
A Box to Put the Baby in: UK Parent Perceptions of Two Baby Box Programmes Promoted for Infant Sleep


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Participants
3.2. Information Provision
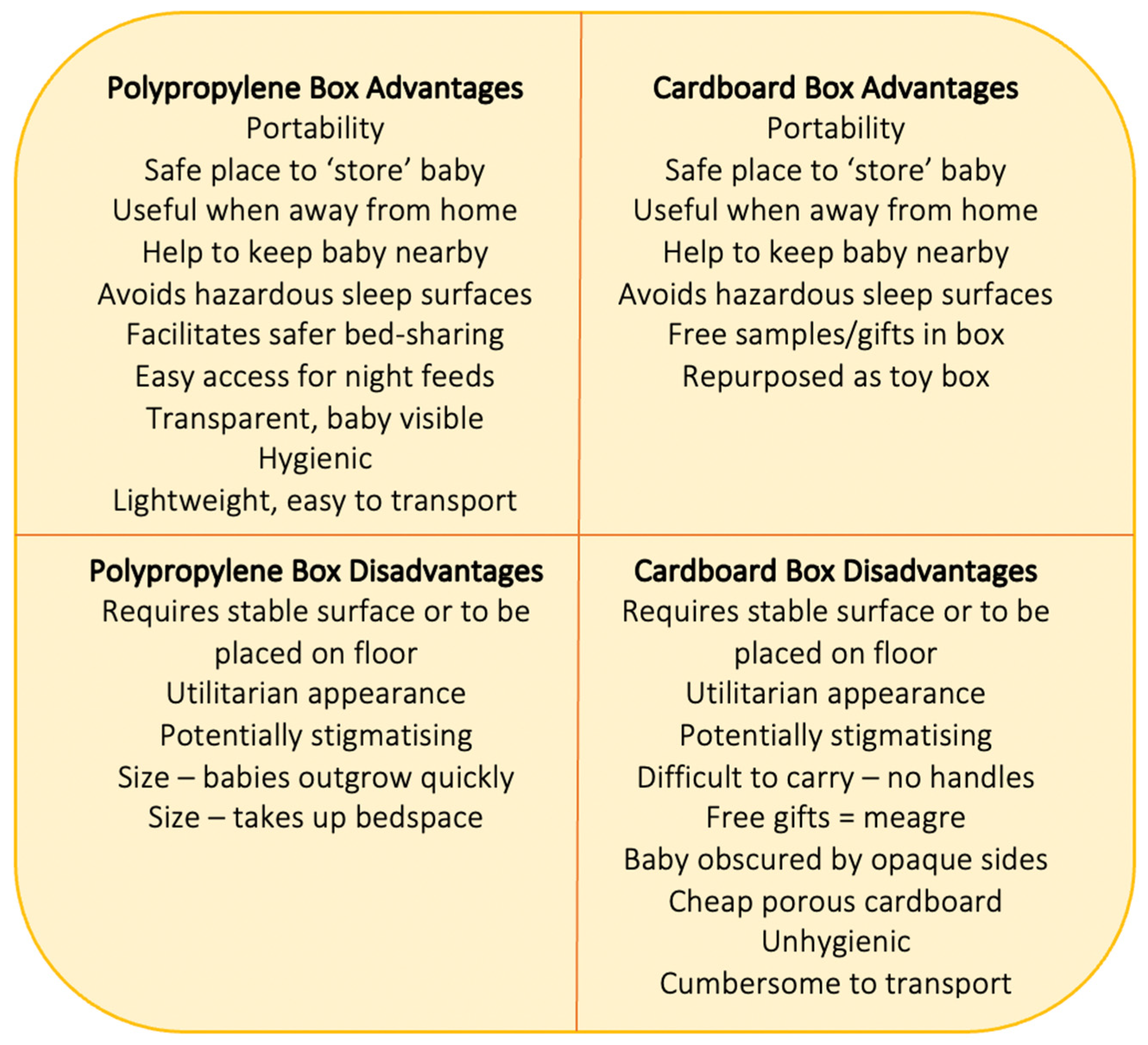
3.3. Using the Boxes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ISPID Epidemiology & Education Working Group. Evidence-Based Safe Infant Sleep Recommendations. 2016. Available online: https://www.ispid.org/infantdeath/factsheets (accessed on 13 August 2021).
- Volpe, L.E.; Ball, H.L. Infant sleep-related deaths: Why do parents take risks? Arch. Dis. Child. 2015, 100, 603–604. [Google Scholar] [CrossRef] [Green Version]
- Cole, R.; Young, J.; Kearney, L.; Thompson, J.M.D. Infant care practices and parent uptake of safe sleep messages: A cross-sectional survey in Queensland, Australia. BMC Pediatr. 2020, 20, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pease, A.; Blair, P.S.; Ingram, J.; Fleming, P. Conversations with families about reducing the risk of sudden infant death syndrome. J. Health Visit. 2019, 7, 226–231. [Google Scholar] [CrossRef] [Green Version]
- Crane, D.; Ball, H.L. A qualitative study in parental perceptions and understanding of SIDS-reduction guidance in a UK bi-cultural urban community. BMC Pediatr. 2016, 16, 23. [Google Scholar] [CrossRef] [Green Version]
- Lau, A.; Hall, W. Safe sleep, day and night: Mothers’ experiences regarding infant sleep safety. J. Clin. Nurs 2016, 25, 2816–2826. [Google Scholar] [CrossRef]
- Tipene-Leach, D.; Abel, S. Innovation to prevent sudden infant death: The wahakura as an Indigenous vision for a safe sleep environment. Aust. J. Prim. Health 2019, 25, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Cowan, S.; Clark, J.; Bennett, S. Using Pēpi-Pods: Report on Feedback from Families Who Used Protected Sleeping Spaces for Babies Following the Christchurch Earthquake of February 2011. 2012. Available online: www.changeforourchildren.co.nz (accessed on 13 August 2021).
- Ball, H.L.; Taylor, C.E. Baby-box schemes in England: Parent and practitioner experiences, and recommendations. BMC Pediatr. 2020, 20, 154. [Google Scholar] [CrossRef] [Green Version]
- Middlemiss, W.; Brownstein, N.C.; Leddy, M.; Nelson, S.; Manchiraju, S.; Grzywacz, J.G. Baby box distributions: Public Health benefit or concern? Public Health Rep. 2019, 134, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Cowan, S.; Bennett, S.; Clarke, J.; Pease, A. An evaluation of portable sleeping spaces for babies following the Christchurch earthquake of February 2011. J. Paediatr. Child Health 2013, 49, 364–368. [Google Scholar] [CrossRef]
- Tipene-Leach, D.; A Baddock, S.; Williams, S.M.; Tangiora, A.; Jones, R.; McElnay, C.; Taylor, B.J. The Pēpi-Pod study: Overnight video, oximetry and thermal environment while using an in-bed sleep device for sudden unexpected death in infancy prevention. J. Paediatr. Child Health 2018, 54, 638–646. [Google Scholar] [CrossRef]
- Cowan, S. Their First 500 Sleeps. Pēpi-Pod Report: 2012–2014. Describing Three Years of Distribution and Use of Portable Sleep Spaces for Babies at Increased Risk of Sudden Infant Death. Change for Our Children, Ltd, New Zealand. 2015. Available online: http://www.changeforourchildren.nz/files/docs/pepi-pod%20programme/their%20first%20500%20sleeps.pdf (accessed on 13 August 2021).
- Mitchell, E.A.; Cowan, S.; Tipene-Leach, D. The recent fall in postperinatal mortality in New Zealand and the Safe Sleep programme. Acta Paediatr. 2016, 105, 1312–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, J.; Watson, K.; Craigie, L.; Cowan, S.; Kearney, L. Uniting cultural practices and safe sleep environments for vulnerable indigenous australian infants. Aust. Nurs. Midwifery J. 2017, 24, 37. [Google Scholar] [PubMed]
- Young, J.; Watson, K.; Craigie, L.; Neville, J.; Hunt, J. Best practice principles for research with Aboriginal and Torres Strait Islander communities in action: Case study of a safe infant sleep strategy. Women Birth 2019, 32, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Young, J.; Cowan, S.; Watson, K.; Kearney, L.; Craigie, L. A Strategy to Promote Safe Sleeping Environments and Reduce the Risk of Sudden Unexpected Death in Infancy in Aboriginal and Torres Strait Islander communities. (ID: 99489008702621) Final Implementation Project Report for the Department of Child Safety, Y. 2020. Available online: https://csds.qld.edu.au/sdc/Provectus/ISIS/Module%201%20-%20Defining%20the%20priority%20health%20issue/unit-21092011070721240814/files/QH_Safe_Sleeping_Policy_StatementAndGuidelinesNov08.pdf (accessed on 30 October 2021). [CrossRef]
- Young, J.; Craigie, L.; Cowan, S.; Kearney, L.; Watson, K. Reducing Risk for Aboriginal and Torres Strait Islander Babies: Trial of a Safe Sleep Enabler to Reduce the Risk of Sudden Unexpected Deaths in Infancy in High Risk Environments (The Queensland Pepi-Pod Program). Final Research Project Report; Sippy Downs, Queensland, Australia. 2018. Available online: https://research.usc.edu.au/esploro/outputs/99450633202621 (accessed on 30 October 2021).
- Kela. Maternity Package. 2021. Available online: https://www.kela.fi/web/en/maternitypackage (accessed on 31 August 2021).
- Lee, H. Why Finnish Babies Sleep in Boxes. BBC News, 4 June 2013. Available online: https://www.bbc.co.uk/news/magazine-22751415(accessed on 13 August 2021).
- Koivu, A.; Phan, Y.T.H.; Näsi, E.; Abuhamed, J.; Perry, B.L.; Atkins, S.; Perkiö, M.; Koivusalo, M. The Baby Box Enhancing the Wellbeing of Babies and Mothers around the World; Kela: Helsinki, Finland, 2020. [Google Scholar]
- Taylor, C.E.; Ball, H.L. Parents’ perceptions and usage of baby boxes: An online survey of parents and practitioners in England. Child. Health Care Dev. 2021. under review. [Google Scholar]
- Osorio, J.C.; Feld, H.; Young, T.; Bahamonde, M. Case series: First 6 cases of ongoing randomized controlled trial on the effects of the introduction of a Cardboard Baby Box in the promotion of safe infant sleep practices in a sub-urban community of Santo Domingo, Ecuador. Pediatrics 2020, 146, 263. [Google Scholar]
- Craig, P.; Doi, L.; Tirman, L. Evaluability Assessment of Scotland’s Baby Box—Report to the Scottish Government. Scottish Government; 2018. Available online: https://www.gov.scot/publications/evaluability-assessment-scotlands-baby-box-report-scottish-government (accessed on 13 August 2021).
- Pantoja, R.; Herrine, G.; Zhao, H.; Swiecki-Sikora, A.L.; Kiani, K.; Datwani, H. Baby boxes and breastfeeding: A study of the impact of safe sleeping environments on infant feeding method [26H]. Obstet. Gynecol. 2019, 133, 91S. [Google Scholar] [CrossRef]
- Dalvie, N.; Nguyen, V.; Colson, E.; Loyal, J. Mothers’ perceptions of the cardboard box as a potential sleep space. Acad. Pediatr. 2019, 19, 787–792. [Google Scholar] [CrossRef]
- Heere, M.; Moughan, B.; Alfonsi, J.; Rodriguez, J.; Aronoff, S. Effect of education and cardboard bassinet distribution on newborn bed-sharing. Glob. Pediatr. Health 2019, 6, 2333794X19829173. [Google Scholar] [CrossRef] [Green Version]
- Reid, J.; David, S. Decolonising the Finnish Baby box: A sociomaterial approach to designing interventions for infant and maternal health and well-being in Zambia. J. Early Child. Educ. Res. 2019, 8, 312–331. [Google Scholar]
- Bartick, M.; Tomori, C.; Ball, H.L. Babies in boxes and the missing links on safe sleep: Human evolution and cultural revolution. Matern. Child Nutr. 2017, 14, e12544. [Google Scholar] [CrossRef] [PubMed]
- Blair, P.; Pease, A.; Bates, F.; Ball, H.L.; Thompson, J.M.D.; Hauck, F.R.; Moon, R.; McEntire, B.; Shatz, A.; Cohen, M.; et al. Concerns about the promotion of a cardboard baby box as a place for infants to sleep. BMJ 2018, 363, k4243. [Google Scholar] [CrossRef] [PubMed]
- Mulford, K. Why New Jersey is Encouraging Moms to Put Their Newborns in a Box. The Courier-Post, 27 June 2017. Available online: https://eu.courierpostonline.com/story/news/health/2017/01/26/baby-box-program-rolls-out-nj/96963836/(accessed on 13 August 2021).
- Barford, V. Why Babies all over the World are now Sleeping in Boxes. BBC News Magazine, 4 April 2016. Available online: https://www.bbc.co.uk/news/magazine-35834370(accessed on 13 August 2021).
- Ball, H.L.; Taylor, C.E.; Yuill, C.M. Let’s Talk About Sleep: Final Report Executive Summary. 2019. Available online: https://www.durham.ac.uk/disc/research/projects/ (accessed on 13 August 2021).
- Russell, C.; Whitmore, M.; Burrows, D.; Ball, H.L. Where might my baby sleep? Design and evaluation of a novel discussion tool for parent education. Int. J. Birth Parent. Educ. 2015, 2, 12–16. [Google Scholar]
- Cowan, S. Creating change: How knowledge translates into action for protecting babies from sudden infant death? Curr. Pediatr. Rev. 2010, 6, 86–94. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.R.; Mathur, A. The value of online surveys. Internet Res. 2005, 15, 195–219. [Google Scholar] [CrossRef]
- Ball, H.L. Conducting Online Surveys. J. Hum. Lact. 2018, 35, 413–417. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | Polypropylene Box Scheme | Cardboard Box Scheme |
|---|---|---|
| N | 79 | 77 |
| Follow-up | 68 (86%) | 65 (89%) |
| Mean Maternal Age | 21.4 years | no data |
| Primiparas | 51 (75%) | no data |
| Partnered | 44 (64%) | no data |
| Smokers | 24 (35%) | no data |
| Post-compulsory education | 2 (3%) | no data |
| Ethnicity = ‘White’ | 66 (97%) | no data |
| Education Type | Polypropylene Box Scheme (n = 68) | Cardboard Box Scheme (n = 65) |
|---|---|---|
| Received any information about safe box use | 97.5% | 95% |
| Written information | 97.5% | 54% |
| In-person discussion with health professional | 90% | 7% |
| Narrated video | 82% | 74% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ball, H.L.; Taylor, C.E.; Yuill, C.M. A Box to Put the Baby in: UK Parent Perceptions of Two Baby Box Programmes Promoted for Infant Sleep. Int. J. Environ. Res. Public Health 2021, 18, 11473. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111473
Ball HL, Taylor CE, Yuill CM. A Box to Put the Baby in: UK Parent Perceptions of Two Baby Box Programmes Promoted for Infant Sleep. International Journal of Environmental Research and Public Health. 2021; 18(21):11473. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111473
Chicago/Turabian StyleBall, Helen L., Catherine E. Taylor, and Cassandra M. Yuill. 2021. "A Box to Put the Baby in: UK Parent Perceptions of Two Baby Box Programmes Promoted for Infant Sleep" International Journal of Environmental Research and Public Health 18, no. 21: 11473. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111473