
A Focus Group Study to Understand the Perspectives of Physiotherapists on Barriers and Facilitators to Advancing Rehabilitation in Low-Resource and Conflict Settings

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. FGD Facilitators’ Profiles
2.4. Study Population
2.5. Ethics Statement
2.6. Data Collection
2.7. Data Analysis
3. Results
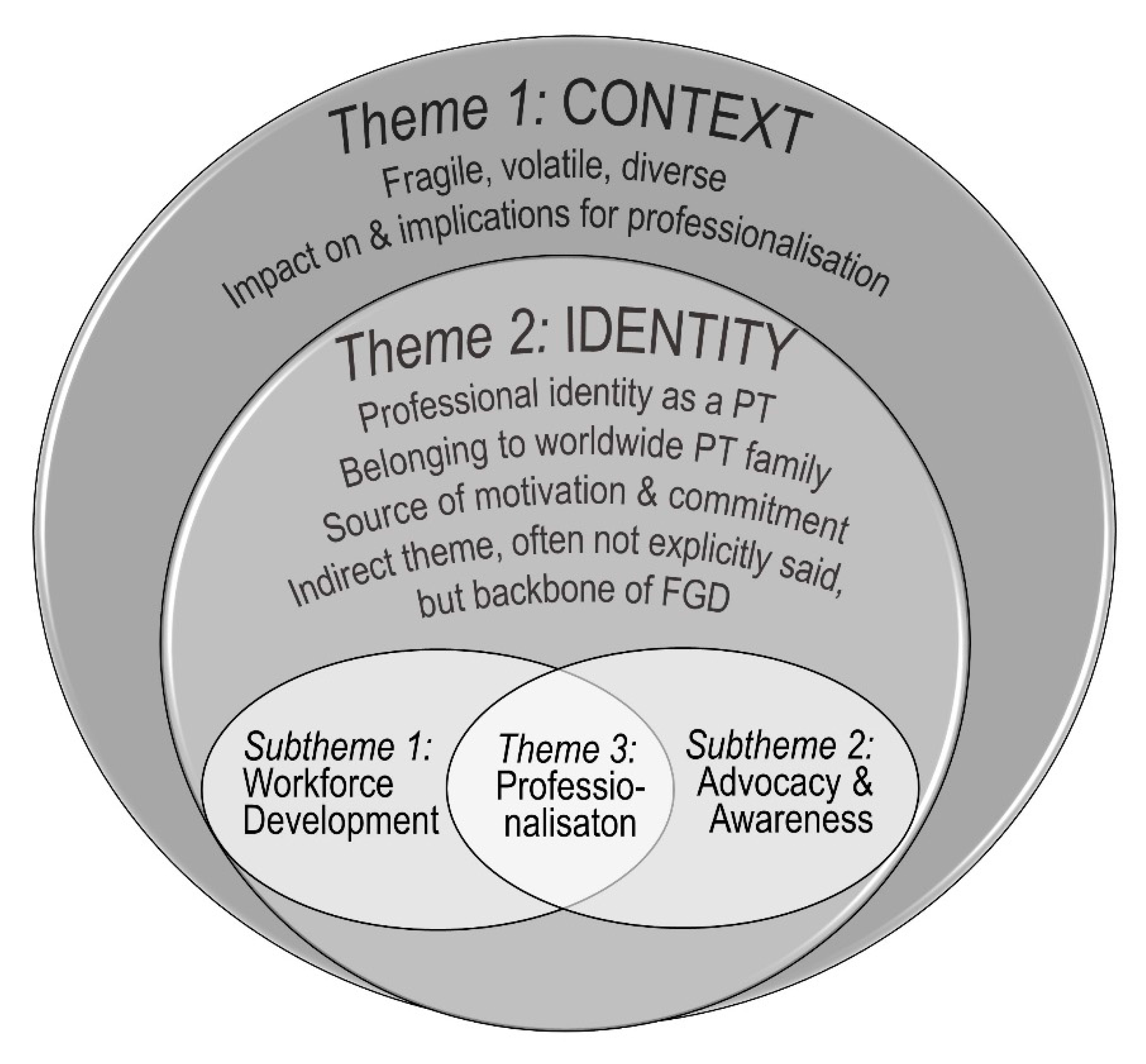
3.1. Three Key Themes: Context, Professional Identity and Professionalisation
3.2. Theme 1: Context
“Now we are in peace in the country. So, we can do something and not only surviving but to do something to our profession.”
“The hospital project is for weapon wounded. … we have the physiotherapy, the normal private sector and we have … the ICRC who is supporting weapon wounded and disabled people and the vulnerable … from [neighbouring country at war] … they are very, very, very vulnerable people … so it is two different sectors.”
“These things do not reach us, the articles or the practice of physiotherapy. So we need these things to be available … but mostly the internet in some locations [is] not available, you know access is difficult to the network … where I come from, even a telephone call you cannot make.”
“[The] mother of that patient doesn’t know about the … pregnancy … low age they get married and … they deliver at home and because of that the level of cerebral palsy is high.”
“You are already … living daily with a lot of tension and you are still continuing … and working a lot. This give[s] you more opportunity to have well experience. … When you are saying that [colleagues from HIC] are using … shockwave … or ultrasound … I don’t have electricity … And you are … going to treat the persons which should … be at the ICU [intensive care unit] … these challenges give you a lot of experience.”
3.3. Theme 2: Professional Identity
“When you work a lot in a context and the things don’t improve, you have no results and you feel a bit frustrated and when you … discover that many colleagues in different countries, different contexts have same challenges as you even bigge[r] challenges than you … and you can learn from their experiences and try to improve your context.”
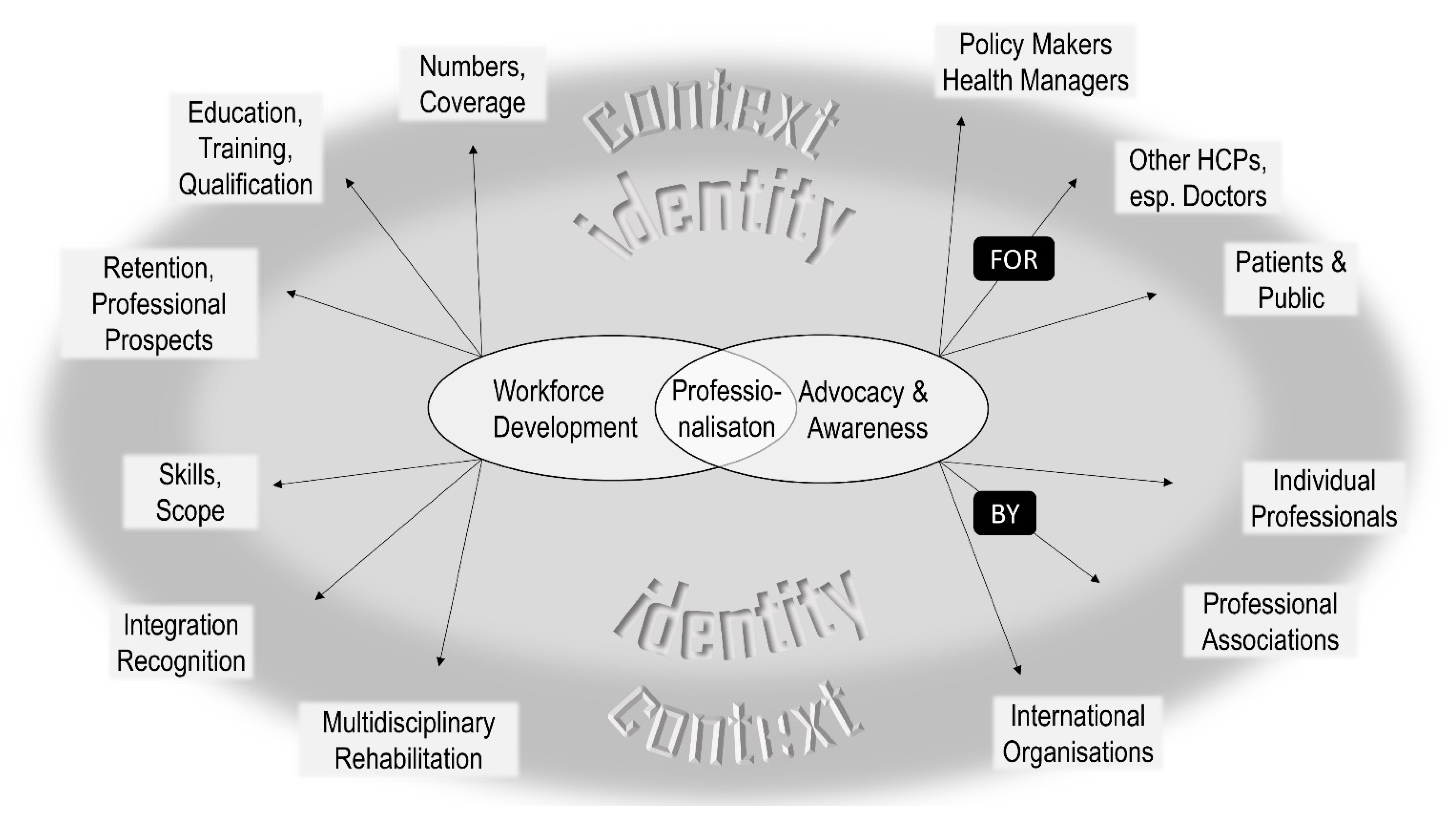
3.4. Theme 3: Professionalisation
3.4.1. Subtheme 1: Workforce Development
(a) Numbers, Coverage
“For a population of two million people there is only five physiotherapists … of these … four are working in the only rehabilitation centre that exists in the country, it is in the capital. And the other physiotherapist work[s] in the [capital’s] public hospital … to reach from the capital to the most far regions maybe it is nine hours travel with difficult roads … [and] two days to come from the most far islands to the capital.”
(b) Education, Training, Qualification
“Even for me, when I went to school to study it, some people were saying: ‘There is no better qualification that you[’re] suppose[d] to study? Why do you study physiotherapy? What is the benefit of that?’ So people were blocking my interest even to do it.”
“They have to go out of [the country] and pay lots of money … that’s why we have no opportunity to upgrade our knowledge.”
“We are currently discussing with Ministry of Health and Ministry of Education to include diploma physiotherapy in the curriculum … because we need them at the low level of care.”
“If you want the doctor or the other health professional to recognise the physical therapy you need to upscale the degree. Because right now when we talk the doctor, doctor said your level cannot talk with us. That’s the problem and then we do not have any physiotherapists position in the ministry.”
(c) Skills, Scope
(d) Integration, Recognition
“Physio as a profession within the health is growing slowly but yet we have a lot of obstacles with medical doctors and physicians who are trying to put blocks in front of us.”
(e) Retention, Professional Prospects
“We have very rare of students to enrolment … very few students … we can make the awareness to … the high school students … so that they will know about the benefit of physiotherapy so they can consider that profession.”
“Physiotherapy is recruited by the Ministry of Health to work at the hospital but they do not work as a physiotherapy profession they work as the nurses, pharmacists and … administrator.”
“So we are graduating … [an] army of physios but most of them, they are leaving … to gulf countries or Europe for better life conditions and good opportunities … In a governmental hospital you will be supervised by a doctor … you will be just an applier. You will get a premade treatment plan and … repeat the same thing for one or two years … so they do not feel that they are developing in their career…. That’s why recently, there is a new fashion happening that people … after they finish their bachelor they go and study again medicine. … after wasting four years because at the end … you will always feel like … I am not recognised by the health profession.”
(f) Multidisciplinary Rehabilitation
“Right now we do not have any OT [occupational therapist]. We don’t have ST [speech therapist]. So the physiotherapy in [country] [is] doing all the job of the OT and ST.”
“You have other professional rehabilitation as OT, no?”--“In my country we have … speech therapist … but they are … not more than five.”--“I ask this because our … strategy with … government … we have a federation of professional rehabilitation and we have [to] go together in the lobbying … because the matter of the profession is not only PT [physiotherapy], it is about rehabilitation.”
3.4.2. Subtheme 2: Professional Advocacy and Awareness Raising
“The first thing in my country is the lack of awareness at all levels. When I say at all levels, I mean at community level, health professionals about physiotherapy and at ministry of health level.”
“The discovery for me was the importance … [of] advocacy of the profession and the association … I understood why it is important [to] repeat again and again … what is the competences of physiotherapists and how we can contribute, not only for the care of the patient, but also to the overall health system, how we can help other colleagues and how is important to have a national association to have a dialogue with policy makers and international organisations and have the support to develop the physiotherapy in the country.”
“Until you get disabled, or you have a pain or you need to go to a physio clinic, then you will understand what is physiotherapy. It is not like a dermatologist or gynaecologist or whatever of medical professions. They [the patients] know exactly what they [other medical professions] do even if you are not in need for them, in general.”
“I started to realise the importance of the … national associations of physiotherapy and how much its strengthening … [means] for the physios in their country. How they can be united. How they can share the ideas and give the force to be recognized nationally and later internationally. And this is what we are missing in [country]. The weakness of the association. It was just recently started.”
“We do … lobbying in our government because now … we are members of the WCPT, and we must follow the rules and the programmes.”
“We need [to] show to ourselves and to the others that this profession is something … That it is a health profession that can change your life. So, it [is] for us and for the patient to believe in this.”
“We received a lot [of] patients that tried another treatment and come to the physiotherapy as the last resort because nothing [else] have helped … they have many months or even years of evolution and possibilities of improvement are, of course, clinically very reduced.”
“Sometimes the situation can push you … out of the evidence … there are some patients…, they come with their own ideas: ‘If you treat me like [this] I am not going to accept.’ What you do then? You have to listen, then you … try and … convince him … favouring what he is saying, then almost leaving your line of profession, then later you come in agreement to treat him almost in the way that he [is] proposing, … less than what you want … as a professional.”
“Now the role of physiotherapy there is to help identify this people …, give them awareness, also those who have reached to the hospital make proper assessment and give proper services to this people.”
4. Discussion
4.1. The Role of Physiotherapists
4.2. Full Integration in Health Systems
4.3. Multi-Stakeholder Engagement and Support
4.4. The Importance of Context and Its Implications
4.5. Limitations, Strengths and Trustworthiness
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fennelly, O.; Blake, C.; FitzGerald, O.; Breen, R.; O’Sullivan, C.; O’Mir, M.; Desmeules, F.; Cunningham, C. Advanced musculoskeletal physiotherapy practice in Ireland: A National Survey. Musculoskelet. Care 2018, 16, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Bury, T.J.; Stokes, E.K. A Global view of direct access and patient self-referral to physical therapy: Implications for the profession. Phys. Ther. 2013, 93, 449–459. [Google Scholar] [CrossRef]
- Sommers, J.; Engelbert, R.H.H.; Dettling-Ihnenfeldt, D.; Gosselink, R.; Spronk, P.E.; Nollet, F.; Van Der Schaaf, M. Physiotherapy in the intensive care unit: An evidence-based, expert driven, practical statement and rehabilitation recommendations. Clin. Rehabil. 2015, 29, 1051–1063. [Google Scholar] [CrossRef] [PubMed]
- Van Melick, N.; Van Cingel, R.E.H.; Brooijmans, F.; Neeter, C.; Van Tienen, T.; Hullegie, W.; Nijhuis-Van Der Sanden, M.W.G. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [Green Version]
- Wilson, L.M.; Morrison, L.; Robinson, K.A. Airway clearance techniques for cystic fibrosis: An overview of Cochrane systematic reviews. Cochrane Database Syst. Rev. 2019, 2019, CD011231. [Google Scholar] [CrossRef] [PubMed]
- Shields, G.E.; Wells, A.; Doherty, P.; Heagerty, A.; Buck, D.; Davies, L.M. Cost-effectiveness of cardiac rehabilitation: A systematic review. Heart 2018, 104, 1403–1410. [Google Scholar] [CrossRef]
- Oldridge, N.; Taylor, R.S. Cost-effectiveness of exercise therapy in patients with coronary heart disease, chronic heart failure and associated risk factors: A systematic review of economic evaluations of randomized clinical trials. Eur. J. Prev. Cardiol. 2020, 27, 1045–1055. [Google Scholar] [CrossRef]
- Khan, K.A.; Mazuquin, B.; Canaway, A.; Petrou, S.; Bruce, J. Systematic review of economic evaluations of exercise and physiotherapy for patients treated for breast cancer. Breast Cancer Res. Treat. 2019, 176, 37–52. [Google Scholar] [CrossRef] [Green Version]
- Guillon, M.; Rochaix, L.; Dupont, J.C.K. Cost-effectiveness of interventions based on physical activity in the treatment of chronic conditions: A systematic literature review. Int. J. Technol. Assess. Health Care 2018, 34, 481–497. [Google Scholar] [CrossRef]
- Howard-Wilsher, S.; Irvine, L.; Fan, H.; Shakespeare, T.; Suhrcke, M.; Horton, S.; Poland, F.; Hooper, L.; Song, F. Systematic overview of economic evaluations of health-related rehabilitation. Disabil. Health J. 2016, 9, 11–25. [Google Scholar] [CrossRef] [Green Version]
- Kamenov, K.; Mills, J.-A.; Chatterji, S.; Cieza, A. Needs and unmet needs for rehabilitation services: A scoping review. Disabil. Rehabil. 2019, 41, 1227–1237. [Google Scholar] [CrossRef]
- Bello, A.I.; Adegoke, B.O.A. Ethics in Physiotherapy Practice—An African Perspective. In African Perspectives on Ethics for Healthcare Professionals; Nortjé, N., Hoffmann, W.A., De Jongh, J.-C., Eds.; Springer: Cham, Switzerland, 2018; Volume 13, pp. 133–146. [Google Scholar]
- Barth, C.A. Meeting the needs of people with physical disabilities in crisis settings. Bull. World Health Organ. 2019, 97, 790–790A. [Google Scholar] [CrossRef] [PubMed]
- Agho, A.O.; John, E.B. Occupational therapy and physiotherapy education and workforce in Anglophone sub-Saharan Africa countries. Hum. Resour. Health 2017, 15, 37. [Google Scholar] [CrossRef] [PubMed]
- Jesus, T.S.; Landry, M.D.; Dussault, G.; Fronteira, I. Human resources for health (and rehabilitation): Six Rehab-Workforce Challenges for the century. Hum. Resour. Health 2017, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Jesus, T.S.; Landry, M.D.; Hoenig, H. Global Need for Physical Rehabilitation: Systematic Analysis from the Global Burden of Disease Study 2017. Int. J. Environ. Res. Public Health 2019, 16, 980. [Google Scholar] [CrossRef] [Green Version]
- World Physiotherapy Profile of the Global Profession. World Physiotherapy. Available online: https://world.physio/membership/profession-profile (accessed on 22 April 2021).
- Mamin, F.A.; Hayes, R. Physiotherapy in Bangladesh: Inequality Begets Inequality. Front. Public Health 2018, 6, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wickford, J.; Duttine, A. Answering global health needs in low-income countries: Considering the role of physical therapists. World Med. Health Policy 2013, 5, 141–160. [Google Scholar] [CrossRef]
- Mcpherson, A.; Durham, J.; Richards, N.; Gouda, H.; Rampatige, R.; Whittaker, M. Strengthening health information systems for disability-related rehabilitation in LMICs. Health Policy Plan. 2017, 32, 384–394. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.; Roberts, B.; Knight, A.; Gosselin, R.; Blanchet, K. A systematic literature review of the quality of evidence for injury and rehabilitation interventions in humanitarian crises. Int. J. Public Health 2015, 60, 865–872. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. World Report on Disability; World Health Organisation: Geneva, Switzerland, 2011; ISBN 9789241564182. [Google Scholar]
- Blanchet, K.; Ramesh, A.; Frison, S.; Warren, E.; Hossain, M.; Smith, J.; Knight, A.; Post, N.; Lewis, C.; Woodward, A.; et al. Evidence on public health interventions in humanitarian crises. Lancet 2017, 390, 2287–2296. [Google Scholar] [CrossRef]
- Bourgeois, A.; Cheriet, I.; Drum, S.; Friedel, F.; Angama Mueller, L.; Powell, T.; Rau, B.; Schmid, C. Physiotherapy at the ICRC. Reference Manual; International Committee of the Red Cross: Geneva, Switzerland, 2017. [Google Scholar]
- Pascal, M.R.; Mann, M.; Dunleavy, K.; Chevan, J.; Kirenga, L.; Nuhu, A. Leadership development of rehabilitation Professionals in a low-resource Country: A transformational leadership, project-based model. Front. Public Health 2017, 5, 143. [Google Scholar] [CrossRef] [Green Version]
- Musani, A.; Brennan, R.; Norton, I.; Thieren, M.; Salama, P. Examining humanitarian principles in changing warfare. Lancet 2018, 391, 2322. [Google Scholar] [CrossRef]
- Giannou, C.; Baldan, M.; Molde, A. War Surgery: Working With Limited Resources in Armed Conflict and Other Situations of Violence; International Committee of the Red Cross: Geneva, Switzerland, 2013; Volume 2. [Google Scholar]
- Barth, C.A.; Wladis, A.; Blake, C.; Bhandarkar, P.; Aebischer Perone, S.; O’Sullivan, C. Retrospective observational study of characteristics of persons with amputations accessing International Committee of the Red Cross (ICRC) rehabilitation centres in five conflict and post-conflict countries. BMJ Open 2021, in press. [Google Scholar]
- Bright, T.; Wallace, S.; Kuper, H. A Systematic Review of Access to Rehabilitation for People with Disabilities in Low- and Middle-Income Countries. Int. J. Environ. Res. Public Health 2018, 15, 2165. [Google Scholar] [CrossRef] [Green Version]
- International Committee of the Red Cross. Physical Rehabilitation Programme. Annual Report 2019; International Committee of the Red Cross: Geneva, Switzerland, 2020. [Google Scholar]
- Lathia, C.; Skelton, P.; Clift, Z. (Eds.) Early Rehabilitation in Conflicts and Disasters; Humanity and Inclusion: London, UK, 2020. [Google Scholar]
- World Confederation for Physical Therapy. The Role of Physical Therapists in Disaster Management; World Confederation for Physical Therapy: London, UK, 2016. [Google Scholar]
- Mousavi, G.; Ardalan, A.; Khankeh, H.; Kamali, M.; Ostadtaghizadeh, A. Physical Rehabilitation Services in Disasters and Emergencies: A Systematic Review. Iran. J. Public Health 2019, 48, 808–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Rehabilitation 2030—A Call for Action—Concept Note; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Smith, J.; Bekker, H.; Cheater, F. Theoretical versus pragmatic design in qualitative research. Nurse Res. 2011, 18, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Glasgow, R.E. What Does It Mean to Be Pragmatic? Pragmatic Methods, Measures, and Models to Facilitate Research Translation. Source Health Educ. Behav. 2013, 40, 257–265. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Barth, C.A.; Bjoerk, M.; Cemulini, V.; O’Sullivan, C.; Björk, M.; Cemulini, V.; O’Sullivan, C. Workshop Report for ICRC-Sponsored Delegates to WCPT Congress. 2019. Available online: https://world.physio/news/workshop-report-for-ICRC-sponsored-delegates-to-WCPT-Congress-2019 (accessed on 15 July 2019).
- Van Zyl, C.; Badenhorst, M.; Hanekom, S.; Heine, M. Unravelling “low-resource settings”: A systematic scoping review with qualitative content analysis. BMJ Glob. Health 2021, 6, 5190. [Google Scholar] [CrossRef] [PubMed]
- International Committee of the Red Cross. Protracted Conflict and Humanitarian Action: Some Recent ICRC Experiences; International Committee of the Red Cross: Geneva, Switzerland, 2016. [Google Scholar]
- United Nations Office for the Coordination of Humanitarian Affairs (OCHA). Global Humanitarian Overview 2020. United Nations-Coordinated Support to People Affected by Disaster and Conflict; United Nations: New York, NY, USA, 2020. [Google Scholar]
- Halcomb, E.J.; Gholizadeh, L.; DiGiacomo, M.; Phillips, J.; Davidson, P.M. Literature review: Considerations in undertaking focus group research with culturally and linguistically diverse groups. J. Clin. Nurs. 2007, 16, 1000–1011. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V.; Hayfield, N. ‘A starting point for your journey, not a map’: Nikki Hayfield in conversation with Virginia Braun and Victoria Clarke about thematic analysis. Qual. Res. Psychol. 2019, 1–22. [Google Scholar] [CrossRef]
- Taylor, R.; Zwisler, A.D.; Uddin, J. Global health-care systems must prioritise rehabilitation. Lancet 2020, 396, 1946–1947. [Google Scholar] [CrossRef]
- Jacobsen, K.H.; Zeraye, H.A.; Bisesi, M.S.; Gartin, M.; Malouin, R.A.; Waggett, C.E. Master of public health global health concentration competencies: Preparing culturally skilled practitioners to serve internationally, nationally, and locally. Am. J. Public Health 2019, 109, 1189–1190. [Google Scholar] [CrossRef] [PubMed]
- Fonn, S.; Egesah, O.; Cole, D.; Griffiths, F.; Manderson, L.; Kabiru, C.; Ezeh, A.; Thorogood, M.; Izugbara, C. Building the capacity to solve complex health challenges in sub-Saharan Africa: CARTA’s multidisciplinary PhD training. Can. J. Public Health 2016, 107, 381–386. [Google Scholar] [CrossRef]
- Rauch, A.; Negrini, S.; Cieza, A. Toward Strengthening Rehabilitation in Health Systems: Methods Used to Develop a WHO Package of Rehabilitation Interventions. Arch. Phys. Med. Rehabil. 2019, 100, 2205–2211. [Google Scholar] [CrossRef]
- The Lancet Prioritising disability in universal health coverage. Lancet 2019, 394, 187. [CrossRef]
- Stucki, G.; Bickenbach, J.; Gutenbrunner, C.; Melvin, J. Rehabilitation: The health strategy of the 21st century. J. Rehabil. Med. 2018, 50, 309–316. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Rehabilitation in Health Systems; World Health Organisation: Geneva, Switzerland, 2017; ISBN 9789241549974. [Google Scholar]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef]
- Bury, T.; Moffat, M. Physiotherapists have a vital part to play in combatting the burden of noncommunicable diseases. Physiotherapy 2014, 100, 94–96. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, N.; Barnes, R.; Mlenzana, N.; Mostert, K.; Amosun, S.L. Physiotherapy in rehabilitation and prohabilitation across the lifespan. S. Afr. Med. J. 2019, 109, 142–144. [Google Scholar] [CrossRef] [Green Version]
- Narain, S.; Mathye, D. Do physiotherapists have a role to play in the sustainable development goals? A qualitative exploration. S. Afr. J. Physiother. 2019, 75, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kunstler, B.E.; Cook, J.L.; Freene, N.; Finch, C.F.; Kemp, J.L.; O’Halloran, P.D.; Gaida, J.E. Physiotherapist-led physical activity interventions are efficacious at increasing physical activity levels: A systematic review and meta-analysis. Clin. J. Sport Med. 2018, 28, 304–315. [Google Scholar] [CrossRef]
- Heinemann, A.W.; Feuerstein, M.; Frontera, W.R.; Gard, S.A.; Kaminsky, L.A.; Negrini, S.; Richards, L.G.; Vallée, C.; Zalm, M. Rehabilitation is a global health priority. Arch. Phys. Med. Rehabil. 2020, 20, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Christian, A.; González-Fernández, M.; Mayer, R.S.; Haig, A.J. Rehabilitation needs of persons discharged from an African trauma center. Pan Afr. Med. J. 2011, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guide for Rehabilitation Workforce Evaluation. Available online: https://cdn.who.int/media/docs/default-source/documents/health-topics/rehabilitation/2942-dar-r-wep-info-sheet-170221.pdf?sfvrsn=81541771_5&download=true (accessed on 20 September 2021).
- Louw, Q.; Twizeyemariya, A.; Grimmer, K.; Leibbrandt, D. Estimating the costs and benefits of stroke rehabilitation in South Africa. J. Eval. Clin. Pract. 2020, 26, 1181–1187. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.E.; Holmer, H.; Maraka, J.; Ayana, B.; Hansen, L.; Lavy, C.B.D. Cost-effectiveness of club-foot treatment in low-income and middle-income countries by the Ponseti method. BMJ Glob. Health 2016, 1, e000023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naicker, A.S.; Htwe, O.; Tannor, A.Y.; De Groote, W.; Yuliawiratman, B.S.; Naicker, M.S. Facilitators and Barriers to the Rehabilitation Workforce Capacity Building in Low- to Middle-Income Countries. Phys. Med. Rehabil. Clin. N. Am. 2019, 30, 867–877. [Google Scholar] [CrossRef]
- The New Humanitarian. Saving Lives and Making Money: Can Humanitarian Impact Bonds Marry the Two? Available online: https://www.thenewhumanitarian.org/analysis/2019/08/15/humanitarian-impact-bonds (accessed on 18 September 2021).
- International Committee of the Red Cross. The ICRC Strategy to Assure Health Care for People Affected by Armed Conflict and Other Situations of Violence; International Committee of the Red Cross: Geneva, Switzerland, 2014. [Google Scholar]
- The New Humanitarian. Racism and Decolonisation in International Development. Available online: https://www.thenewhumanitarian.org/opinion/2020/07/13/decolonisation-aid-humanitarian-development-racism-black-lives-matter (accessed on 16 September 2021).
- Aloudat, T. The Damage Aid Workers Can Do—with Just Their Words. The National. Available online: https://www.thenationalnews.com/opinion/comment/the-damage-aid-workers-can-do-with-just-their-words-1.1190907 (accessed on 23 April 2021).
- Peace Direct; Paige, S. Time to Decolonise Aid. Insights and Lessons from a Global Consultation; Peace Direct: London, UK, 2021. [Google Scholar]
- World Health Organization. Rehabilitation 2030. 8–9 July 2019. Meeting Report; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- McSweeney, E.; Gowran, R.J. Wheelchair service provision education and training in low and lower middle income countries: A scoping review. Disabil. Rehabil. Assist. Technol. 2019, 14, 33–45. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, C.; Kazibwe, H.; Whitehouse, Z.; Blake, C. Constructing a global learning partnership in physiotherapy: An Ireland-Uganda initiative. Front. Public Health 2017, 5, 107. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Evaluation du Domaine de la Réadaptation au Bénin; World Health Organisation: Geneva, Switzerland, 2019. [Google Scholar]
- Shahabi, S.; Skempes, D.; Pardhan, S.; Jalali, M.; Lankarani, K.B. Nine years of war and internal conflicts in Syria: A call for physical rehabilitation services. Disabil. Soc. 2021, 36, 508–512. [Google Scholar] [CrossRef]
- Ugarte, D.; Verardi, V. Does Aid Induce Brain Drain? The Effect of Foreign Aid on Migration Selection. Cent. Res. Econ. Dev. 2010, 1, 1–38. [Google Scholar]
- Hossain, F. Global responsibility vs. individual dreams: Addressing ethical dilemmas created by the migration of healthcare practitioners. Glob. Bioeth. 2020, 31, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Michael, M.; Roth, K. Against all odds: A qualitative study of rehabilitation of persons with spinal cord injury in Afghanistan. Spinal Cord 2012, 50, 864–868. [Google Scholar] [CrossRef] [PubMed]
- The New Humanitarian. Sri Lankans Disabled by War, Forgotten in Peace. Available online: https://www.thenewhumanitarian.org/news/2015/09/16/sri-lankans-disabled-war-forgotten-peace (accessed on 16 September 2021).
- Gohy, B.; Ali, E.; Van den Bergh, R.; Schillberg, E.; Nasim, M.; Naimi, M.M.; Cheréstal, S.; Falipou, P.; Weerts, E.; Skelton, P.; et al. Early physical and functional rehabilitation of trauma patients in the Médecins Sans Frontières trauma centre in Kunduz, Afghanistan: Luxury or necessity? Int. Health 2016, 8, 381–389. [Google Scholar] [CrossRef] [Green Version]
- Barth, C.A. ICRC Physical Rehabilitation Programme. Evaluation of Former MoveAbility Operations, West. Africa: Benin, Ivory Coast, Togo; International Committee of the Red Cross: Geneva, Switzerland, 2020. [Google Scholar]
- The Africa Region of the World Confederation for Physical Therapy. Strategic Objectives—WCPT Africa Region. Available online: https://www.wcptafrica.org/about-us/strategic-objectives/ (accessed on 3 November 2021).
- Dirienzo, C.; Das, J. The Spillover Effects of Country Fragility in Africa. Focus 2017, 7, 62–67. [Google Scholar]
- World Health Organization. Rehabilitation. Available online: https://www.who.int/news-room/fact-sheets/detail/rehabilitation (accessed on 27 January 2020).
- Cieza, A.; Sabariego, C.; Bickenbach, J.; Chatterji, S. Rethinking Disability. BMC Med. 2018, 16, 10–14. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Universal Health Coverage. Available online: https://www.who.int/publications-detail/universal-health-coverage (accessed on 8 April 2020).
- United Nations Goal 3. Department of Economic and Social Affairs. Sustainable Developmet. Targets and Indicators 2015. Available online: https://sdgs.un.org/goals/goal3 (accessed on 14 June 2021).
- World Health Organization. Social Determinants of Health. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 13 September 2021).
- Skempes, D.; Bickenbach, J. Strengthening rehabilitation for people with disabilities: A human rights approach as the essential next step to accelerating global progress. Am. J. Phys. Med. Rehabil. 2015, 94, 823–828. [Google Scholar] [CrossRef] [Green Version]
- Krug, E.; Cieza, A. Strengthening health systems to provide rehabilitation services. Am. J. Phys. Med. Rehabil. 2017, 96, 438–439. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Demographics | |||
| Sex | Female 13/Male 18 (42% female) | ||
| Age range in years (median) | 25–68 (34) | ||
| Workplace | |||
| African Region | Algeria, Benin, DR Congo, Ethiopia, Guinea-Bissau, Ivory Coast, Madagascar, Mali, Niger, South Sudan, Sudan, Togo | ||
| Eastern Meditarranean Region | Afghanistan, Iraq, Lebanon | ||
| European Region | Switzerland * | ||
| South-East Asian Region | India, Myanmar | ||
| Western Pacific Region | Cambodia | ||
| Work Context (numbers of participants) | |||
| High-income country (1) | Switzerland * (1) | ||
| Low-resource context (7) | Benin (2), Guinea-Bissau (1), India (New Delhi) (1), Ivory Coast (1), Madagascar (1), Togo (1) | ||
| Hosting refugees from neighbouring countries (3) | Algeria (1), Lebanon (2) | ||
| Prolonged conflict (14) | Afghanistan (3), DR Congo (2), India (Kashmir) (1), Iraq (1), Mali (1), Myanmar (2), Niger (1), South Sudan (2), Sudan (1) | ||
| Post-conflict (6) | Cambodia (4), Ethiopia (2) | ||
| Profession | Female | Male | |
| Experience | <5 Years 5–10 Years >10 Years | 1 7 5 | 0 5 13 |
| Physiotherapy training | Assistant Diploma BSc MSc (MPH) PhD | 0 5 6 2 0 | 1 2 9 5 1 |
| Current role | Physiotherapist (clinician) Physiotherapist (clinician+) ** Physiotherapist (team leader) Project assistant Project manager/Advisor Teacher/Trainer | 6 3 1 1 2 0 | 9 2 3 1 1 2 |
| Topic | Time | Question |
|---|---|---|
| Ground rules | 10 min | What should every one of us do or respect in a group discussion? |
| Warm up | 5 min | Can you tell us your name, country and workplace? |
| Introductory question | 15 min | Is anyone happy to share his or her experience at the congress? |
| Guiding questions | 90–105 min | Based on experiences during the congress where do you see physiotherapy in your context in the next 10 years? What do you perceive as the priority health conditions that need to be addressed in your country and what is the role of physiotherapy in addressing these health priorities? What are the challenges and opportunities for the development of physiotherapy in your country? What is your role in addressing these challenges and harnessing opportunities? |
| Wrap-up | 15 min | Of all the things we’ve just discussed, what would you say are the most important conclusions you will take with you? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barth, C.A.; Donovan-Hall, M.; Blake, C.; Jahan Akhtar, N.; Capo-Chichi, J.M.; O’Sullivan, C. A Focus Group Study to Understand the Perspectives of Physiotherapists on Barriers and Facilitators to Advancing Rehabilitation in Low-Resource and Conflict Settings. Int. J. Environ. Res. Public Health 2021, 18, 12020. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212020
Barth CA, Donovan-Hall M, Blake C, Jahan Akhtar N, Capo-Chichi JM, O’Sullivan C. A Focus Group Study to Understand the Perspectives of Physiotherapists on Barriers and Facilitators to Advancing Rehabilitation in Low-Resource and Conflict Settings. International Journal of Environmental Research and Public Health. 2021; 18(22):12020. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212020
Chicago/Turabian StyleBarth, Cornelia Anne, Maggie Donovan-Hall, Catherine Blake, Noor Jahan Akhtar, Joseph Martial Capo-Chichi, and Cliona O’Sullivan. 2021. "A Focus Group Study to Understand the Perspectives of Physiotherapists on Barriers and Facilitators to Advancing Rehabilitation in Low-Resource and Conflict Settings" International Journal of Environmental Research and Public Health 18, no. 22: 12020. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212020