
The Relationship between Practitioners and Caregivers during a Treatment of Palliative Care: A Grounded Theory of a Challenging Collaborative Process


Abstract
:1. Introduction
Palliative Care and the Process of Dying: Beliefs, Conditions, Practices
2. Materials and Methods
- (a)
- the central unit of the network: in three networks it was a public hospital, while in the remaining it was a different healthcare provider (a not-for-profit organization coordinating the provision of palliative care in the territory)
- (b)
- the presence of professionals: all networks included medical practitioners (clinicians, physicians and nurses), while the presence of other practitioners (psychologists, social workers and so on) within the network was different
- (c)
- the settings: the networks worked in and with different modalities and settings (hospitals, hospices, home)
- (d)
- the institutional composition: each network includes different types of organization (public, private, third-sector organization), combined in different ways
- −
- Who suggested the treatment of palliative care?
- −
- What did you expect from this treatment?
- −
- How was the relation with practitioners? Did you encounter some troubles in collaborating with them?
- −
- Could you identify the benefits you, as caregivers, enjoyed by this treatment?
3. Results
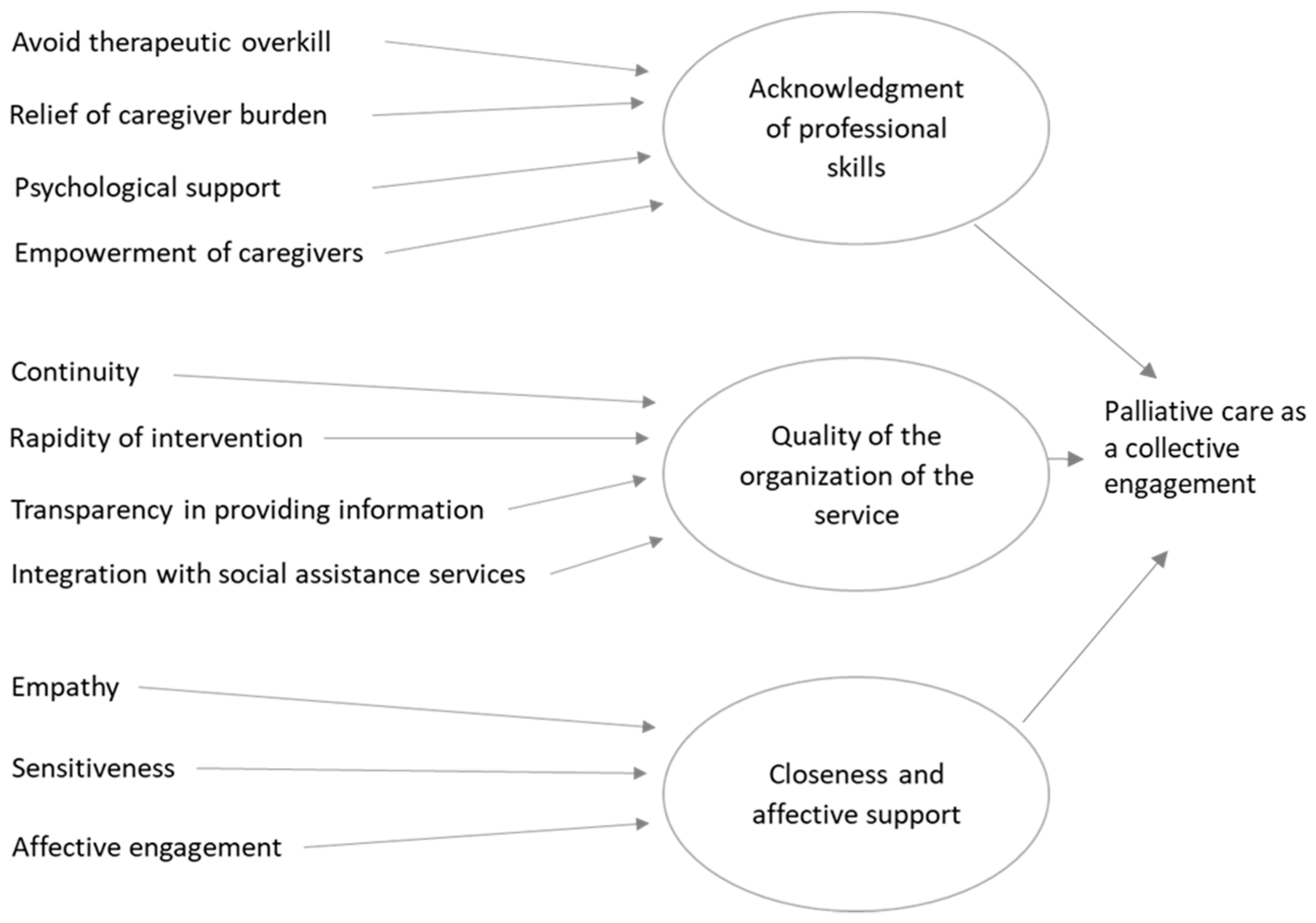
3.1. In the Eyes of the Caregivers: Palliative Care as an Effective and Collective Engagement
‘Yes, they all (the social worker, the psychologist, the oncologist, the nurses) were all truly impeccable, appropriate to the circumstance. I found great help, we found support at an emotional and organizational level. We also learned the type of disease my father had, how to interact, how to deal with it’.(P2f)
‘I have to say they were very close to me, even when my sister was sedated. They explained to me and my nephew the whole procedure, they were very, very careful also psychologically, they helped us a lot’.(Fo4)
‘Beyond the very high professionalism, which I expected, I found a great level of humanity and psychological support not only for the patient, because obviously that is fundamental, but also for us, for the family. When the situation worsened, they came to explain [to] us what were the next stages of that dramatic situation’.(Fo3)
‘I think there is a big difference with what we experienced before, because before we were accustomed to interact with doctors highly trained but very cold, who treat you at times like a number. Instead, we were supported (in the palliative care unit, we were assisted psychologically. You notice that behind this there is a preparation for the psychological support, which is priceless’.(Fo5)
‘I thought they were just coming to see, something like that, to provide drugs. No … they supported us at a psychological level, and they were always available: they did much, much more than I expected. Staying at home for two and a half months alone with a terminal patient, with a doctor who comes and goes, is not being supported, while they supported us’.(Fo4)
‘The activation of the care was very fast, it lasted around ten days. They made an interview, they provided us a report, and after a week they started’.(L6)
‘I am truly grateful to the doctors, the nurses, all of them. Whatever problem I had I phoned them, they answered me at any time and intervened in a very short time’.(Fi3)
‘When the oncologist told me: “Look, he has 6 months left, with palliative care he won’t suffer particularly.” I feared the opposite. The Palliative Care doctor told me that he wasn’t going to discuss the diagnosis but he reassured me. He told me “I’m not going to investigate, of course, but if something is going wrong call me if it is the case we intervene”. Before we had to go through every week the same sequence: going to the laboratory, make an exam, waiting for its result… I felt growing anxiety, day by day, because we didn’t know what would happen the days after, whom we would have to speak to, and so on’.(Fi3)
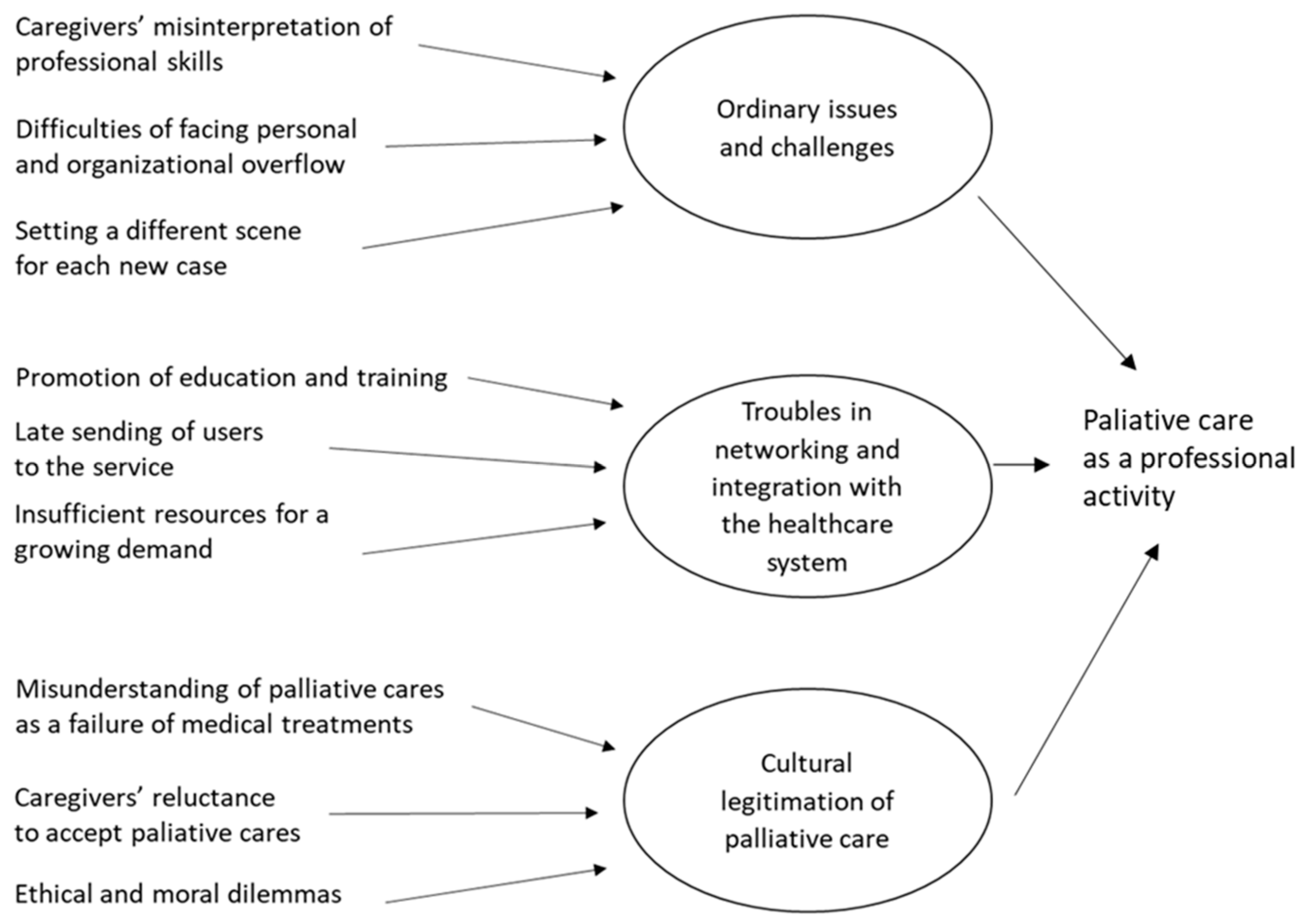
3.2. A Professional Activity, Rather Than a Mission
‘The thing that needs to be said is that the thing that bothers us the most, in the end, is being recognized as angels. That’s something that bothers the whole team a lot. (…). It bothers us a lot, because the important thing for us is that we want to be recognized as professionals. So, when so many times, caregivers ask us: “but, how do you do it?” I think this is my work’.(MDF1)
‘This is a very important thing, on which there is still a lot of work to be done: the palliative care team is not made by angels, as often it looks like, but is made by professionals. In my opinion, this would be the most important and greater recognition for all of us’.(MDF1)
‘Why do they call us angels? Angels with respect to whom? I think, in their views, we are perceived as angels when compared to what they experienced before’.(INFP1)
‘Caregivers are happy to be listened [to] … we talk, we listen, we answer them and this seems an extraordinary thing… Angels? No, it’s ordinary stuff, daily work: listening to the needs, and trying, where you can, to buffer, to help them. This is what we do’.(INFP4)
‘When patients enter the hospice, in the first interview with family members we ask them what they think about it, because there are some caregivers who say: absolutely not. After that, we try to illustrate the path, before moving to the analysis of the specific situation of the patient. Their understandings often depend on the conditions of the patient, because the evolution sometimes is so rapid that this communication needs to be very fast: so you explain in detail what it involves, what are the implications (…) because not all the families always accept the fact of not being able to have direct communication with the patient. So they struggle: “Could s/he does not wake up after? », and you have to tell «No, s/he may not wake up”’.(MDFo2)
‘A lot of elderly doctors have no idea of palliative care, whereas now, the training of General Practitioners generally provides for at least two months of study or internship. There is an inverse relation between the proximity to retirement and the propensity to palliative care’.(MDF2)
‘It is possible to say that there are two worlds. The smaller community of experts of palliative care and the broader medical community. Within the latter, it is possible to find practitioners who question the value of palliative care, institutions who do not listen to us, and hospitals who does not talk our language… But the world of palliative care is growing and enlarging. This is a good thing, because we learnt to talk to each other, to speak the same language. Unfortunately, there are still some problems with the rest of the world. We all witness this issue: those who have greater experience in this field, those who come from the world of reanimation wards or intensive care units… Everyone who joins this world realizes that this is a different world. We have a very strong need, a cultural need in the broadest sense: presenting an acceptable way of good dying, at all levels: social, institutional, in all sectors. And, of course, we cannot limit ourselves to doing what we have done so far: when a person or a family accesses our service, that is the moment when we do not only provide care, but we convey the ‘culture of good dying’.(MDP7)
‘Many times the patient already arrives almost in a coma, I do not say dying, but unfortunately, the clinical conditions are such that at home s/he can no longer be assisted (…). In these cases, the operative center of palliative care calls us and moves the patient to our facilities (…). According to me, we should succeed to create a network of home palliative care between home services, hospices and hopefully also hospital, in order to create a unit for avoiding delays’.(MDP2)
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Radbruch, L.; De Lima, L.; Knaul, F.; Wenk, R.; Ali, Z.; Bhatnaghar, S.; Blanchard, C.; Bruera, E.; Buitrago, R.; Burla, C.; et al. Redefining Palliative Care—A New Consensus-Based Definition. J. Pain Symptom Manag. 2020, 60, 754–764. [Google Scholar] [CrossRef]
- Timmermans, S. Death brokering: Constructing culturally appropriate deaths. Sociol. Health Illn. 2005, 27, 993–1013. [Google Scholar] [CrossRef]
- Baugher, J.E. Pathways Through Grief to Hospice Volunteering. Qual. Sociol. 2015, 38, 305–326. [Google Scholar] [CrossRef]
- Amblàs-Novellas, J.; Murray, A.S.; Espaulella, J.; Martori, J.C.; Oller, R.; Martínez-Muñoz, M.; Molist, N.; Blay, C.; Gomez-Batiste, X. Identifying patients with advanced chronic conditions for a progressive palliative care approach: A cross-sectional study of prognostic indicators related to end-of-life trajectories. BMJ Open 2016, 6, e012340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, D.A.; Sheppard, V.; Mangan, P.A.; Taylor, K.L.; Tallarico, M.; Adams, I.; Ingham, J. Caregiving at the End of Life: Perceptions of Health Care Quality and Quality of Life Among Patients and Caregivers. J. Pain Symptom Manag. 2006, 31, 407–420. [Google Scholar] [CrossRef] [PubMed]
- McNamara, B. Good enough death: Autonomy and choice in Australian palliative care. Soc. Sci. Med. 2004, 58, 929–938. [Google Scholar] [CrossRef]
- Meier, E.A.; Gallegos, J.V.; Thomas, L.P.M.; Depp, C.A.; Irwin, S.A.; Jeste, D.V. Defining a Good Death (Successful Dying): Literature Review and a Call for Research and Public Dialogue. Am. J. Geriatr. Psychiatry 2016, 24, 261–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krikorian, A.; Maldonado, C.; Pastrana, T. Patient’s Perspectives on the Notion of a Good Death: A Systematic Review of the Literature. J. Pain Symptom Manag. 2020, 59, 152–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cain, C.L.; McCleskey, S. Expanded definitions of the ‘good death’? Race, ethnicity and medical aid in dying. Sociol. Health Illn. 2019, 41, 1175–1191. [Google Scholar] [CrossRef]
- Hart, B.; Sainsbury, P.; Short, S. Whose dying? A sociological critique of the ‘good death’. Mortality 1998, 3, 65–77. [Google Scholar] [CrossRef]
- Walter, T. Modern Death: Taboo or not Taboo? Sociology 1991, 25, 293–310. [Google Scholar] [CrossRef]
- Cox, G.R.; Thompson, N. Death and Dying: Sociological Perspectives, 1st ed.; Routledge: New York, NY, USA, 2020. [Google Scholar]
- Long, S.O. Cultural scripts for a good death in Japan and the United States: Similarities and differences. Soc. Sci. Med. 2004, 58, 913–928. [Google Scholar] [CrossRef] [PubMed]
- Wegleitner, K.; Schuchter, P.; Prieth, S. ‘Ingredients’ of a supportive web of caring relationships at the end of life: Findings from a community research project in Austria. Sociol. Health Illn. 2018, 42, 987–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter, T. Historical and cultural variants on the good death. BMJ 2003, 327, 218–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Geest, S. Dying peacefully: Considering good death and bad death in Kwahu-Tafo, Ghana. Soc. Sci. Med. 2004, 58, 899–911. [Google Scholar] [CrossRef] [PubMed]
- Zaman, S.; Inbadas, H.; Whitelaw, A.; Clark, D. Common or multiple futures for end of life care around the world? Ideas from the ‘waiting room of history’. Soc. Sci. Med. 2017, 172, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Callaghan, K.A.; Fanning, J.B. Managing Bias in Palliative Care: Professional Hazards in Goals of Care Discussions at the End of Life. Am. J. Hosp. Palliat. Care. 2017, 35, 355–363. [Google Scholar] [CrossRef]
- Hilário, A.P.; Augusto, F.R. Pathways for a ‘Good Death’: Understanding End-of-Life Practices Through an Ethnographic Study in Two Portuguese Palliative Care Units. Sociol. Res. Online 2020. [Google Scholar] [CrossRef]
- Walshe, C.; Todd, C.; Caress, A.; Chew-Graham, C. Patterns of Access to Community Palliative Care Services: A Literature Review. J. Pain Symptom Manag. 2009, 37, 884–912. [Google Scholar] [CrossRef]
- Sallnow, L.; Schneider, N.; Murray, S.A.; Mitchell, G.; Abela, J.; Moine, S.; Firth, A.; Eynden, B.V.D.; Lynch, M.; Downing, J.; et al. Promoting palliative care in the community: Production of the primary palliative care toolkit by the European Association of Palliative Care Taskforce in primary palliative care. Palliat. Med. 2015, 29, 101–111. [Google Scholar] [CrossRef]
- Kirk, T.W.; Mahon, M.M. National Hospice and Palliative Care Organization (NHPCO) Position Statement and Commentary on the Use of Palliative Sedation in Imminently Dying Terminally Ill Patients. J. Pain Symptom Manag. 2010, 39, 914–923. [Google Scholar] [CrossRef] [PubMed]
- Bailey, S.; Hodgson, D.; Lennie, S.; Bresnen, M.; Hyde, P. Managing death: Navigating divergent logics in end-of-life care. Sociol. Health Illn. 2020, 42, 1277–1295. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, C. Acceptance of dying: A discourse analysis of palliative care literature. Soc. Sci. Med. 2012, 75, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, A.M.; Lakoma, M.D.; Block, S.D. The status of medical education in end-of-life care: A national report. J. Gen. Intern. Med. 2003, 18, 685–695. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, A.M.; Lakoma, M.D.; Billings, J.A.; Peters, A.S.; Block, S.D. Teaching and Learning End-of-Life Care: Evaluation of a Faculty Development Program in Palliative Care. Acad. Med. 2005, 80, 657–668. [Google Scholar] [CrossRef] [Green Version]
- Docherty, A.; Owens, A.; Asadi-Lari, M.; Petchey, R.; Williams, J.; Carter, Y.H. Knowledge and information needs of informal caregivers in palliative care: A qualitative systematic review. Palliat. Med. 2008, 22, 153–171. [Google Scholar] [CrossRef] [Green Version]
- Bass, D.M.; Noelker, L.S.; McCarthy, C.A. The Influence of Formal and Informal Helpers on Primary Caregivers’ Perceptions of Quality of Care. J. Appl. Gerontol. 1999, 18, 177–199. [Google Scholar] [CrossRef]
- Guberman, N.; Gagnon, E.; Côté, D.; Gilbert, C.; Thivièrge, N.; Tremblay, M. How the Trivialization of the Demands of High-Tech Care in the Home is Turning Family Members into Para-Medical Personnel. J. Fam. Issues 2005, 26, 247–272. [Google Scholar] [CrossRef]
- Levine, C.; Halper, D.; Peist, A.; Gould, D.A.; Hibbard, J.H.; Greene, J.; Becker, E.R.; Roblin, U.; Painter, M.W.; Pérez, D.J.; et al. Bridging Troubled Waters: Family Caregivers, Transitions, And Long-Term Care. Health Aff. 2010, 29, 116–124. [Google Scholar] [CrossRef]
- Stacey, C.L.; Ayers, L.L. Caught Between Love and Money: The Experiences of Paid Family Caregivers. Qual. Sociol. 2011, 35, 47–64. [Google Scholar] [CrossRef]
- Caron, C.D.; Bowers, B.J. Deciding whether to continue, share, or relinquish caregiving: Caregiver views. Qual. Health Res. 2003, 13, 1252–1271. [Google Scholar] [CrossRef]
- Ice, G.H.; Sadruddin, A.F.; Vagedes, A.; Yogo, J.; Juma, E. Stress associated with caregiving: An examination of the stress process model among Kenyan Luo elders. Soc. Sci. Med. 2012, 74, 2020–2027. [Google Scholar] [CrossRef]
- Benson, J.J.; Oliver, D.P.; Demiris, G.; Washington, K. Accounts of Family Conflict in Home Hospice Care: The Central Role of Autonomy for Informal Caregiver Resilience. J. Fam. Nurs. 2019, 25, 190–218. [Google Scholar] [CrossRef]
- Teo, I.; Baid, D.; Ozdemir, S.; Malhotra, C.; Singh, R.; Harding, R.; Malhotra, R.; Yang, M.G.; Neo, S.H.-S.; Cheung, Y.B.; et al. Family caregivers of advanced cancer patients: Self-perceived competency and meaning-making. BMJ Support. Palliat. Care 2019, 10, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Finucane, A.M.; Lugton, J.; Kennedy, C.; Spiller, J.A. The experiences of caregivers of patients with delirium, and their role in its management in palliative care settings: An integrative literature review. Psycho Oncol. 2016, 26, 291–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morita, T.; Hirai, K.; Sakaguchi, Y.; Maeyama, E.; Tsuneto, S.; Shima, Y. Measuring the quality of structure and process in end-of-life care from the bereaved family perspective. J. Pain Symptom Manag. 2004, 27, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Sisk, R.J. Caregiver burden and health promotion. Int. J. Nurs. Stud. 2000, 37, 37–43. [Google Scholar] [CrossRef]
- Yoon, S.; Kim, J.-S.; Jung, J.-G.; Kim, S.-S.; Kim, S. Modifiable factors associated with caregiver burden among family caregivers of terminally ill Korean cancer patients. Support. Care Cancer 2014, 22, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Krug, K.; Miksch, A.; Peters-Klimm, F.; Engeser, P.; Szecsenyi, J. Correlation between patient quality of life in palliative care and burden of their family caregivers: A prospective observational cohort study. BMC Palliat. Care 2016, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Bastawrous, M. Caregiver burden? A critical discussion. Int. J. Nurs. Stud. 2013, 50, 431–441. [Google Scholar] [CrossRef]
- Novak, M.; Guest, C. Application of a Multidimensional Caregiver Burden Inventory. Gerontologist 1989, 29, 798–803. [Google Scholar] [CrossRef]
- van Staa, A.L.; Visser, A.; van der Zouwe, N. Caring for caregivers: Experiences and evaluation of interventions for a palliative care team. Patient Educ. Couns. 2000, 41, 93–105. [Google Scholar] [CrossRef]
- Vedel, I.; Ghadi, V.; Lapointe, L.; Routelous, C.; Aegerter, P.; Guirimand, F. Patients’, family caregivers’, and professionals’ perspectives on quality of palliative care: A qualitative study. Palliat. Med. 2014, 28, 1128–1138. [Google Scholar] [CrossRef]
- Mota Vargas, R.; Mahtani-Chugani, V.; Solano Pallero, M.; Rivero Jiménez, B.; Cabo Domínguez, R.; Robles Alonso, V. The transformation process for palliative care professionals: The metamorphosis, a qualitative research study. Palliat. Med. 2016, 30, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Scaccabarozzi, G.; Amodio, E.; Riva, L.; Corli, O.; Maltoni, M.; Di Silvestre, G.; Turriziani, A.; Morino, P.; Pellegrini, G.; Crippa, M. Clinical Care Conditions and Needs of Palliative Care Patients from Five Italian Regions: Preliminary Data of the DEMETRA Project. Healthcare 2020, 8, 221. [Google Scholar] [CrossRef] [PubMed]
- Eisenhardt, K.M.; Graebner, M. Theory Building from Cases: Opportunities and Challenges. Acad. Manag. J. 2007, 50, 25–32. [Google Scholar] [CrossRef]
- Thornberg, R.; Charmaz, K. Grounded Theory and Theoretical Coding. In The SAGE Handbook of Qualitative Data Analysis; Publications Ltd.: London, UK, 2014; pp. 153–169. Available online: http://0-methods-sagepub-com.brum.beds.ac.uk/book/the-sage-handbook-of-qualitative-data-analysis/n11.xml (accessed on 25 May 2021).
- Attride-Stirling, J. Thematic networks: An analytic tool for qualitative research. Qual. Res. 2001, 1, 385–405. [Google Scholar] [CrossRef]
- Corbin, J.; Strauss, A. Techniques and Procedures for Developing Grounded Theory. In Basics of Qualitative Research, 3rd ed.; Publications Inc.: Thousand Oaks, CA, USA, 2008; Available online: http://0-methods-sagepub-com.brum.beds.ac.uk/book/basics-of-qualitative-research (accessed on 25 May 2021).
- Glaser, B.G.; Strauss, A.L. Awareness Contexts and Social Interaction. Am. Sociol. Rev. 1964, 29, 669. [Google Scholar] [CrossRef]
- Walsh, I.; Holton, J.A.; Bailyn, L.; Fernandez, W.; Levina, N.; Glaser, B. What Grounded Theory Is…A Critically Reflective Conversation among Scholars. Organ. Res. Methods 2015, 18, 581–599. [Google Scholar] [CrossRef] [Green Version]
- Naegele, K.D.; Goffman, E. The Presentation of Self in Everyday Life. Am. Sociol. Rev. 1956, 21, 631. [Google Scholar] [CrossRef]
- Glajchen, M.; Goehring, A. The Family Meeting in Palliative Care: Role of the Oncology Nurse. Semin. Oncol. Nurs. 2017, 33, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Nicolini, D. Practice as the Site of Knowing: Insights from the Field of Telemedicine. Organ. Sci. 2011, 22, 602–620. [Google Scholar] [CrossRef]
- Abel, J.; Kellehear, A.; Karapliagou, A. Palliative care—The new essentials. Ann. Palliat. Med. 2018, 7, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Ryan, T.; Amen, K.M.; McKeown, J. The advance care planning experiences of people with dementia, family caregivers and professionals: A synthesis of the qualitative literature. Ann. Palliat. Med. 2017, 6, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Cosby, R.; Gzik, D.; Harle, I.; Harrold, D.; Incardona, N.; Walton, T. Provider Tools for Advance Care Planning and Goals of Care Discussions: A Systematic Review. Am. J. Hosp. Palliat. Care. 2018, 35, 1123–1132. [Google Scholar] [CrossRef]
- Agarwal, R.; Epstein, A.S. Advance Care Planning and End-of-Life Decision Making for Patients with Cancer. Semin. Oncol. Nurs. 2018, 34, 316–326. [Google Scholar] [CrossRef]
- Abel, J.; Kellehear, A. Palliative care reimagined: A needed shift. BMJ Support. Palliat. Care 2016, 6, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Hazelwood, M.A.; Patterson, R.M. Scotland’s public health palliative care alliance. Ann. Palliat. Med. 2018, 7, S99–S108. [Google Scholar] [CrossRef]
- Hudson, P. Focus group interviews: A guide for palliative care researchers and clinicians. Int. J. Palliat. Nurs. 2003, 9, 202–207. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Location of Each Focus Group | Number of Participants | Duration | Collection Period |
|---|---|---|---|
| Lecco | 6 | 110 min | April 2018 |
| Firenze | 7 | 80 min | June 2018 |
| Forlì | 7 | 87 min | September 2018 |
| Palermo | 11 | 85 min | January 2019 |
| Location of Each Focus Group | Number of Participants | Practitioners’ Profession | Duration | Collection Period |
|---|---|---|---|---|
| Lecco | 6 | 4 physicians, 2 nurses | 81 min | March 2019 |
| Firenze | 8 | 6 physicians, 1 nurse, 1 psychologist | 106 min | June 2018 |
| Forlì | 4 | 2 physicians, 2 nurses | 57 min | September 2018 |
| Palermo | 13 | 7 physicians, 4 nurses, 2 social workers | 105 min | January 2019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, P.; Crippa, M.; Scaccabarozzi, G. The Relationship between Practitioners and Caregivers during a Treatment of Palliative Care: A Grounded Theory of a Challenging Collaborative Process. Int. J. Environ. Res. Public Health 2021, 18, 8081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158081
Rossi P, Crippa M, Scaccabarozzi G. The Relationship between Practitioners and Caregivers during a Treatment of Palliative Care: A Grounded Theory of a Challenging Collaborative Process. International Journal of Environmental Research and Public Health. 2021; 18(15):8081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158081
Chicago/Turabian StyleRossi, Paolo, Matteo Crippa, and Gianlorenzo Scaccabarozzi. 2021. "The Relationship between Practitioners and Caregivers during a Treatment of Palliative Care: A Grounded Theory of a Challenging Collaborative Process" International Journal of Environmental Research and Public Health 18, no. 15: 8081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158081