
A Longitudinal Study of the Relationship between Shift Work and Prostate-Specific Antigen in Healthy Male Workers


Abstract
:1. Introduction
2. Materials and Methods
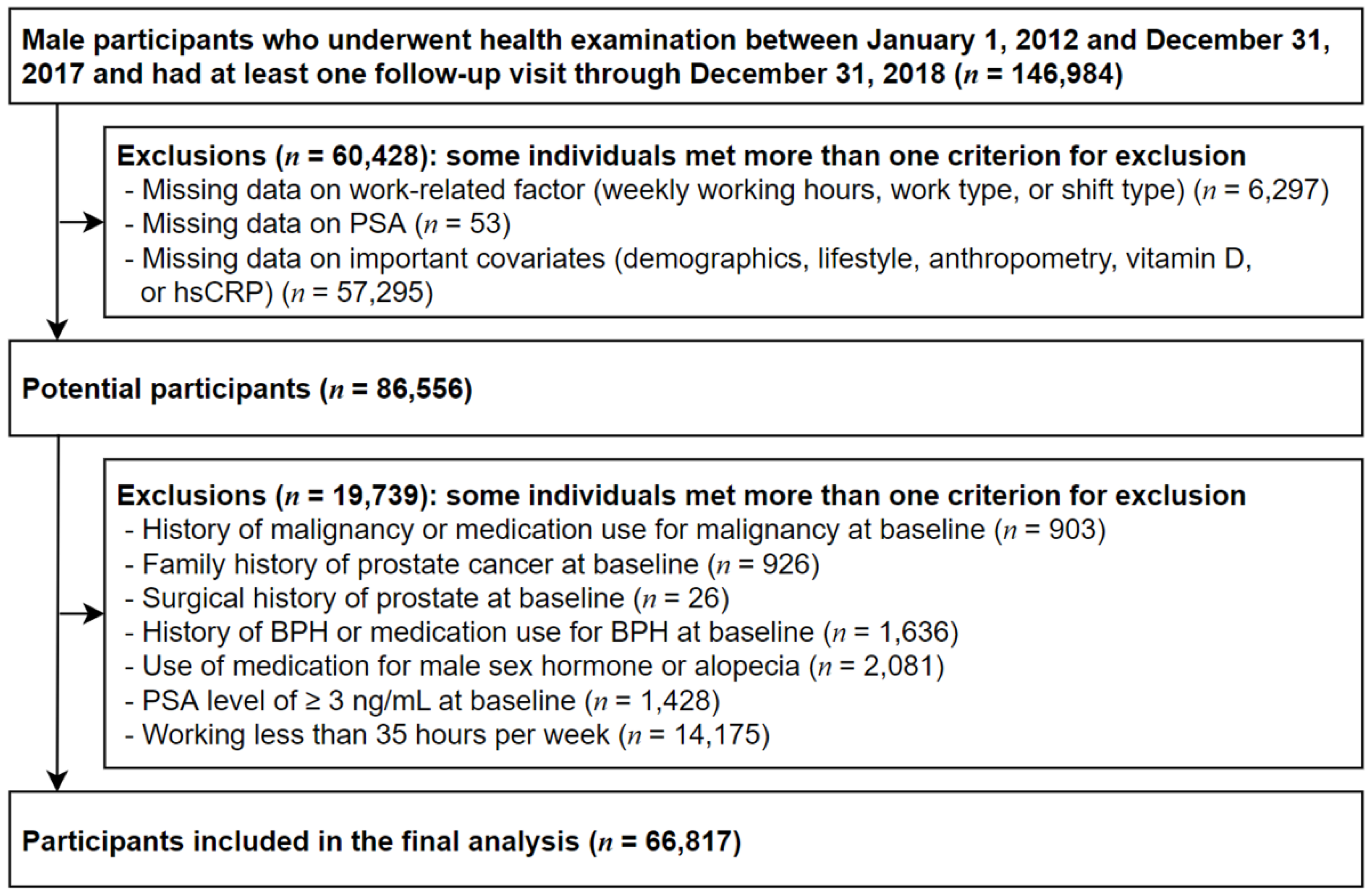
2.1. Study Population
2.2. Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bonnefond, A.; Tassi, P.; Roge, J.; Muzet, A. A critical review of techniques aiming at enhancing and sustaining worker’s alertness during the night shift. Ind. Health 2004, 42, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, M.Y.; Kwon, H.J.; Choi, K.H.; Kang, C.W.; Kim, H. The relationship between shift work and mental health among electronics workers in South Korea: A cross-sectional study. PLoS ONE 2017, 12, e0188019. [Google Scholar] [CrossRef]
- Alterman, T.; Luckhaupt, S.E.; Dahlhamer, J.M.; Ward, B.W.; Calvert, G.M. Prevalence rates of work organization characteristics among workers in the U.S.: Data from the 2010 National Health Interview Survey. Am. J. Ind. Med. 2013, 56, 647–659. [Google Scholar] [CrossRef] [Green Version]
- Do you Work Shifts? (Working Time)—European Working Conditions Survey—Data Visualisation. Available online: https://www.eurofound.europa.eu/data/european-working-conditions-survey (accessed on 21 February 2021).
- Han, S.H. Research Report for the Second Half of 2015: Chapter 3. Statistical Analysis of Working Hours; Statistics Research Institute of Statistics Korea: South, Korea, 2016.
- Torquati, L.; Mielke, G.I.; Brown, W.J.; Kolbe-Alexander, T. Shift work and the risk of cardiovascular disease. A systematic review and meta-analysis including dose-response relationship. Scand. J. Work. Environ. Health 2018, 44, 229–238. [Google Scholar] [CrossRef] [Green Version]
- D’Oliveira, T.C.; Anagnostopoulos, A. The Association Between Shift Work And Affective Disorders: A Systematic Review. Chronobiol. Int. 2021, 38, 182–200. [Google Scholar] [CrossRef]
- Knutsson, A.; Bøggild, H. Gastrointestinal disorders among shift workers. Scand. J. Work. Environ. Health 2010, 36, 85–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, E.M.; Germolec, D.; Kogevinas, M.; McCormick, D.; Vermeulen, R.; Anisimov, V.N.; Aronson, K.J.; Bhatti, P.; Cocco, P.; Costa, G.; et al. Carcinogenicity of night shift work. Lancet Oncol. 2019, 20, 1058–1059. [Google Scholar] [CrossRef]
- Straif, K.; Baan, R.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Bouvard, V.; Altieri, A.; Benbrahim-Tallaa, L.; Cogliano, V. Carcinogenicity of shift-work, painting, and fire-fighting. Lancet Oncol. 2007, 8, 1065–1066. [Google Scholar] [CrossRef]
- Cordina-Duverger, E.; Menegaux, F.; Popa, A.; Rabstein, S.; Harth, V.; Pesch, B.; Brüning, T.; Fritschi, L.; Glass, D.C.; Heyworth, J.S.; et al. Night shift work and breast cancer: A pooled analysis of population-based case-control studies with complete work history. Eur. J. Epidemiol. 2018, 33, 369–379. [Google Scholar] [CrossRef]
- Behrens, T.; Rabstein, S.; Wichert, K.; Erbel, R.; Eisele, L.; Arendt, M.; Dragano, N.; Bruning, T.; Jockel, K.H. Shift work and the incidence of prostate cancer: A 10-year follow-up of a German population-based cohort study. Scand. J. Work. Environ. Health 2017, 43, 560–568. [Google Scholar] [CrossRef] [Green Version]
- Lozano-Lorca, M.; Olmedo-Requena, R.; Vega-Galindo, M.V.; Vazquez-Alonso, F.; Jimenez-Pacheco, A.; Salcedo-Bellido, I.; Sanchez, M.J.; Jimenez-Moleon, J.J. Night Shift Work, Chronotype, Sleep Duration, and Prostate Cancer Risk: CAPLIFE Study. Int. J. Environ. Res. Public Health 2020, 17, 6300. [Google Scholar] [CrossRef] [PubMed]
- Mancio, J.; Leal, C.; Ferreira, M.; Norton, P.; Lunet, N. Does the association of prostate cancer with night-shift work differ according to rotating vs. fixed schedule? A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2018, 21, 337–344. [Google Scholar] [CrossRef] [Green Version]
- Catalona, W.J.; Smith, D.S.; Ratliff, T.L.; Dodds, K.M.; Coplen, D.E.; Yuan, J.J.; Petros, J.A.; Andriole, G.L. Measurement of prostate-specific antigen in serum as a screening test for prostate cancer. N. Engl. J. Med. 1991, 324, 1156–1161. [Google Scholar] [CrossRef]
- Whittemore, A.S.; Cirillo, P.M.; Feldman, D.; Cohn, B.A. Prostate specific antigen levels in young adulthood predict prostate cancer risk: Results from a cohort of Black and White Americans. J. Urol. 2005, 174, 872–876. [Google Scholar] [CrossRef]
- Schröder, F.H.; Hugosson, J.; Roobol, M.J.; Tammela, T.L.; Zappa, M.; Nelen, V.; Kwiatkowski, M.; Lujan, M.; Määttänen, L.; Lilja, H.; et al. Screening and prostate cancer mortality: Results of the European Randomised Study of Screening for Prostate Cancer (ERSPC) at 13 years of follow-up. Lancet 2014, 384, 2027–2035. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.; Kim, J.H.; Noh, J.W.; Cho, Y.S.; Park, H.J.; Joo, K.J.; Ryu, S. Prostate-Specific Antigen Within the Reference Range, Subclinical Coronary Atherosclerosis, and Cardiovascular Mortality. Circ. Res. 2019, 124, 1492–1504. [Google Scholar] [CrossRef]
- Song, Z.Y.; Yao, Q.; Zhuo, Z.; Ma, Z.; Chen, G. Circulating vitamin D level and mortality in prostate cancer patients: A dose-response meta-analysis. Endocr. Connect. 2018, 7, R294–R303. [Google Scholar] [CrossRef] [Green Version]
- Gann, P.H.; Hennekens, C.H.; Stampfer, M.J. A prospective evaluation of plasma prostate-specific antigen for detection of prostatic cancer. JAMA 1995, 273, 289–294. [Google Scholar] [CrossRef]
- Flynn-Evans, E.E.; Mucci, L.; Stevens, R.G.; Lockley, S.W. Shiftwork and prostate-specific antigen in the National Health and Nutrition Examination Survey. J. Natl. Cancer Inst. 2013, 105, 1292–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, S.; Park, W.J.; Kang, W.; Lim, D.Y.; Kim, S.; Moon, J.D. Night shiftwork and prostate-specific antigen level in a tire manufacturing factory. Ann. Occup. Environ. Med. 2019, 31, e19. [Google Scholar] [CrossRef] [PubMed]
- Barul, C.; Richard, H.; Parent, M.E. Night-Shift Work and Risk of Prostate Cancer: Results From a Canadian Case-Control Study, the Prostate Cancer and Environment Study. Am. J. Epidemiol. 2019, 188, 1801–1811. [Google Scholar] [CrossRef]
- Du, H.B.; Bin, K.Y.; Liu, W.H.; Yang, F.S. Shift work, night work, and the risk of prostate cancer: A meta-analysis based on 9 cohort studies. Medicine 2017, 96, e8537. [Google Scholar] [CrossRef] [PubMed]
- Gan, Y.; Li, L.; Zhang, L.; Yan, S.; Gao, C.; Hu, S.; Qiao, Y.; Tang, S.; Wang, C.; Lu, Z. Association between shift work and risk of prostate cancer: A systematic review and meta-analysis of observational studies. Carcinogenesis 2018, 39, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Jung, H.S.; Cho, J.; Zhang, Y.; Yun, K.E.; Lazo, M.; Pastor-Barriuso, R.; Ahn, J.; Kim, C.W.; Rampal, S.; et al. Metabolically Healthy Obesity and the Development of Nonalcoholic Fatty Liver Disease. Am. J. Gastroenterol. 2016, 111, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.; Yu, H.; Bai, Y.; Zheng, X.; Xie, L. Does night-shift work increase the risk of prostate cancer? A systematic review and meta-analysis. Onco Targets Ther. 2015, 8, 2817–2826. [Google Scholar] [CrossRef] [Green Version]
- Kubo, T.; Ozasa, K.; Mikami, K.; Wakai, K.; Fujino, Y.; Watanabe, Y.; Miki, T.; Nakao, M.; Hayashi, K.; Suzuki, K.; et al. Prospective cohort study of the risk of prostate cancer among rotating-shift workers: Findings from the Japan collaborative cohort study. Am. J. Epidemiol. 2006, 164, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Kubo, T.; Oyama, I.; Nakamura, T.; Kunimoto, M.; Kadowaki, K.; Otomo, H.; Fujino, Y.; Fujimoto, N.; Matsumoto, T.; Matsuda, S. Industry-based retrospective cohort study of the risk of prostate cancer among rotating-shift workers. Int. J. Urol. 2011, 18, 206–211. [Google Scholar] [CrossRef]
- Azab, S.; Osama, A.; Rafaat, M. Does normalizing PSA after successful treatment of chronic prostatitis with high PSA value exclude prostatic biopsy? Transl. Androl. Urol. 2012, 1, 148–152. [Google Scholar] [CrossRef]
- Werny, D.M.; Thompson, T.; Saraiya, M.; Freedman, D.; Kottiri, B.J.; German, R.R.; Wener, M. Obesity is negatively associated with prostate-specific antigen in U.S. men, 2001–2004. Cancer Epidemiol. Biomark. Prev. 2007, 16, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Romano, A.; Vigna, L.; Belluigi, V.; Conti, D.M.; Barberi, C.E.; Tomaino, L.; Consonni, D.; Riboldi, L.; Tirelli, A.S.; Andersen, L.L. Shift work and serum 25-OH vitamin D status among factory workers in Northern Italy: Cross-sectional study. Chronobiol. Int. 2015, 32, 842–847. [Google Scholar] [CrossRef]
- Petrou, S.; Mamais, I.; Lavranos, G.; Tzanetakou, I.P.; Chrysostomou, S. Effect of Vitamin D Supplementation in Prostate Cancer: A Systematic Review of Randomized Control Trials. Int. J. Vitam. Nutr. Res. 2018, 88, 100–112. [Google Scholar] [CrossRef]
- Fleet, J.C.; Kovalenko, P.L.; Li, Y.; Smolinski, J.; Spees, C.; Yu, J.G.; Thomas-Ahner, J.M.; Cui, M.; Neme, A.; Carlberg, C.; et al. Vitamin D Signaling Suppresses Early Prostate Carcinogenesis in TgAPT(121) Mice. Cancer Prev. Res. 2019, 12, 343–356. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N. Engl. J. Med. 2019, 380, 33–44. [Google Scholar] [CrossRef]
- Shahvazi, S.; Soltani, S.; Ahmadi, S.M.; de Souza, R.J.; Salehi-Abargouei, A. The Effect of Vitamin D Supplementation on Prostate Cancer: A Systematic Review and Meta-Analysis of Clinical Trials. Horm. Metab. Res. 2019, 51, 11–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganesan, S.; Magee, M.; Stone, J.E.; Mulhall, M.D.; Collins, A.; Howard, M.E.; Lockley, S.W.; Rajaratnam, S.M.W.; Sletten, T.L. The Impact of Shift Work on Sleep, Alertness and Performance in Healthcare Workers. Sci. Rep. 2019, 9, 4635. [Google Scholar] [CrossRef] [PubMed]
- Kakizaki, M.; Inoue, K.; Kuriyama, S.; Sone, T.; Matsuda-Ohmori, K.; Nakaya, N.; Fukudo, S.; Tsuji, I. Sleep duration and the risk of prostate cancer: The Ohsaki Cohort Study. Br. J. Cancer 2008, 99, 176–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savvidis, C.; Koutsilieris, M. Circadian rhythm disruption in cancer biology. Mol. Med. 2012, 18, 1249–1260. [Google Scholar] [CrossRef]
- Liu, R.; Wu, S.; Zhang, B.; Guo, M.; Zhang, Y. The association between sleep duration and prostate cancer: A systematic review and meta-analysis. Medicine 2020, 99, e21180. [Google Scholar] [CrossRef]
- Razavi, P.; Devore, E.E.; Bajaj, A.; Lockley, S.W.; Figueiro, M.G.; Ricchiuti, V.; Gauderman, W.J.; Hankinson, S.E.; Willett, W.C.; Schernhammer, E.S. Shift Work, Chronotype, and Melatonin Rhythm in Nurses. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1177–1186. [Google Scholar] [CrossRef]
- Xi, S.C.; Tam, P.C.; Brown, G.M.; Pang, S.F.; Shiu, S.Y. Potential involvement of mt1 receptor and attenuated sex steroid-induced calcium influx in the direct anti-proliferative action of melatonin on androgen-responsive LNCaP human prostate cancer cells. J. Pineal Res. 2000, 29, 172–183. [Google Scholar] [CrossRef]
- Shen, D.; Ju, L.; Zhou, F.; Yu, M.; Ma, H.; Zhang, Y.; Liu, T.; Xiao, Y.; Wang, X.; Qian, K. The inhibitory effect of melatonin on human prostate cancer. Cell Commun. Signal. 2021, 19, 34. [Google Scholar] [CrossRef] [PubMed]
- Altuwaijri, S. Role of Prostate Specific Antigen (PSA) in Pathogenesis of Prostate Cancer. J. Cancer Ther. 2012, 3, 331–336. [Google Scholar] [CrossRef] [Green Version]
- Bleyer, A.; Spreafico, F.; Barr, R. Prostate cancer in young men: An emerging young adult and older adolescent challenge. Cancer 2020, 126, 46–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidal, A.C.; Oyekunle, T.; Feng, T.; Freedland, A.R.; Moreira, D.; Castro-Santamaria, R.; Andriole, G.L.; Freedland, S.J.; Allott, E.H. Asian Race and Risk of Prostate Cancer: Results from the REDUCE Study. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2165–2170. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Shift Work Status | p-Value § | |||
|---|---|---|---|---|
| Characteristics | Overall | Daytime Worker | Shift Worker | |
| Number | 66,817 | 62,147 | 4670 | |
| Age (years) * | 37.2 (6.4) | 37.5 (6.4) | 33.0 (5.6) | <0.001 |
| Working hours (hours/week) * | 51.8 (9.2) | 51.8 (9.1) | 51.5 (10.3) | 0.068 |
| Sleep duration (hours/day) * | 6.2 (1.0) | 6.2 (1.0) | 6.3 (1.1) | <0.001 |
| Ever smoker (%) | 72.5 | 72.8 | 68.7 | <0.001 |
| Alcohol intake (%) a | 56.1 | 55.8 | 60.0 | <0.001 |
| Regular exercise (%) b | 13.3 | 13.0 | 16.8 | <0.001 |
| High education level (%) c | 90.4 | 92.0 | 69.4 | <0.001 |
| High household income (%) d | 33.3 | 34.7 | 15.4 | <0.001 |
| Marital status—married (%) | 79.2 | 80.5 | 61.3 | <0.001 |
| Obesity (%) e | 40.9 | 41.0 | 39.9 | 0.149 |
| BMI (kg/m2) * | 24.6 (3.0) | 24.6 (3.0) | 24.5 (3.3) | 0.013 |
| hsCRP (mg/L) # | 0.05 (0.03–0.10) | 0.05 (0.03–0.10) | 0.05 (0.03–0.10) | 0.766 |
| Total vitamin D (ng/mL) # | 16.5 (12.7–21.3) | 16.7 (12.8–21.4) | 14.9 (11.5–19.2) | <0.001 |
| PSA (ng/mL) * | 0.91 (0.46) | 0.91 (0.46) | 0.92 (0.47) | 0.592 |
| Shift Work Status | Person-Years (PY) | Incident Cases | Multivariable-Adjusted HR (95% CI) a | HR (95% CI) b in Model Using Time-Dependent Variables | |||
|---|---|---|---|---|---|---|---|
| Age-Adjusted Model | Model 1 * | Model 2 ** | Model 3 *** | ||||
| Daytime worker | 252,841.7 | 970 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Shift worker | 16,605.5 | 60 | 1.33 (1.02–1.72) | 1.35 (1.03–1.78) | 1.35 (1.03–1.77) | 1.37 (1.04–1.80) | 1.36 (1.04–1.79) |
| Shift Schedule Type | Person-Years (PY) | Incident Cases | Multivariable-Adjusted HR (95% CI) a | HR (95% CI) b in Model Using Time-Dependent Variables | |||
|---|---|---|---|---|---|---|---|
| Age-Adjusted Model | Model 1 * | Model 2 ** | Model 3 *** | ||||
| Daytime worker (n = 62,278) | 252,841.7 | 970 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Fixed shift worker (n = 245) | 978.5 | 4 | 1.11 (0.42–2.97) | 1.07 (0.40–2.86) | 1.07 (0.40–2.86) | 1.09 (0.41–2.90) | 1.08 (0.40–2.88) |
| Rotating shift worker (n = 3413) | 11,857.7 | 42 | 1.39 (1.02–1.90) | 1.45 (1.05–2.00) | 1.44 (1.04–2.00) | 1.47 (1.06–2.03) | 1.46 (1.06–2.02) |
| Other shift worker (n = 1018) | 3769.3 | 14 | 1.22 (0.72–2.06) | 1.22 (0.72–2.08) | 1.21 (0.71–2.06) | 1.23 (0.72–2.09) | 1.22 (0.72–2.07) |
| Subgroup | Shift Schedule Type | p for Interaction | |||
|---|---|---|---|---|---|
| Daytime Worker | Fixed Shift Worker | Rotating Shift Worker | Other Shift Worker | ||
| Age | 0.552 | ||||
| <40 years (n = 43,638) | 1.00 (reference) | 1.01 (0.25–4.06) | 1.33 (0.88–2.02) | 0.94 (0.44–1.99) | |
| ≥40 years (n = 23,179) | 1.00 (reference) | 1.17 (0.29–4.71) | 1.74 (1.02–2.97) | 1.74 (0.82–3.69) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.; Lee, W.; Kim, H.-R. A Longitudinal Study of the Relationship between Shift Work and Prostate-Specific Antigen in Healthy Male Workers. Int. J. Environ. Res. Public Health 2021, 18, 7458. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147458
Lee Y, Lee W, Kim H-R. A Longitudinal Study of the Relationship between Shift Work and Prostate-Specific Antigen in Healthy Male Workers. International Journal of Environmental Research and Public Health. 2021; 18(14):7458. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147458
Chicago/Turabian StyleLee, Yesung, Woncheol Lee, and Hyoung-Ryoul Kim. 2021. "A Longitudinal Study of the Relationship between Shift Work and Prostate-Specific Antigen in Healthy Male Workers" International Journal of Environmental Research and Public Health 18, no. 14: 7458. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147458