The Primary Care-Video Intervention Therapy for Growth-Vulnerable Infants. A Case Study

Abstract
:1. Introduction
1.1. Video-Feedback Interventions
1.2. The Video Intervention Therapy and Primary-Care Video Intervention Therapy
2. Methods
2.1. Case Illustration
2.2. The Primary Care-Video Intervention Therapy
2.3. Analysis of Parental Discourse
3. Results
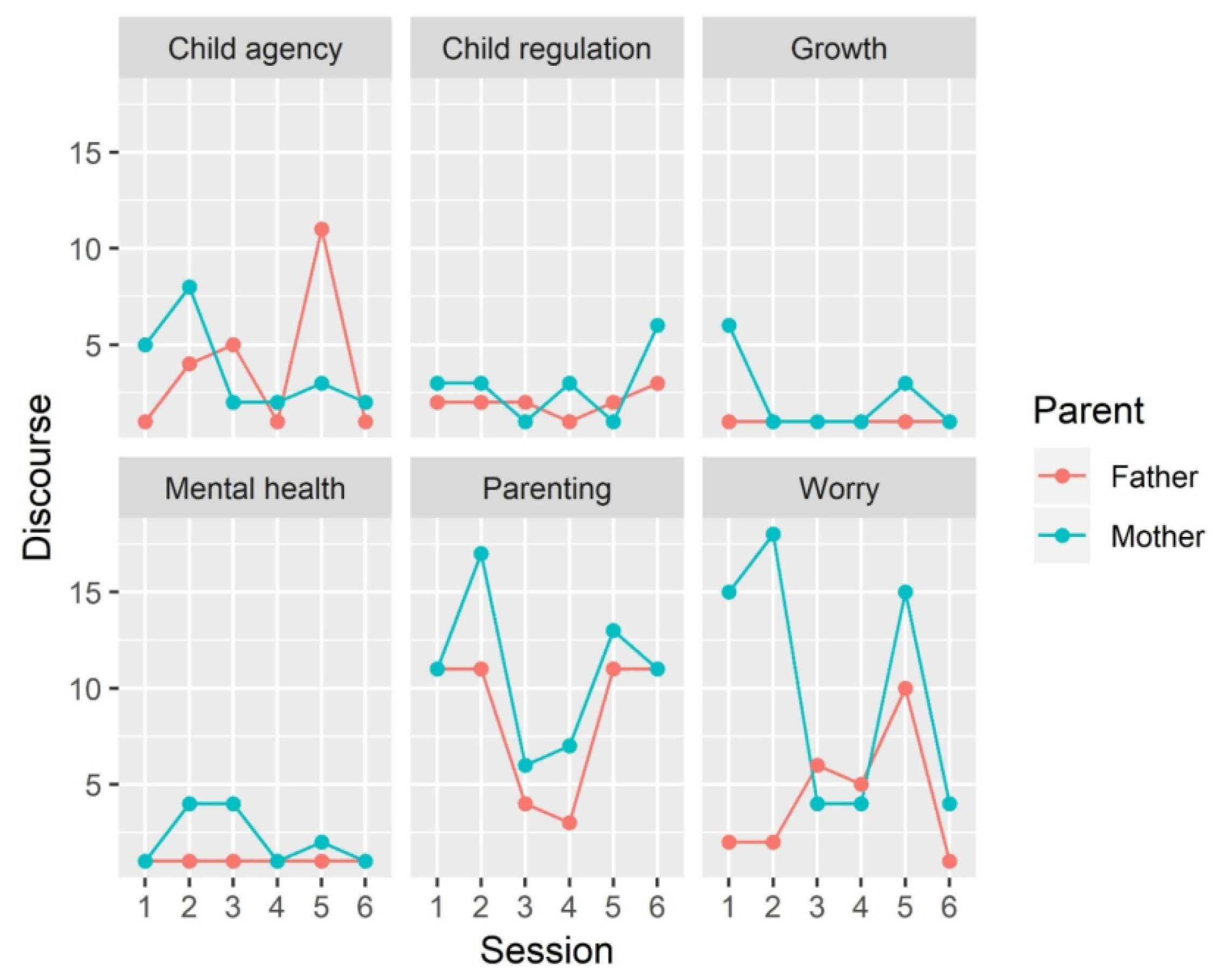
3.1. Development of Parental Discourse
3.2. Clinical Vignette: Eating Together (Third Session)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sacchi, C.; De Carli, P.; Mento, G.; Farroni, T.; Visentin, S.; Simonelli, A. Socio-Emotional and Cognitive Development in Intrauterine Growth Restricted (IUGR) and Typical Development Infants: Early Interactive Patterns and Underlying Neural Correlates. Rationale and Methods of the Study. Front. Behav. Neurosci. 2018, 12, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Westrupp, E.M.; Mensah, F.K.; Giallo, R.; Cooklin, A.; Nicholson, J.M. Mental Health in Low-to-Moderate Risk Preterm, Low Birth Weight, and Small for Gestational Age Children at 4 to 5 Years: The Role of Early Maternal Parenting. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 313–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miles, M.S.; Holditch-Davis, D. Compensatory Parenting: How Mothers Describe Parenting Their 3-Year-Old, Prematurely Born Children. J. Pediatr. Nurs. 1995, 10, 243–253. [Google Scholar] [CrossRef]
- Montirosso, R.; Arrigoni, F.; Casini, E.; Nordio, A.; De Carli, P.; Di Salle, F.; Moriconi, S.; Re, M.; Reni, G.; Borgatti, R. Greater Brain Response to Emotional Expressions of Their Own Children in Mothers of Preterm Infants: An FMRI Study. J. Perinatol. 2017, 37, 716. [Google Scholar] [CrossRef]
- Howe, T.-H.; Sheu, C.-F.; Hsu, Y.-W.; Wang, T.-N.; Wang, L.-W. Predicting Neurodevelopmental Outcomes at Preschool Age for Children with Very Low Birth Weight. Res. Dev. Disabil. 2016, 48, 231–241. [Google Scholar] [CrossRef]
- Puga, B.; Gil, P.; De Arriba, A.B.; Labarta, J.I.; Romo, A.; Mayayo, E.; Ferrández Longás, Á. Neurocognitive Development of Children Born Small for Gestational Age (SGA). An Update. Pediatr. Endocrinol. Rev. 2012, 9, 716–726. [Google Scholar]
- Figueras, F.; Eixarch, E.; Meler, E.; Iraola, A.; Figueras, J.; Puerto, B.; Gratacos, E. Small-for-Gestational-Age Fetuses with Normal Umbilical Artery Doppler Have Suboptimal Perinatal and Neurodevelopmental Outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 136, 34–38. [Google Scholar] [CrossRef]
- Watt, J. Small-for-Gestational Age Infants: Perinatal, Physical and Social Factors in the First Year of Life. N. Z. Med. J. 1989, 102, 469–472. [Google Scholar]
- Feldman, R.; Eidelman, A.I. Neonatal State Organization, Neuromaturation, Mother-Infant Interaction, and Cognitive Development in Small-for-Gestational-Age Premature Infants. Pediatrics 2006, 118, e869–e878. [Google Scholar] [CrossRef] [Green Version]
- Geva, R.; Eshel, R.; Leitner, Y.; Valevski, A.F.; Harel, S. Neuropsychological Outcome of Children with Intrauterine Growth Restriction: A 9-Year Prospective Study. Pediatrics 2006, 118, 91–100. [Google Scholar] [CrossRef]
- Bakermans-Kranenburg, M.J.; van IJzendoorn, M.H. The Hidden Efficacy of Interventions: Gene× Environment Experiments from a Differential Susceptibility Perspective. Annu. Rev. Psychol. 2015, 66, 381–409. [Google Scholar] [CrossRef] [PubMed]
- Fukkink, R.G. Video Feedback in Widescreen: A Meta-Analysis of Family Programs. Clin. Psychol. Rev. 2008, 28, 904–916. [Google Scholar] [CrossRef]
- Brazelton, T.B. How to Help Parents of Young Children: The Touchpoints Model. J. Perinatol. 1999, 19, S6–S7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simões, R.V.B.; Cruz-Lemini, M.; Bargalló, N.; Gratacós, E.; Sanz-Cortés, M. Brain Metabolite Differences in One-Year-Old Infants Born Small at Term and Association with Neurodevelopmental Outcome. Am. J. Obstet. Gynecol. 2015, 213, 210.e1–210.e11. [Google Scholar] [CrossRef] [PubMed]
- Singhal, A. Long-Term Adverse Effects of Early Growth Acceleration or Catch-up Growth. Ann. Nutr. Metab. 2017, 70, 236–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakermans-Kranenburg, M.J.; Van Ijzendoorn, M.H.; Juffer, F. Less Is More: Meta-Analyses of Sensitivity and Attachment Interventions in Early Childhood. Psychol. Bull. 2003, 129, 195. [Google Scholar] [CrossRef]
- Juffer, F.; Struis, E.; Werner, C.; Bakermans-Kranenburg, M.J. Effective Preventive Interventions to Support Parents of Young Children: Illustrations from the Video-Feedback Intervention to Promote Positive Parenting and Sensitive Discipline (VIPP-SD). J. Prev. Interv. Community 2017, 45, 202–214. [Google Scholar] [CrossRef] [Green Version]
- Dozier, M.; Peloso, E.; Lindhiem, O.; Gordon, M.K.; Manni, M.; Sepulveda, S.; Ackerman, J.; Bernier, A.; Levine, S. Developing Evidence-Based Interventions for Foster Children: An Example of a Randomized Clinical Trial with Infants and Toddlers. J. Soc. Issues 2006, 62, 767–785. [Google Scholar] [CrossRef]
- Juffer, F.; Steele, M. What Words Cannot Say: The Telling Story of Video in Attachment-Based Interventions. Attach. Hum. Dev. 2014, 16, 307–314. [Google Scholar] [CrossRef]
- Marvin, R.S.; Cooper, C.; Hoffman, K.T.; Powell, B. The Circle of Security Project: Attachment-Based Intervention with Caregiver–Preschool Dyads’. Security 2002, 4, 248. [Google Scholar] [CrossRef]
- Cassidy, J.; Woodhouse, S.S.; Sherman, L.J.; Stupica, B.; Lejuez, C.W. Enhancing Infant Attachment Security: An Examination of Treatment Efficacy and Differential Susceptibility. Dev. Psychopathol. 2011, 23, 131–148. [Google Scholar] [CrossRef] [PubMed]
- Powell, B.; Cooper, G.; Hoffman, K.; Marvin, B. The Circle of Security Intervention: Enhancing Attachment in Early Parent–Child Relationships; Guilford Publications: New York, NY, USA, 2013. [Google Scholar]
- Beebe, B.; Steele, M. How Does Microanalysis of Mother-Infant Communication Inform Maternal Sensitivity and Infant Attachment? Attach. Hum. Dev. 2013, 15, 583–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downing, G.; Wortmann-fleischer, S.; Von Einsiedel, R.; Jordan, W.; Reck, C. Video Intervention Therapy for Parents With Psychiatric Disturbance. Infant Early Child. Ment. Heal. core concepts Clin. Pract. 2013, 261–280. [Google Scholar] [CrossRef]
- Papoušek, M. Resilience, Strengths, and Regulatory Capacities: Hidden Resources in Developmental Disorders of Infant Mental Health. Infant Ment. Health J. 2011, 32, 29–46. [Google Scholar] [CrossRef] [PubMed]
- Papousek, M.; Schieche, M.; Wurmser, H. Disorders of Behavioral and Emotional Regulation in the First Years of Life: Early Risks and Intervention in the Developing Parent–infant Relationship; ERIC: Washington DC, USA, 2007.
- Beebe, B. Brief Mother-Infant Treatment: Psychoanalytically Informed Video Feedback. Infant Ment. Health J. 2003, 24, 24–52. [Google Scholar] [CrossRef]
- Fonagy, P.; Steele, M.; Steele, H.; Moran, G.S.; Higgitt, A.C. The Capacity for Understanding Mental States: The Reflective Self in Parent and Child and Its Significance for Security of Attachment. Infant Ment. Health J. 1991, 12, 201–218. [Google Scholar] [CrossRef]
- Leyton, F.; Olhaberry, M.; Alvarado, R.; Rojas, G.; Dueñas, L.A.; Downing, G.; Steele, H. Video Feedback Intervention to Enhance Parental Reflective Functioning in Primary Caregivers of Inpatient Psychiatric Children: Protocol for a Randomized Feasibility Trial. Trials 2019, 20, 268. [Google Scholar] [CrossRef]
- Downing, G.; Bürgin, D.; Reck, C.; Ziegenhain, U. Interfaces between Intersubjectivity and Attachment: Three Perspectives on a Mother–Infant Inpatient Case. Infant Ment. Heal. J. Off. Publ. World Assoc. Infant Ment. Heal. 2008, 29, 278–295. [Google Scholar] [CrossRef]
- Crugnola, C.R.; Ierardi, E.; Albizzati, A.; Downing, G. Effectiveness of an Attachment-Based Intervention Program in Promoting Emotion Regulation and Attachment in Adolescent Mothers and Their Infants: A Pilot Study. Front. Psychol. 2016, 7, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Fonagy, P. Affect Regulation, Mentalization and the Development of the Self; Routledge: Abingdon, UK, 2018. [Google Scholar]
- Slade, A.; Holland, M.L.; Ordway, M.R.; Carlson, E.A.; Jeon, S.; Close, N.; Mayes, L.C.; Sadler, L.S. Minding the Baby®: Enhancing Parental Reflective Functioning and Infant Attachment in an Attachment-Based, Interdisciplinary Home Visiting Program. Dev. Psychopathol. 2020, 32, 123–137. [Google Scholar] [CrossRef]
- Sharp, C.; Fonagy, P. The Parent’s Capacity to Treat the Child as a Psychological Agent: Constructs, Measures and Implications for Developmental Psychopathology: Topic Review. Soc. Dev. 2008, 17, 737–754. [Google Scholar] [CrossRef] [Green Version]
- Facchini, S.; Martin, V.; Downing, G. Pediatricians, Well-Baby Visits, and Video Intervention Therapy: Feasibility of a Video-Feedback Infant Mental Health Support Intervention in a Pediatric Primary Health Care Setting. Front. Psychol 2016, 7, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Facchini, S.; Simonelli, A.; Sacchi, C.; Miscioscia, M.; Martin, V.; Downing, G.L. Intervention Vidéo Dans Les Soins Primaires Du Jeune Enfant (PC-VIT): La Consultation Du Pédiatre Comme Nouvelle Voie d’ Intervention Précoce En Vidéo-Feedback Video Intervention Therapy in Primary Care as a New Way for Early Intervention Utilisat. Devenir 2018, 30, 101–123. [Google Scholar] [CrossRef]
- Chambers, P.L.; Mahabee-Gittens, E.M.; Leonard, A.C. Vulnerable Child Syndrome, Parental Perception of Child Vulnerability, and Emergency Department Usage. Pediatr. Emerg. Care 2011, 27, 1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, R. Parenting Behavior as the Environment Where Children Grow. In Cambridge Handbooks in Psychology. The Cambridge Handbook of Environment in Human Development; Mayes, L.C., Lewis, M., Eds.; Cambridge University Press: Cambridge, UK, 2012; pp. 535–567. [Google Scholar] [CrossRef] [Green Version]
- Tronick, E. The Neurobehavioral and Social-Emotional Development of Infants and Children (Norton Series on Interpersonal Neurobiology); WW Norton and Company: New York, NY, USA, 2007. [Google Scholar]
- Eisenberg, N.; Spinrad, T.L.; Eggum, N.D. Emotion-Related and Its Relation to Children’s Maladjustment. Annu. Rev. Clin. Psychol. 2010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ordway, M.R.; Webb, D.; Sadler, L.S.; Slade, A. Parental Reflective Functioning: An Approach to Enhancing Parent–child Relationships in Pediatric Primary Care. J. Pediatr. Heal. Care 2015, 29, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Simpson, T.E.; Condon, E.; Price, R.M.; Finch, B.K.; Sadler, L.S.; Ordway, M.R. Demystifying Infant Mental Health: What the Primary Care Provider Needs to Know. J. Pediatr. Heal. Care 2016, 30, 38–48. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| PC-VIT Session | Theme | Task |
|---|---|---|
| 1 month | Touch and Cry | Free contact |
| 3 months | Affective matching/Descriptive language | Face to face |
| 6 months | Feeding | Eating together |
| 8 months | Separation and Autonomy | Separation procedure |
| 12 months | Reading | Reading together |
| 18 months | Limit setting | Don’t care procedure |
 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sacchi, C.; Facchini, S.; Downing, G.; Simonelli, A. The Primary Care-Video Intervention Therapy for Growth-Vulnerable Infants. A Case Study. Int. J. Environ. Res. Public Health 2020, 17, 1796. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051796
Sacchi C, Facchini S, Downing G, Simonelli A. The Primary Care-Video Intervention Therapy for Growth-Vulnerable Infants. A Case Study. International Journal of Environmental Research and Public Health. 2020; 17(5):1796. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051796
Chicago/Turabian StyleSacchi, Chiara, Sergio Facchini, George Downing, and Alessandra Simonelli. 2020. "The Primary Care-Video Intervention Therapy for Growth-Vulnerable Infants. A Case Study" International Journal of Environmental Research and Public Health 17, no. 5: 1796. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051796