
Peripheral Alterations Affect the Loss in Force after a Treadmill Downhill Run


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
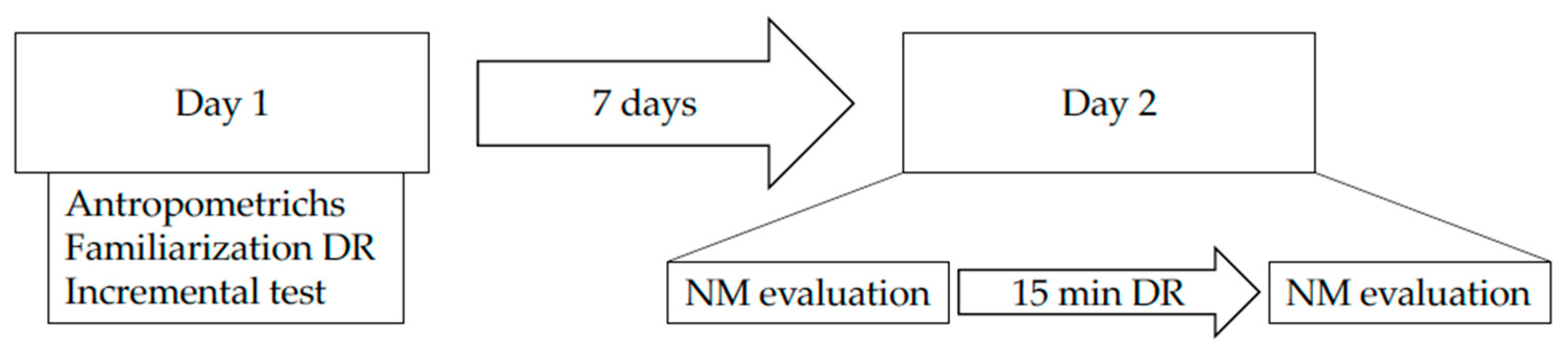
2.2. Design and Procedures
2.3. Voluntary Activation and Muscle Contractility
2.4. Electromyographic Measurements
2.5. Physiological Measurements during the Downhill Running Trial
2.6. Rate of Perceived Exertion (RPE)
2.7. Contact and Flight Time
2.8. Statistical Analysis
3. Results
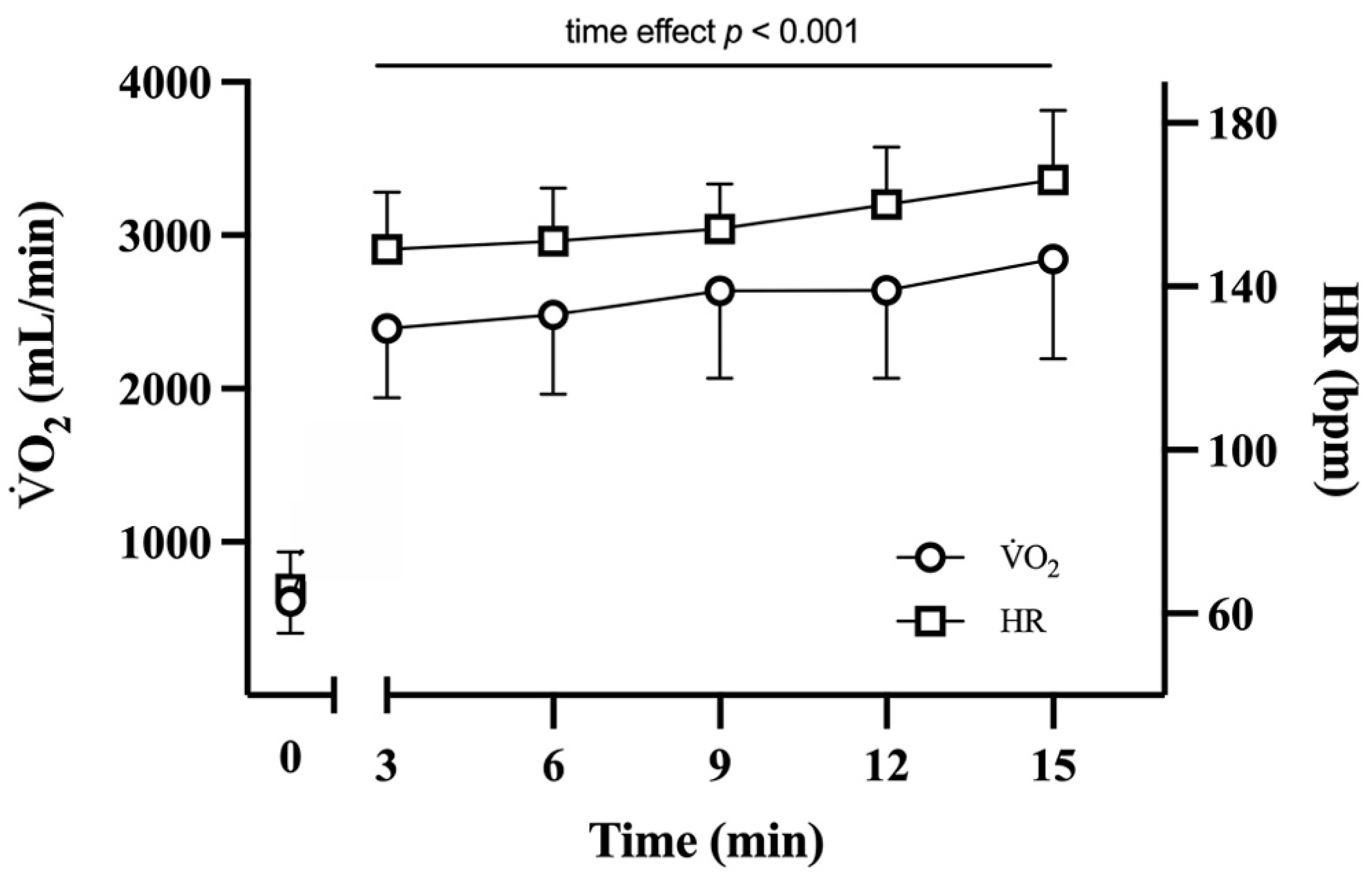
3.1. Downhill Running Trial
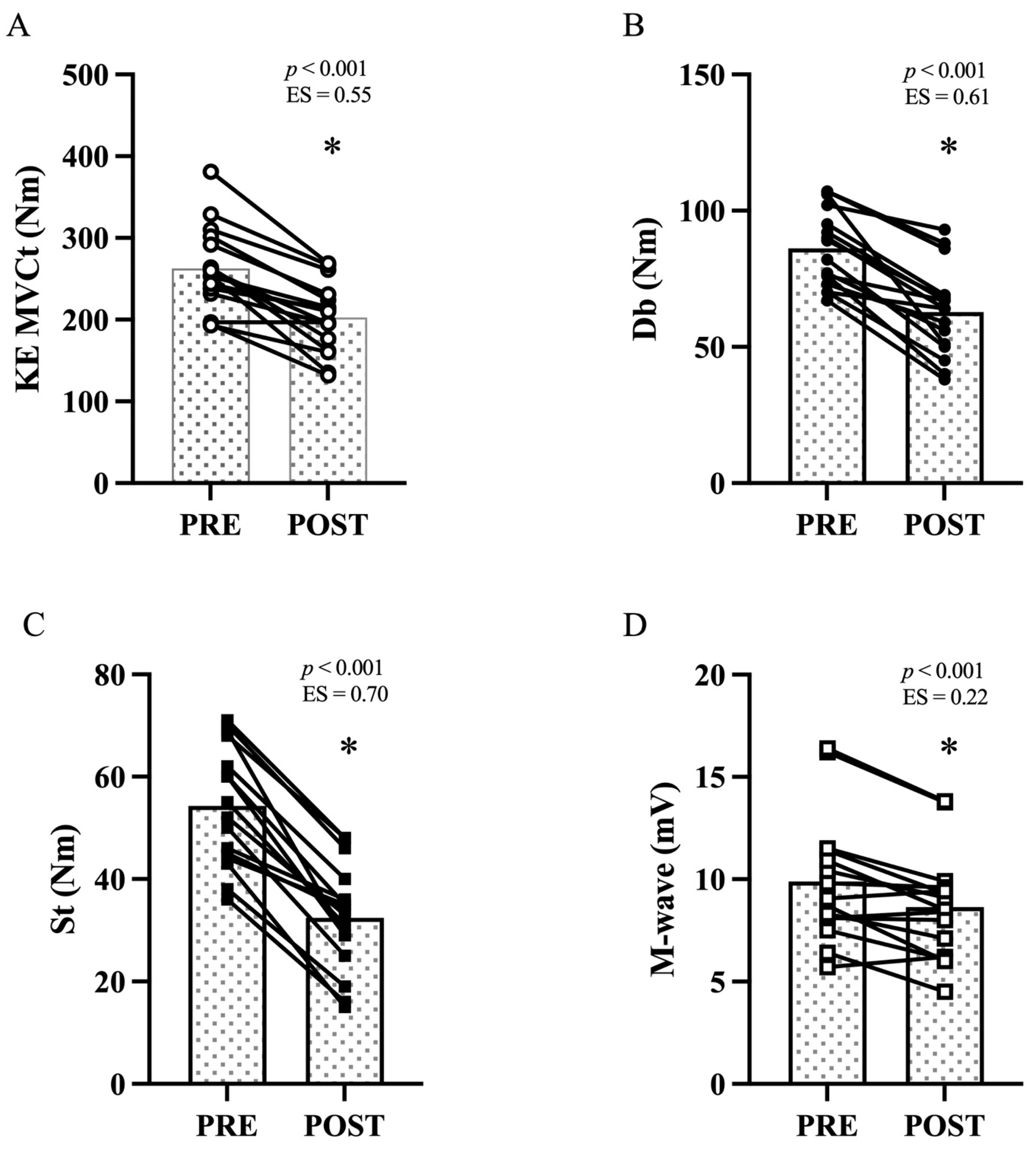
3.2. Maximal Voluntary Contraction Torque and Voluntary Activation
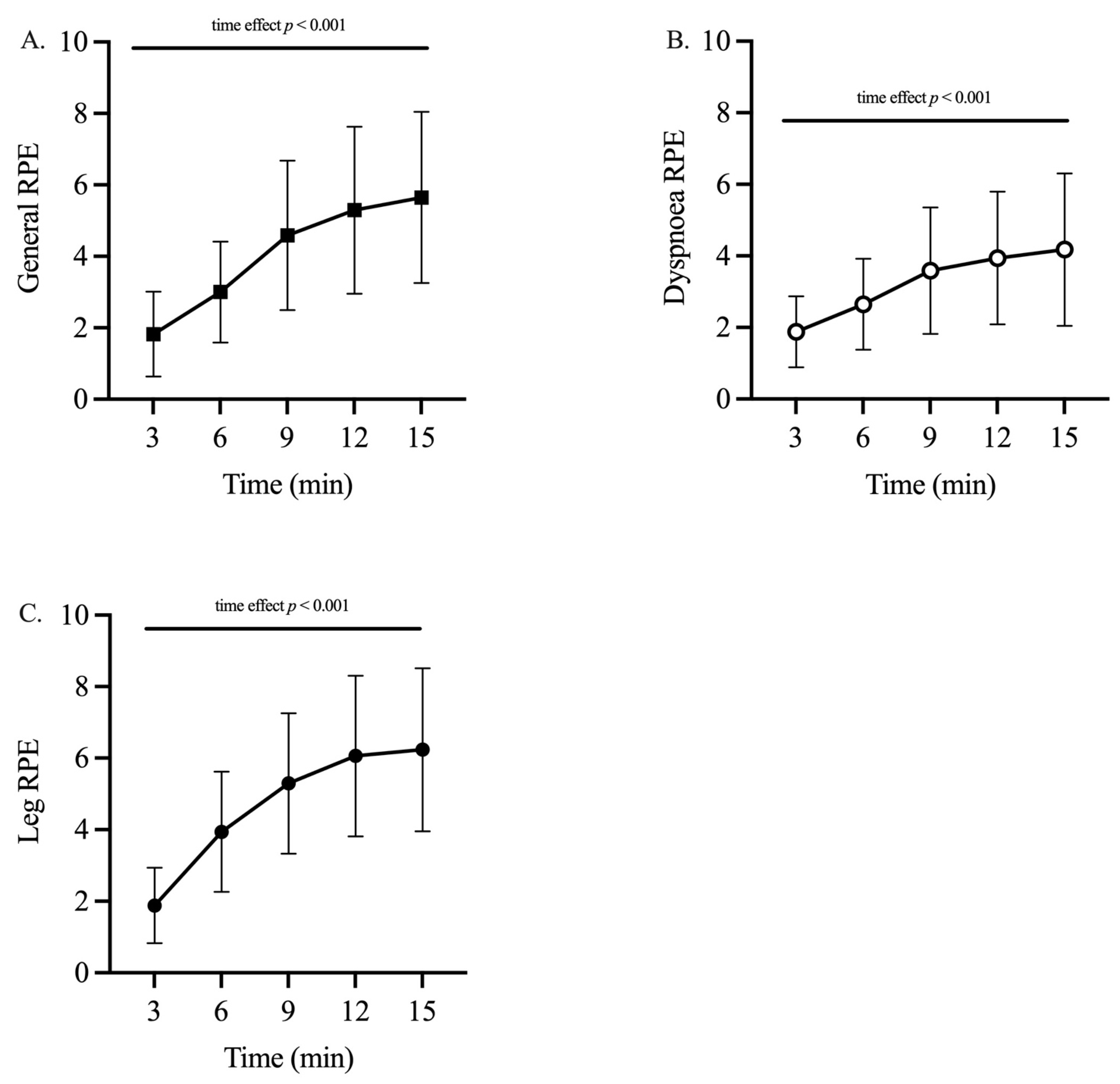
3.3. Perceived Exertion
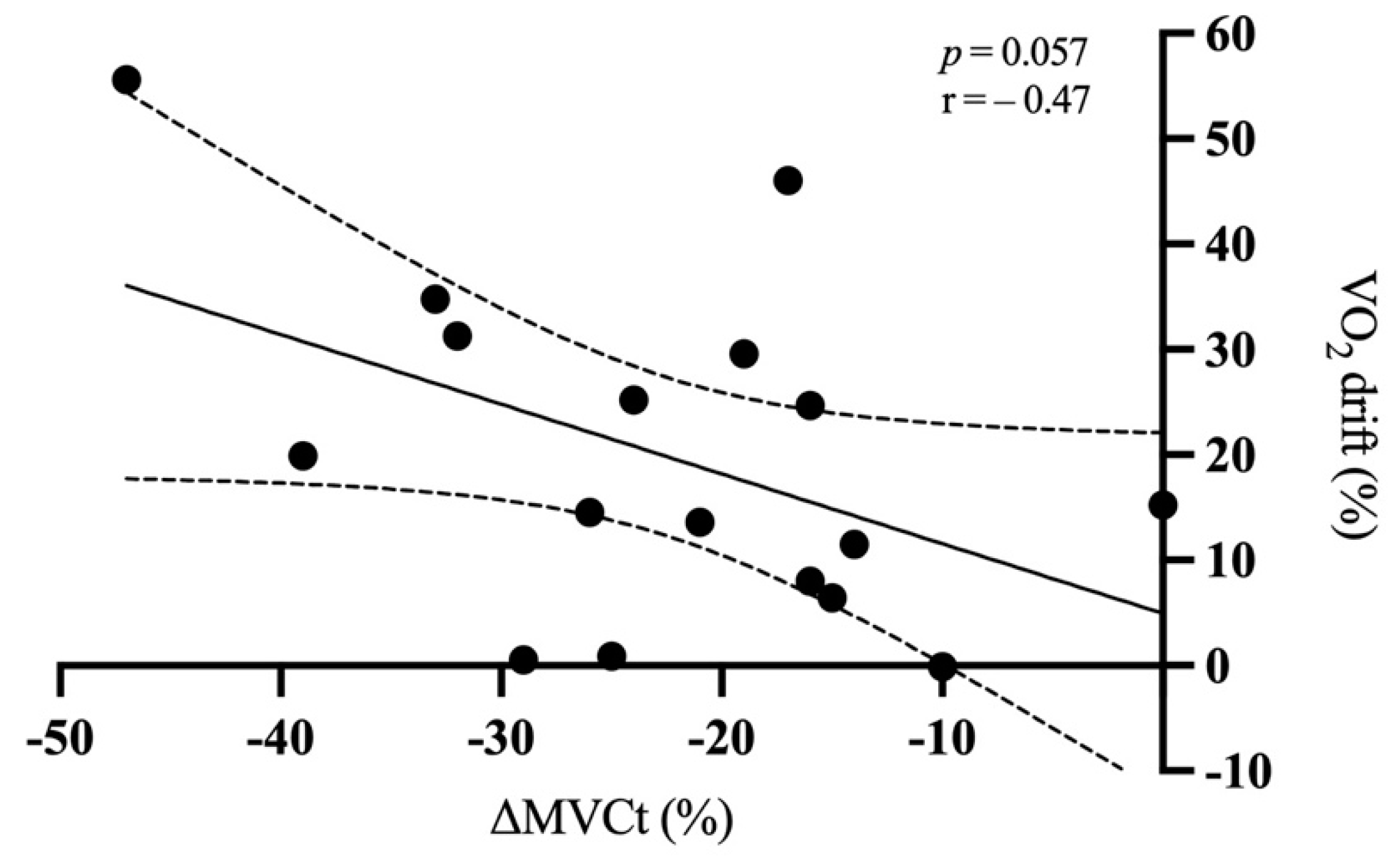
3.4. Correlation between Oxygen Drift and MVCt
3.5. Mechanical Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pokora, I.; Kempa, K.; Chrapusta, S.J.; Langfort, J. Effects of downhill and uphill exercises of equivalent submaximal intensities on selected blood cytokine levels and blood creatine kinase activity. Biol. Sport 2014, 31, 173–178. [Google Scholar] [CrossRef]
- Eston, R.G.; Mickleborough, J.; Baltzopoulos, V. Eccentric activation and muscle damage: Biomechanical and physiological considerations during downhill running. Br. J. Sports Med. 1995, 29, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malm, C.; Sjodin, T.L.; Sjoberg, B.; Lenkei, R.; Renstrom, P.; Lundberg, I.E.; Ekblom, B. Leukocytes, cytokines, growth factors and hormones in human skeletal muscle and blood after uphill or downhill running. J. Physiol. 2004, 556, 983–1000. [Google Scholar] [CrossRef]
- Giandolini, M.; Horvais, N.; Rossi, J.; Millet, G.Y.; Morin, J.B.; Samozino, P. Acute and delayed peripheral and central neuromuscular alterations induced by a short and intense downhill trail run. Scand. J. Med. Sci. Sports 2016, 26, 1321–1333. [Google Scholar] [CrossRef]
- Giandolini, M.; Horvais, N.; Rossi, J.; Millet, G.Y.; Morin, J.B.; Samozino, P. Effects of the foot strike pattern on muscle activity and neuromuscular fatigue in downhill trail running. Scand. J. Med. Sci. Sports 2017, 27, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Dick, R.W.; Cavanagh, P.R. An explanation of the upward drift in oxygen uptake during prolonged sub-maximal downhill running. Med. Sci. Sports Exerc. 1987, 19, 310–317. [Google Scholar] [CrossRef]
- Sargeant, A.J.; Dolan, P. Human muscle function following prolonged eccentric exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Pierrynowski, M.R.; Tudus, P.M.; Plyley, M.J. Effects of downhill or uphill training prior to a downhill run. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Nicol, C.; Avela, J.; Komi, P.V. The stretch-shortening cycle: A model to study naturally occurring neuromuscular fatigue. Sports Med. 2006, 36, 977–999. [Google Scholar] [CrossRef]
- Bigland-Ritchie, B.; Woods, J.J. Integrated EMG and oxygen uptake during dynamic contractions of human muscles. J. Appl. Physiol. 1974, 36, 475–479. [Google Scholar] [CrossRef]
- Bontemps, B.; Vercruyssen, F.; Gruet, M.; Louis, J. Downhill Running: What Are the Effects and How Can We Adapt? A Narrative Review. Sports Med. 2020, 50, 2083–2110. [Google Scholar] [CrossRef]
- Vollestad, N.K. Measurement of human muscle fatigue. J. Neurosci. Methods 1997, 74, 219–227. [Google Scholar] [CrossRef]
- Gandevia, S.C. Spinal and supraspinal factors in human muscle fatigue. Physiol. Rev. 2001, 81, 1725–1789. [Google Scholar] [CrossRef]
- Saugy, J.; Place, N.; Millet, G.Y.; Degache, F.; Schena, F.; Millet, G.P. Alterations of Neuromuscular Function after the World’s Most Challenging Mountain Ultra-Marathon. PLoS ONE 2013, 8, e65596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, V.; Millet, G.Y.; Martin, A.; Deley, G.; Lattier, G. Assessment of low-frequency fatigue with two methods of electrical stimulation. J. Appl. Physiol. 2004, 97, 1923–1929. [Google Scholar] [CrossRef]
- Giroux, C.; Roduit, B.; Rodriguez-Falces, J.; Duchateau, J.; Maffiuletti, N.A.; Place, N. Short vs. long pulses for testing knee extensor neuromuscular properties: Does it matter? Eur. J. Appl. Physiol. 2018, 118, 361–369. [Google Scholar] [CrossRef]
- Lemire, M.; Hureau, T.J.; Remetter, R.; Geny, B.; Kouassi, B.Y.L.; Lonsdorfer, E.; Isner-Horobeti, M.E.; Favret, F.; Dufour, S.P. Trail Runners Cannot Reach V[Combining Dot above]O2max during a Maximal Incremental Downhill Test. Med. Sci. Sports Exerc. 2020, 52, 1135–1143. [Google Scholar] [CrossRef]
- Rejc, E.; Lazzer, S.; Antonutto, G.; Isola, M.; di Prampero, P.E. Bilateral deficit and EMG activity during explosive lower limb contractions against different overloads. Eur. J. Appl. Physiol. 2010, 108, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Merton, P.A. Voluntary strength and fatigue. J. Physiol. 1954, 123, 553–564. [Google Scholar] [CrossRef]
- Millet, G.Y.; Tomazin, K.; Verges, S.; Vincent, C.; Bonnefoy, R.; Boisson, R.C.; Gergele, L.; Feasson, L.; Martin, V. Neuromuscular consequences of an extreme mountain ultra-marathon. PLoS ONE 2011, 6, e17059. [Google Scholar] [CrossRef] [Green Version]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Borg, G.A. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Giovanelli, N.; Taboga, P.; Rejc, E.; Simunic, B.; Antonutto, G.; Lazzer, S. Effects of an Uphill Marathon on Running Mechanics and Lower Limb Muscles Fatigue. Int. J. Sports Physiol. Perform. 2016, 11, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Motulsky, H.J.; Brown, R.E. Detecting outliers when fitting data with nonlinear regression—A new method based on robust nonlinear regression and the false discovery rate. BMC Bioinform. 2006, 7, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vernillo, G.; Aguiar, M.; Savoldelli, A.; Martinez, A.; Giandolini, M.; Horvais, N.; Edwards, W.B.; Millet, G.Y. Regular changes in foot strike pattern during prolonged downhill running do not influence neuromuscular, energetics, or biomechanical parameters. Eur. J. Sport Sci. 2020, 20, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Baumann, C.W.; Green, M.S.; Doyle, J.A.; Rupp, J.C.; Ingalls, C.P.; Corona, B.T. Muscle injury after low-intensity downhill running reduces running economy. J. Strength Cond. Res. 2014, 28, 1212–1218. [Google Scholar] [CrossRef]
- Newham, D.J.; Jones, D.A.; Ghosh, G.; Aurora, P. Muscle fatigue and pain after eccentric contractions at long and short length. Clin. Sci. 1988, 74, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Braun, W.A.; Dutto, D.J. The effects of a single bout of downhill running and ensuing delayed onset of muscle soreness on running economy performed 48 h later. Eur. J. Appl. Physiol. 2003, 90, 29–34. [Google Scholar] [CrossRef]
- Bjorklund, G.; Swaren, M.; Born, D.P.; Stoggl, T. Biomechanical Adaptations and Performance Indicators in Short Trail Running. Front. Physiol. 2019, 10, 506. [Google Scholar] [CrossRef]
- Millet, G.Y.; Martin, V.; Lattier, G.; Ballay, Y. Mechanisms contributing to knee extensor strength loss after prolonged running exercise. J. Appl. Physiol. 2003, 94, 193–198. [Google Scholar] [CrossRef]
- Piitulainen, H.; Bottas, R.; Komi, P.; Linnamo, V.; Avela, J. Impaired action potential conduction at high force levels after eccentric exercise. J. Electromyogr. Kinesiol. 2010, 20, 879–887. [Google Scholar] [CrossRef]
- Place, N.; Yamada, T.; Bruton, J.D.; Westerblad, H. Muscle fatigue: From observations in humans to underlying mechanisms studied in intact single muscle fibres. Eur. J. Appl. Physiol. 2010, 110, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.; Twist, C.; Eston, R. Neuromuscular function after exercise-induced muscle damage: Theoretical and applied implications. Sports Med. 2004, 34, 49–69. [Google Scholar] [CrossRef] [PubMed]
- Westerlind, K.C.; Byrnes, W.C.; Mazzeo, R.S. A comparison of the oxygen drift in downhill vs. level running. J. Appl. Physiol. 1992, 72, 796–800. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giovanelli, N.; Floreani, M.; Vaccari, F.; Lazzer, S. Peripheral Alterations Affect the Loss in Force after a Treadmill Downhill Run. Int. J. Environ. Res. Public Health 2021, 18, 8135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158135
Giovanelli N, Floreani M, Vaccari F, Lazzer S. Peripheral Alterations Affect the Loss in Force after a Treadmill Downhill Run. International Journal of Environmental Research and Public Health. 2021; 18(15):8135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158135
Chicago/Turabian StyleGiovanelli, Nicola, Mirco Floreani, Filippo Vaccari, and Stefano Lazzer. 2021. "Peripheral Alterations Affect the Loss in Force after a Treadmill Downhill Run" International Journal of Environmental Research and Public Health 18, no. 15: 8135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158135