Cerebellar Degeneration in Epilepsy: A Systematic Review



Abstract
:1. Introduction
2. Methodology
2.1. Protocol
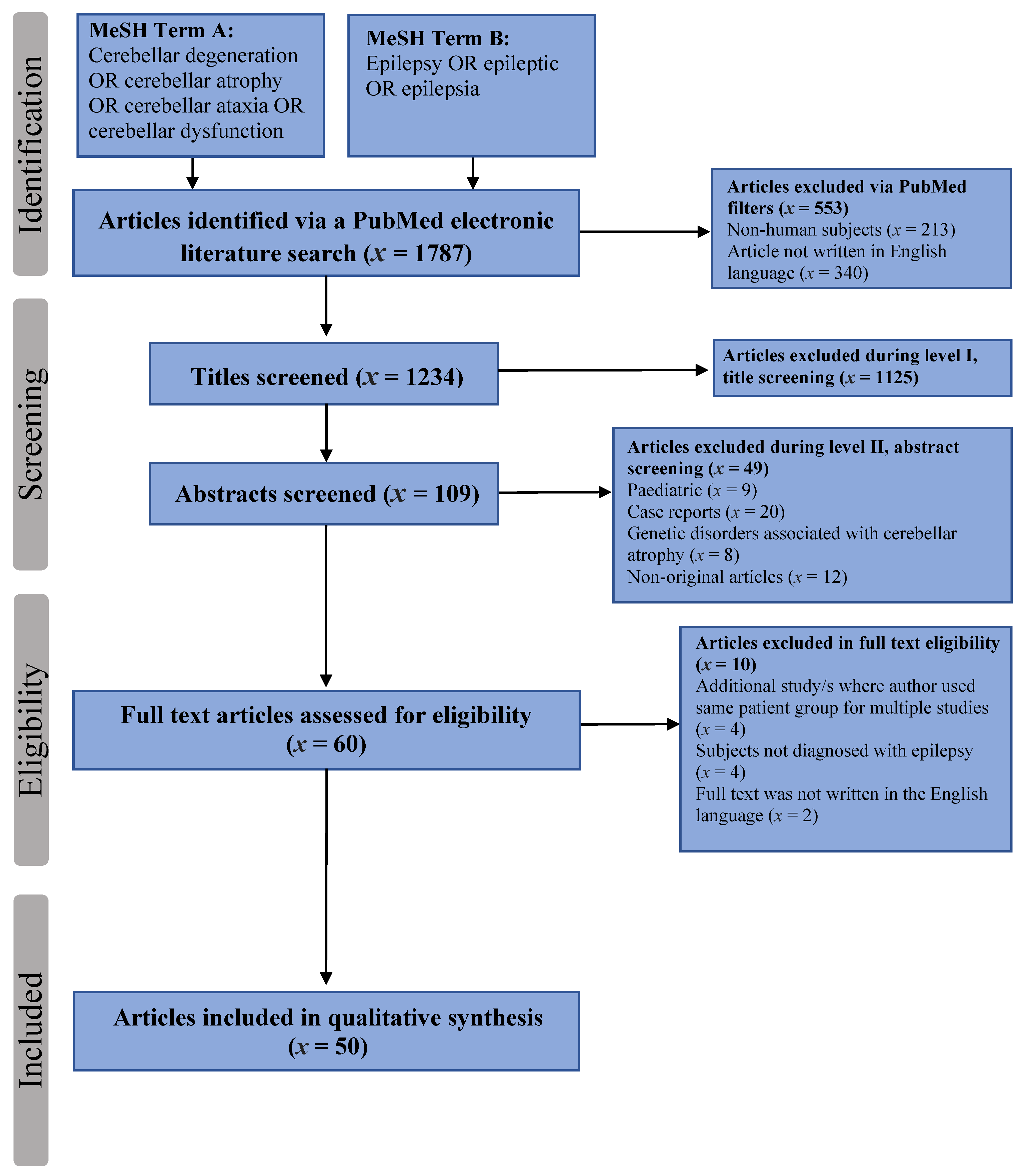
2.2. Search Strategy
2.3. Inclusion Criteria
- All recruited in the studies were human subjects
- All patients were diagnosed with epilepsy
- All studies discussed cerebellar degeneration in relation to epilepsy and/or anti-epileptic drugs
- All studies investigated clinical and/or neuroimaging and/or pathological findings of cerebellar degeneration in patients with epilepsy
- The full publication text was written in English
2.4. Exclusion Criteria
- Animal studies
- Paediatric studies
- Case-reports
- Studies reporting patients with encephalopathy or status epilepticus or post stroke epilepsy
- Studies detailing cerebellar degeneration in epilepsy caused by another disorder, e.g., alcohol related, autoimmune, mitochondrial
- Studies where the patient group had been used in multiple studies
2.5. Data Extraction Process
- Study details (author, year of publication, study design, location of study); population demographics (size, age, and gender)
- Epilepsy characteristics (classification of epilepsy; seizure or epilepsy type, duration of epilepsy, seizure control); anti-epileptic drug (AED) therapy (monotherapy or polytherapy, type of AED at study onset, and duration of treatment).
- Clinical characteristics of cerebellar degeneration included gait and/or limb ataxia, tremor, nystagmus, and clinical signs of peripheral neuropathy
- Neuroimaging characteristics included whether cerebellar atrophy was “present” or “absent”; if present whether this was single or bilateral cerebellar hemispheric atrophy, vermian atrophy, or whole cerebellar atrophy); and any focal brain structural changes
- Neuropathological characteristics on post-mortem included microscopic and macroscopic descriptions of the cerebellum, and when available cause of death.
2.6. Synthesis of Results
2.7. Assessment of Bias
2.8. Ethical Guidelines
3. Results
3.1. Selected Studies
3.2. Epilepsy Characteristics
3.3. Antiepileptic Medication History
3.4. Prevalence of Cerebellar Degeneration
3.4.1. Clinical Characteristics
Clinical vs. Imaging Characteristics
Clinical vs. Epilepsy and AED Characteristics
3.4.2. Neuroimaging Characteristics
Radiological Techniques and Sequences
Imaging Characteristics—Brain Atrophy
Imaging Characteristics—Hippocampal Atrophy
Brain Atrophy vs. Type of Epilepsy vs. AED
Imaging Characteristics—Cerebellar Atrophy
3.4.3. Neuropathological Characteristics
4. Discussion
4.1. TLE and Cerebellar Degeneration
4.2. Pharmaco-Resistance and Cerebellar Degeneration
4.3. Phenytoin and Cerebellar Degeneration
4.4. Clinical Characteristics of Cerebellar Degeneration
5. Limitations
6. Future Studies
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Epilepsy. Available online: https://www.who.int/news-room/fact-sheets/detail/epilepsy (accessed on 20 July 2019).
- National Institute for Care and Health Excellence (NICE). Epilepsies: Diagnosis and Management. Available online: https://www.nice.org.uk/guidance/cg137/chapter/Introduction (accessed on 21 July 2019).
- Stafstrom, C.E.; Carmant, L. Seizures and epilepsy: An overview for neuroscientists. Cold Spring Harb. Perspect Med. 2015, 5, a022426. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.S.; Cross, J.H.; French, J.A.; Higurashi, N.; Hirsch, E.; Jansen, F.E.; Lagae, L.; Moshe, S.L.; Peltola, J.; Roulet Perez, E.; et al. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 522–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squire, L.R. Fundamental Neuroscience, 4th ed.; Elsevier: Amsterdam, The Netherlands; Academic Press: Boston, MA, USA, 2013. [Google Scholar]
- van Gaalen, J.; Kerstens, F.G.; Maas, R.P.; Harmark, L.; van de Warrenburg, B.P. Drug-induced cerebellar ataxia: A systematic review. CNS Drugs 2014, 28, 1139–1153. [Google Scholar] [CrossRef] [PubMed]
- Buckner, R.L. The cerebellum and cognitive function: 25 years of insight from anatomy and neuroimaging. Neuron 2013, 80, 807–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strick, P.L.; Dum, R.P.; Fiez, J.A. Cerebellum and nonmotor function. Annu. Rev. Neurosci. 2009, 32, 413–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murdoch, B.E. The cerebellum and language: Historical perspective and review. Cortex 2010, 46, 858–868. [Google Scholar] [CrossRef]
- Schmahmann, J.D. The role of the cerebellum in cognition and emotion: Personal reflections since 1982 on the dysmetria of thought hypothesis, and its historical evolution from theory to therapy. Neuropsychol. Rev. 2010, 20, 236–260. [Google Scholar] [CrossRef]
- D’Angelo, E.; Casali, S. Seeking a unified framework for cerebellar function and dysfunction: From circuit operations to cognition. Front. Neural Circuits 2012, 6, 116. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Neurological Disorders and Stroke (NIH). Cerebellar Degeneration Information Page: What Research is Being Done? Available online: https://www.ninds.nih.gov/disorders/All-Disorders/Cerebellar-Degeneration-Information-Page (accessed on 18 September 2019).
- Khemani, P. Overview of adult onset cerebellar ataxia. Pract. Neurol. 2013, 4, 38–40. [Google Scholar]
- Sarva, H.; Shanker, V.L. Treatment Options in Degenerative Cerebellar Ataxia: A Systematic Review. Mov. Disord Clin. Pract. 2014, 1, 291–298. [Google Scholar] [CrossRef]
- Oscar-Berman, M.; Marinkovic, K. Alcoholism and the brain: An overview. Alcohol. Res. Health 2003, 27, 125–133. [Google Scholar]
- Nussinovitch, M.; Prais, D.; Volovitz, B.; Shapiro, R.; Amir, J. Post-infectious acute cerebellar ataxia in children. Clin. Pediatr. (Phila) 2003, 42, 581–584. [Google Scholar] [CrossRef]
- Darnell, R.B.; Posner, J.B. Paraneoplastic syndromes involving the nervous system. N. Engl. J. Med. 2003, 349, 1543–1554. [Google Scholar] [CrossRef] [PubMed]
- Poretti, A.; Boltshauser, E. Terminology in morphological anomalies of the cerebellum does matter. Cerebellum Ataxias 2015, 2, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcian, V.; Filip, P.; Bares, M.; Brazdil, M. Cerebellar Dysfunction and Ataxia in Patients with Epilepsy: Coincidence, Consequence, or Cause? Tremor Other Hyperkinet. Mov. 2016, 6, 376. [Google Scholar] [CrossRef]
- Ney, G.C.; Lantos, G.; Barr, W.B.; Schaul, N. Cerebellar atrophy in patients with long-term phenytoin exposure and epilepsy. Arch. Neurol. 1994, 51, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Specht, U.; May, T.; Schulz, R.; Rohde, M.; Ebner, A.; Schmidt, R.C.; Schutz, M.; Wolf, P. Cerebellar atrophy and prognosis after temporal lobe resection. J. Neurol. Neurosurg. Psychiatry 1997, 62, 501–506. [Google Scholar] [CrossRef] [Green Version]
- Crooks, R.; Mitchell, T.; Thom, M. Patterns of cerebellar atrophy in patients with chronic epilepsy: A quantitative neuropathological study. Epilepsy Res. 2000, 41, 63–73. [Google Scholar] [CrossRef]
- Dow, R.S.; Fernandez-Guardiola, A.; Manni, E. The influence of the cerebellum on experimental epilepsy. Electroencephalogr. Clin. Neurophysiol. 1962, 14, 383–398. [Google Scholar] [CrossRef]
- Bonilha, L.; Elm, J.J.; Edwards, J.C.; Morgan, P.S.; Hicks, C.; Lozar, C.; Rumboldt, Z.; Roberts, D.R.; Rorden, C.; Eckert, M.A. How common is brain atrophy in patients with medial temporal lobe epilepsy? Epilepsia 2010, 51, 1774–1779. [Google Scholar] [CrossRef]
- Keller, S.S.; Mackay, C.E.; Barrick, T.R.; Wieshmann, U.C.; Howard, M.A.; Roberts, N. Voxel-based morphometric comparison of hippocampal and extrahippocampal abnormalities in patients with left and right hippocampal atrophy. Neuroimage 2002, 16, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.S.; Lemieux, L.; Bell, G.S.; Bartlett, P.A.; Sander, J.W.; Sisodiya, S.M.; Shorvon, S.D.; Duncan, J.S. A longitudinal quantitative MRI study of community-based patients with chronic epilepsy and newly diagnosed seizures: Methodology and preliminary findings. Neuroimage 2001, 14, 231–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.S.; Lemieux, L.; Bell, G.S.; Sisodiya, S.M.; Shorvon, S.D.; Sander, J.W.; Duncan, J.S. A longitudinal study of brain morphometrics using quantitative magnetic resonance imaging and difference image analysis. Neuroimage 2003, 20, 22–33. [Google Scholar] [CrossRef]
- Liu, R.S.; Lemieux, L.; Bell, G.S.; Sisodiya, S.M.; Bartlett, P.A.; Shorvon, S.D.; Sander, J.W.; Duncan, J.S. Cerebral damage in epilepsy: A population-based longitudinal quantitative MRI study. Epilepsia 2005, 46, 1482–1494. [Google Scholar] [CrossRef] [PubMed]
- Iivanainen, M.; Viukari, M.; Helle, E.P. Cerebellar atrophy in phenytoin-treated mentally retarded epileptics. Epilepsia 1977, 18, 375–386. [Google Scholar] [CrossRef]
- Salcman, M.; Defendini, R.; Correll, J.; Gilman, S. Neuropathological changes in cerebellar biopsies of epileptic patients. Ann. Neurol. 1978, 3, 10–19. [Google Scholar] [CrossRef]
- Nakazawa, Y.; Ohkawa, T. Study of the side effects of long-term anticonvulsant treatment. Folia Psychiatr. Neurol. Jpn. 1980, 34, 271–275. [Google Scholar] [CrossRef]
- Botez, M.I.; Attig, E.; Vezina, J.L. Cerebellar atrophy in epileptic patients. Can. J. Neurol. Sci 1988, 15, 299–303. [Google Scholar] [CrossRef] [Green Version]
- Benvenuti, F.; Bandinelli, S.; Mencarelli, M.A.; Lunardelli, M.L.; Campostrini, R.; Zaccara, G.; Pantaleo, T. Alterations of ballistic movements in epileptic patients with phenytoin intoxication. Epilepsia 1992, 33, 376–388. [Google Scholar] [CrossRef]
- Jibiki, I.; Kido, H.; Matsuda, H.; Yamaguchi, N.; Hisada, K. Probable cerebellar abnormality on 123I-IMP SPECT scans in epileptic patients with long-term high-dose phenytoin therapy. Based on observation of multiple cases. Acta Neurol. 1993, 15, 16–24. [Google Scholar]
- Luef, G.; Chemelli, A.; Birbamer, G.; Aichner, F.; Bauer, G. Phenytoin overdosage and cerebellar atrophy in epileptic patients: Clinical and MRI findings. Eur. Neurol. 1994, 34 (Suppl. 1), 79–81. [Google Scholar] [CrossRef]
- Specht, U.; Rohde, M.; May, T.; Schmidt, R.C.; Meencke, H.J.; Wolf, P. Cerebellar atrophy does not increase susceptibility to carbamazepine toxicity. Acta Neurol. Scand. 1994, 89, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Luef, G.; Burtscher, J.; Kremser, C.; Birbamer, G.; Aichner, F.; Bauer, G.; Felber, S. Magnetic resonance volumetry of the cerebellum in epileptic patients after phenytoin overdosages. Eur. Neurol. 1996, 36, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Misra, U.K.; Kalita, J.; Babu, G.N.; Dwivedi, K.D. Clinical psychometry and P3 in patients on phenytoin monotherapy. Electromyogr. Clin. Neurophysiol. 1997, 37, 123–127. [Google Scholar] [PubMed]
- Specht, U.; May, T.W.; Rohde, M.; Wagner, V.; Schmidt, R.C.; Schutz, M.; Wolf, P. Cerebellar atrophy decreases the threshold of carbamazepine toxicity in patients with chronic focal epilepsy. Arch. Neurol 1997, 54, 427–431. [Google Scholar] [CrossRef]
- Recio, M.V.; Gallagher, M.J.; McLean, M.J.; Abou-Khalil, B. Clinical features of epilepsy in patients with cerebellar structural abnormalities in a referral center. Epilepsy Res. 2007, 76, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Shanmugarajah, P.D.; Hoggard, N.; Aeschlimann, D.P.; Aeschlimann, P.C.; Dennis, G.J.; Howell, S.J.; Reuber, M.; Grunewald, R.A.; Hadjivassiliou, M. Phenytoin-related ataxia in patients with epilepsy: Clinical and radiological characteristics. Seizure 2018, 56, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Ballenger, C.E., 3rd; Lucke, J.F.; King, D.W.; El Gammal, T.; Brooks, B.S.; Green, J.B. Cerebellar atrophy in epilepsy and headache: Lack of relationship to phenytoin. Neurology 1982, 32, 910–912. [Google Scholar] [CrossRef]
- Theodore, W.H.; Fishbein, D.; Dietz, M.; Baldwin, P. Complex partial seizures: Cerebellar metabolism. Epilepsia 1987, 28, 319–323. [Google Scholar] [CrossRef]
- Bekkelund, S.I.; Pierre-Jerome, C.; Mellgren, S.I. Quantitative cerebral MRI in epileptic patients. Acta Neurol. Scand. 1996, 94, 378–382. [Google Scholar] [CrossRef]
- Savic, I.; Altshuler, L.; Passaro, E.; Baxter, L.; Engel, J., Jr. Localized cerebellar hypometabolism in patients with complex partial seizures. Epilepsia 1996, 37, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Savic, I.; Thorell, J.O. Localized cerebellar reductions in benzodiazepine receptor density in human partial epilepsy. Arch. Neurol 1996, 53, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Blum, D.E.; Ehsan, T.; Dungan, D.; Karis, J.P.; Fisher, R.S. Bilateral temporal hypometabolism in epilepsy. Epilepsia 1998, 39, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Bohnen, N.I.; O’Brien, T.J.; Mullan, B.P.; So, E.L. Cerebellar changes in partial seizures: Clinical correlations of quantitative SPECT and MRI analysis. Epilepsia 1998, 39, 640–650. [Google Scholar] [CrossRef] [Green Version]
- Sandok, E.K.; O’Brien, T.J.; Jack, C.R.; So, E.L. Significance of cerebellar atrophy in intractable temporal lobe epilepsy: A quantitative MRI study. Epilepsia 2000, 41, 1315–1320. [Google Scholar] [CrossRef]
- Hagemann, G.; Lemieux, L.; Free, S.L.; Krakow, K.; Everitt, A.D.; Kendall, B.E.; Stevens, J.M.; Shorvon, S.D. Cerebellar volumes in newly diagnosed and chronic epilepsy. J. Neurol. 2002, 249, 1651–1658. [Google Scholar] [CrossRef]
- Keller, S.S.; Wieshmann, U.C.; Mackay, C.E.; Denby, C.E.; Webb, J.; Roberts, N. Voxel based morphometry of grey matter abnormalities in patients with medically intractable temporal lobe epilepsy: Effects of side of seizure onset and epilepsy duration. J. Neurol. Neurosurg. Psychiatry 2002, 73, 648–655. [Google Scholar] [CrossRef] [Green Version]
- De Marcos, F.A.; Ghizoni, E.; Kobayashi, E.; Li, L.M.; Cendes, F. Cerebellar volume and long-term use of phenytoin. Seizure 2003, 12, 312–315. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.K.; Mori, S.; Kim, D.J.; Kim, S.Y.; Kim, S.Y.; Chu, M.; Heo, K.; Lee, B.I.; Kim, D.I. Diffusion tensor MRI and fiber tractography of cerebellar atrophy in phenytoin users. Epilepsia 2003, 44, 1536–1540. [Google Scholar] [CrossRef] [Green Version]
- Bonilha, L.; Rorden, C.; Castellano, G.; Pereira, F.; Rio, P.A.; Cendes, F.; Li, L.M. Voxel-based morphometry reveals gray matter network atrophy in refractory medial temporal lobe epilepsy. Arch. Neurol. 2004, 61, 1379–1384. [Google Scholar] [CrossRef] [Green Version]
- Hermann, B.; Seidenberg, M.; Sears, L.; Hansen, R.; Bayless, K.; Rutecki, P.; Dow, C. Cerebellar atrophy in temporal lobe epilepsy affects procedural memory. Neurology 2004, 63, 2129–2131. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.S.; Wilke, M.; Wieshmann, U.C.; Sluming, V.A.; Roberts, N. Comparison of standard and optimized voxel-based morphometry for analysis of brain changes associated with temporal lobe epilepsy. Neuroimage 2004, 23, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Hermann, B.P.; Bayless, K.; Hansen, R.; Parrish, J.; Seidenberg, M. Cerebellar atrophy in temporal lobe epilepsy. Epilepsy Behav. 2005, 7, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Szabo, C.A.; Lancaster, J.L.; Lee, S.; Xiong, J.H.; Cook, C.; Mayes, B.N.; Fox, P.T. MR imaging volumetry of subcortical structures and cerebellar hemispheres in temporal lobe epilepsy. AJNR Am. J. Neuroradiol. 2006, 27, 2155–2160. [Google Scholar] [PubMed]
- McDonald, C.R.; Hagler, D.J., Jr.; Ahmadi, M.E.; Tecoma, E.; Iragui, V.; Dale, A.M.; Halgren, E. Subcortical and cerebellar atrophy in mesial temporal lobe epilepsy revealed by automatic segmentation. Epilepsy Res. 2008, 79, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Riederer, F.; Lanzenberger, R.; Kaya, M.; Prayer, D.; Serles, W.; Baumgartner, C. Network atrophy in temporal lobe epilepsy: A voxel-based morphometry study. Neurology 2008, 71, 419–425. [Google Scholar] [CrossRef]
- Bilevicius, E.; Yasuda, C.L.; Silva, M.S.; Guerreiro, C.A.; Lopes-Cendes, I.; Cendes, F. Antiepileptic drug response in temporal lobe epilepsy: A clinical and MRI morphometry study. Neurology 2010, 75, 1695–1701. [Google Scholar] [CrossRef]
- Bonilha, L.; Edwards, J.C.; Kinsman, S.L.; Morgan, P.S.; Fridriksson, J.; Rorden, C.; Rumboldt, Z.; Roberts, D.R.; Eckert, M.A.; Halford, J.J. Extrahippocampal gray matter loss and hippocampal deafferentation in patients with temporal lobe epilepsy. Epilepsia 2010, 51, 519–528. [Google Scholar] [CrossRef] [Green Version]
- Oyegbile, T.O.; Bayless, K.; Dabbs, K.; Jones, J.; Rutecki, P.; Pierson, R.; Seidenberg, M.; Hermann, B. The nature and extent of cerebellar atrophy in chronic temporal lobe epilepsy. Epilepsia 2011, 52, 698–706. [Google Scholar] [CrossRef] [Green Version]
- Scanlon, C.; Mueller, S.G.; Tosun, D.; Cheong, I.; Garcia, P.; Barakos, J.; Weiner, M.W.; Laxer, K.D. Impact of methodologic choice for automatic detection of different aspects of brain atrophy by using temporal lobe epilepsy as a model. AJNR Am. J. Neuroradiol. 2011, 32, 1669–1676. [Google Scholar] [CrossRef] [Green Version]
- Alhusaini, S.; Doherty, C.P.; Scanlon, C.; Ronan, L.; Maguire, S.; Borgulya, G.; Brennan, P.; Delanty, N.; Fitzsimons, M.; Cavalleri, G.L. A cross-sectional MRI study of brain regional atrophy and clinical characteristics of temporal lobe epilepsy with hippocampal sclerosis. Epilepsy Res. 2012, 99, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Hellwig, S.; Gutmann, V.; Trimble, M.R.; van Elst, L.T. Cerebellar volume is linked to cognitive function in temporal lobe epilepsy: A quantitative MRI study. Epilepsy Behav. 2013, 28, 156–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sequeira, K.M.; Tabesh, A.; Sainju, R.K.; DeSantis, S.M.; Naselaris, T.; Joseph, J.E.; Ahlman, M.A.; Spicer, K.M.; Glazier, S.S.; Edwards, J.C.; et al. Perfusion network shift during seizures in medial temporal lobe epilepsy. PLoS ONE 2013, 8, e53204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.M.; Han, Y.H.; Kim, T.H.; Mun, C.W.; Shin, K.J.; Ha, S.Y.; Park, J.; Hur, Y.J.; Kim, H.Y.; Park, S.H.; et al. Cerebellar white matter changes in patients with newly diagnosed partial epilepsy of unknown etiology. Clin. Neurol. Neurosurg. 2015, 138, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Alvim, M.K.; Coan, A.C.; Campos, B.M.; Yasuda, C.L.; Oliveira, M.C.; Morita, M.E.; Cendes, F. Progression of gray matter atrophy in seizure-free patients with temporal lobe epilepsy. Epilepsia 2016, 57, 621–629. [Google Scholar] [CrossRef] [Green Version]
- Marcian, V.; Marecek, R.; Koritakova, E.; Pail, M.; Bares, M.; Brazdil, M. Morphological changes of cerebellar substructures in temporal lobe epilepsy: A complex phenomenon, not mere atrophy. Seizure 2018, 54, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Rajjoub, R.K.; Wook, J.H.; Van Buren, J.M. Significance of Purkinje cell density in seizure suppresion by chronic cerebellar stimulation. Neurology 1976, 26, 645–650. [Google Scholar] [CrossRef]
- Shields, L.B.; Hunsaker, D.M.; Hunsaker, J.C., 3rd; Parker, J.C., Jr. Sudden unexpected death in epilepsy: Neuropathologic findings. Am. J. Forensic Med. Pathol. 2002, 23, 307–314. [Google Scholar] [CrossRef]
- Rambeck, B.; Schnabel, R.; May, T.; Jurgens, U.; Villagran, R. Postmortem concentrations of phenytoin in different regions of the brain and in the serum: Analysis of autoptic specimens from 24 epileptic patients. Ther. Drug Monit. 1992, 14, 27–35. [Google Scholar] [CrossRef]
- Robertson, L.T.; Dow, R.S.; Cooper, I.S.; Levy, L.F. Morphological changes associated with chronic cerebellar stimulation in the human. J. Neurosurg. 1979, 51, 510–520. [Google Scholar] [CrossRef]
- Keppel Hesselink, J.M.; Kopsky, D.J. Phenytoin: 80 years young, from epilepsy to breast cancer, a remarkable molecule with multiple modes of action. J. Neurol. 2017, 264, 1617–1621. [Google Scholar] [CrossRef] [PubMed]
- Gaitatzis, A.; Sander, J.W. The long-term safety of antiepileptic drugs. CNS Drugs 2013, 27, 435–455. [Google Scholar] [CrossRef] [PubMed]
- Tellez-Zenteno, J.F.; Hernandez-Ronquillo, L. A review of the epidemiology of temporal lobe epilepsy. Epilepsy Res. Treat. 2012, 2012, 630853. [Google Scholar] [CrossRef] [PubMed]
- Caciagli, L.; Bernasconi, A.; Wiebe, S.; Koepp, M.J.; Bernasconi, N.; Bernhardt, B.C. A meta-analysis on progressive atrophy in intractable temporal lobe epilepsy: Time is brain? Neurology 2017, 89, 506–516. [Google Scholar] [CrossRef] [Green Version]
- Janszky, J.; Janszky, I.; Schulz, R.; Hoppe, M.; Behne, F.; Pannek, H.W.; Ebner, A. Temporal lobe epilepsy with hippocampal sclerosis: Predictors for long-term surgical outcome. Brain 2005, 128, 395–404. [Google Scholar] [CrossRef] [Green Version]
- Thom, M. Review: Hippocampal sclerosis in epilepsy: A neuropathology review. Neuropathol. Appl. Neurobiol. 2014, 40, 520–543. [Google Scholar] [CrossRef]
- Sone, D.; Sato, N.; Ota, M.; Maikusa, N.; Kimura, Y.; Matsuda, H. Abnormal neurite density and orientation dispersion in unilateral temporal lobe epilepsy detected by advanced diffusion imaging. Neuroimage Clin. 2018, 20, 772–782. [Google Scholar] [CrossRef]
- Duncan, J.S. Brain imaging in epilepsy. Pract. Neurol. 2019, 19, 438–443. [Google Scholar] [CrossRef]
- Sankaraneni, R.; Lachhwani, D. Antiepileptic drugs—a review. Pediatr. Ann. 2015, 44, e36–e42. [Google Scholar] [CrossRef] [Green Version]
- Perucca, E.; Beghi, E.; Dulac, O.; Shorvon, S.; Tomson, T. Assessing risk to benefit ratio in antiepileptic drug therapy. Epilepsy Res. 2000, 41, 107–139. [Google Scholar] [CrossRef]
- Kwan, P.; Brodie, M.J. Early identification of refractory epilepsy. N. Engl. J. Med. 2000, 342, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Moshe, S.L.; Perucca, E.; Ryvlin, P.; Tomson, T. Epilepsy: New advances. Lancet 2015, 385, 884–898. [Google Scholar] [CrossRef]
- Campos, M.S.A.; Ayres, L.R.; Morelo, M.R.S.; Carizio, F.A.M.; Pereira, L.R.L. Comparative efficacy of antiepileptic drugs for patients with generalized epileptic seizures: Systematic review and network meta-analyses. Int. J. Clin. Pharm. 2018, 40, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Jobst, B.C. Consensus Over Individualism: Validation of the ILAE Definition for Drug Resistant Epilepsy. Epilepsy Curr. 2015, 15, 172–173. [Google Scholar] [CrossRef] [Green Version]
- Laxer, K.D.; Trinka, E.; Hirsch, L.J.; Cendes, F.; Langfitt, J.; Delanty, N.; Resnick, T.; Benbadis, S.R. The consequences of refractory epilepsy and its treatment. Epilepsy Behav. 2014, 37, 59–70. [Google Scholar] [CrossRef] [Green Version]
- French, J.A. Refractory epilepsy: Clinical overview. Epilepsia 2007, 48 (Suppl. 1), 3–7. [Google Scholar] [CrossRef]
- Magiorkinis, E.; Diamantis, A.; Sidiropoulou, K.; Panteliadis, C. Highights in the history of epilepsy: The last 200 years. Epilepsy Res. Treat. 2014, 2014, 582039. [Google Scholar] [CrossRef] [Green Version]
- Craig, S. Phenytoin poisoning. Neurocrit. Care 2005, 3, 161–170. [Google Scholar] [CrossRef]
- Young, G.B.; Oppenheimer, S.R.; Gordon, B.A.; Wells, G.A.; Assis, L.P.; Kreeft, J.H.; Lohuis, N.A.; Blume, W.T. Ataxia in institutionalized patients with epilepsy. Can. J. Neurol. Sci. 1994, 21, 252–258. [Google Scholar] [CrossRef] [Green Version]
- Hess, D.R. Retrospective studies and chart reviews. Respir. Care 2004, 49, 1171–1174. [Google Scholar]
- Pannucci, C.J.; Wilkins, E.G. Identifying and avoiding bias in research. Plast Reconstr. Surg. 2010, 126, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Pedraza, O.; Bowers, D.; Gilmore, R. Asymmetry of the hippocampus and amygdala in MRI volumetric measurements of normal adults. J. Int. Neuropsychol. Soc. 2004, 10, 664–678. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.S.; Leung, C.Y.W.; Ho, C.C.A.; Yung, A. Classifications of seizures and epilepsies, where are we?—A brief historical review and update. J. Formos Med. Assoc. 2017, 116, 736–741. [Google Scholar] [CrossRef]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combinations for literature searches in systematic reviews: A prospective exploratory study. Syst. Rev. 2017, 6, 245. [Google Scholar] [CrossRef] [PubMed]
- Duncan, J.S. Neuroimaging methods to evaluate the etiology and consequences of epilepsy. Epilepsy Res. 2002, 50, 131–140. [Google Scholar] [CrossRef]


{kind=link}
| Total Number of Studies Included in this Review | 50 |
|---|---|
| Types of publications (%) | |
| Cross-sectional | 18 (36) |
| Correlational | 14 (28) |
| Case-Control | 10 (20) |
| Cohort | 7 (14) |
| Longitudinal | 1 (2) |
| Year of publication | |
| Range | 1976–2018 |
| Number of publications per decade | |
| 1970–1980 | 5 |
| 1981–1990 | 3 |
| 1991–2000 | 17 |
| 2001–2010 | 14 |
| 2011–present | 11 |
| Number of patients with epilepsy studied | |
| Total number of patients with epilepsy | 2826 |
| Mean number of patients per study (SD) | 56.5 (54.6) |
| Range | 3–248 |
| Median | 41 |
| Type of Treatment (%) | ||
|---|---|---|
| Monotherapy | 430 (34.8) | |
| Polytherapy | 804 (65.2) | |
| AED Type | Number of Patients | (%) |
| Phenytoin | 914 | (44) |
| Phenobarbital * | 324 | (15.5) |
| Carbamazepine | 299 | (14.3) |
| Sodium Valproate/Valproic Acid | 167 | (8.25) |
| Primidone | 119 | (5.88) |
| Diazepam | 74 | (3.66) |
| Acetazolamide | 44 | (2.17) |
| Lamotrigine | 30 | (1.48) |
| Nitrazepam | 25 | (1.24) |
| Gabapentin | 22 | (1.09) |
| Clonazepam | 19 | (0.94) |
| Vigabatrin | 15 | (0.74) |
| Sulthiamine | 14 | (0.69) |
| Topiramate | 11 | (0.54) |
| Trimethadione | 5 | (0.25) |
| Ethosuximide | 3 | (0.15) |
| Fluoxetine | 2 | (0.10) |
| Zonisamide | 2 | (0.10) |
| Felbamate | 2 | (0.10) |
| Haloperidol | 1 | (0.05) |
| Tiagabine | 1 | (0.05) |
| AED Type | Number of Patients | (%) |
|---|---|---|
| Phenytoin | 41 | (30.37) |
| Phenobarbital | 32 | (23.7) |
| Carbamazepine | 22 | (16.3) |
| Clonazepam | 9 | (6.67) |
| Sodium Valproate/Valproic acid | 7 | (5.19) |
| Primidone | 7 | (5.19) |
| Lamotrigine | 6 | (4.44) |
| Vigabatrin | 5 | (3.7) |
| Diazepam | 4 | (2.96) |
| Ethosuximide | 1 | (0.74) |
| Acetazolamide | 1 | (0.74) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibdali, M.; Hadjivassiliou, M.; Grünewald, R.A.; Shanmugarajah, P.D. Cerebellar Degeneration in Epilepsy: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 473. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020473
Ibdali M, Hadjivassiliou M, Grünewald RA, Shanmugarajah PD. Cerebellar Degeneration in Epilepsy: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(2):473. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020473
Chicago/Turabian StyleIbdali, Manar, Marios Hadjivassiliou, Richard A. Grünewald, and Priya D. Shanmugarajah. 2021. "Cerebellar Degeneration in Epilepsy: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 2: 473. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020473