
TB Antigen-Stimulated CXCR3 Ligand Assay for Diagnosis of Tuberculous Lymphadenitis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Lymph Node Sample Collection
2.2. Mycobacterial Culture
2.3. Histopathology
2.4. Polymerase Chain Reaction
2.5. Evaluation and Treatment of TB
2.6. Plasma Sampling and Measurement of Marker Levels
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
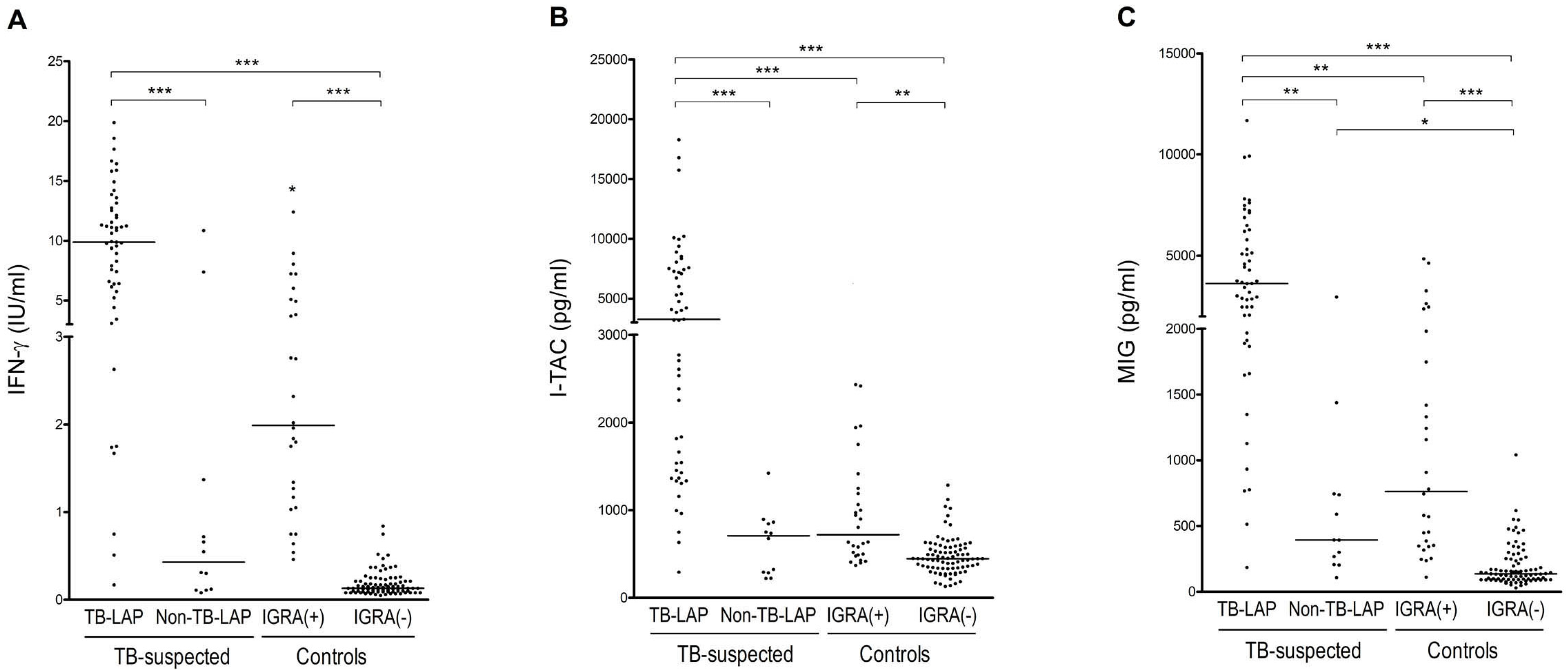
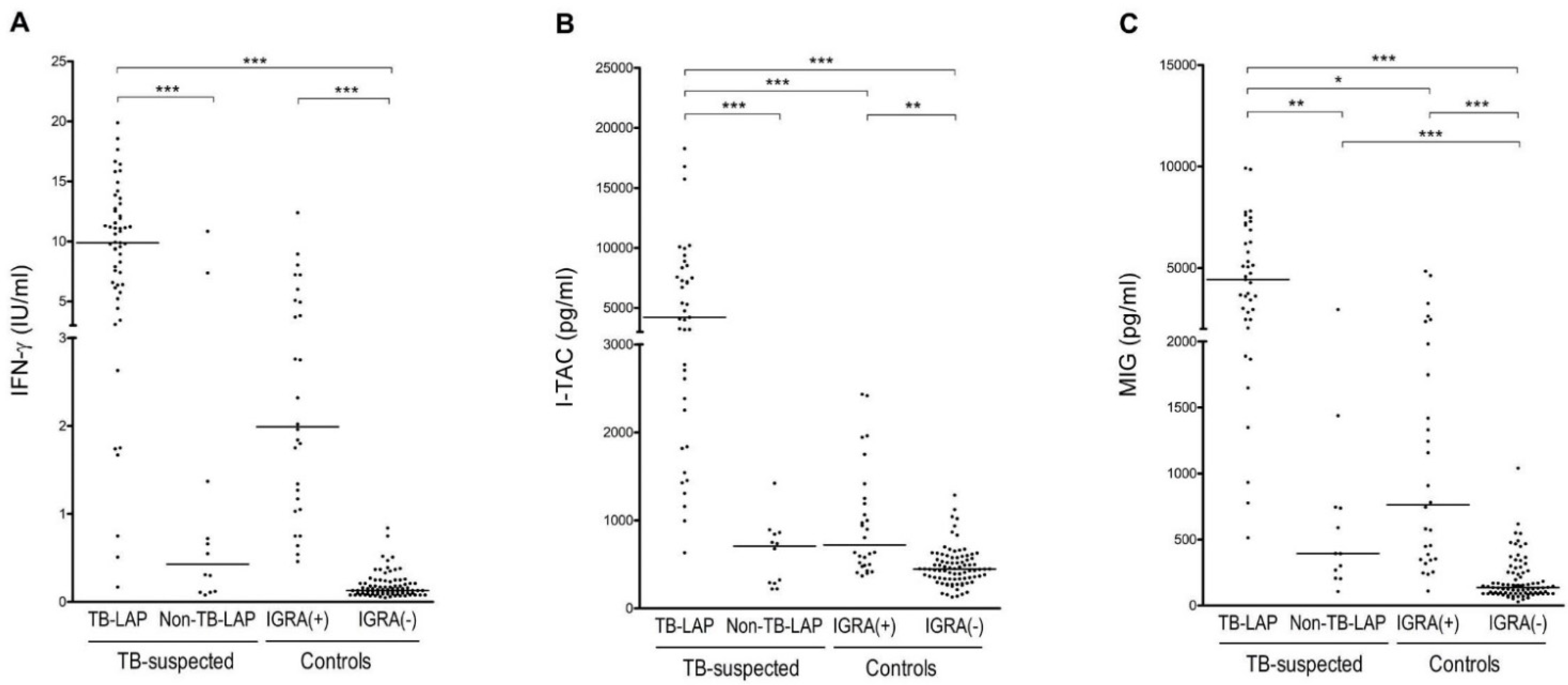
3.2. Comparison of CXCR3 Ligands and IFN-γ Levels
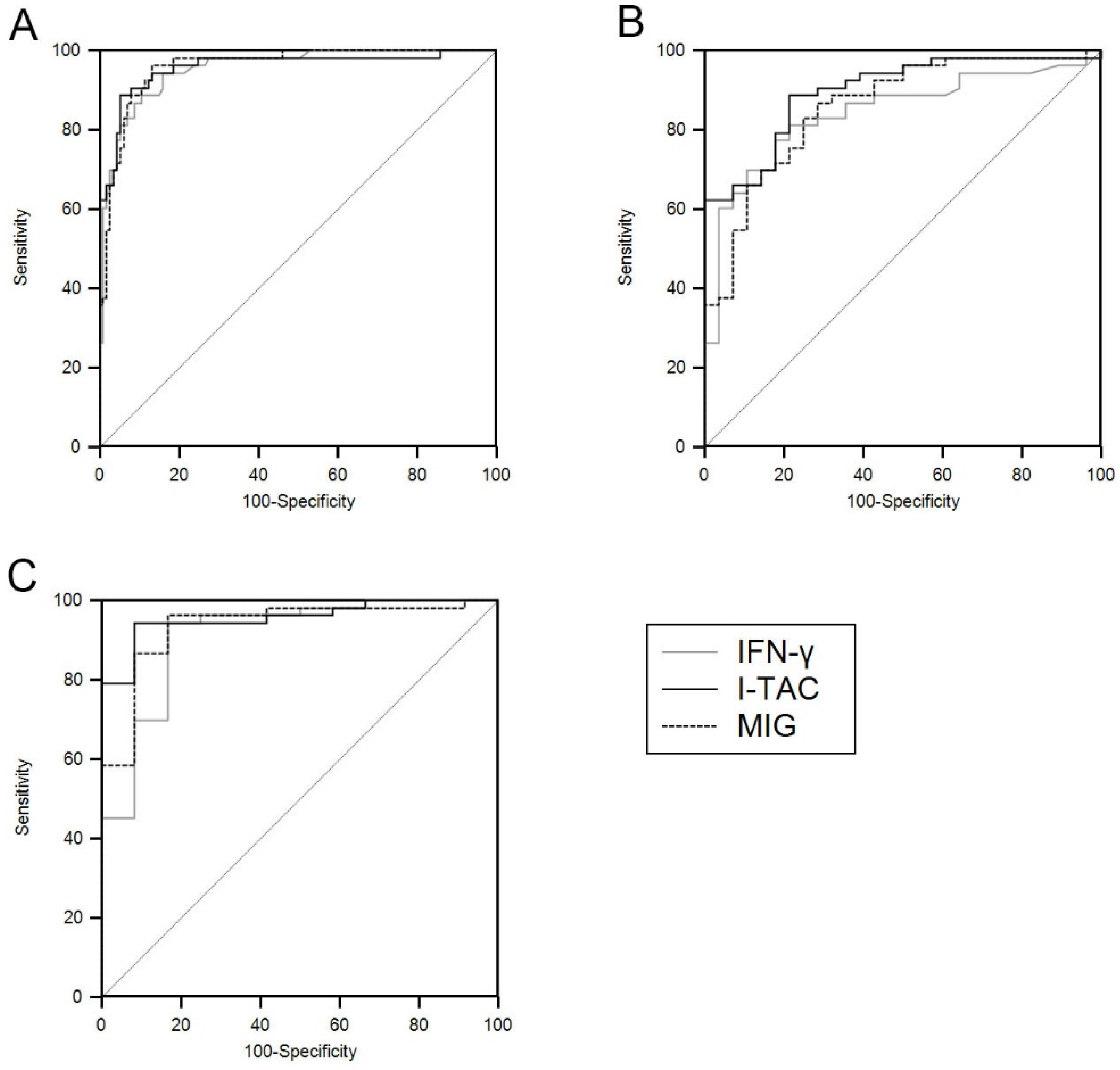
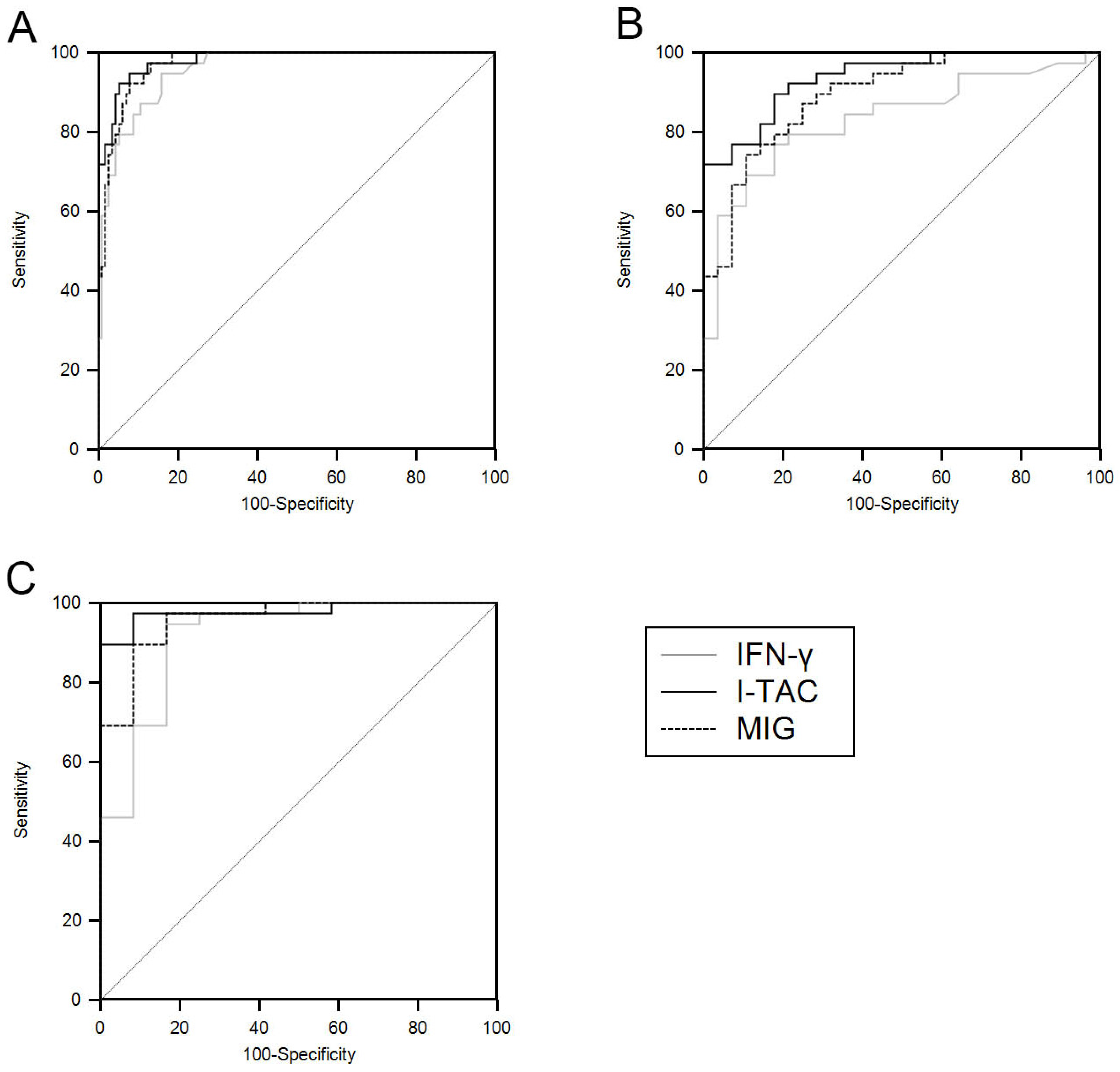
3.3. ROC Analysis
3.4. Co-Application of the Markers by Combination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Sharma, S.K.; Mohan, A. Extrapulmonary tuberculosis. Indian J. Med. Res. 2004, 120, 316–353. [Google Scholar]
- Artenstein, A.W.; Kim, J.H.; Williams, W.J.; Chung, R.C. Isolated peripheral tuberculous lymphadenitis in adults: Current clinical and diagnostic issues. Clin. Infect. Dis. 1995, 20, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.K.; Prasad, C.E.; Aparna, S.; Gokhale, S. A study of mycobacterial species causing lymphadenitis. Southeast Asian J. Trop. Med. Public Health 2008, 39, 130–135. [Google Scholar] [PubMed]
- Griffith, D.E.; Aksamit, T.; Brown-Elliott, B.A.; Catanzaro, A.; Daley, C.; Gordin, F.; Holland, S.M.; Horsburgh, R.; Huitt, G.; Iademarco, M.F.; et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 2007, 175, 367–416. [Google Scholar] [CrossRef] [PubMed]
- Deveci, H.S.; Kule, M.; Kule, Z.A.; Habesoglu, T.E. Diagnostic challenges in cervical tuberculous lymphadenitis: A review. North Clin. Istanb. 2016, 3, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Carrol, E.D.; Mankhambo, L.A.; Guiver, M.; Banda, D.L.; Group, I.P.D.S.; Denis, B.; Dove, W.; Jeffers, G.; Molyneux, E.M.; Molyneux, M.E.; et al. PCR improves diagnostic yield from lung aspiration in Malawian children with radiologically confirmed pneumonia. PLoS ONE 2011, 6, e21042. [Google Scholar] [CrossRef] [PubMed]
- Fontanilla, J.M.; Barnes, A.; von Reyn, C.F. Current diagnosis and management of peripheral tuberculous lymphadenitis. Clin. Infect. Dis. 2011, 53, 555–562. [Google Scholar] [CrossRef] [Green Version]
- Cho, O.H.; Park, K.H.; Kim, S.M.; Park, S.J.; Moon, S.M.; Chong, Y.P.; Sung, H.; Kim, M.N.; Jeong, J.Y.; Lee, S.O.; et al. Diagnostic performance of T-SPOT.TB for extrapulmonary tuberculosis according to the site of infection. J. Infect. 2011, 63, 362–369. [Google Scholar] [CrossRef]
- Jia, H.; Pan, L.; Du, B.; Sun, Q.; Wei, R.; Xing, A.; Du, F.; Sun, H.; Zhang, Z. Diagnostic performance of interferon-γ release assay for lymph node tuberculosis. Diagn. Microbiol. Infect. Dis. 2016, 85, 56–60. [Google Scholar] [CrossRef]
- Kim, K.H.; Kim, R.B.; Woo, S.H. The efficacy of the interferon-γ release assay for diagnosing cervical tuberculous lymphadenitis: A prospective controlled study. Laryngoscope 2016, 126, 378–384. [Google Scholar] [CrossRef]
- Kim, Y.K.; Uh, Y.; Lee, N.S.; Cho, M.Y.; Eom, M.; Kim, H.Y. Whole-blood interferon-gamma release assay for diagnosis of tuberculous lymphadenitis. Tohoku J. Exp. Med. 2011, 224, 189–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangaka, M.X.; Wilkinson, K.A.; Glynn, J.R.; Ling, D.; Menzies, D.; Mwansa-Kambafwile, J.; Fielding, K.; Wilkinson, R.J.; Pai, M. Predictive value of interferon-γ release assays for incident active tuberculosis: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 45–55. [Google Scholar] [CrossRef] [Green Version]
- Sester, M.; Sotgiu, G.; Lange, C.; Giehl, C.; Girardi, E.; Migliori, G.B.; Bossink, A.; Dheda, K.; Diel, R.; Dominguez, J.; et al. Interferon-γ release assays for the diagnosis of active tuberculosis: A systematic review and meta-analysis. Eur. Respir. J. 2011, 37, 100–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Y.P.; Kim, S.J.; Lew, W.J.; Lee, E.K.; Han, Y.C. The seventh nationwide tuberculosis prevalence survey in Korea, 1995. Int. J. Tuberc. Lung Dis. 1998, 2, 27–36. [Google Scholar]
- Cho, K.S. Tuberculosis control in the Republic of Korea. Epidemiol. Health 2018, 40, e2018036. [Google Scholar] [CrossRef]
- Groom, J.R.; Luster, A.D. CXCR3 in T cell function. Exp. Cell Res. 2011, 317, 620–631. [Google Scholar] [CrossRef]
- Chung, W.Y.; Lee, K.S.; Jung, Y.J.; Lee, H.L.; Kim, Y.S.; Park, J.H.; Sheen, S.S.; Park, K.J. A TB antigen-stimulated CXCR3 ligand assay for the diagnosis of active pulmonary TB. Chest 2014, 146, 283–291. [Google Scholar] [CrossRef]
- Lee, K.; Chung, W.; Jung, Y.; Kim, Y.; Park, J.; Sheen, S.; Park, K. CXCR3 ligands as clinical markers for pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 2015, 19, 191–199. [Google Scholar] [CrossRef]
- Syed Ahamed Kabeer, B.; Raman, B.; Thomas, A.; Perumal, V.; Raja, A. Role of QuantiFERON-TB gold, interferon gamma inducible protein-10 and tuberculin skin test in active tuberculosis diagnosis. PLoS ONE 2010, 5, e9051. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.Y.; Jung, G.S.; Kim, H.; Kim, Y.M.; Lee, H.J.; Cho, S.N.; Kim, S.K.; Chang, J.; Kang, Y.A. Efficacy of inducible protein 10 as a biomarker for the diagnosis of tuberculosis. Int. J. Infect. Dis. 2012, 16, e855–e859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whittaker, E.; Gordon, A.; Kampmann, B. Is IP-10 a better biomarker for active and latent tuberculosis in children than IFNgamma? PLoS ONE 2008, 3, e3901. [Google Scholar] [CrossRef] [Green Version]
- Chung, W.; Lee, K.; Jung, Y.; Kim, Y.; Park, J.; Sheen, S.; Lee, J.; Kang, D.; Park, K. Serum CXCR3 ligands as biomarkers for the diagnosis and treatment monitoring of tuberculosis. Int. J. Tuberc. Lung Dis. 2015, 19, 1476–1484. [Google Scholar] [CrossRef]
- Chung, W.Y.; Yoon, D.; Lee, K.S.; Jung, Y.J.; Kim, Y.S.; Sheen, S.S.; Park, K.J. The Usefulness of Serum CXCR3 Ligands for Evaluating the Early Treatment Response in Tuberculosis: A Longitudinal Cohort Study. Medicine 2016, 95, e3575. [Google Scholar] [CrossRef]
- Chung, W.; Jung, Y.; Lee, K.; Park, J.; Sheen, S.; Park, K. CXCR3 ligands in pleural fluid as markers for the diagnosis of tuberculous pleural effusion. Int. J. Tuberc. Lung Dis. 2017, 21, 1300–1306. [Google Scholar] [CrossRef]
- Sinha, P.; Gupta, A.; Prakash, P.; Anupurba, S.; Tripathi, R.; Srivastava, G.N. Differentiation of Mycobacterium tuberculosis complex from non-tubercular mycobacteria by nested multiplex PCR targeting IS6110, MTP40 and 32kD alpha antigen encoding gene fragments. BMC Infect. Dis. 2016, 16, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathiasen, V.D.; Andersen, P.H.; Johansen, I.S.; Lillebaek, T.; Wejse, C. Clinical features of tuberculous lymphadenitis in a low-incidence country. Int. J. Infect. Dis. 2020, 98, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Adle-Biassette, H.; Huerre, M.; Breton, G.; Ruimy, R.; Carbonnelle, A.; Trophilme, D.; Yacoub, M.; Régnier, B.; Yéni, P.; Vildé, J.L.; et al. Non tuberculous mycobacterial diseases. Ann. Pathol. 2003, 23, 216–235. [Google Scholar] [PubMed]
- You, S.H.; Kim, B.; Yang, K.S.; Kim, B.K. Cervical necrotic lymphadenopathy: A diagnostic tree analysis model based on CT and clinical findings. Eur. Radiol. 2019, 29, 5635–5645. [Google Scholar] [CrossRef]
- Gregoire, V.; Levendag, P.; Ang, K.K.; Bernier, J.; Braaksma, M.; Budach, V.; Chao, C.; Coche, E.; Cooper, J.S.; Cosnard, G.; et al. CT-based delineation of lymph node levels and related CTVs in the node-negative neck: DAHANCA, EORTC, GORTEC, NCIC, RTOG consensus guidelines. Radiother. Oncol. 2003, 69, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Korea Centers for Disease Control and Prevention. Korean Guidelines for Tuberculosis; Korea Centers for Disease Control and Prevention: Cheongju, Korea, 2011. [Google Scholar]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Schisterman, E.F.; Perkins, N.J.; Liu, A.; Bondell, H. Optimal cut-point and its corresponding Youden Index to discriminate individuals using pooled blood samples. Epidemiology 2005, 16, 73–81. [Google Scholar] [CrossRef]
- Wolf, A.J.; Desvignes, L.; Linas, B.; Banaiee, N.; Tamura, T.; Takatsu, K.; Ernst, J.D. Initiation of the adaptive immune response to Mycobacterium tuberculosis depends on antigen production in the local lymph node, not the lungs. J. Exp. Med. 2008, 205, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, T.; Leversen, N.A.; Sviland, L.; Wiker, H.G. Differential in vivo expression of mycobacterial antigens in Mycobacterium tuberculosis infected lungs and lymph node tissues. BMC Infect. Dis. 2014, 14, 535. [Google Scholar] [CrossRef] [Green Version]
- Shang, X.; Wang, L.; Liu, Y.; Liu, X.; Lv, J.; Zhou, X.; Wang, H.; Nazierhan, S.; Wang, J.; Ma, X. Diagnostic value of CXCR3 and its ligands in spinal tuberculosis. Exp. Ther. Med. 2021, 21, 73. [Google Scholar] [CrossRef]
- Sun, H.; Fan, J.; Shang, X.; Tuohetaerbaike, B.; Li, Y.; Lv, J.; Wang, Y.; Wang, L.; Wang, J.; Ma, X. Study on the relationship between CXCR3 and its ligands and tubal tuberculosis. Life Sci. 2021, 272, 119047. [Google Scholar] [CrossRef]
- Suárez, I.; Rohr, S.; Stecher, M.; Lehmann, C.; Winter, S.; Jung, N.; Priesner, V.; Berger, M.; Wyen, C.; Augustin, M.; et al. Plasma interferon-γ-inducible protein 10 (IP-10) levels correlate with disease severity and paradoxical reactions in extrapulmonary tuberculosis. Infection 2020, 1–9. [Google Scholar] [CrossRef]
- Hasan, Z.; Jamil, B.; Ashraf, M.; Islam, M.; Yusuf, M.S.; Khan, J.A.; Hussain, R. ESAT6-induced IFNgamma and CXCL9 can differentiate severity of tuberculosis. PLoS ONE 2009, 4, e5158. [Google Scholar] [CrossRef] [Green Version]
- Pai, M.; Zwerling, A.; Menzies, D. Systematic review: T-cell-based assays for the diagnosis of latent tuberculosis infection: An update. Ann. Intern. Med. 2008, 149, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.A.; Lee, H.W.; Yoon, H.I.; Cho, B.; Han, S.K.; Shim, Y.S.; Yim, J.J. Discrepancy between the tuberculin skin test and the whole-blood interferon gamma assay for the diagnosis of latent tuberculosis infection in an intermediate tuberculosis-burden country. JAMA J. Am. Med. Assoc. 2005, 293, 2756–2761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewan, P.K.; Grinsdale, J.; Kawamura, L.M. Low sensitivity of a whole-blood interferon-gamma release assay for detection of active tuberculosis. Clin. Infect. Dis. 2007, 44, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.H.; Chou, C.H.; Lai, C.C.; Huang, Y.T.; Tan, C.K.; Hsu, H.L.; Hsueh, P.R. Diagnostic performance of an enzyme-linked immunospot assay for interferon-gamma in extrapulmonary tuberculosis varies between different sites of disease. J. Infect. 2009, 59, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.A.; Chang, Y.S.; Kim, H.J.; Ahn, C.M.; Byun, M.K. Diagnostic utility of interferon-gamma release assay in extrapulmonary tuberculosis. Diagn. Microbiol. Infect. Dis. 2015, 82, 44–48. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Genes | Cycles | Primers | Sequence (5’-3’) | Size (bp) |
|---|---|---|---|---|
| IS6110 | First round | MTBC F | CGGAGACGGTGCGTAAGTGG | 984 |
| MTBC R | GATGGACCGCCAGGGCTTGC | |||
| Nested cycles | MTBC2F | CGATCGCCCCATCGACCTACT | 500 | |
| MTBC2 R | GGTCGAGTACGCCTTCTTGT | |||
| MTP40 | First round | MTB F | CGGCAACGCGCCGTCGGTGG | 396 |
| MTB R | CCCCCCACGGCACCGCCGGG | |||
| Nested cycles | MTB2 F | CGTTCGGGATGCACTGCG | 342 | |
| MTB2 R | CACCCGGCGAATTCGTCAC | |||
| 32kD α-antigen | First round | NTM F | TTCCTGACCAGCGAGCTGCCG | 506 |
| NTM R | CCCCAGTACTCCCAGCTGTGC | |||
| Nested cycles | NTM2 F | CACCCGCAGTTCATCTA | 413 | |
| NTM2 R | CGTTGTAGGCGTCCTGG |
| TB-LAP | Non-TB-LAP | Controls | ||
|---|---|---|---|---|
| IGRA (+) | IGRA (–) | |||
| Subjects | 53 | 12 | 27 | 86 |
| Age (years) | 41 (28–58) | 45 (36–59) | 42 (38–48) | 40 (34–47) |
| Male | 21 (39%) | 5 (41%) | 21 (77%) | 49 (57%) |
| Smoking history | 14(26%) | 3 (25%) | 9 (33%) | 19 (21%) |
| Alcohol abuse history | 4 | 2 | 0 | 0 |
| Recent close contact with active TB | 7 | 0 | 0 | 0 |
| IGRA results | ||||
| Positive | 46 | 5 | 27 | 0 |
| Negative | 4 | 6 | 0 | 86 |
| Indeterminate | 1 | |||
| Steroid use | 3 | 2 | 0 | 0 |
| Underlying conditions | ||||
| Diabetes mellitus | 3 | 0 | 2 | 0 |
| Malignancy | 5 | 1 | 0 | 0 |
| Immunosuppression | 1 | 1 | 0 | 0 |
| History of old TB | 6 | 1 | 2 | 0 |
| Pulmonary Tuberculosis * | |||||
| Absent (n = 40) | Present (n = 13) | p-value | |||
| IFN-γ (IU/mL) | 9.68 | (5.91–12.21) | 10.62 | (7.41–15.81) | 0.320 |
| I-TAC (pg/mL) | 3226.3 | (1397.3–7298.9) | 4751.3 | (2254.0–8349.3) | 0.272 |
| MIG (pg/mL) | 3313.2 | (1900.5–6036.7) | 4435.4 | (3012.2–6203.5) | 0.263 |
| Number of involved lymph node levels ** | |||||
| <3 (n = 27) | ≥3 (n = 26) | ||||
| IFN-γ (IU/mL) | 9.78 | (5.85–11.54) | 9.88 | (7.73–13.90) | 0.335 |
| I-TAC (pg/mL) | 3518.2 | (1543.1–8042.1) | 3260.3 | (1482.0–7343.9) | 0.923 |
| MIG (pg/mL) | 3222.3 | (1968.3–6203.5) | 4285.3 | (2268.9–6036.7) | 0.678 |
| Number of involved lymph nodes # | |||||
| <4 (n = 22) | ≥4 (n = 31) | ||||
| IFN-γ (IU/mL) | 10.01 | (5.90–11.97) | 10.62 | (6.98–12.83) | 0.795 |
| I-TAC (pg/mL) | 3276.5 | (453.5–7179.1) | 3845.3 | (1539.9–7463.0) | 0.585 |
| MIG (pg/mL) | 2986.4 | (1968.3–6203.5) | 3752.4. | (2268.9–5910.1) | 0.536 |
| AUC | 95%CI | Cutoff | Sensitivity | Specificity | |
|---|---|---|---|---|---|
| TB-LAP TB vs. all Controls | |||||
| IFN-γ | 0.955 | 0.911–0.981 | 1.34 IU/mL | 94.3 | 84.1 |
| I-TAC | 0.958 | 0.915–0.983 | 1287.2 pg/mL | 88.7 | 94.7 |
| MIG | 0.959 | 0.917–0.984 | 745.7 pg/mL | 96.2 | 86.7 |
| TB-LAP vs. IGRA-positive Controls | |||||
| IFN-γ | 0.841 | 0.743–0.913 | 5.09 IU/mL | 81.1 | 78.6 |
| I-TAC | 0.896 | 0.808–0.953 | 1250.4 pg/mL | 88.7 | 78.6 |
| MIG | 0.858 | 0.762–0.925 | 1419.6 pg/mL | 86.8 | 71.4 |
| TB-LAP vs. Non-TB-LAP | |||||
| IFN-γ | 0.912 | 0.815–0.968 | 1.37 IU/mL | 94.3 | 83.3 |
| I-TAC | 0.956 | 0.874–0.991 | 894.8 pg/mL | 94.3 | 91.7 |
| MIG | 0.936 | 0.846–0.981 | 745.6 pg/mL | 96.2 | 83.3 |
| AUC | 95%CI | Cutoff | Sensitivity | Specificity | |
|---|---|---|---|---|---|
| TB-LAP vs. all Controls | |||||
| IFN-γ | 0.958 | 0.913–0.984 | 1.34 IU/mL | 94.9 | 84.1 |
| I-TAC | 0.981 | 0.944–0.996 | 1287.2 pg/mL | 92.3 | 94.7 |
| MIG | 0.973 | 0.932–0.992 | 1330.7 pg/mL | 92.3 | 92.0 |
| TB-LAP vs. IGRA-positive Controls | |||||
| IFN-γ | 0.835 | 0.724–0.914 | 6.01 IU/mL | 76.9 | 82.1 |
| I-TAC | 0.939 | 0.852–0.982 | 1250.4 pg/mL | 89.7 | 82.1 |
| MIG | 0.895 | 0.795–0.956 | 2634.4 pg/mL | 74.4 | 89.3 |
| TB-LAP vs. Non-TB- LAP | |||||
| IFN-γ | 0.919 | 0.807–0.976 | 1.37 IU/mL | 94.9 | 83.3 |
| I-TAC | 0.979 | 0.892–0.997 | 1422.1 pg/mL | 89.7 | 100 |
| MIG | 0.959 | 0.863–0.994 | 1438.6 pg/mL | 89.7 | 91.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, W.-Y.; Lee, K.-S.; Park, J.-H.; Jung, Y.-J.; Sheen, S.-S.; Park, J.-E.; Sun, J.-S.; Ko, Y.-H.; Park, K.-J. TB Antigen-Stimulated CXCR3 Ligand Assay for Diagnosis of Tuberculous Lymphadenitis. Int. J. Environ. Res. Public Health 2021, 18, 8020. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158020
Chung W-Y, Lee K-S, Park J-H, Jung Y-J, Sheen S-S, Park J-E, Sun J-S, Ko Y-H, Park K-J. TB Antigen-Stimulated CXCR3 Ligand Assay for Diagnosis of Tuberculous Lymphadenitis. International Journal of Environmental Research and Public Health. 2021; 18(15):8020. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158020
Chicago/Turabian StyleChung, Wou-Young, Keu-Sung Lee, Joo-Hun Park, Yun-Jung Jung, Seung-Soo Sheen, Ji-Eun Park, Joo-Sung Sun, Young-Hwa Ko, and Kwang-Joo Park. 2021. "TB Antigen-Stimulated CXCR3 Ligand Assay for Diagnosis of Tuberculous Lymphadenitis" International Journal of Environmental Research and Public Health 18, no. 15: 8020. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158020