrossRef]
- Dumitrescu, A.L. Depression and inflammatory periodontal disease considerations-an interdisciplinary approach. Front. Psychol. 2016, 7, 347. [Google Scholar] [CrossRef] [Green Version]
- Lund Håheim, L.; Schwarze, P.E.; Thelle, D.S.; Nafstad, P.; Rønningen, K.S.; Olsen, I. Low levels of antibodies for the oral bacterium Tannerella forsythia predict cardiovascular disease mortality in men with myocardial infarction: A prospective cohort study. Med. Hypotheses 2020, 138, 109575. [Google Scholar] [CrossRef]
- Dong, M.; Loignon, C.; Levine, A.; Bedos, C. Perceptions of oral illness among Chinese immigrants in Montreal: A qualitative study. J. Dent. Educ. 2007, 71, 1340–1347. [Google Scholar] [CrossRef]
- Corah, N.L. Development of a dental anxiety scale. J. Dent. Res. 1969, 48, 596. [Google Scholar] [CrossRef]
- Corah, N.L.; Gale, E.N.; Illig, S.J. Assessment of a dental anxiety scale. J. Am. Dent. Assoc. 1978, 97, 816–819. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Institut National de la Statistique et des Etudes Economiques (INSEE). Population par sexe et Groupe d’âges. 2020. Available online: https://www.insee.fr/fr/statistiques/2381474 (accessed on 12 April 2020).
- Institut National de la Statistique et des Etudes Economiques (INSEE). Catégorie Socioprofessionnelle selon le sexe et l’âge. 2019. Available online: https://www.insee.fr/fr/statistiques/2489546 (accessed on 12 April 2020).
- Blicher, B.; Joshipura, K.; Eke, P. Validation of self-reported periodontal disease: A systematic review. J. Dent. Res. 2005, 84, 881–890. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Gift, H.C. Awareness and assessment of periodontal problems among dentists and the public. Int. Dent. J. 1988, 38, 147–153. [Google Scholar] [PubMed]
- Taani, D.Q. Periodontal awareness and knowledge, and pattern of dental attendance among adults in Jordan. Int. Dent. J. 2002, 52, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.C.; Dias-Pereira, A.C.; Branco-de-Almeida, L.S.; Martins, C.C.; Paiva, S.M. Impact of periodontal disease on quality of life: A systematic review. J. Periodont. Res. 2017, 52, 651–665. [Google Scholar] [CrossRef]
- Acharya, S. Oral health-related quality of life and its associated factors in an Indian adult population. Oral Health Prev. Dent. 2008, 6, 175–184. [Google Scholar]
- Figuero, E.; Herrera, D.; Tobías, A.; Serrano, J.; Roldán, S.; Escribano, M.; Martín, C. Efficacy of adjunctive anti-plaque chemical agents in managing gingivitis: A systematic review and network meta-analyses. J. Clin. Periodontol. 2019, 46, 723–739. [Google Scholar] [CrossRef]
- James, P.; Worthington, H.V.; Parnell, C.; Harding, M.; Lamont, T.; Cheung, A.; Whelton, H.; Riley, P. Chlorhexidine mouthrinse as an adjunctive treatment for gingival health. Cochrane Database Syst. Rev. 2017, 3, CD008676. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Van der Weijden, F.; Doerfer, C.; Herrera, D.; Shapira, L.; Polak, D.; Madianos, P.; Louropoulou, A.; Machtei, E.; Donos, N.; et al. Primary prevention of periodontitis: Managing gingivitis. J. Clin. Periodontol. 2015, 42, 71–76. [Google Scholar] [CrossRef] [Green Version]
- Roy, R.; Tiwari, M.; Donelli, G.; Tiwari, V. Strategies for combating bacterial biofilms: A focus on anti-biofilm agents and their mechanisms of action. Virulence 2018, 9, 522–554. [Google Scholar] [CrossRef]
- Baruah, K.; Thumpala, V.K.; Khetani, P.; Baruah, Q.; Tiwari, R.V.; Dixit, H. A Review on Toothbrushes and Tooth Brushing Methods. Int. J. Pharm. Sci. Invent. 2017, 6, 29–38. [Google Scholar]
- Yaacob, M.; Worthington, H.V.; Deacon, S.A.; Deery, C.; Walmsley, A.D.; Robinson, P.G.; Glenny, A.M. Powered versus manual toothbrushing for oral health. Cochrane Database Syst. Rev. 2014, 2014, CD002281. [Google Scholar] [CrossRef] [PubMed]
- Mastroberardino, S.; Cagetti, M.G.; Cocco, F.; Campus, G.; Pizzocri, J.; Strohmenger, L. Vertical brushing versus horizontal brushing: A randomized split-mouth clinical trial. Quintessence Int. 2014, 45, 653–661. [Google Scholar] [PubMed]
- De Freitas, G.C.; Pinto, T.M.P.; Grellmann, A.P.; Dutra, D.A.M.; Susin, C.; Kantorski, K.Z.; Moreira, C.H. Effect of self-performed mechanical plaque control frequency on gingival inflammation revisited: A randomized clinical trial. J. Clin. Periodontol. 2016, 43, 354–358. [Google Scholar] [CrossRef]
- Worthington, H.V.; MacDonald, L.; Poklepovic Pericic, T.; Sambunjak, D.; Johnson, T.M.; Imai, P.; Clarkson, J.E. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database Syst. Rev. 2019, 2019, CD012018. [Google Scholar] [CrossRef] [Green Version]
- Bourgeois, D.; Bravo, M.; Llodra, J.C.; Inquimbert, C.; Viennot, S.; Dussart, C.; Carrouel, F. Calibrated interdental brushing for the prevention of periodontal pathogens infection in young adults—A randomized controlled clinical trial. Sci. Rep. 2019, 9, 15127. [Google Scholar] [CrossRef] [Green Version]
- Bourgeois, D.; Saliasi, I.; Llodra, J.C.; Bravo, M.; Viennot, S.; Carrouel, F. Efficacy of interdental calibrated brushes on bleeding reduction in adults: A 3-month randomized controlled clinical trial. Eur. J. Oral. Sci. 2016, 124, 566–571. [Google Scholar] [CrossRef]
- Carrouel, F.; Viennot, S.; Santamaria, J.; Veber, P.; Bourgeois, D. Quantitative Molecular Detection of 19 Major Pathogens in the Interdental Biofilm of Periodontally Healthy Young Adults. Front. Microbiol. 2016, 7, 840. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Eickholz, P.; Loos, B.G.; Papapanou, P.; Van der Velden, U.; Armitage, G.; Bouchard, P.; Deinzer, R.; Dietrich, T.; Hughes, F.; et al. Principles in prevention of periodontal diseases: Consensus report of group 1 of the 11th European Workshop on Periodontology on effective prevention of periodontal and peri-implant diseases. J. Clin. Periodontol. 2015, 42, 5–11. [Google Scholar] [CrossRef]
- Geisinger, M.L.; Ogdon, D.; Kaur, M.; Valiquette, G.; Geurs, N.C.; Reddy, M.S. Toss the Floss? Evidence-Based Oral Hygiene Recommendations for the Periodontal Patient in the Age of ‘Flossgate’. Clin. Adv. Periodontics 2019, 9, 83–90. [Google Scholar] [CrossRef]
- Lundberg, K.; Wegner, N.; Yucel-Lindberg, T.; Venables, P.J. Periodontitis in RA-the citrullinated enolase connection. Nat. Rev. Rheumatol. 2010, 6, 727–730. [Google Scholar] [CrossRef]
- Loe, H.; Theilade, E.; Jensen, S.B. Experimental gingivitis in man. J. Periodontol. 1965, 36, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Monsarrat, P.; Blaizot, A.; Kémoun, P.; Ravaud, P.; Nabet, C.; Sixou, M.; Vergnes, J.N. Clinical research activity in periodontal medicine: A systematic mapping of trial registers. J. Clin. Periodontol. 2016, 43, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Dubar, M.; Delatre, V.; Moutier, C.; Sy, K.; Agossa, K. Awareness and practices of general practitioners towards the oral-systemic disease relationship: A regionwide survey in France. J. Eval. Clin. Pract. 2019. [Google Scholar] [CrossRef] [PubMed]
- Vinel, A.; Vachon, C.; Barthet, P.; Laurencin-Dalacieux, S. Periodontal Diseases and Systemic Disorders: What Do Our Doctors Know? A General Practitioner’s Survey Conducted in Southern France. J. Evid. Based Dent. Pract. 2017, 17, 361–369. [Google Scholar]
- Hajj, A.; Hallit, S.; Azzo, C.; Abdou, F.; Akel, M.; Sacre, H.; Salameh, P.; Rabbaa Khabbaz, L. Assessment of knowledge, attitude and practice among community pharmacists towards dental care: A national cross sectional survey. Saudi Pharm. J. 2019, 27, 475–483. [Google Scholar] [CrossRef]
- Bawazir, O.A. Knowledge and attitudes of pharmacists regarding oral healthcare and oral hygiene products in riyadh, saudi arabia. J. Int. Oral Health 2014, 6, 10–13. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics of Respondents | All Respondents | Self-Reported Gingival Bleeding | ||
|---|---|---|---|---|
| n | % | n | % | |
| All | 794 | 100.0 | 502 | 63.2 |
| Center | ||||
| Preventive medicine | 399 | 50.3 | 283 | 70.9 |
| Mall | 198 | 24.9 | 99 | 50.0 |
| Railway station | 197 | 24.8 | 120 | 60.9 |
| Sex | ||||
| Female | 418 | 52.6 | 278 | 66.5 |
| Male | 376 | 47.4 | 224 | 59.6 |
| Age group (years) | ||||
| 18–40 | 367 | 46.2 | 260 | 70.8 |
| 41–60 | 267 | 33.6 | 169 | 63.3 |
| >60 | 160 | 20.2 | 73 | 45.6 |
| Level of education | ||||
| Low | 280 | 35.3 | 179 | 63.9 |
| Medium | 143 | 18.0 | 93 | 65.0 |
| High | 371 | 46.7 | 230 | 62.0 |
| Profession/occupations | ||||
| Unemployed/student/ other | 233 | 29.3 | 165 | 70.8 |
| worker/salaried/artisan/merchant/official | 301 | 37.9 | 205 | 68.1 |
| executive/teacher/ liberal profession | 119 | 15.0 | 65 | 54.6 |
| Pensioner/retired | 141 | 17.8 | 67 | 47.5 |
| Level of dental anxiety | ||||
| None | 438 | 55.2 | 253 | 57.8 |
| Moderate | 197 | 24.8 | 130 | 66.0 |
| High | 159 | 20.0 | 119 | 74.8 |
| Characteristics of Respondents | Mouthwash | Soft-Bristle Toothbrush | Brushing Technique Modification | Dental Appointment | Stop Brushing | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | p | n | % | p | n | % | p | n | % | p | n | % | p | |
| All | 147 | 29.3 | 101 | 20.1 | 97 | 19.3 | 80 | 15.9 | 21 | 4.2 | |||||
| Sex | 1.0 | 0.1 | 0.2 | 0.3 | 0.007 | ||||||||||
| Male (n = 120) | 57 | 47.5 | 33 | 27.5 | 33 | 27.5 | 35 | 29.2 | 14 | 11.7 | |||||
| Female (n = 189) | 90 | 47.6 | 68 | 36 | 64 | 33.9 | 45 | 23.8 | 7 | 3.7 | |||||
| Age group (years) | 0.03 | 0.6 | 0.6 | 0.04 | 0.1 | ||||||||||
| 18–40 (n = 158) | 66 | 41.8 | 51 | 32.3 | 53 | 33.5 | 33 | 20.9 | 14 | 8.9 | |||||
| 41–60 (n = 107) | 53 | 49.5 | 33 | 30.8 | 33 | 30.8 | 37 | 34.6 | 3 | 2.8 | |||||
| >60 (n = 44) | 28 | 63.6 | 17 | 38.6 | 11 | 25.0 | 10 | 22.7 | 4 | 9.1 | |||||
| Level of education | 0.3 | 0.3 | 0.6 | 0.5 | 0.3 | ||||||||||
| Low (n = 115) | 60 | 52.2 | 36 | 31.3 | 32 | 27.8 | 26 | 22.6 | 11 | 9.6 | |||||
| Middle (n = 55) | 28 | 50.9 | 14 | 25.5 | 18 | 32.7 | 14 | 25.5 | 2 | 3.6 | |||||
| High (n = 139) | 59 | 42.4 | 51 | 36.7 | 42 | 33.8 | 40 | 28.8 | 8 | 5.8 | |||||
| Profession/occupations | 0.5 | 0.6 | 0.04 | 0.4 | 0.6 | ||||||||||
| Unemployed/student/ other (n = 95) | 45 | 47.4 | 27 | 28.4 | 40 | 42.1 | 21 | 22.1 | 6 | 6.3 | |||||
| Worker/salaried/ artisan/merchant/ official (n = 134) | 65 | 48.5 | 44 | 32.8 | 33 | 24.6 | 33 | 24.6 | 12 | 9.0 | |||||
| Executive/teacher/liberal profession (n = 42) | 16 | 38.1 | 17 | 40.5 | 12 | 28.6 | 15 | 35.7 | 1 | 2.4 | |||||
| Pensioner/retired (n = 38) | 21 | 55.3 | 13 | 34.2 | 12 | 31.6 | 11 | 28.9 | 2 | 5.3 | |||||
| Level of anxiety | 0.2 | 0.7 | 0.07 | 0.7 | 0.002 | ||||||||||
| None (n = 142) | 75 | 52.8 | 46 | 32.4 | 42 | 29.6 | 40 | 28.2 | 7 | 4.9 | |||||
| Moderate (n = 89) | 37 | 41.6 | 32 | 36 | 26 | 40.4 | 21 | 23.6 | 2 | 2.2 | |||||
| High/severe (n = 78) | 35 | 44.9 | 23 | 29.5 | 19 | 24.4 | 19 | 24.4 | 12 | 15.4 | |||||
| Reactions/Responses of Healthcare Professionals | Physician | Dentist | Pharmacist | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| This bleeding is not serious | 34 | 47.9 | 59 | 27.3 | 13 | 32.5 |
| It is a common and normal phenomenon | 4 | 5.6 | 6 | 2.8 | 1 | 2.5 |
| Prescription of appropriate mouthwash or toothpaste | 20 | 28.2 | 119 | 55.1 | 18 | 45.0 |
| Change for a soft-bristle toothbrush | 15 | 21.1 | 79 | 36.6 | 12 | 30.0 |
| Tooth brushing education | 11 | 15.5 | 83 | 38.4 | 0 | 0.0 |
| You should see a dentist | 19 | 26.8 | NA | NA | 10 | 25.0 |
| Gingival examination | NA | NA | 88 | 40.7 | NA | NA |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baudet, A.; Veynachter, T.; Rousseau, H.; Anagnostou, F.; Jeanne, S.; Orti, V.; Thilly, N.; Clément, C.; Bisson, C. Perception of Gingival Bleeding by People and Healthcare Professionals: A Multicentre Study in an Adult French Population. Int. J. Environ. Res. Public Health 2020, 17, 5982. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165982
Baudet A, Veynachter T, Rousseau H, Anagnostou F, Jeanne S, Orti V, Thilly N, Clément C, Bisson C. Perception of Gingival Bleeding by People and Healthcare Professionals: A Multicentre Study in an Adult French Population. International Journal of Environmental Research and Public Health. 2020; 17(16):5982. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165982
Chicago/Turabian StyleBaudet, Alexandre, Thomas Veynachter, Hélène Rousseau, Fani Anagnostou, Sylvie Jeanne, Valérie Orti, Nathalie Thilly, Céline Clément, and Catherine Bisson. 2020. "Perception of Gingival Bleeding by People and Healthcare Professionals: A Multicentre Study in an Adult French Population" International Journal of Environmental Research and Public Health 17, no. 16: 5982. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165982