
Cultural Adaptation and Psychometric Properties of the Spanish Version of the Occupational Balance Questionnaire: An Instrument for Occupation-Based Research

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Recruitment
2.3. Instruments
2.4. Procedure
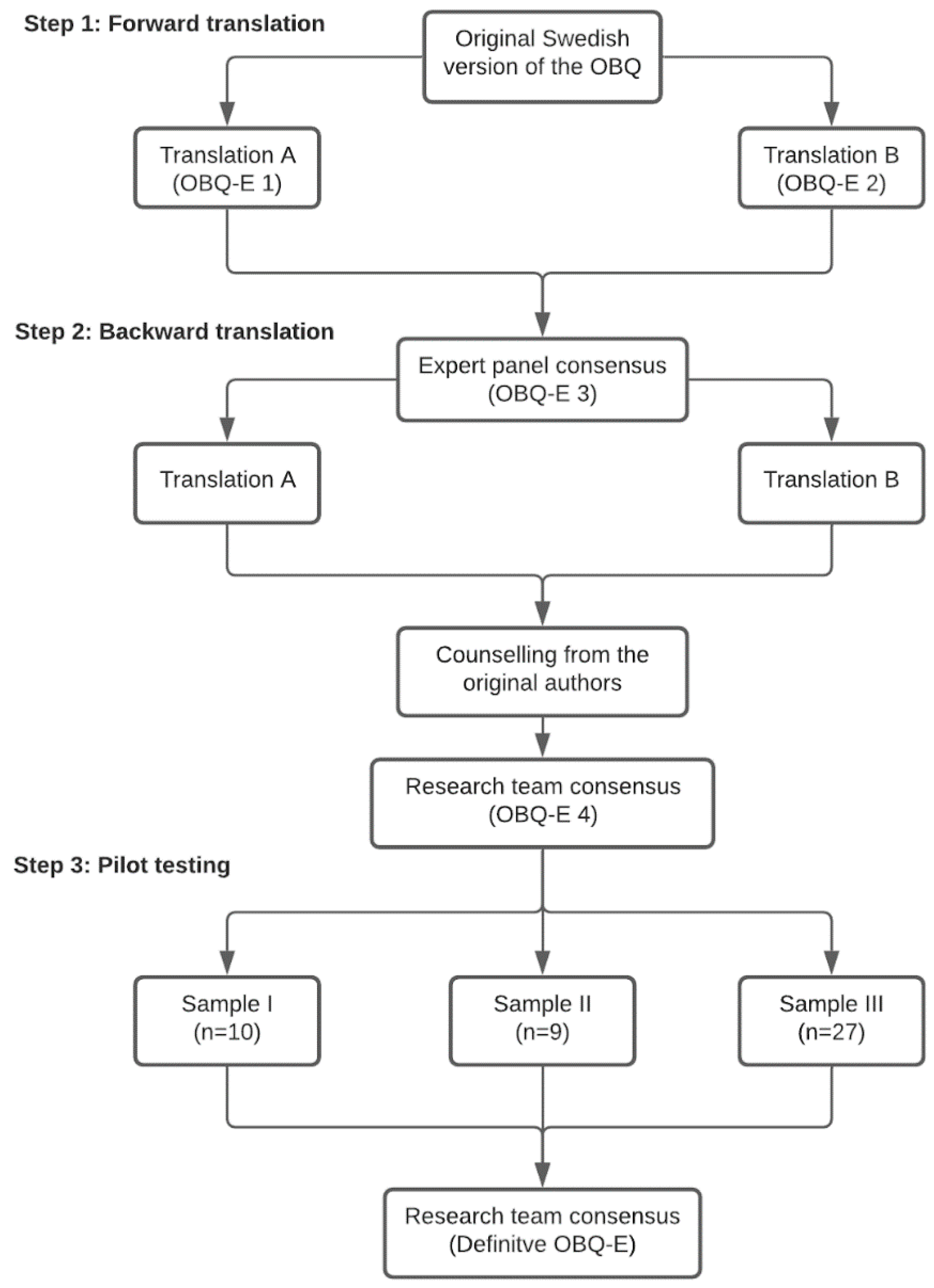
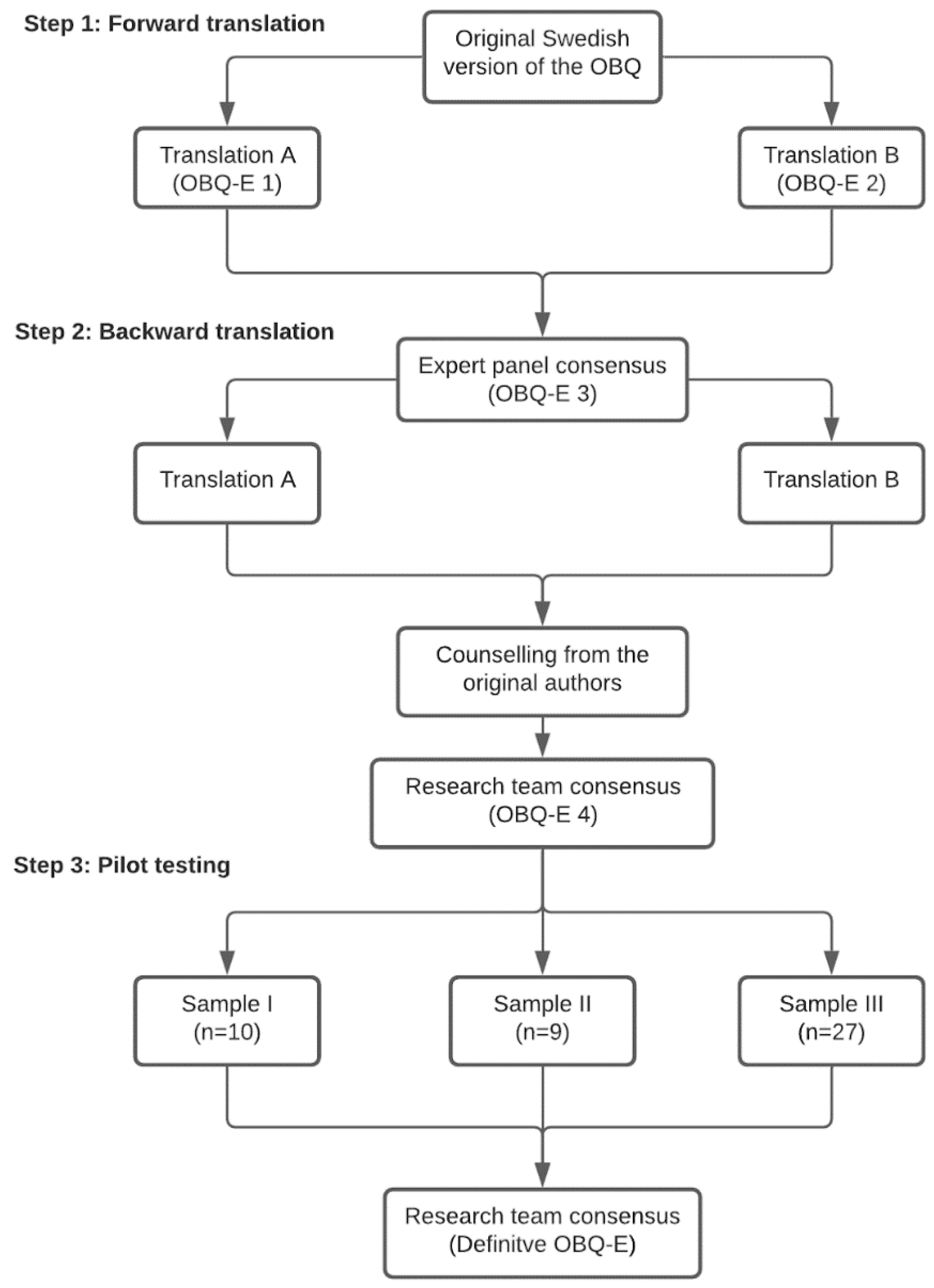
2.4.1. First Phase: Cross-Cultural Adaptation and Translation of the OBQ-E
2.4.2. Second Phase: Psychometric Testing of the OBQ-E
2.5. Data Analysis
3. Results
3.1. Cross-Cultural Adaptation, Translation, and Content Validity of the OBQ-E
3.1.1. Report on the Forward Translation
3.1.2. Report on the Backward Translation
3.1.3. Pilot Testing of the OBQ-E
3.2. Psychometric Testing of the OBQ-E
Internal Consistency, Test–Retest Reliability, and Convergent Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilcock, A.A. Occupation and Health: Are They One and the Same? J. Occup. Sci. 2007, 14, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Lee, H.J.; Jeon, B.-J.; Yoo, E.-Y.; Kim, J.-B.; Park, J.-H. Effects of Occupational Balance on Subjective Health, Quality of Life, and Health-Related Variables in Community-Dwelling Older Adults: A Structural Equation Modeling Approach. PLoS ONE 2021, 16, e0246887. [Google Scholar] [CrossRef]
- Wilcock, A.A. Occupational Science: Bridging Occupation and Health. Can. J. Occup. Ther. 2005, 72, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Håkansson, C.; Björkelund, C.; Eklund, M. Associations between Women’s Subjective Perceptions of Daily Occupations and Life Satisfaction, and the Role of Perceived Control. Aust. Occup. Ther. J. 2011, 58, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Håkansson, C.; Lissner, L.; Björkelund, C.; Sonn, U. Engagement in Patterns of Daily Occupations and Perceived Health among Women of Working Age. Scand. J. Occup. Ther. 2009, 16, 110–117. [Google Scholar] [CrossRef]
- Wagman, P.; Håkansson, C. Exploring Occupational Balance in Adults in Sweden. Scand. J. Occup. Ther. 2014, 21, 415–420. [Google Scholar] [CrossRef]
- Wilcock, A.A.; Chelin, M.; Hall, M.; Hamley, N.; Morrison, B.; Scrivener, L.; Townsend, M.; Treen, K. The Relationship between Occupational Balance and Health: A Pilot Study. Occup. Ther. Int. 1997, 4, 17–30. [Google Scholar] [CrossRef]
- Håkansson, C.; Ahlborg, G., Jr. Perceptions of Employment, Domestic Work, and Leisure as Predictors of Health among Women and Men. J. Occup. Sci. 2010, 17, 150–157. [Google Scholar] [CrossRef]
- Hunt, E.; McKay, E.A.; Dahly, D.L.; Fitzgerald, A.P.; Perry, I.J.; Person-Centred, A. Analysis of the Time-Use, Daily Activities and Health-Related Quality of Life of Irish School-Going Late Adolescents. Qual. Life Res. 2015, 24, 1303–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Håkansson, C.; Ahlborg, G. Occupational Imbalance and the Role of Perceived Stress in Predicting Stress-Related Disorders. Scand. J. Occup. Ther. 2018, 25, 278–287. [Google Scholar] [CrossRef]
- Matuska, K.; Bass, J.; Schmitt, J.S. Life Balance and Perceived Stress: Predictors and Demographic Profile. OTJR Occup. Particip. Health 2013, 33, 146–158. [Google Scholar] [CrossRef] [PubMed]
- Eklund, M.; Orban, K.; Argentzell, E.; Bejerholm, U.; Tjörnstrand, C.; Erlandsson, L.-K.; Håkansson, C. The Linkage between Patterns of Daily Occupations and Occupational Balance: Applications within Occupational Science and Occupational Therapy Practice. Scand. J. Occup. Ther. 2017, 24, 41–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dür, M.; Unger, J.; Stoffer, M.; Drăgoi, R.; Kautzky-Willer, A.; Fialka-Moser, V.; Smolen, J.; Stamm, T. Definitions of Occupational Balance and Their Coverage by Instruments. Br. J. Occup. Ther. 2015, 78, 4–15. [Google Scholar] [CrossRef]
- Wagman, P.; Håkansson, C. Introducing the Occupational Balance Questionnaire (OBQ). Scand. J. Occup. Ther. 2014, 21, 227–231. [Google Scholar] [CrossRef]
- Eklund, M.; Argentzell, E. Perception of Occupational Balance by People with Mental Illness: A New Methodology. Scand. J. Occup. Ther. 2016, 23, 304–313. [Google Scholar] [CrossRef]
- Dür, M.; Steiner, G.; Fialka-Moser, V.; Kautzky-Willer, A.; Dejaco, C.; Prodinger, B.; Stoffer, M.A.; Binder, A.; Smolen, J.; Stamm, T.A. Development of a New Occupational Balance-Questionnaire: Incorporating the Perspectives of Patients and Healthy People in the Design of a Self-Reported Occupational Balance Outcome Instrument. Health Qual. Life Outcomes 2014, 12, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eklund, M.; Erlandsson, L.-K.; Persson, D.; Hagell, P. Rasch Analysis of an Instrument for Measuring Occupational Value: Implications for Theory and Practice. Scand. J. Occup. Ther. 2009, 16, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Håkansson, C.; Wagman, P.; Hagell, P. Construct Validity of a Revised Version of the Occupational Balance Questionnaire. Scand. J. Occup. Ther. 2020, 27, 441–449. [Google Scholar] [CrossRef]
- Romero-Tébar, A.; Rodríguez-Hernández, M.; Segura-Fragoso, A.; Cantero-Garlito, P.A. Analysis of Occupational Balance and Its Relation to Problematic Internet Use in University Occupational Therapy Students. Healthcare 2021, 9, 197. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, P.; González-Santos, J.; Santamaría-Peláez, M.; Soto-Cámara, R.; González-Bernal, J.J. Exploring the Occupational Balance of Young Adults during Social Distancing Measures in the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 5809. [Google Scholar] [CrossRef]
- González-Bernal, J.J.; Santamaría-Peláez, M.; González-Santos, J.; Rodríguez-Fernández, P.; León del Barco, B.; Soto-Cámara, R. Relationship of Forced Social Distancing and Home Confinement Derived from the COVID-19 Pandemic with the Occupational Balance of the Spanish Population. J. Clin. Med. 2020, 9, 3606. [Google Scholar] [CrossRef]
- Fayers, P.; Bottomley, A.; EORTC Quality of Life Group; Quality of Life Unit. Quality of Life Research within the EORTC—The EORTC QLQ-C30. European Organisation for Research and Treatment of Cancer. Eur. J. Cancer 2002, 38 (Suppl. 4), S125–S133. [Google Scholar] [CrossRef]
- Nolte, S.; Liegl, G.; Petersen, M.A.; Aaronson, N.K.; Costantini, A.; Fayers, P.M.; Groenvold, M.; Holzner, B.; Johnson, C.D.; Kemmler, G.; et al. General Population Normative Data for the EORTC QLQ-C30 Health-Related Quality of Life Questionnaire Based on 15,386 Persons across 13 European Countries, Canada and the Unites States. Eur. J. Cancer 2019, 107, 153–163. [Google Scholar] [CrossRef]
- Arraras, J.I.; Arias, F.; Tejedor, M.; Pruja, E.; Marcos, M.; Martínez, E.; Valerdi, J. The EORTC QLQ-C30 (Version 3.0) Quality of Life Questionnaire: Validation Study for Spain with Head and Neck Cancer Patients. Psychooncology 2002, 11, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Atienza, F.L.; Pons, D.; Balaguer, I.; García-Merita, M. Propiedades psicométricas de la escala de satisfacción con la vida en adolescentes. Psicothema 2000, 12, 314–319. [Google Scholar]
- Pepper, D.; Hodgen, J.; Lamesoo, K.; Kõiv, P.; Tolboom, J. Think Aloud: Using Cognitive Interviewing to Validate the PISA Assessment of Student Self-Efficacy in Mathematics. Int. J. Res. Method Educ. 2018, 41, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality Criteria Were Proposed for Measurement Properties of Health Status Questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Faremi, Y.A. Reliability Coefficient of Multiple–Choice and Short Answer Objective Test Items in Basic Technology: Comparative Approach. J. Educ. Policy Entrep. Res. 2016, 3, 59–69. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; ISBN 978-0-203-77158-7. [Google Scholar]
- Yu, Y.; Manku, M.; Backman, C.L. Measuring Occupational Balance and Its Relationship to Perceived Stress and Health: Mesurer l’équilibre Occupationnel et Sa Relation Avec Le Stress Perçus et La Santé. Can. J. Occup. Ther. 2018, 85, 117–127. [Google Scholar] [CrossRef]
- Muñiz, J.; Elosua, P.; Hambleton, R.K.; International Test Commission. International Test Commission Guidelines for test translation and adaptation: Second edition. Psicothema 2013, 25, 151–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvajal, A.; Centeno, C.; Watson, R.; Martínez, M.; Sanz Rubiales, Á. ¿Cómo Validar Un Instrumento de Medida de La Salud? An. Sist. Sanit. Navar. 2011, 34, 63–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Streiner, D. Health Measurement Scales: A Practical Guide to Their Development and Use, 5th ed.; Oxford University Press: New York, NY, USA, 2015; ISBN 9780191765452. [Google Scholar]
- Instituto Nacional de Estadística (INE). Available online: https://www.ine.es/ (accessed on 16 June 2021).

{kind=link}
| Variables | Sample I 1 (n = 10) | Sample II 1 (n = 9) | Sample III 1 (n = 27) | Sample IV 1 (n = 219) |
|---|---|---|---|---|
| Age, mean (SD) | 47.2 (9.2) | 31.6 (7.5) | 26.2 (4.0) | 22.2 (3.9) |
| Age range, min.-max. | 35–64 | 23–46 | 23–37 | 18–48 |
| Sex, n (%) | ||||
| Male | 1 (10.0) | - | 2 (7.4) | 23 (10.5) |
| Female | 9 (90.0) | 9 (100.0) | 25 (99.6) | 196 (89.5) |
| Marital status, n (%) | ||||
| Single/divorced | 2 (20.0) | 6 (66.6) | 22 (81.5) | 207 (94.5) |
| Spouse/domestic partner | 8 (80.0) | 3 (33.3) | 5 (18.5) | 9 (4.1) |
| Children aged less than 18, n (%) | ||||
| yes | 4 (40.0) | 3 (33.3) | 1 (3.7) | 7 (3.2) |
| no | 6 (60.0) | 6 (66.6) | 26 (96.3) | 206 (94.1) |
| Professional status, n (%) | ||||
| Student | - | 7 (77.7) | - | 174 (79.5) |
| Student and worker | - | 2 (22.2) | - | 45 (20.5) |
| Worker | 9 (90.0) | - | 17 (63.0) | - |
| Unemployed | 1 (10.0) | - | 10 (37.0) | - |
| Educational level, n (%) | ||||
| Primary studies | 1 (10.0) | - | - | - |
| Secondary studies | 5 (50.0) | - | - | - |
| University studies | 4 (40.0) | 9 (100.0) | 27 (100.0) | 219 (100.0) |
| Degree in occupational therapy, n (%) | ||||
| 1st year | - | - | - | 38 (17.4) |
| 2nd year | - | - | - | 59 (26.9) |
| 3rd year | - | - | - | 51 (23.3) |
| 4th year | - | 9 (100.0) | - | 71 (32.4) |
| Item Description | Sample I 1 (n = 10) | Sample II 1 (n = 9) | Sample III 1 (n = 27) |
|---|---|---|---|
| 1. Balance between doing things for others/for oneself. | Understandable. Proposals: to specify activities (work, leisure, etc.), replace balance with another word. | Understandable. No proposals. | Understandable. No proposals. |
| 2. Perceiving one’s occupations as meaningful. | Understandable. Proposals: to specify activities (work, leisure, etc.). | Understandable. Proposals: to explain what the activities of daily life are. | Understandable. Proposals: to specify more or ask as a question. |
| 3. Time for doing things wanted. | Understandable. Proposals: to specify activity by activity, e.g., “I do the work I really want to do”. | Understandable. Proposals: to specify more. | Understandable. No proposals. |
| 4. Balance between work, home, family, leisure, rest, and sleep. | Understandable. No proposals. | Understandable. No proposals. | Understandable. Proposals: to add the “study”. |
| 5. Balance between doing things alone/with others. | It was understood as either variety between groups of activities or difference between groups. Proposals: to divide the item by types of activity. | It was understood as either variety between groups of activities or difference between groups. No proposals | It was understood as either variety between groups of activities or difference between groups. Proposals: to clarify the comparison by indicating if they are imposed activities or not. |
| 6. Having sufficient to do during a typical week. | Understandable. Proposals: to indicate if it is about leisure activities or obligations. | Understandable. Proposals: to indicate if it is about leisure activities or obligations. | Understandable. Proposals: to clarify the term “sufficient” and specify activities (work, leisure, etc.). |
| 7. Have sufficient time for doing obligatory occupations. | Understandable. Proposals: to specify if activities are general or specific. | Understandable. No proposals. | Understandable. Proposals: to indicate if it refers to obligations or activities that you want to do. |
| 8. Balance between physical, social, mental, and restful occupations. | Understandable. Proposals: to ask as a question considering the time factor. | Understandable. No proposals. The question arises whether all the items must be answered even if they seem similar. | Understandable. Proposals: to include “emotional” activities. |
| 9. Satisfaction with how time is spent in daily life. | Understandable. No proposals. | Understandable. No proposals. | Understandable. No proposals. |
| 10. Satisfaction with the number of activities during a typical week. | Understandable. Proposals: to specify if activities are general or leisure activities. | Understandable. Proposals: to specify if activities are general or leisure activities. | Understandable. No proposals. |
| 11. Balance between obligatory/voluntary occupations. | Understandable. No proposals. | Understandable. Proposal: to include the temporal factor. | Understandable. Proposal: to clarify the term “variety”, make the item more concrete. |
| 12. Balance between energy-giving/energy-taking activities. | Understandable. Proposals: to give concrete examples. | Understandable. Proposals: to give concrete examples. | Understandable. Proposals: to give concrete examples. |
| 13. Satisfaction with time spent in rest, recovery, and sleep. | Understandable. No proposals. | Understandable. No proposals. | Understandable. No proposals. |
| Measures | Min. | Max. | Median | P25 | P75 | M | SD | rs | p |
|---|---|---|---|---|---|---|---|---|---|
| OBQ-E | 22 | 65 | 44 | 39 | 49 | 43.6 | 7.8 | - | - |
| GHS/HoL | |||||||||
| Overall status | 1 | 7 | 6 | 5 | 6 | 5.5 | 1 | 0.37 | <0.001 |
| Related QoL | 1 | 7 | 6 | 5 | 6 | 5.7 | 1.1 | 0.42 | <0.001 |
| SWLS | 6 | 25 | 20 | 18 | 22 | 19.4 | 3.7 | 0.54 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peral-Gómez, P.; López-Roig, S.; Pastor-Mira, M.Á.; Abad-Navarro, E.; Valera-Gran, D.; Håkansson, C.; Wagman, P. Cultural Adaptation and Psychometric Properties of the Spanish Version of the Occupational Balance Questionnaire: An Instrument for Occupation-Based Research. Int. J. Environ. Res. Public Health 2021, 18, 7506. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147506
Peral-Gómez P, López-Roig S, Pastor-Mira MÁ, Abad-Navarro E, Valera-Gran D, Håkansson C, Wagman P. Cultural Adaptation and Psychometric Properties of the Spanish Version of the Occupational Balance Questionnaire: An Instrument for Occupation-Based Research. International Journal of Environmental Research and Public Health. 2021; 18(14):7506. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147506
Chicago/Turabian StylePeral-Gómez, Paula, Sofía López-Roig, María Ángeles Pastor-Mira, Ester Abad-Navarro, Desirée Valera-Gran, Carita Håkansson, and Petra Wagman. 2021. "Cultural Adaptation and Psychometric Properties of the Spanish Version of the Occupational Balance Questionnaire: An Instrument for Occupation-Based Research" International Journal of Environmental Research and Public Health 18, no. 14: 7506. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147506