Association between Satisfaction with Life and Personality Types A and D in Young Women with Acne Vulgaris



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Acne Vulgaris
2.2.2. Satisfaction with Life
2.2.3. Type A Behavior Pattern
2.2.4. Type D Personality
2.3. Procedure
2.4. Statistical Analysis
3. Results
3.1. Differences in Satisfaction with Life andPersonality Types A and D Between the WAV and AV Groups
3.2. Association Between Satisfaction with Life and Personality Types A and D in Women with Acne
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bhate, K.; Williams, H.C. Epidemiology of acne vulgaris. Br. J. Dermatol. 2013, 168, 474–485. [Google Scholar] [CrossRef] [PubMed]
- Chilicka, K.; Maj, J.; Panaszek, B. General quality of life of patients with acne vulgaris before and after performing selected cosmetological treatments. Patient Prefer. Adherence 2017, 11, 1357–1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chilicka, K.; Rogowska, A.M.; Szyguła, R.; Taradaj, J. Examining Quality of Life after Treatment with Azelaic and Pyruvic Acid Peels in Women with Acne Vulgaris. Clin. Cosmet. Investig. Dermatol. 2020, 13, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Oon, H.H.; Wong, S.-N.; Aw, D.C.W.; Cheong, W.K.; Goh, C.L.; Tan, H.H. Acne management guidelines by the dermatological society of Singapore. J. Clin. Aesthet. Dermatol. 2019, 12, 34–50. [Google Scholar]
- Zhang, J.; Shen, Y.; Wang, T.; Zhou, C.; Wang, X.; Ding, X.; Tian, S.; Liu, Y.; Peng, G.; Xue, S.; et al. Prevalence of acne vulgaris in Chinese adolescents and adults: A community-based study of 17,345 subjects in six cities. Acta Derm. Venereol. 2012, 92, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Babar, O.; Mobeen, A. Prevalence and psychological impact of acne vulgaris in female undergraduate medical students of Rawalpindi and Islamabad, Pakistan. Cureus 2019, 11, e5722. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.E.; Irwin, B.; Mauriello, D.; Liang, L.; Pappert, A.; Kimball, A.B. Self-reported acne severity, treatment, and belief patterns across multiple racial and ethnic groups in adolescent students. Pediatr. Dermatol. 2010, 27, 446–452. [Google Scholar] [CrossRef]
- Szepietowski, J.; Kapińska-Mrowiecka, M.; Kaszuba, A.; Lagner, A.; Placek, W.; Wolska, H.; Matusiak, L. Acne vulgaris: Pathogenesis and treatment. Consensus of the polish dermatological society. Dermatol. Rev. 2012, 6, 649–673. [Google Scholar]
- Fabbrocini, G.; Cacciapuoti, S.; Monfrecola, G.A. Qualitative investigation of the impact of acne on health-related quality of life (HRQL): Development of a conceptual model. Dermatol. Ther. 2018, 8, 85–99. [Google Scholar] [CrossRef] [Green Version]
- Altunay, I.K.; Özkur, E.; Dalgard, F.J.; Gieler, U.; Aragones, L.T.; Lien, L.; Poot, F.; Jemec, G.B.; Misery, L.; Szabó, C.; et al. Psychosocial Aspects of Adult Acne: Data from 13 European Countries. Acta Derm. Venereol. 2020, 100, adv00051. [Google Scholar] [CrossRef] [Green Version]
- Dréno, B. Assessing quality of life in patients with acne vulgaris: Implications for treatment. Am. J. Clin. Dermatol. 2006, 7, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.K. Psychosocial impact of acne vulgaris: Evaluating the evidence. Skin Ther. Letter. 2004, 9, 1–9. [Google Scholar]
- Alanazi, M.S.; Hammad, S.M.; Mohamed, A.E. Prevalence and psychological impact of Acne vulgaris among female secondary school students in Arar city, Saudi Arabia, in 2018. Electron. Physician 2018, 10, 7224–7229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cengiz, G.F.; Gürel, G. Difficulties in emotion regulation and quality of life in patients with acne. Qual. Life Res. 2020, 29, 431–438. [Google Scholar] [CrossRef]
- Gallitano, S.M.; Berson, D.S. How Acne Bumps Cause the Blues: The Influence of Acne Vulgaris on Self-Esteem. Int. J. Womens Dermatol. 2017, 4, 12–17. [Google Scholar] [CrossRef]
- Hosthota, A.; Bondade, S.; Basavaraja, V. Impact of acne vulgaris on quality of life and self-esteem. Cutis 2016, 98, 121–124. [Google Scholar]
- Krejci-Manwaring, J.; Kerchner, K.; Feldman, S.R.; Rapp, D.A.; Rapp, S.R. Social sensitivity and acne: The role of personality in negative social consequences and quality of life. Int. J. Psychiatry Med. 2006, 36, 121–130. [Google Scholar] [CrossRef]
- Samuels, D.V. An Unblemished Look: Understanding the Role of Acne in Internalizing Problems. Ph.D. Thesis, University of California, Riverside, CA, USA, 2018. [Google Scholar]
- Tasoula, E.; Gregoriou, S.; Chalikias, J.; Lazarou, D.; Danopoulou, I.; Katsambas, A.; Rigopoulos, D. The impact of acne vulgaris on quality of life and psychic health in young adolescents in Greece. Results of a population survey. An. Bras. Dermatol. 2012, 87, 862–869. [Google Scholar] [CrossRef]
- Vilar, G.N.; Santos, L.A.; Sobral Filho, J.F. Quality of life, self-esteem and psychosocial factors in adolescents with acne vulgaris. An. Bras. Dermatol. 2015, 90, 622–629. [Google Scholar] [CrossRef]
- Diener, E. Subjective well-being. Psychol. Bull. 1984, 95, 542–575. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Asses 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Diener, E. New findings and future directions for subjective well-being research. Am. Psychol. 2012, 67, 590–597. [Google Scholar] [CrossRef] [PubMed]
- López-Ortega, M.; Torres-Castro, S.; Rosas-Carrasco, O. Psychometric properties of the Satisfaction with Life Scale (SWLS): Secondary analysis of the Mexican Health and Aging Study. Health Qual. Life Outcomes 2016, 14, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beutel, M.E.; Glaesmer, H.; Wiltink, J.; Marian, H.; Brähler, E. Life satisfaction, anxiety, depression and resilience across the life span of men. Aging Male 2010, 13, 32–39. [Google Scholar] [CrossRef]
- Kong, F.; Ding, K.; Zhao, J. The relationships among gratitude, self-esteem, social support and life satisfaction among undergraduate students. J. Happiness Stud. 2015, 16, 477–489. [Google Scholar] [CrossRef]
- Lee, J.; Kim, E.; Wachholtz, A. The effect of perceived stress on life satisfaction: The mediating effect of self-efficacy. ChongsonyonhakYongu 2016, 23, 29–47. [Google Scholar]
- Martínez-Martí, M.L.; Ruch, W. Character strengths predict resilience over and above positive affect, self-efficacy, optimism, social support, self-esteem, and life satisfaction. J. Posit. Psychol. 2017, 12, 110–119. [Google Scholar] [CrossRef]
- Praharso, N.F.; Tear, M.J.; Cruwys, T. Stressful life transitions and well-being: A comparison of the stress-buffering hypothesis and the social identity model of identity change. Psychiat. Res. 2017, 247, 265–275. [Google Scholar] [CrossRef] [Green Version]
- Gana, K.; Bailly, N.; Saada, Y.; Joulain, M.; Trouillet, R.; Hervé, C.; Alaphilippe, D. Relationship between life satisfaction and physical health in older adults: A longitudinal test of cross-lagged and simultaneous effects. Health Psychol. 2013, 32, 896–904. [Google Scholar] [CrossRef]
- Rogowska, A.M.; Zmaczyńska-Witek, B.; Mazurkiewicz, M.; Kardasz, Z. The mediating effect of self-efficacy on the relationship between health locus of control and life satisfaction: A moderator role of movement disability. Dis. Health J. 2020, 100923. [Google Scholar] [CrossRef]
- Zonash, R.; Chishty, H.; Aymun, S.; Iman, T.; Batool, M. Acne vulgaris: Effect of body image and life satisfaction on rejection sensitivity. Pak. J. Med. Res. 2019, 58, 66–72. [Google Scholar]
- Ferguson, E.; Williams, L.; O’Connor, R.C.; Howard, S.; Hughes, B.M.; Johnston, D.W.; Allan, J.; O’Connor, D.B.; Lewis, C.A.; Grealy, M.A.; et al. A Taxometric Analysis of Type-D Personality. Psychosom. Med. 2009, 71, 981–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilberto, J.M.; Davenport, M.K.; Beier, M.E. Personality, health, wealth, and subjective well-being: Testing an integrative model with retired and working older adults. J. Res. Person. 2020, 87, 103959. [Google Scholar] [CrossRef]
- Huang, I.-C.; Lee, J.L.; Ketheeswaran, P.; Jones, C.M.; Revicki, D.A.; Wu, A.W. Does personality affect health-related quality of life? A systematic review. PLoS ONE 2017, 12, e0173806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenman, R.H. Current and past history of Type A behavior pattern. In Biological and Psychological Factors in Cardiovascular Disease; Schmidt, T.H., Dembroski, T.M., Blumchen, G., Eds.; Springer: New York, NY, USA, 1986; pp. 15–40. [Google Scholar]
- Thomas, S.P. A descriptive profile of Type B personality. Image J. Nurs. Scholar. 1986, 18, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Hisam, A.; Rahman, M.U.; Mashhadi, S.F.; Raza, G. Type A and Type B personality among Undergraduate Medical Students: Need for psychosocial rehabilitation. Pak. J. Med. Sci. 2014, 30, 1304–1307. [Google Scholar]
- Lala, A.; Bobîrnac, G.; Tipa, R. Stress levels, Alexithymia, Type A and Type C personality patterns in undergraduate students. J. Med. Life 2010, 3, 200–205. [Google Scholar]
- Lohse, T.; Rohrmann, S.; Richard, A.; Bopp, M.; Faeh, D. Swiss National Cohort Study Group. Type A personality and mortality: Competitiveness but not speed is associated with increased risk. Atherosclerosis 2017, 262, 19–24. [Google Scholar] [CrossRef]
- Allan, R. John Hunter: Early Association of Type A Behavior With Cardiac Mortality. Am. J. Cardiol. 2014, 114, 148–150. [Google Scholar] [CrossRef]
- Brantley, P.J.; Ames, S.C. Psychobiology of Health and Disease. In Comprehensive Handbook of Psychopathology, 3rd ed.; Sutker, P.B., Adams, H.E., Eds.; Kluwer Academic Plenum Publishers: New York, NY, USA, 2001; pp. 777–795. [Google Scholar]
- Miličić, D.; Brajković, L.; Maček, J.L.; Andrić, A.; Ardalić, Ž.; Buratović, T.; Marčinko, D. Type a Personality, Stress, Anxiety and Health Locus of Control in Patients with Acute Myocardial Infarction. Psychiatr. Danubina. 2016, 28, 409–414. [Google Scholar]
- Begley, T.M.; Lee, C.; Czajka, J.M. The relationships of Type A behavior and optimism with job performance and blood pressure. J. Bus. Psychol. 2000, 15, 215–227. [Google Scholar] [CrossRef]
- Al-Asadi, J.N. Type A behaviour pattern: Is it a risk factor for hypertension? EMHJ 2010, 16, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Folsom, A.R.; for the Multiple Risk Factor Intervention Trial Group; Hughes, J.R.; Buehler, J.F.; Mittelmark, M.B.; Jacobs, D.R.; Grimm, R.H. Do Type A men drink more frequently than Type B Men? Findings in the multiple risk factor intervention trial (MRFIT). J. Behav. Med. 1985, 8, 227–235. [Google Scholar] [CrossRef]
- Johnson, C.C.; Hunter, S.; Amos, C.I.; Elder, S.T.; Berenson, G.S. Cigarette smoking, alcohol, and oral contraceptive use by Type A adolescent-The Bogalusa heart study. J. Behav. Med. 1989, 12, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Rogowska, A. Association between Type A/B Behavior Pattern and Alcohol Consumption in Undergraduate Students. Proc. Soc. Behav. Sci. 2014, 159, 682–685. [Google Scholar] [CrossRef] [Green Version]
- Zeichner, A.; Edwards, P.W.; Cohe, E. Acute effects of alcohol on cardiovascular reactivity to stress in college-age Type A (coronary prone) individuals. J. Psychopathol. Behav. Assess. 1985, 7, 75–89. [Google Scholar] [CrossRef]
- Matteson, M.T.; Ivancevich, J.M. Type A and B behavior patterns and self- reported health symptoms and stress: Examining individual and organizational fit. J. Occup. Med. 1982, 24, 585–589. [Google Scholar] [CrossRef]
- Houston, B.K.; Smith, T.W.; Zurawski, R.M. Principal dimensions of the Framingham Type A scale: Differential relationships to cardiovascular reactivity and anxiety. J. Hum. Stress. 1986, 12, 105–112. [Google Scholar]
- Smith, T.W.; Housto, B.K.; Zurawski, R.M. The Framingham Type A Scale and anxiety, irrational beliefs, and self-control. J. Hum. Stress. 1983, 9, 32–37. [Google Scholar] [CrossRef]
- Smith, T.W.; Houston, B.K.; Zurawski, R.M. The framingham Type A Scale: Cardiovascular and cognitive-behavioral responses to interpersonal challenge. Motiv. Emot. 1985, 9, 123–134. [Google Scholar] [CrossRef]
- Smith, T.W.; O’Keeffe, J.L.; Allred, K.D. Neuroticism, symptom reports, and type A behavior: Interpretive cautions for the Framingham Scale. J. Behav. Med. 1989, 12, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Denollet, J. Type D personality. A potential risk factor refined. J. Psychosom. Res. 2000, 49, 255–266. [Google Scholar] [CrossRef] [Green Version]
- Denollet, J. DS14: Standard assessment of negative affectivity, social inhibition, and Type D personality. Psychosom. Med. 2005, 67, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Grande, G.; Romppel, M.; Glaesmer, H.; Petrowski, K.; Herrmann-Lingen, C. The type-D scale (DS14)—Norms and prevalence of type-D personality in a population-based representative sample in Germany. Pers. Individ. Differ. 2010, 48, 935–939. [Google Scholar] [CrossRef]
- Pedersen, S.S.; Denollet, J. Type D personality, cardiac events, and impaired quality of life: A review. Eur. J. Cardiovasc. Prev. Rehabil. 2003, 10, 241–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sher, L. Type D personality: The heart, stress, and cortisol. QJM 2005, 98, 323–329. [Google Scholar] [CrossRef] [Green Version]
- Van Dooren, F.E.P.; Verhey, F.R.J.; Pouwer, F.; Schalkwijk, C.G.; Sep, S.J.S.; Stehouwer, C.D.; Henry, R.; Dagnelie, P.C.; Schaper, N.C.; Van Der Kallen, C.J.; et al. Association of Type D personality with increased vulnerability to depression: Is there a role for inflammation or endothelial dysfunction?—The Maastricht Study. J. Affect. Disord. 2016, 189, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Garİp, Y.; GÜler, T.; Bozkurt Tuncer, Ö.; Önen, S. Type D Personality is Associated with Disease Severity and Poor Quality of Life in Turkish Patients with Fibromyalgia Syndrome: A Cross-Sectional Study. Arch. Rheumatol. 2019, 35, 13–19. [Google Scholar] [CrossRef]
- Kupper, N.; Denollet, J. Type D Personality as a risk factor in coronary heart disease: A review of current evidence. Curr. Cardiol. Rep. 2018, 20, 104. [Google Scholar] [CrossRef] [Green Version]
- Mols, F.; Thong, M.S.Y.; Van De Poll-Franse, L.V.; Roukema, J.A.; Denollet, J. Type D (distressed) personality is associated with poor quality of life and mental health among 3080 cancer survivors. J. Affect. Disord. 2012, 136, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Allen, S.F.; Wetherell, M.A.; Smith, M.A. A one-year prospective investigation of Type D personality and self-reported physical health. Psychol. Health 2019, 34, 773–795. [Google Scholar] [CrossRef] [PubMed]
- De Vroege, L.; De Heer, E.W.; Van Der Thiel, E.; Broek, K.C.V.D.; Sluijs, J.F.V.E.V.D.; Van Der Feltz-Cornelis, C.M. Type D Personality, Concomitant Depressive and Anxiety Disorders, and Treatment Outcomes in Somatic Symptom and Related Disorders: An Observational Longitudinal Cohort Study. Front. Psychiatry 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Kasai, Y.; Suzuki, E.; Iwase, T.; Doi, H.; Takao, S. Type D personality is associated with psychological distress and poor self-rated health among the elderly: A population-based study in Japan. PLoS ONE 2013, 8, e77918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mols, F.; Denollet, J. Type D personality among noncardiovascular patient populations: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Mols, F.; Denollet, J. Type D personality in the general population: A systematic review of health status, mechanisms of disease, and work-related problems. Health Qual. Life Outcomes 2010, 8, 9. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.A.; Riccalton, V.C.; Kelly-Hughes, D.H.; Craw, O.A.; Allen, S.F.; O’Connor, D.B.; Wetherell, M.A. The relationship between Type D personality and physical health complaints is mediated by perceived stress and anxiety but not diurnal cortisol secretion. Stress 2018, 21, 229–236. [Google Scholar] [CrossRef]
- Horwood, S.; Anglim, J.; Tooley, G. Statistically modelling the relationships between Type D personality and social support, health behaviors and symptom severity in chronic illness groups. Psychol. Health 2016, 31, 1047–1063. [Google Scholar] [CrossRef] [Green Version]
- Klaassen, K.; Nyklíček, I.; Traa, S.; De Nijs, R. Distressed personality is associated with lower psychological well-being and life satisfaction, but not disability or disease activity in rheumatoid arthritis patients. Clin. Rheumatol. 2012, 31, 661–667. [Google Scholar] [CrossRef] [Green Version]
- Bartels, H.; Pedersen, S.S.; Van Der Laan, B.F.A.M.; Staal, M.J.; Albers, F.W.J.; Middel, B. The impact of Type D personality on health-related quality of life in tinnitus patients is mainly mediated by anxiety and depression. Otol. Neurotol. 2010, 31, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Akram, U.; Mccarty, K.; Akram, A.; Gardani, M.; Tan, A.; Villarreal, D.; Bilsborough, E.; Dooher, G.; Gibbs, G.; Hudson, J.L.; et al. The relationship between Type D personality and insomnia. Sleep Health 2018, 4, 360–363. [Google Scholar] [CrossRef] [Green Version]
- Aguayo-Carreras, P.; Ruiz-Carrascosa, J.C.; Molina-Leyva, A. Type D personality is associated with poor quality of life, social performance, and psychological impairment in patients with moderate to severe psoriasis: A cross-sectional study of 130 patients. Indian J. Dermatol. Venereol. Leprol. 2020, 86, 375–381. [Google Scholar]
- Basińska, M.A.; Woźniewicz, A. The relation between type D personality and the clinical condition of patients suffering from psoriasis. Postep. Derm. Alergol. 2013, 30, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina-Leyva, A.; Caparros-Delmoral, I.; Ruiz-Carrascosa, J.; Naranjo-Sintes, R.; Jiménez-Moleón, J.J. Elevated prevalence of Type D (distressed) personality in moderate to severe psoriasis is associated with mood status and quality of life impairment: A comparative pilot study. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1710–1717. [Google Scholar] [CrossRef] [PubMed]
- Tekin, A.; Atiş, G.; Yaşar, Ş.; Goktay, F.; Aytekin, S. The relationship of Type D personality and quality of life in patients with psoriasis: A cross-sectional study in Turkish population. Acta Med. Mediter. 2018, 34, 1009. [Google Scholar] [CrossRef]
- Kupper, N.; Denollet, J. Type D personality as a prognostic factor in heart disease: Assessment and mediating mechanisms. J. Pers. Assess. 2007, 89, 265–276. [Google Scholar] [CrossRef]
- Kupper, N.; Pedersen, S.S.; Höfer, S.; Saner, H.; Oldridge, N.; Denollet, J. Cross-cultural analysis of type D (distressed) personality in 6222 patients with ischemic heart disease: A study from the International HeartQoL Project. Int. J. Cardiol. 2013, 166, 327–333. [Google Scholar] [CrossRef]
- Sogaro, E.; Schinina, F.; Burgisser, C.; Orso, F.; Pallante, R.; Aloi, T.; Vanni, D.; Pazzagli, A.; Fattirolli, F. Type D personality impairs quality of life, coping and short-term psychological outcome in patients attending an outpatient intensive program of cardiac rehabilitation. Monaldi Arch. Chest. Dis. 2010, 74, 181–191. [Google Scholar] [CrossRef] [Green Version]
- Annagür, B.B.; Demir, K.; Avci, A.; Uygur, Ö.F. Impact of a Type D Personality on Clinical and Psychometric Properties in a Sample of Turkish Patients with a First Myocardial Infarction. J. Psychiat. Pract. 2017, 23, 3–10. [Google Scholar] [CrossRef]
- Denollet, J. Personality and coronary heart disease: The type-D scale-16 (DS16). An. Behav. Med. 1998, 20, 209–215. [Google Scholar] [CrossRef]
- Kupper, N.; Denollet, J. Type D personality is associated with social anxiety in the general population. Int. J. Behav. Med. 2014, 21, 496–505. [Google Scholar] [CrossRef]
- Svansdottir, E.; Broek, K.C.V.D.; Karlsson, H.D.; Olason, D.T.; Thorgilsson, H.; Denollet, J. The distressed (Type D) and Five-Factor Models of personality in young, healthy adults and their association with emotional inhibition and distress. Pers. Individ. Differ. 2013, 55, 123–128. [Google Scholar] [CrossRef]
- Sereflican, B.; Tuman, T.C.; Tuman, B.A.; Parlak, A.H. Type D personality, anxiety sensitivity, social anxiety, and disability in patients with acne: A cross-sectional controlled study. Adv. Dermatol. Allergol. 2019, 36, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Dehghani, F. Type D personality and life satisfaction: The mediating role of social support. Pers. Individ. Differ. 2018, 134, 75–80. [Google Scholar] [CrossRef]
- Kowalewska, B.; Cybulski, M.; Jankowiak, B.; Krajewska-Kułak, E. Acceptance of Illness, Satisfaction with Life, Sense of Stigmatization, and Quality of Life among People with Psoriasis: A Cross-Sectional Study. Dermatol. Ther. 2020, 10, 413–430. [Google Scholar] [CrossRef] [Green Version]
- Kozaka, J.; Kobus, P. Relationship between type D personality, satisfaction with life and coping with cancer. Psychoonkologia 2015, 2, 74–79. [Google Scholar]
- Ferguson, E. Personality is of central concern to understand health: Towards a theoretical model for health psychology. Health Psychol. Rev. 2013, 7, S32–S70. [Google Scholar] [CrossRef] [Green Version]
- Rout, U.R.; Rout, J.K. Stress Management: Individual Strategies; Springer: Boston, MA, USA, 2002. [Google Scholar]
- Maruyama, S.; Morimoto, K. The Effects of Lifestyle and Type A Behavior on the Life-Stress Process. Environ. Health Prevent. Med. 1997, 2, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Lodder, P. Modeling synergy: How to assess a Type D personality effect. J. Psychosom. Res. 2020, 132, 109990. [Google Scholar] [CrossRef]
- Chilicka, K.; Rogowska, A.M.; Szyguła, R.; Dzieńdziora-Urbińska, I.; Taradaj, J. A comparison of the effectiveness of azelaic and pyruvic acid peels in the treatment of female adult acne: A randomized controlled trial. Sci. Rep. 2020, 10, 12612. [Google Scholar] [CrossRef]
- Juczyński, Z. Measurement Tools in Health Promotion and Psychology; PTP: Warsaw, Poland, 2001. [Google Scholar]
- Pavot, W.; Diener, E. Review of the Satisfaction With Life Scale. Psychol. Assess. 1993, 5, 164–172. [Google Scholar] [CrossRef]
- Haynes, S.G.; Levine, S.; Scotch, N.; Feinleib, M.; Kannel, W.B. The relationship of psychosocial factors to coronary heart disease in the framingham study. Am. J. Epidemiol. 1978, 107, 362–383. [Google Scholar] [CrossRef] [PubMed]
- Ogińska-Bulik, N.; Juczyński, Z. Type D personality in Poland: Validity and application of the Polish DS14. Polish Psychol. Bull. 2009, 40, 130–136. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Hayes, A.F. PROCESS (Version 3.3.), Macro for Windows and SPSS. 2019. Available online: http://www.processmacro.org/download.html (accessed on 23 September 2019).
- Preacher, K.J.; Rucker, D.D.; Hayes, A.F. Assessing moderated mediation hypotheses: Theory, methods, and prescriptions. Multivar. Behav. Res. 2007, 42, 185–227. [Google Scholar] [CrossRef] [PubMed]
- George, D.; Mallery, P. IBM SPSS Statistics 26 Step by Step: A Simple Guide and Reference, 16th ed.; Taylor & Francis: New York, NY, USA, 2019. [Google Scholar]
- Denollet, J.; Pedersen, S.S.; Ong, A.T.; Erdman, R.A.M.; Serruys, P.W.; Van Domburg, R.T. Social inhibition modulates the effect of negative emotions on cardiac prognosis following percutaneous coronary intervention in the drug-eluting stent era†. Eur. Hear. J. 2005, 27, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Wan, S. The Cause and Treatment of Acne Vulgaris: Fact Versus Fiction. Master’s Thesis, School of Medicine, Boston University, Boston, MA, USA, 2015. [Google Scholar]
- Vitaliano, P.P.; Maiuro, R.D.; Russo, J.; Mitchell, E.S.; Carr, J.E.; Van Citters, R.L. A biopsychosocial model of medical student distress. J. Behav. Med. 1988, 11, 311–331. [Google Scholar] [CrossRef]
- Jandackova, V.K.; Koenig, J.; Jarczok, M.N.; Fischer, J.E.; Thayer, J.F. Potential biological pathways linking Type-D personality and poor health: A cross-sectional investigation. PLoS ONE 2017, 12, e0176014. [Google Scholar] [CrossRef] [Green Version]
- Michal, M.; Wiltink, J.; Grande, G.; Beutel, M.E.; Brähler, E. Type D personality is independently associated with major psychosocial stressors and increased health care utilization in the general population. J. Affect. Disord. 2011, 134, 396–403. [Google Scholar] [CrossRef]
- Bayram, N.; Bilgel, N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 667–672. [Google Scholar] [CrossRef]
- Hintsa, T.; Jokela, M.; Pulkki-Råback, L.; Keltikangasjarvinen, L. Age- and Cohort-Related Variance of Type-A Behavior Over 24 Years: The Young Finns Study. Int. J. Behav. Med. 2013, 21, 927–935. [Google Scholar] [CrossRef]
- Timmermans, I.; Versteeg, H.; Duijndam, S.; Graafmans, C.; Polak, P.; Denollet, J. Social inhibition and emotional distress in patients with coronary artery disease: The Type D personality construct. J. Health Psychol. 2017, 24, 1929–1944. [Google Scholar] [CrossRef]
- Williams, L.; O’Connor, R.C.; Grubb, N.R.; O’Carroll, R.E. Type D personality and three-month psychosocial outcomes among patients post-myocardial infarction. J. Psychosom. Res. 2012, 72, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.A.; Thompson, A.; Hall, L.J.; Allen, S.F.; Wetherell, M.A. The physical and psychological health benefits of positive emotional writing: Investigating the moderating role of Type D (distressed) personality. Br. J. Heal. Psychol. 2018, 23, 857–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Range | M | SD | Median | Skewness | Kurtosis |
|---|---|---|---|---|---|---|
| Satisfaction with life | 5–35 | 19.36 | 6.86 | 18.00 | 0.15 | −0.53 |
| Type A behavior pattern | 0–1 | 0.67 | 0.23 | 0.73 | −0.86 | 0.32 |
| TypeD personality | ||||||
| Negative Affectivity | 0–28 | 14.77 | 6.23 | 16.00 | −0.55 | −0.32 |
| Social inhibition | 0–28 | 11.15 | 5.84 | 11.00 | −0.02 | −0.38 |
| Variable | WAV | AV | t (298) | p | d | ||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| Satisfaction with life | 21.57 | 7.24 | 17.14 | 5.66 | 5.91 | 0.000 | 0.68 |
| Type A personality | 0.57 | 0.26 | 0.77 | 0.14 | −8.27 | 0.000 | 0.96 |
| Type D personality | |||||||
| Negative Affectivity | 11.88 | 6.46 | 17.66 | 4.39 | −9.07 | 0.000 | 1.05 |
| Social inhibition | 8.51 | 5.64 | 13.79 | 4.75 | −8.77 | 0.000 | 1.01 |
| Variable | WAV | AV | χ2(1) | p | ϕ | ||
|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||
| Life satisfaction | 43.88 | 0.000 | −0.38 | ||||
| No (SWLS < 20) | 55 | 18.33 | 112 | 37.33 | |||
| Yes (SWLS ≥ 20) | 95 | 31.67 | 38 | 12.67 | |||
| Type A behavior pattern | 19.89 | 0.000 | 0.26 | ||||
| No (FTAS < 0.79) | 115 | 38.33 | 78 | 26.00 | |||
| Yes (FTAS ≥ 80) | 35 | 11.67 | 72 | 24.00 | |||
| Type D personality | 76.22 | 0.000 | 0.50 | ||||
| No (NA ≤ 10; SI ≤ 10) | 103 | 34.33 | 28 | 9.33 | |||
| Yes (NA ≥ 10; SI ≥ 10) | 47 | 15.67 | 122 | 40.67 | |||
| Variable | Samples | ||
|---|---|---|---|
| Total | WAV | AV | |
| Type A behavior pattern | −0.06 | 0.14 | −0.01 |
| Type D personality | |||
| Negative affectivity | −0.37 *** | −0.23 ** | −0.31 *** |
| Social inhibition | −0.38 *** | −0.19 * | −0.41 *** |
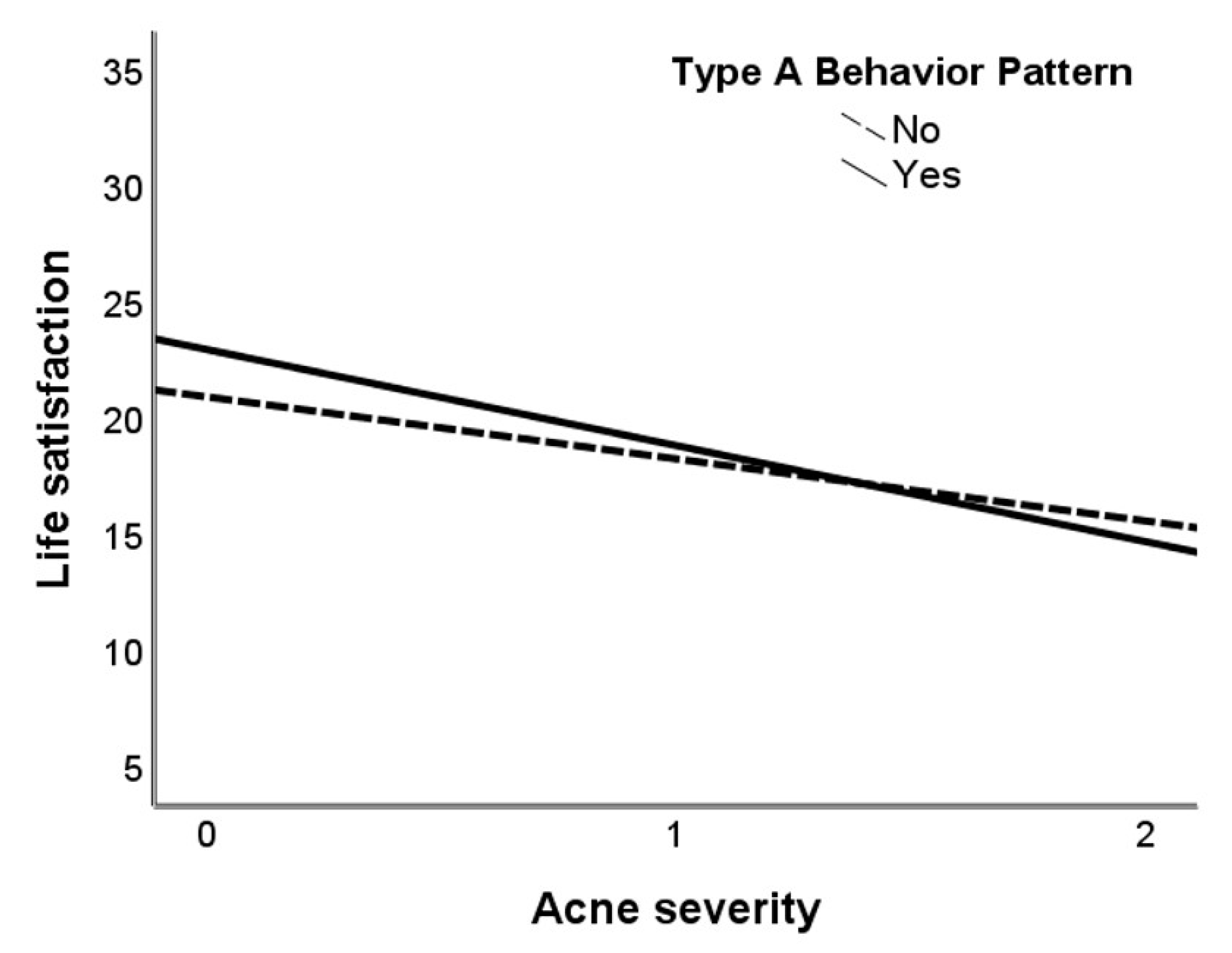
| Variable | Bootstrap 95% CI | |||||||
|---|---|---|---|---|---|---|---|---|
| b | SE | t | p | M | SE | LL | UL | |
| Constant | 21.26 | 0.60 | 35.59 | 0.000 | 21.26 | 0.68 | 19.90 | 22.59 |
| Acne severity (AS) | ||||||||
| First-degree on the HVS (AS 1) | −4.50 | 1.08 | −4.17 | 0.000 | −4.49 | 0.94 | −6.31 | −2.63 |
| Second degree on the HVS (AS 2) | −4.26 | 1.37 | −3.11 | 0.002 | −4.26 | 1.32 | −6.79 | −1.60 |
| Type A behavior pattern (TABP) | 1.34 | 1.24 | 1.08 | 0.280 | 1.34 | 1.43 | −1.58 | 4.04 |
| Interaction term AS × TABP | ||||||||
| Int 1 AS 1 × TABP | 1.30 | 1.80 | 0.72 | 0.472 | 1.29 | 1.82 | −2.18 | 4.95 |
| Int 2 AS 2 × TABP | −4.12 | 2.14 | −1.93 | 0.055 | −4.11 | 2.03 | −8.12 | −0.05 |
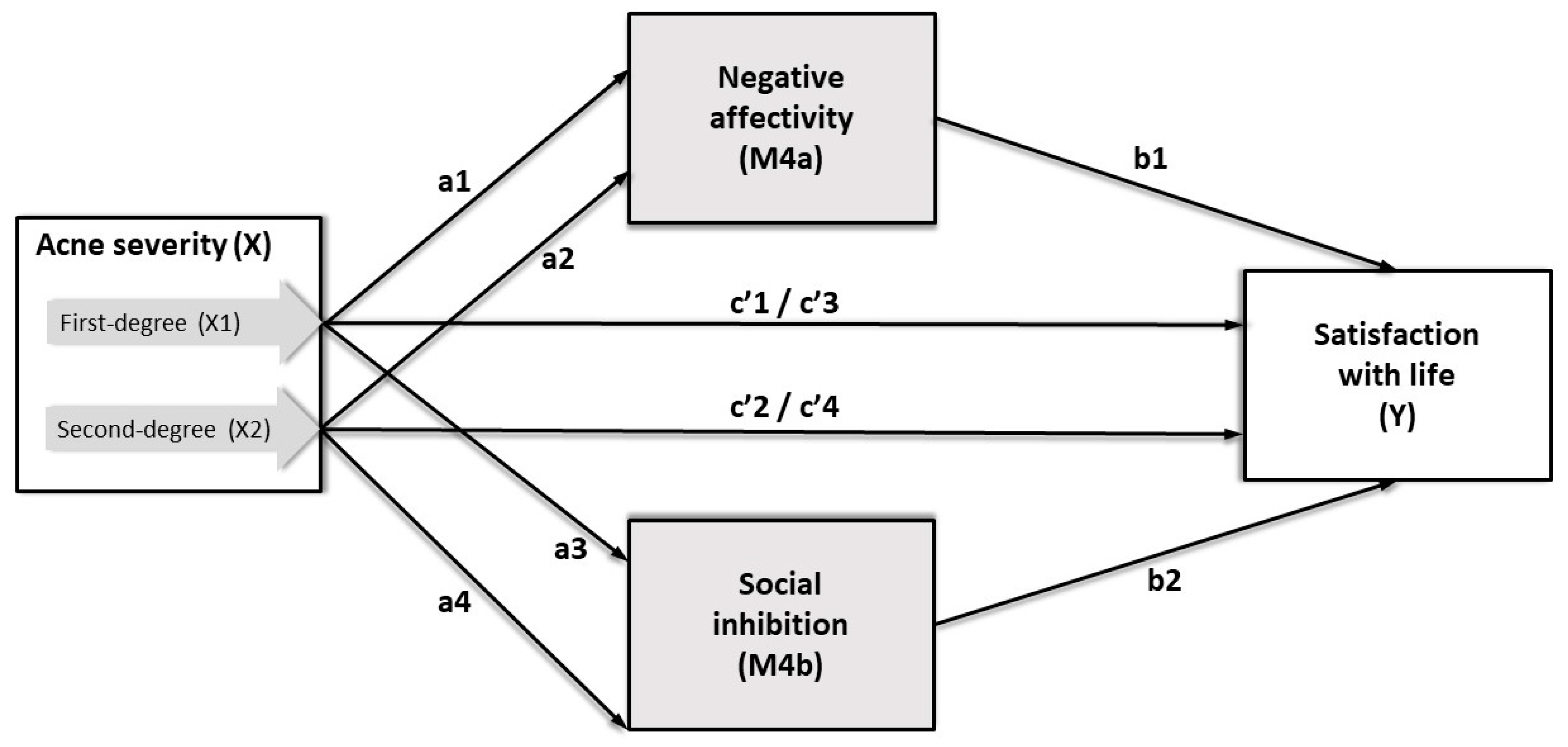
| Antecedent Study Model 4a (M4a) | Consequent | |||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | M4a (Negative Affectivity) | Estimate | Y (Satisfaction with Life) | |||||
| Coefficient | SE | p | Coefficient | SE | p | |||
| X1 (first-degree AV) | a1 | 5.41 | 0.72 | 0.000 | c’1 | −1.98 | 0.89 | 0.027 |
| X2 (second-degree AV) | a2 | 6.44 | 0.88 | 0.000 | c’2 | −4.07 | 1.08 | 0.000 |
| M4a (negative affectivity) | - | - | - | b1 | −0.29 | 0.07 | 0.000 | |
| Constant | iM1 | 11.88 | 0.45 | 0.000 | iY | 25.06 | 0.93 | 0.000 |
| R2 = 0.22 | R2 = 0.18 | |||||||
| F(2, 297) = 41.71 p < 0.001 | F(3, 296) = 20.86 p < 0.001 | |||||||
| Study Model 4b (M4b) | M4b (Social Inhibition) | Y (Satisfaction with Life) | ||||||
| Coefficient | SE | p | Coefficient | SE | p | |||
| X1 (first-degree AV) | a3 | 4.74 | 0.68 | 0.000 | c’3 | −1.97 | 0.88 | 0.025 |
| X2 (second-degree AV) | a4 | 6.23 | 0.83 | 0.000 | c’4 | −3.86 | 1.08 | 0.000 |
| M4b (social inhibition) | - | - | - | b2 | −0.34 | 0.07 | 0.000 | |
| Constant | iM2 | 8.51 | 0.42 | 0.000 | iY | 24.45 | 0.78 | 0.000 |
| R2 = 0.21 | R2 = 0.18 | |||||||
| F(2, 297) = 40.13 p < 0.001 | F(3, 296) = 22.26 p < 0.001 | |||||||
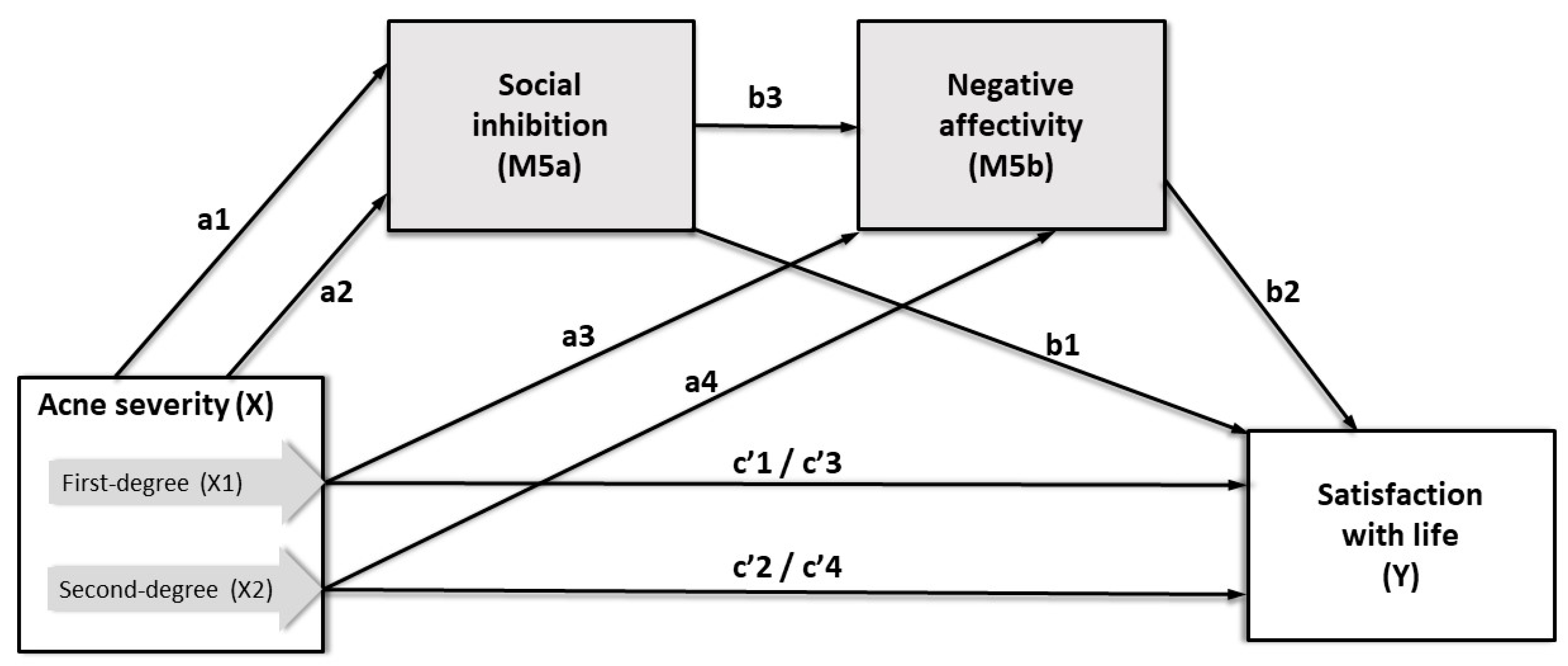
| Antecedent Study Model 5a (M5a) | Consequent | |||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | M5a (Social Inhibition) | Estimate | Y (Satisfaction with Life) | |||||
| Coefficient | SE | p | Coefficient | SE | p | |||
| X1 (first-degree AV) | a1 | 4.74 | 0.68 | 0.000 | c’1 | −3.57 | 0.84 | 0.000 |
| X2 (second-degree AV) | a2 | 6.23 | 0.83 | 0.000 | c’2 | −5.96 | 1.03 | 0.000 |
| M5a (social inhibition) | - | - | - | - | b1 | −0.24 | 0.08 | 0.002 |
| Constant | iM1 | 8.51 | 0.42 | 0.000 | iY | 21.57 | 0.53 | 0.000 |
| R2 = 0.21 | R2 = 0.12 | |||||||
| F(2, 297) = 40.13 p < 0.001 | F(2, 297) = 20.04 p < 0.001 | |||||||
| Study Model 5b (M5b) | M5b (Negative Affectivity) | Y (Satisfaction with Life) | ||||||
| Coefficient | SE | p | Coefficient | SE | p | |||
| X1 (first-degree AV) | a3 | 3.11 | 0.69 | 0.000 | c’3 | −1.38 | 0.90 | 0.120 |
| X2 (second-degree AV) | a4 | 3.40 | 0.85 | 0.000 | c’4 | −3.22 | 1.10 | 0.004 |
| M5a (social inhibition) | b3 | 0.49 | 0.06 | 0.000 | - | - | - | - |
| M5b (negative affectivity) | - | - | - | b2 | −0.19 | 0.07 | 0.000 | |
| Constant | iM2 | 7.74 | 0.62 | 0.000 | iY | 25.90 | 0.96 | 0.011 |
| R2 = 0.38 | R2 = 0.20 | |||||||
| F(3, 296) = 61.22 p < 0.001 | F(4, 295) = 18.66 p < 0.001 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chilicka, K.; Rogowska, A.M.; Szyguła, R.; Adamczyk, E. Association between Satisfaction with Life and Personality Types A and D in Young Women with Acne Vulgaris. Int. J. Environ. Res. Public Health 2020, 17, 8524. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228524
Chilicka K, Rogowska AM, Szyguła R, Adamczyk E. Association between Satisfaction with Life and Personality Types A and D in Young Women with Acne Vulgaris. International Journal of Environmental Research and Public Health. 2020; 17(22):8524. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228524
Chicago/Turabian StyleChilicka, Karolina, Aleksandra M. Rogowska, Renata Szyguła, and Ewa Adamczyk. 2020. "Association between Satisfaction with Life and Personality Types A and D in Young Women with Acne Vulgaris" International Journal of Environmental Research and Public Health 17, no. 22: 8524. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228524