Skeletal Class III Malocclusion with Lateral Open Bite and Facial Asymmetry Treated with Asymmetric Lower Molar Extraction and Lingual Appliance: A Case Report


Abstract
:1. Introduction
2. Materials and Methods
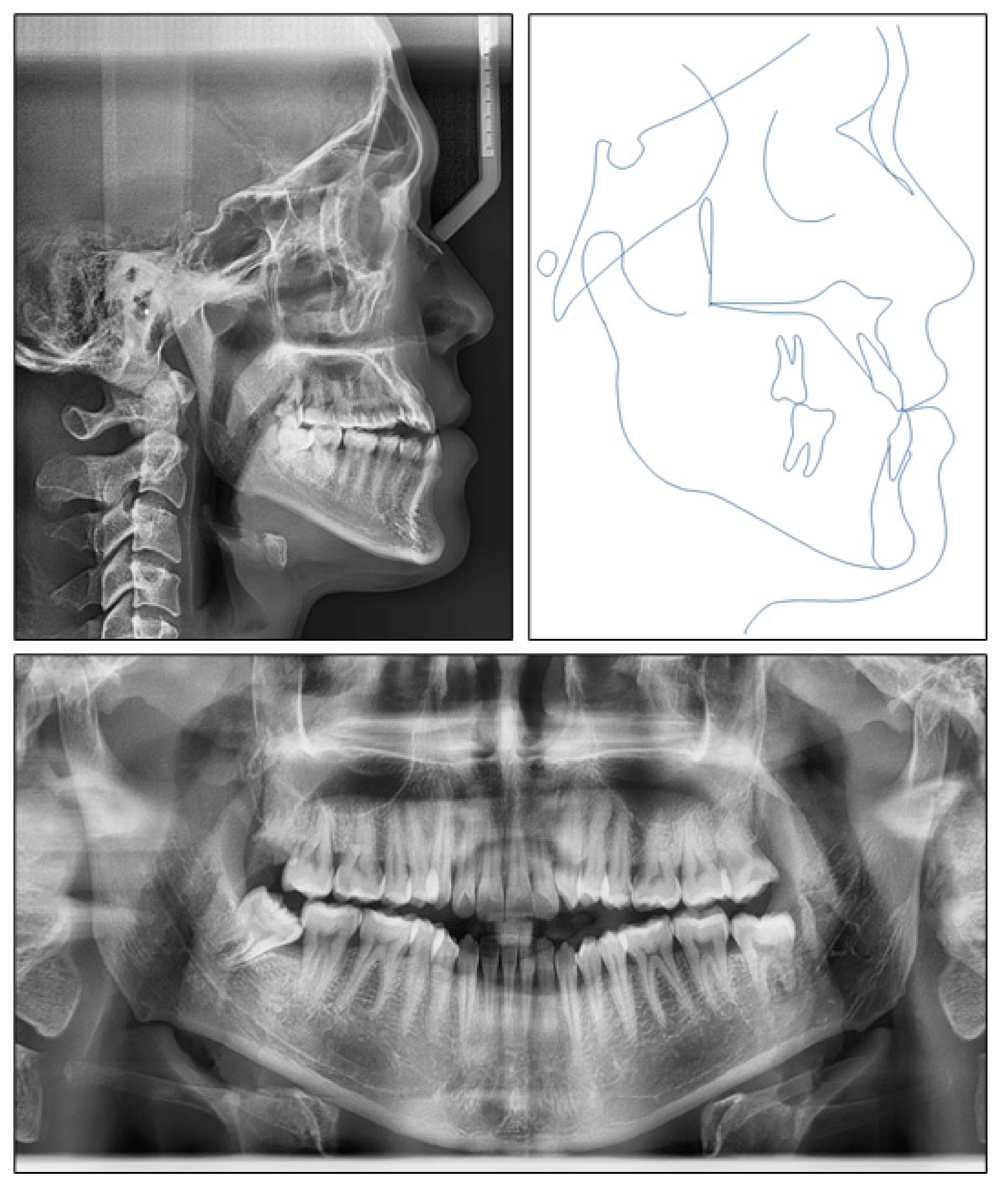
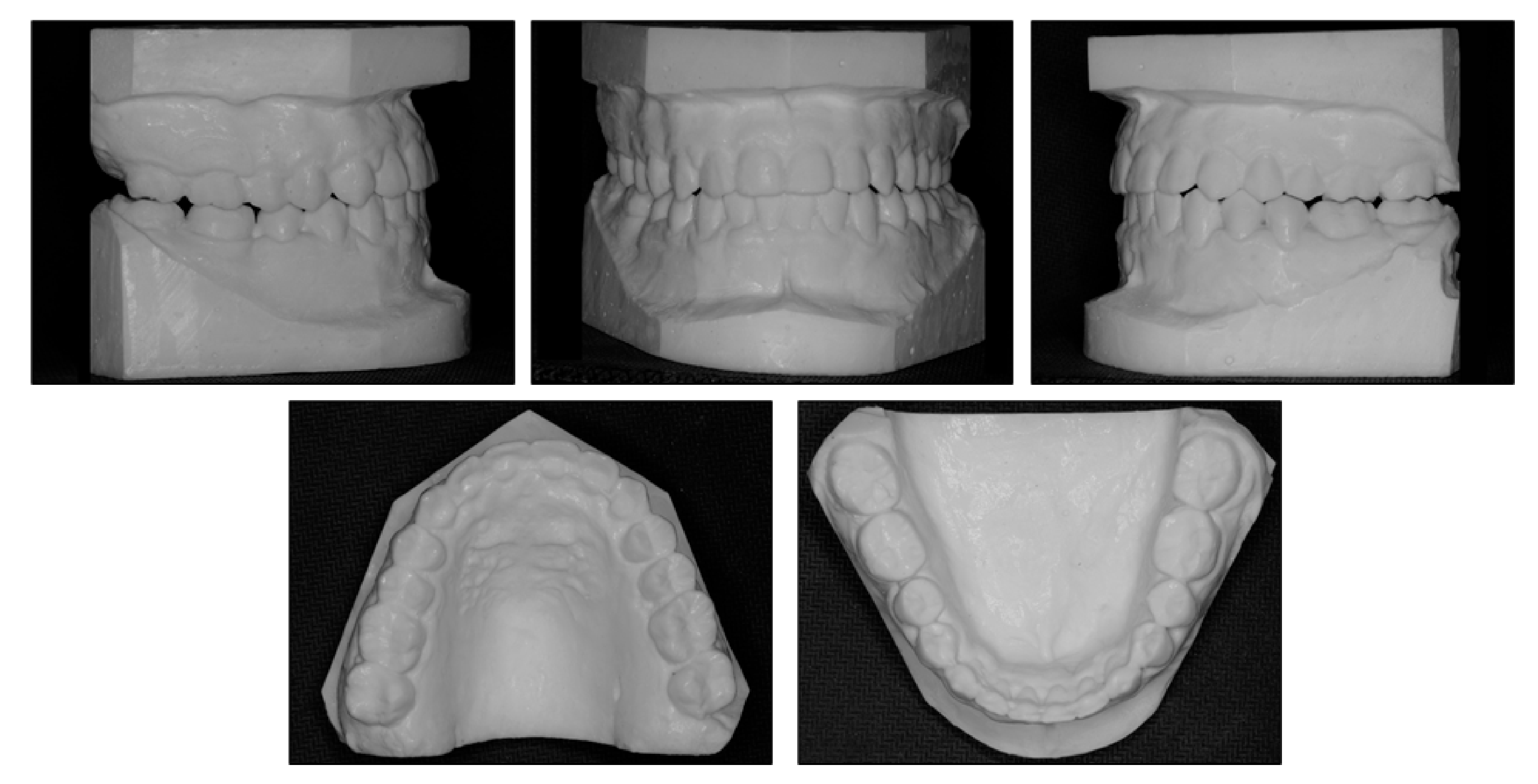
2.1. Diagnosis and Etiology
2.2. Treatment Objectives
2.3. Treatment Alternatives
- Orthognathic surgery would be used to set back the mandible and LeFort I osteotomy would correct the occlusal canting and mandibular lateral deviation. However, the patient refused surgery because of accompanying risks and costs;
- Extraction of upper second premolars and lower first premolars would be performed to achieve normal overjet and overbite, obtain molar Class I relationship and correct midline deviation. However, extraction in the upper arch would retract the upper lip and make the profile more concave;
- Extraction of upper third molars, lower right first premolar and left second premolar could be done. This option would not retract the upper lip, but the molar Class I relationship could not be achieved and the maxillary right second molar’s antagonist would be the mesially tipped third molar;
- Extraction of upper third molars, lower right first molar and left second molar would be performed. With this approach, the upper lip would not be retracted, and molar Class I relationship could be achieved. The rationale of asymmetric molar extraction was that mandibular right first molar extraction would provide more strong posterior molar anchorage to correct midline deviation and canine Class III relationship on the right side;
- Extraction of all four third molars would be applied in order to retract the entire lower arch with the help of temporary anchorage devices. However, the patient did not want to use any kind of skeletal anchorage. Additionally, first/second molar extraction would provide more space for correction of anteroposterior discrepancy.
2.4. Treatment Plan
2.5. Treatment Progress
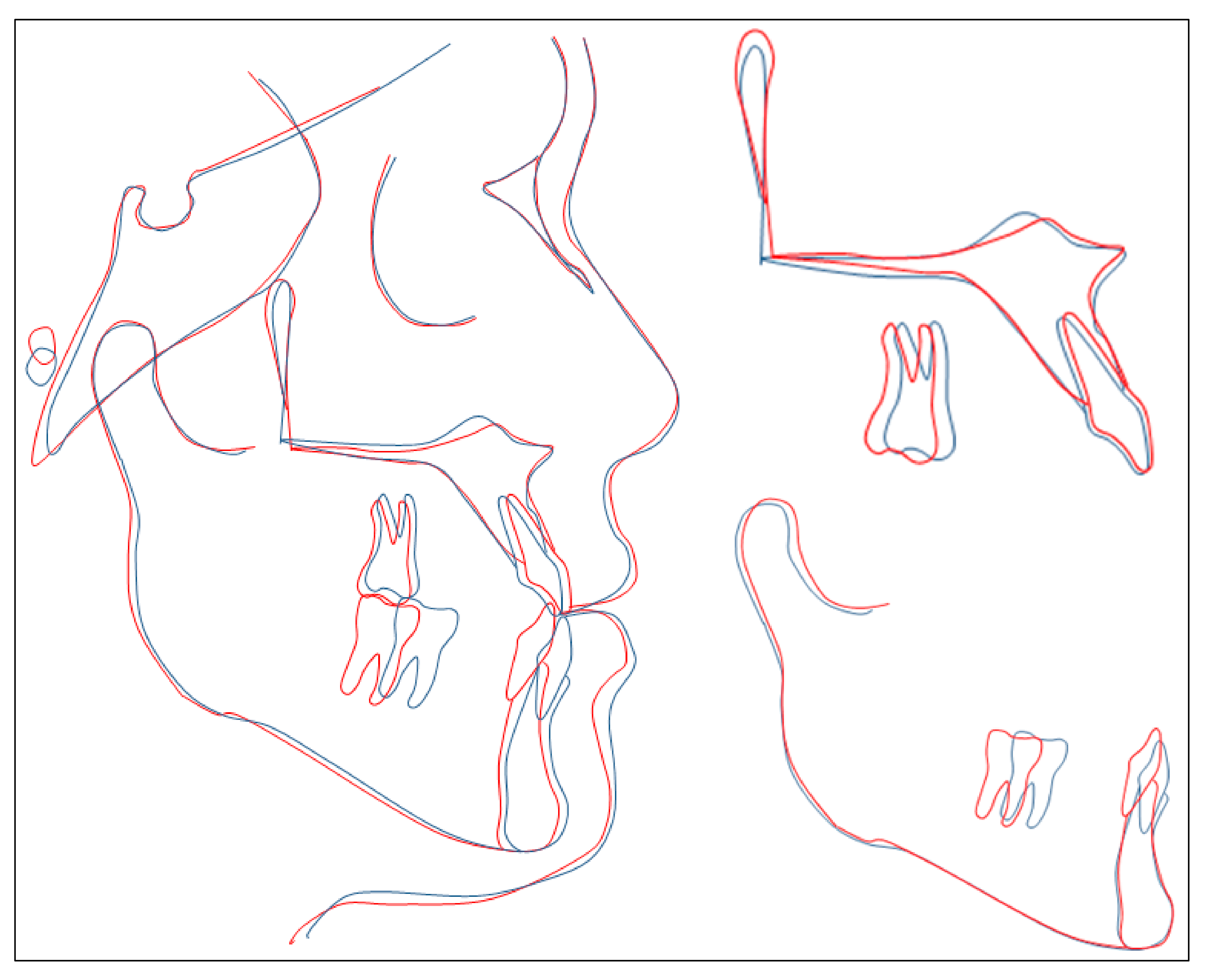
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antelo, O.M.; Meira, T.M.; Oliveira, D.D.; Pithon, M.M.; Tanaka, O.M. Long-term stability of a Class III malocclusion with severe anterior open bite and bilateral posterior crossbite in a hyperdivergent patient. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 408–421. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E., 3rd; McNamara, J.A., Jr. Components of adult Class III malocclusion. J. Oral. Maxillofac. Surg. 1984, 42, 295–305. [Google Scholar] [CrossRef]
- Sarver, D.M.; Weissman, S.M. Nonsurgical treatment of open bite in nongrowing patients. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 651–659. [Google Scholar] [CrossRef]
- Huang, G.J. Long-term stability of anterior open-bitetherapy: A review. Semin. Orthod. 2002, 8, 162–172. [Google Scholar] [CrossRef]
- Toffol, L.D.; Pavoni, C.; Baccetti, T.; Franchi, L.; Cozza, P. Orthopedic treatment outcomes in Class III malocclusion. A systematic review: A systematic review. Angle Orthod. 2008, 78, 561–573. [Google Scholar] [CrossRef]
- Greenlee, G.M.; Huang, G.J.; Chen, S.S.-H.; Chen, J.; Koepsell, T.; Hujoel, P. Stability of treatment for anterior open-bite malocclusion: A meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 154–169. [Google Scholar] [CrossRef]
- Sha, H.N.; Lim, S.Y.; Kwon, S.M.; Cha, J.-Y. Camouflage treatment for skeletal Class III patient with facial asymmetry using customized bracket based on CAD/CAM virtual orthodontic system: A case report. Angle Orthod. 2019, 90, 607–618. [Google Scholar] [CrossRef]
- Ahn, J.; Kim, S.-J.; Lee, J.-Y.; Chung, C.J.; Kim, K.-H. Transverse dental compensation in relation to sagittal and transverse skeletal discrepancies in skeletal Class III patients. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 148–156. [Google Scholar] [CrossRef]
- Seo, Y.-J.; Chung, K.-R.; Kim, S.-H.; Nelson, G. Camouflage treatment of skeletal class III malocclusion with asymmetry using a bone-borne rapid maxillary expander. Angle Orthod. 2015, 85, 322–334. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira Ruellas, A.C.; Baratieri, C.; Roma, M.B.; de Moraes Izquierdo, A.; Boaventura, L.; Rodrigues, C.S.; Telles, V. Angle Class III malocclusion treated with mandibular first molar extractions. Am. J. Orthod Dentofac. Orthop. 2012, 142, 384–392. [Google Scholar] [CrossRef]
- Lin, J.; Gu, Y. Lower second molar extraction in correction of severe skeletal class III malocclusion. Angle Orthod. 2006, 76, 217–225. [Google Scholar]
- Fujita, K. New orthodontic treatment with lingual bracket mushroom arch wire appliance. Am. J. Orthod. 1979, 76, 657–675. [Google Scholar] [CrossRef]
- Bellot-Arcís, C.; Ferrer-Molina, M.; Carrasco-Tornero, Á.; Montiel-Company, J.M.; Almerich-Silla, J.M. Differences in psychological traits between lingual and labial orthodontic patients: Perfectionism, body image, and the impact of dental esthetics. Angle Orthod. 2015, 85, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Rong, Q.; Lin, J.; Xu, B. Torque control of the maxillary incisors in lingual and labial orthodontics: A 3-dimensional finite element analysis. Am. J. Orthod Dentofac. Orthop. 2009, 135, 316–322. [Google Scholar] [CrossRef]
- Nguyen, V.A.; Nguyen, T.T.; Nguyen, T.T.H. Management of an adult patient with missing one mandibular incisor, severe overjet, and midline discrepancy with asymmetric extraction, lingual appliance, and skeletal anchorage: A case report. J. World Fed. Orthod. 2020, 9, 86–94. [Google Scholar] [CrossRef]
- E Cal-Netoa, J.P.; Quintaob, C.C.; de Menezesc, L.M.; Almeidad, M.A. Severe anterior open-bite malocclusion. Angle Orthod. 2006, 76, 728–733. [Google Scholar]
- Proffit, W.R.; Bailey, L.J.; Phillips, C.; Turvey, T.A. Long-term stability of surgical open-bite correction by Le Fort I osteotomy. Angle Orthod. 2000, 70, 112–117. [Google Scholar]
- Lopez-Gavito, G.; Wallen, T.R.; Little, R.M.; Joondeph, D.R. Anterior open-bite malocclusion: A longitudinal 10-year postretention evaluation of orthodontically treated patients. Am. J. Orthod. 1985, 87, 175–186. [Google Scholar] [CrossRef]
- Cao, L.; Zhang, K.; Bai, D.; Jing, Y.; Tian, Y.; Guo, Y. Effect of maxillary incisor labiolingual inclination and anteroposterior position on smiling profile esthetics. Angle Orthod. 2011, 81, 121–129. [Google Scholar] [CrossRef]
- Tai, K.; Park, J.H.; Tatamiya, M.; Kojima, Y. Distal movement of the mandibular dentition with temporary skeletal anchorage devices to correct a Class III malocclusion. Am. J. Orthod Dentofac. Orthop. 2013, 144, 715–725. [Google Scholar] [CrossRef]
- Kamioka, H.; Shiraga, N.; Takano-Yamamoto, T.; Yamashiro, T. Camouflage treatment using implant anchorage in a skeletal Class III patient. Orthod. Waves. 2009, 68, 171–177. [Google Scholar] [CrossRef]
- Yasuda, Y.; Iijima, M.; Mizoguchi, I. Camouflage treatment of severe skeletal Class III malocclusion with miniscrew anchorage. J. World Fed. Orthod. 2014, 3, 137–144. [Google Scholar] [CrossRef]
- Yanagita, T.; Kuroda, S.; Takano-Yamamoto, T.; Yamashiro, T. Class III malocclusion with complex problems of lateral open bite and severe crowding successfully treated with miniscrew anchorage and lingual orthodontic brackets. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 679–689. [Google Scholar] [CrossRef]
- Janson, G.; de Freitas, M.R.; Araki, J.; Franco, E.J.; Barros, S.E.C. Class III subdivision malocclusion corrected with asymmetric intermaxillary elastics. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Burstone, C.J. Diagnosis and treatment planning of patients with asymmetries. Semin. Orthod. 1998, 4, 153–164. [Google Scholar] [CrossRef]
- Burstone, C.J.; Choi, K. (Eds.) The Creative Use of Maxillo-mandibular Elastics. In The Biomechanical Foundation of Clinical Orthodontics; Quintessence Publishing: Batavia, IL, USA, 2015; pp. 63–88. [Google Scholar]
- Moullas, A.T.; Palomo, J.M.; Gass, J.R.; Amberman, B.D.; White, J.; Gustovich, D. Nonsurgical treatment of a patient with a Class III malocclusion. Am. J. Orthod. Dentofac. Orthop. 2006, 129, S111–S118. [Google Scholar] [CrossRef] [PubMed]
- Geron, S. How to control the vertical dimension in lingual orthodontics. In Lingual and Esthetic Orthodontics; Romano, R., Ed.; Quintessence Publishing: New Malden, UK, 2011; pp. 325–347. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pretreatment | Posttreatment | |
|---|---|---|
| SNA (°) | 85.1 | 83.8 |
| SNB (°) | 87.2 | 83.8 |
| ANB (°) | −2.1 | 0 |
| Wits appraisal | −8.1 | −0.3 |
| FMA (°) | 29.0 | 29.7 |
| U1-SN (°) | 110.9 | 107.0 |
| U1-NA (°) | 25.7 | 23.3 |
| U1-NA (mm) | 5.1 | 4.8 |
| L1-MP (°) | 77.2 | 89.6 |
| L1-NB (°) | 14.8 | 24.21 |
| L1-NB (mm) | 3.0 | 3.0 |
| U1-L1 (°) | 141.6 | 132.0 |
| E-line-upper lip (mm) | −3.8 | −2.8 |
| E-line-lower lip (mm) | −0.4 | −2.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngoc, V.T.N.; Phuong, N.T.T.; Anh, N.V. Skeletal Class III Malocclusion with Lateral Open Bite and Facial Asymmetry Treated with Asymmetric Lower Molar Extraction and Lingual Appliance: A Case Report. Int. J. Environ. Res. Public Health 2021, 18, 5381. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105381
Ngoc VTN, Phuong NTT, Anh NV. Skeletal Class III Malocclusion with Lateral Open Bite and Facial Asymmetry Treated with Asymmetric Lower Molar Extraction and Lingual Appliance: A Case Report. International Journal of Environmental Research and Public Health. 2021; 18(10):5381. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105381
Chicago/Turabian StyleNgoc, Vo Truong Nhu, Nguyen Thi Thu Phuong, and Nguyen Viet Anh. 2021. "Skeletal Class III Malocclusion with Lateral Open Bite and Facial Asymmetry Treated with Asymmetric Lower Molar Extraction and Lingual Appliance: A Case Report" International Journal of Environmental Research and Public Health 18, no. 10: 5381. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105381