
Effects and Responsiveness of a Multicomponent Intervention on Body Composition, Physical Fitness, and Leptin in Overweight/Obese Adolescents

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
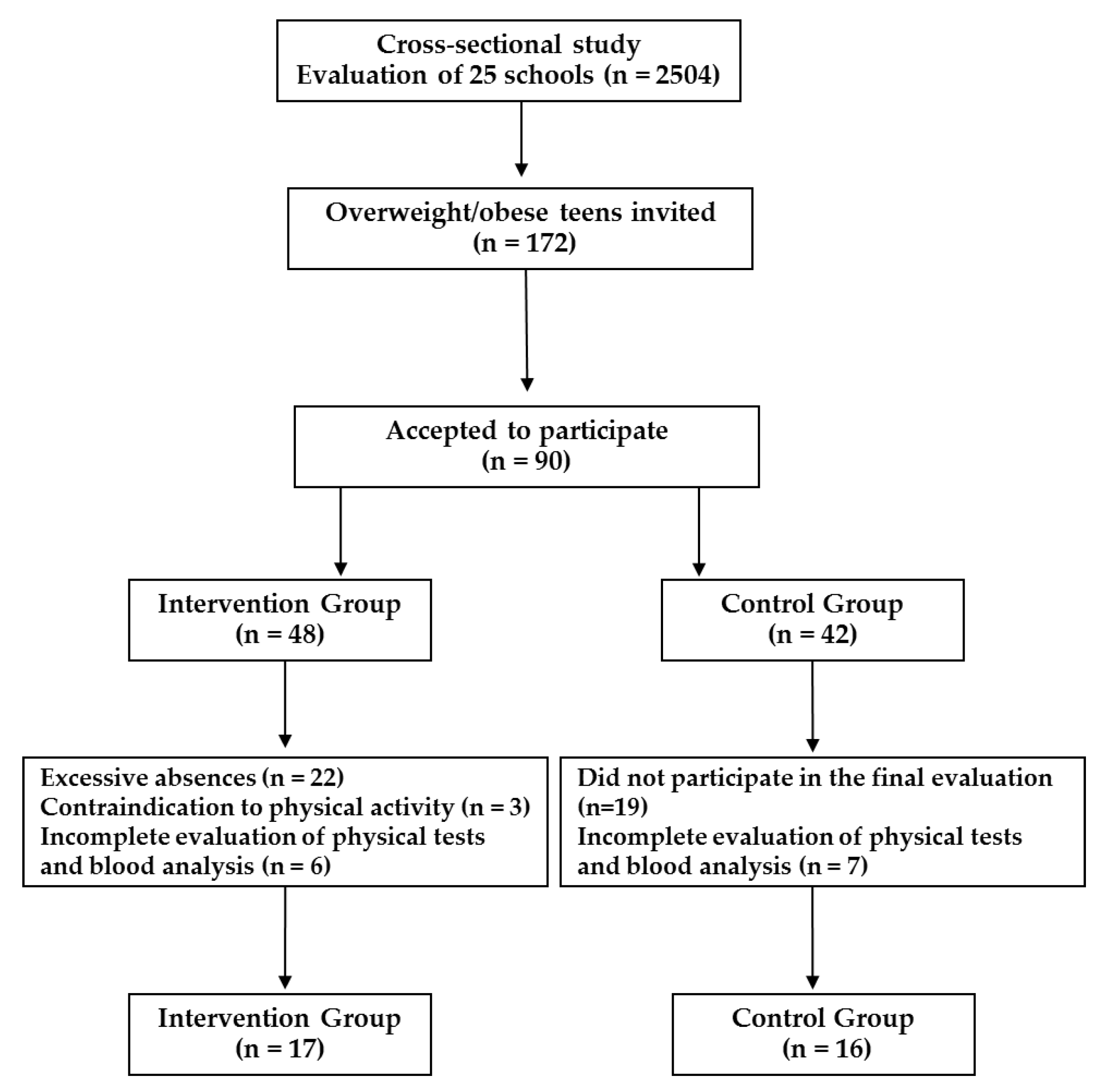
2.1. Study Design
2.2. Participants
2.3. Multicomponent Intervention Program
2.4. Physical Exercise Intervention
2.5. Nutritional Education Intervention
2.6. Psychological Intervention
2.7. Anthropometric Measures and Body Composition
2.8. Maturational Stages
2.9. Physical Fitness
2.10. Biochemical Assays
2.11. Statistical Analysis
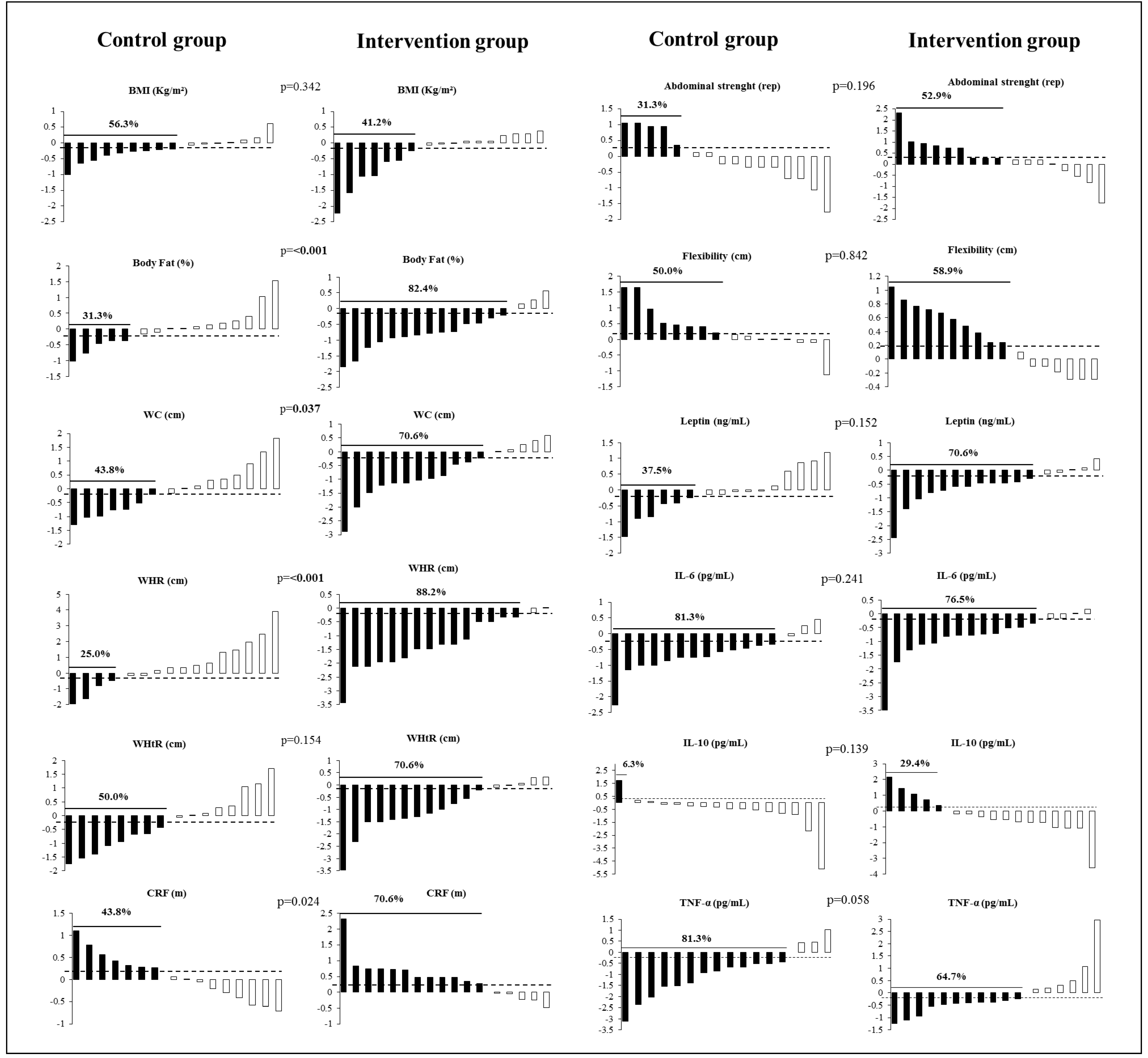
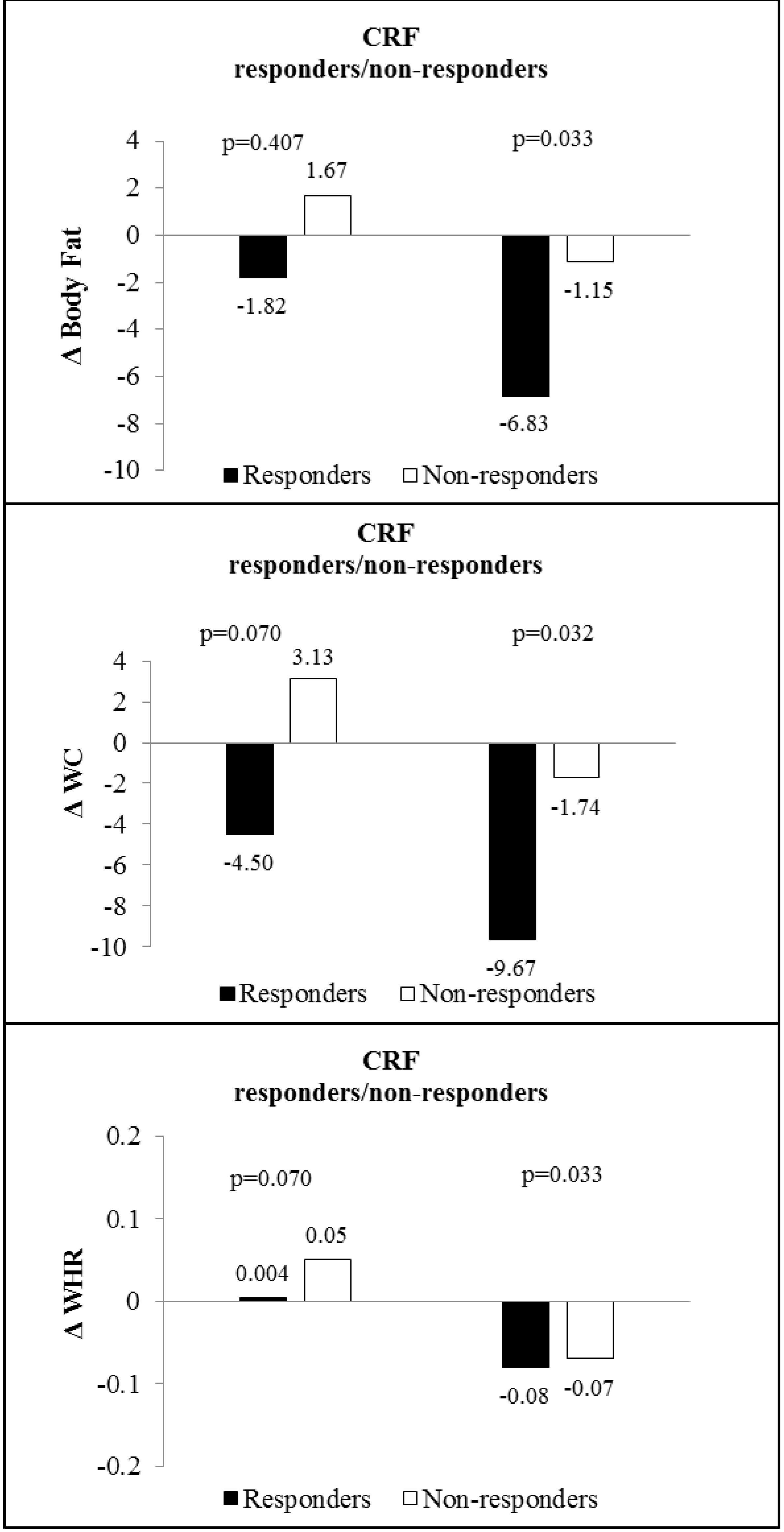
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases Country Profiles 2018. 2018. Available online: https://www.who.int/nmh/publications/ncd-profiles-2018/en/ (accessed on 3 June 2021).
- Yang, L.; Cao, C.; Kantor, E.D.; Nguyen, L.H.; Zheng, X.; Park, Y.; Giovannucci, E.L.; Matthews, C.E.; Colditz, G.A.; Cao, Y. Trends in Sedentary Behavior among the US Population, 2001–2016. J. Am. Med. Assoc. 2019, 321, 1587–1597. [Google Scholar] [CrossRef]
- Lavie, C.J.; De Schutter, A.; Parto, P.; Jahangir, E.; Milani, R.V. Milani obesity and prevalence of cardiovascular diseases and prognosis—The obesity paradox updated. Prog. Cardiovasc. Dis. 2016, 58, 537–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutinho, P.R.; Leite, N.; Lopes, W.A.; da Silva, L.R.; Consentino, C.M.; Araújo, C.T.; Moraes, F.B., Jr.; Jesus, I.C.; Cavaglieri, C.R.; Radominski, R.B. Association between adiposity indicators, metabolic parameters and inflammatory markers in a sample of female adolescents. Arch. Endocrinol. Metab. 2015, 59, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Murawska-Ciałowicz, E. Adipose tissue—Morphological and biochemical characteristic of different depots. Postepy. Hig. Med. Dosw. 2017, 71, 466–484. [Google Scholar] [CrossRef]
- Lumeng, C.N.; Saltiel, A.R. Inflammatory links between obesity and metabolic disease. J. Clin. Investig. 2011, 121, 2111–2117. [Google Scholar] [CrossRef] [Green Version]
- Schuster, D.P. Obesity and the development of type 2 diabetes: The effects of fatty tissue inflammation. Diabetes Metab. Syndr. Obes. Targets Ther. 2010, 3, 253–262. [Google Scholar] [CrossRef] [Green Version]
- Weiss, H.A.; Ferrand, R.A. Improving adolescent health: An evidence-based call to action. Lancet 2019, 393, 1073–1075. [Google Scholar] [CrossRef] [Green Version]
- Ameryoun, A.; Sanaeinasab, H.; Saffari, M.; Koenig, H.G. Impact of Game-Based Health Promotion Programs on body mass index in overweight/obese children and adolescents: A systematic review and meta-analysis of randomized controlled trials. Child. Obes. 2018, 14, 67–80. [Google Scholar] [CrossRef]
- Brand, C.; Martins, C.M.D.L.; Lemes, V.B.; Pessoa, M.L.F.; Dias, A.F.; Cadore, E.L.; Gaya, A.C.A.; Gaya, A.R. Effects and prevalence of responders after a multicomponent intervention on cardiometabolic risk factors in children and adolescents with overweight/obesity: Action for health study. J. Sports Sci. 2020, 38, 682–691. [Google Scholar] [CrossRef]
- Bonney, E.; Ferguson, G.; Burgess, T.; Smits-Engelsman, B. Benefits of activity-based interventions among female adolescents who are overweight and obese. Pediatr. Phys. Ther. 2019, 31, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Labayen, I.; Ruiz, J.R.; Rodríguez, G.; Breidenassel, C.; Castillo, M.; Pedrero, R.; Widhalm, K.; Kafatos, A.; Manios, Y.; et al. Cardiorespiratory fitness, waist circumference and liver enzyme levels in European adolescents: The HELENA cross-sectional study. J. Sci. Med. Sport 2017, 20, 932–936. [Google Scholar] [CrossRef]
- Da Luz Scheffer, D.; Latini, A. Exercise-induced immune system response: Anti-inflammatory status on peripheral and central organs. Biochim. Biophys. Acta–Mol. Basis Dis. 2020, 1866, 165823. [Google Scholar] [CrossRef] [PubMed]
- Dorneles, G.P.; Silva, I.; Boeira, M.C.R.; Valentini, D.; Romo, P.R.T. Cardiorespiratory fitness modulates the proportions of monocytes and T helper subsets in lean and obese men. Scand. J. Med. Sci. Sports 2019, 29, 1755–1765. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Arenaza, L.; Ramírez-Vélez, R.; Ortega, F.B.; Ruiz, J.R.; Labayen, I. Prevalence of responders for hepatic fat, adiposity and liver enzyme levels in response to a lifestyle intervention in children with overweight/obesity: EFIGRO randomized controlled trial. Pediatr. Diabetes 2020, 21, 215–223. [Google Scholar] [CrossRef]
- Leite, N.; Carvalho, H.M.; Padez, C.; Lopes, W.A.; Milano, G.E.; Radominski, R.B.; Coelho-E.-Silva, M.J. Age and menarcheal status do not influence metabolic response to aerobic training in overweight girls. Diabetol. Metab. Syndr. 2013, 5, 7. [Google Scholar] [CrossRef] [Green Version]
- WHO. World Health Organization. Growth Reference Data for 5–19 Years. Available online: https://www.who.int/growthref/who2007_bmi_for_age/en/ (accessed on 13 September 2020).
- Hulley, S.B.; Cummings, S.R.; Browner, W.S.; Grady, D.G.; Newman, T.B. Designing Clinical Research: An Epidemiologic Approach, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Poll, F.A.; Miraglia, F.; D’avila, H.F.; Reuter, C.P.; Mello, E.D. Impact of intervention on nutritional status, consumption of processed foods, and quality of life of adolescents with excess weight. J. Pediatr. 2020, 96, 621–629. [Google Scholar] [CrossRef]
- Lüdtke, L.; Silva, B.M.B.; Peuker, A.C.W.B.; Garcia, E.L. Obesidade, depressão e estresse: Relato de uma intervenção multidisciplinar em grupo com adolescentes Obesity, depression and stress: A report about a multidisciplinary intervention with a group of adolescents. Rev. Interdiscip. Promoção Saúde 2018, 1, 256–266. [Google Scholar] [CrossRef] [Green Version]
- Slaughter, M.H.; Lohman, T.G.; Boileau, R.A.; Horswill, C.A.; Stillman, R.J.; van Loan, M.D.; Bemben, D.A. Skinfold equations for estimation of body fatness in children and youth. Hum. Biol. 1988, 60, 709–723. [Google Scholar] [PubMed]
- Tanner, J.M. Growth at Adolescence, 2nd ed.; Blackwell Scientific: Oxford, UK, 1962. [Google Scholar]
- Gaya, A.; Gaya, A.R. Projeto Esporte Brasil: Manual de Testes e Avaliação; Universidade Federal do Rio Grande do Sul: Porto Alegre, Brazil, 2016. [Google Scholar]
- Gaya, A.C.A. Projeto Esporte Brasil: Manual de Aplicação de Medidas e Testes, Normas e Critérios de Avaliação; Universidade Federal do Rio Grande do Sul: Porto Alegre, Brasil, 2009. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Lopes, W.A.; Leite, N.; da Silva, L.R.D.; Brunelli, D.T.; Gáspari, A.F.; Radominski, R.B.; Chacon-Mikahil, M.P.T.; Cavaglieriet, C.R. Effects of 12 weeks of combined training without caloric restriction on inflammatory markers in overweight girls. J. Sports Sci. 2016, 34, 1902–1912. [Google Scholar] [CrossRef]
- Seo, Y.-G.; Lim, H.; Kim, Y.M.; Ju, Y.-S.; Lee, H.-J.; Jang, H.B.; Park, S.I.; Park, K.H. The effect of a multidisciplinary lifestyle intervention on obesity status, body composition, physical fitness, and cardiometabolic risk markers in children and adolescents with obesity. Nutrients 2019, 11, 137. [Google Scholar] [CrossRef] [Green Version]
- Klijn, P.H.; van der Baan-Slootweg, O.H.; van Stel, H.F. Aerobic exercise in adolescents with obesity: Preliminary evaluation of a modular training program and the modified shuttle test. BMC Pediatr. 2007, 7, 19. [Google Scholar] [CrossRef] [Green Version]
- Zguira, M.S.; Slimani, M.; Bragazzi, N.L.; Khrouf, M.; Chaieb, F.; Saïag, B.; Tabka, Z. Effect of an 8-week individualized training program on blood biomarkers, adipokines and endothelial function in obese young adolescents with and without metabolic syndrome. Int. J. Environ. Res. Public Health 2019, 16, 751. [Google Scholar] [CrossRef] [Green Version]
- Lau, P.W.C.; Kong, Z.; Choi, C.; Yu, C.C.W.; Chan, D.F.Y.; Sung, R.Y.T.; Leung, B.W.C. Effects of short-term resistance training on serum leptin levels in obese adolescents. J. Exerc. Sci. Fit. 2010, 8, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Leite, N.; da Silva, L.R.; da Jesus, Í.C.; Lopes, W.A.; Cavaglieri, C.R.; Consentino, C.L.; Radominski, R.B.; de Souza, R.L.R.; Tureck, L.V.; Furtado-Alle, L. ADRB2 Gln27Glu polymorphism influenced changes in leptin but not body composition or metabolic and other inflammatory parameters after twelve weeks of combined training in overweight adolescents. Mot. Rev. Educ. Física 2018, 23. [Google Scholar] [CrossRef] [Green Version]
- Sharma, V.K.; Subramanian, S.K.; Radhakrishnan, K.; Rajendran, R.; Ravindran, B.S.; Arunachalam, V. Comparison of structured and unstructured physical activity training on predicted VO2max and heart rate variability in adolescents—A randomized control trial. J. Basic Clin. Physiol. Pharm. 2017, 28, 225–238. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A.S.; Steinberger, J.; Olson, T.P.; Dengle, D.R. In the absence of weight loss, exercise training does not improve adipokines or oxidative stress in overweight children. Metabolism 2007, 56, 1005–1009. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Im, J.-A.; Kim, K.C.; Park, J.H.; Suh, S.-H.; Kang, E.S.; Kim, S.H.; Jekal, Y.; Lee, C.W.; Yoon, Y.-J.; et al. Improved insulin sensitivity and adiponectin level after exercise training in obese korean youth. Obesity 2007, 15, 3023–3030. [Google Scholar] [CrossRef]
- Murphy, E.C.-S.; Carson, L.; Neal, W.; Baylis, C.; Yeater, R. Effects of an exercise intervention using Dance Dance Revolution on endothelial function and other risk factors in overweight children. Int. J. Pediatr. Obes. 2009, 4, 205–214. [Google Scholar] [CrossRef]
- Romeo, J.; Martinez-Gomez, D.; Diaz, L.E.; Gómez-Martinez, S.; Marti, A.; Martin-Matillas, M.; Puertollano, M.A.; Veiga, O.L.; Martinez, J.A.; Wärnberg, J.; et al. Changes in cardiometabolic risk factors, appetite-controlling hormones and cytokines after a treatment program in overweight adolescents: Preliminary findings from the EVASYON study. Pediatr. Diabetes 2011, 12, 372–380. [Google Scholar] [CrossRef] [Green Version]
- Petersen, A.M.W.; Pedersen, B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef] [Green Version]
- Walsh, J.J.; Bonafiglia, J.T.; Goldfield, G.S.; Sigal, R.J.; Kenny, G.P.; Doucette, S.; Hadjiyannakis, S.; Alberga, A.S.; Prud’homme, S.; Gurd, B.J.; et al. Interindividual variability and individual responses to exercise training in adolescents with obesity. Appl. Physiol. Nutr. Metab. 2020, 45, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Yetgin, M.K.; Agopyan, A.; Kucukler, F.K.; Gedikbasi, A.; Yetgin, S.; Kayapinar, F.C.; Ozbar, N.; Bicer, B. The influence of physical training modalities on basal metabolic rate and leptin on obese adolescent boys. J. Pak. Med. Assoc. 2018, 68, 929–931. [Google Scholar]
- Aires, L.; Silva, P.; Silva, G.; Santos, M.P.; Ribeiro, J.C.; Mota, J. Intensity of physical activity, cardiorespiratory fitness, and body mass Index in youth. J. Phys. Act. Health 2010, 7, 54–59. [Google Scholar] [CrossRef]
- Do Nascimento, G.A.; Leite, N.; Furtado-Alle, L.; Teixeira, M.D.; Tureck, L.V. FTO rs9939609 does not interact with physical exercise but influences basal insulin metabolism in Brazilian overweight and obese adolescents. J. Obes. 2018, 26, 3134026. [Google Scholar] [CrossRef] [Green Version]
- Bonafiglia, J.T.; Rotundo, M.P.; Whittall, J.P.; Scribbans, T.D.; Gurd, B.J. Inter-individual variability in the adaptive responses to endurance and sprint interval training: A randomized crossover study. PLoS ONE 2016, 11, e0167790. [Google Scholar] [CrossRef] [PubMed]
- Pickering, C.; Kiely, J. Understanding personalized training responses: Can genetic assessment help? Open Sports Sci. J. 2017, 10, 191–213. [Google Scholar] [CrossRef]
- Pickering, C.; Kiely, J. Do non-responders to exercise exist—And if so, what should we do about them? Sport. Med. 2019, 49, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Rynders, C.; Weltman, A.; Delgiorno, C.; Balagopal, P.; Damaso, L.; Killen, K.; Mauras, N. Lifestyle intervention improves fitness independent of metformin in obese adolescents. Med. Sci. Sport. Exerc. 2012, 44, 786–792. [Google Scholar] [CrossRef] [Green Version]
- Elagizi, A.; Kachur, S.; Carbone, S.; Lavie, C.J.; Blair, S.N. A review of obesity, physical activity, and cardiovascular disease. Curr. Obes. Rep. 2020, 9, 571–581. [Google Scholar] [CrossRef]
- Sigal, R.J.; Alberga, A.S.; Goldfield, G.S.; Prud’homme, D.; Hadjiyannakis, S.; Gougeon, R.; Phillips, R.; Tulloch, H.; Malcolm, J.; Doucette, S.; et al. Effects of aerobic training, resistance training, or both on percentage body fat and cardiometabolic risk markers in obese adolescents. JAMA Pediatr. 2014, 168, 1006. [Google Scholar] [CrossRef]
- Mead, E.; Brown, T.; Rees, K.; Azevedo, L.B.; Ells, L.J. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst Rev. 2017, 6, CD012651. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 16) | Intervention Group (n = 17) | p | ||||
|---|---|---|---|---|---|---|
| Sex * | N (%) | N (%) | ||||
| Male | 8 (50.0) | 8 (47.1) | 0.86 | |||
| Female | 8 (50.0) | 9 (52.9) | ||||
| Maturational stages * | ||||||
| Not matured | 5 (31.2) | 1 (5.9) | 0.10 | |||
| Continuing maturation | 8 (50.0) | 14 (82.4) | ||||
| Matured | 3 (18.8) | 2 (11.7) | ||||
| Anova | ||||||
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | F | p | |
| Age (years) | 13.13 (1.41) | 12.37 to 13.88 | 13.00 (1.06) | 12.45 to 13.55 | 0.08 | 0.77 |
| Height (m) | 1.56 (0.09) | 1.50 to 1.60 | 1.60 (0.09) | 1.55 to 1.65 | 2.03 | 0.16 |
| Weight (kg) | 66.40 (13.72) | 59.09 to 73.71 | 72.63 (14.32) | 65.26 to 79.99 | 1.62 | 0.21 |
| BMI (kg/m2) | 27.14 (3.37) | 25.34 to 28.93 | 28.10 (4.38) | 25.85 to 30.35 | 0.49 | 0.48 |
| Body Fat (%) | 28.16 (5.05) | 25.47 to 30.85 | 31.50 (6.87) | 27.96 to 35.03 | 2.49 | 0.12 |
| WC (cm) | 79.57 (7.53) | 75.56 to 83.58 | 86.65 (11.28) | 80.85 to 92.45 | 4.44 | 0.04 |
| WHR (cm) | 0.79 (0.06) | 0.75 to 0.83 | 0.86 (0.07) | 0.81 to 0.89 | 6.60 | 0.01 |
| WHtR (cm) | 51.13 (4.44) | 48.76 to 53.49 | 54.06 (6.96) | 50.48 to 57.64 | 2.04 | 0.16 |
| Abdominal strength (rep) | 22.63 (6.88) | 18.96 to 26.29 | 20.65 (12.72) | 14.11 to 27.29 | 0.30 | 0.58 |
| Flexibility (cm) | 21.15 (10.31) | 15.66 to 26.65 | 20.44 (10.23) | 15.18 to 25.70 | 0.04 | 0.84 |
| CRF (m) | 808.88 (153.27) | 727.20 to 890.55 | 837.65 (168.60) | 750.96 to 924.33 | 0.26 | 0.61 |
| Leptin (ng/mL) | 3.18 (1.81) | 2.21 to 4.15 | 4.54 (2.33) | 3.34 to 5.74 | 3.48 | 0.07 |
| IL-6 (pg/mL) | 15.04 (4.75) | 12.51 to 17.58 | 18.71 (5.38) | 15.94 to 21.48 | 4.27 | 0.04 |
| IL-10 (pg/mL) | 1.68 (1.56) | 0.84 to 2.50 | 1.17 (0.37) | 0.98 to 1.36 | 1.70 | 0.22 |
| TNF-α (pg/mL) | 57.03 (18.65) | 47.09 to 66.96 | 61.65 (18.86) | 51.95 to 71.35 | 0.50 | 0.48 |
| GEE | Effect Size | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Δ% | p | Group | Time | Interaction | Cohen’s d | ||
| BMI (kg/m2) | CG | 27.13 (3.37) | 26.40 (4.21) | −2.72 | 0.347 | 0.672 | 0.005 | 0.322 | −0.52 * |
| IG | 28.10 (4.37) | 26.55 (4.30) | −5.51 | −0.48 | |||||
| Body Fat (%) | CG | 28.16 (5.05) | 28.30 (7.98) | 0.49 | 0.002 | 0. 769 | 0.001 | 0.001 | 0.03 |
| IG | 31.49 (6.87) | 26.33 (8.63) | 16.41 | −1.03 ** | |||||
| WC (cm) | CG | 79.57 (7.52) | 79.36 (10.66) | −0.25 | 0.023 | 0.226 | 0.009 | 0.014 | −0.02 |
| IG | 86.65 (11.27) | 79.31 (8.46) | −8.47 | −0.81 ** | |||||
| WHR (cm) | CG | 0.79 (0.06) | 0.82 (0.08) | 3.79 | <0.001 | 0.652 | 0.058 | <0.001 | 0.32 |
| IG | 0.85 (0.07) | 0.77 (0.04) | −9.30 | −1.41 ** | |||||
| WHtR (cm) | CG | 51.13 (4.44) | 49.85 (5.76) | −2.50 | 0.035 | 0.625 | <0.001 | 0.022 | −0.24 |
| IG | 54.06 (6.96) | 48.50 (4.66) | −10.26 | −0.93 ** | |||||
| Abdominal Strength (rep) | CG | 22.63 (6.87) | 22.00 (9.85) | −2.74 | 0.235 | 0.939 | 0.417 | 0.208 | −0.09 |
| IG | 20.65 (12.71) | 23.53 (8.39) | 13.94 | 0.30 | |||||
| Flexibility (cm) | CG | 21.15 (10.31) | 24.25 (9.21) | 14.66 | 0.998 | 0.826 | 0.001 | 0.998 | 0.46 |
| IG | 20.44 (10.23) | 23.52 (10.62) | 15.12 | 0.68 * | |||||
| CRF (m) | CG | 808.88 (153.27) | 819.06 (175.04) | 1.26 | 0.050 | 0.249 | 0.007 | 0.034 | 0.11 |
| IG | 837.65 (168.59) | 920.94 (202.27) | 9.94 | 0.71 * | |||||
| Leptin (ng/mL) | CG | 3.18 (1.81) | 3.06 (1.87) | −3.77 | 0.026 | 0.222 | 0.003 | 0.016 | −0.09 |
| IG | 4.54 (2.32) | 3.29 (2.17) | −27.5 | −0.85 ** | |||||
| IL-6 (pg/mL) | CG | 15.05 (4.75) | 12.03 (4.75) | −20.06 | 0.308 | 0.059 | <0.001 | 0.279 | −1.01 ** |
| IG | 18.71 (5.38) | 14.32 (5.22) | −23.46 | −0.98 ** | |||||
| IL_10 (pg/mL) | CG | 1.67 (1.55) | 0.92 (0.62) | −44.91 | 0.138 | 0.393 | 0.040 | 0.125 | −0.45 |
| IG | 1.17 (0.37) | 1.06 (0.38) | −9.40 | −0.23 | |||||
| TNF-α (pg/mL) | CG | 57.02 (18.64) | 41.18 (15.84) | −27.78 | 0.071 | 0.058 | 0.014 | 0.052 | −0.85 ** |
| IG | 61.65 (18.85) | 59.70 (28.90) | −3.01 | −0.07 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borfe, L.; Brand, C.; Schneiders, L.d.B.; Mota, J.; Cavaglieri, C.R.; Leite, N.; Renner, J.D.P.; Reuter, C.P.; Gaya, A.R. Effects and Responsiveness of a Multicomponent Intervention on Body Composition, Physical Fitness, and Leptin in Overweight/Obese Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 7267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147267
Borfe L, Brand C, Schneiders LdB, Mota J, Cavaglieri CR, Leite N, Renner JDP, Reuter CP, Gaya AR. Effects and Responsiveness of a Multicomponent Intervention on Body Composition, Physical Fitness, and Leptin in Overweight/Obese Adolescents. International Journal of Environmental Research and Public Health. 2021; 18(14):7267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147267
Chicago/Turabian StyleBorfe, Leticia, Caroline Brand, Letícia de Borba Schneiders, Jorge Mota, Claudia Regina Cavaglieri, Neiva Leite, Jane Dagmar Pollo Renner, Cézane Priscila Reuter, and Anelise Reis Gaya. 2021. "Effects and Responsiveness of a Multicomponent Intervention on Body Composition, Physical Fitness, and Leptin in Overweight/Obese Adolescents" International Journal of Environmental Research and Public Health 18, no. 14: 7267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147267