
Family Planning Uptake in Kagera and Mara Regions in Tanzania: A Cross-Sectional Community Survey


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Sampling and Population
2.3. Measurements and Variables
2.4. Data Collection
2.5. Statistical Analysis
2.6. Ethics Approval and Consent to Participate
3. Results
3.1. Characteristics of Participants
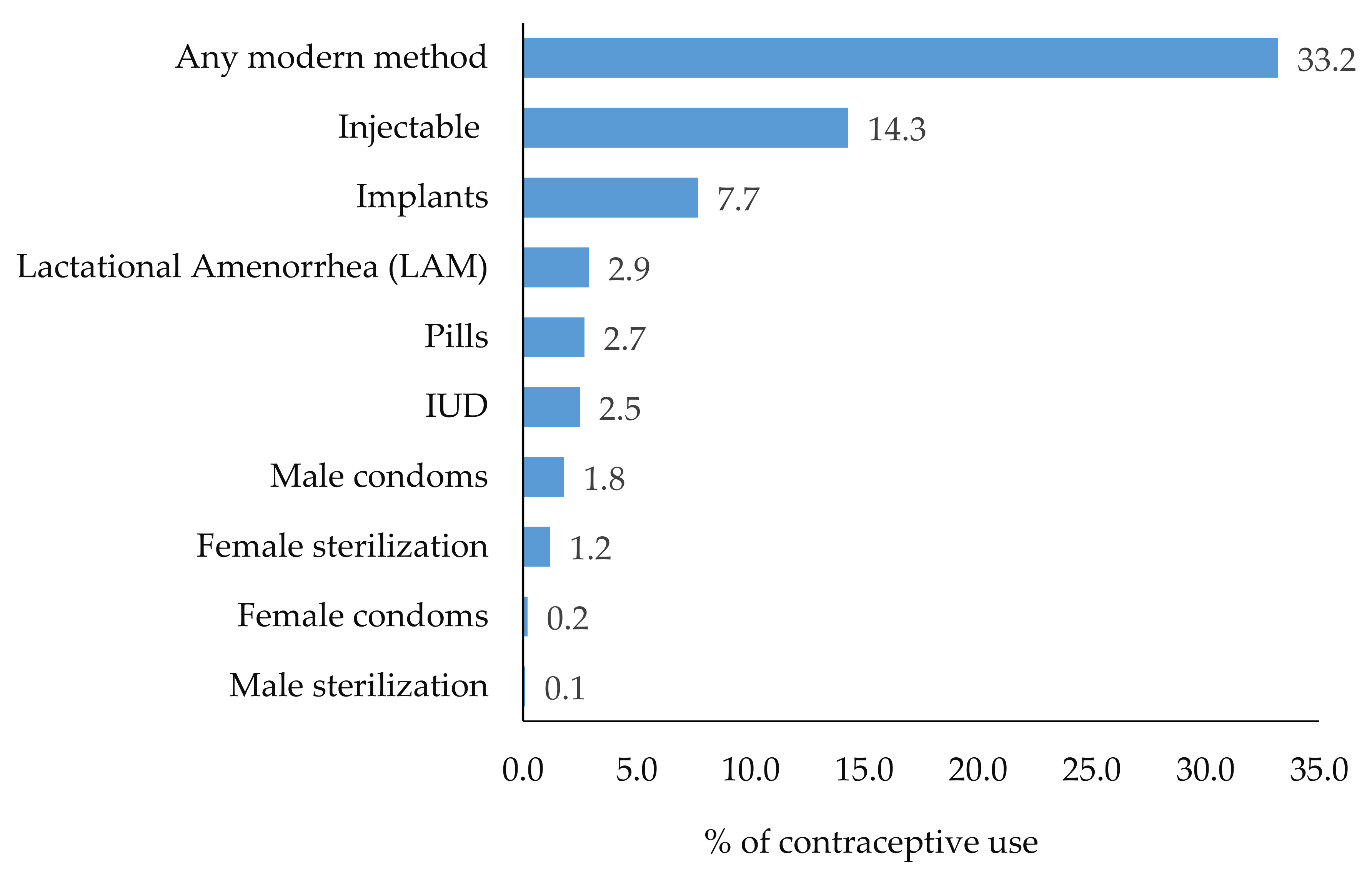
3.2. Prevalence of Family Planning Use
3.3. Factors Associated with Family Planning Use
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Variable | Discussed Family Planning with Male Partner | Chi-Square p-Value | ||
|---|---|---|---|---|
| No | Yes | Opted Not to Disclose | ||
| n (%) | n (%) | n (%) | ||
| Education | p = 0.124 | |||
| No Education | 54 (23.1) | 122 (52.1) | 58 (24.8) | |
| Primary and above | 274 (28.8) | 431 (45.4) | 245 (25.8) | |
| Age category | p = 0.559 | |||
| 15–24 | 143 (28.8) | 230 (46.4) | 123 (24.4) | |
| 25–34 | 138 (27.0) | 233 (45.5) | 141 (27.5) | |
| 35+ | 47 (26.7) | 90 (51.1) | 39 (22.2) | |
| Parity | p = 0.386 | |||
| 1 | 65 (26.4) | 126 (51.2) | 55 (22.4) | |
| 2 to 4 | 156 (28.7) | 239 (43.9) | 149 (27.4) | |
| 5+ | 107 (27.2) | 188 (47.7) | 99 (25.1) | |
| Wealth | p < 0.001 | |||
| Poor | 114 (29.8) | 163 (42.5) | 106 (27.7) | |
| Middle | 129 (33.2) | 162 (41.8) | 97 (25.0) | |
| Rich | 75 (19.9) | 206 (54.8) | 95 (25.3) | |
| Decision making on health | p < 0.01 | |||
| Alone | 31 (17.7) | 105 (60.0) | 39 (22.3) | |
| Jointly | 176 (30.3) | 254 (43.7) | 151 (26.0) | |
| Male partner/others alone | 121 (28.7) | 194 (46.1) | 106 (25.2) | |
Appendix B
| Variable | Total | Kagera | Mara | Chi-Square p-Value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Women reported male partner Participated on FP counseling | 0.33 | ||||||
| No | 1064 | 89.9 | 538 | 90.7 | 526 | 89.0 | |
| Yes | 120 | 10.1 | 55 | 9.3 | 65 | 11.0 | |
| Awareness on FP methods | <0.001 | ||||||
| No | 211 | 18.0 | 137 | 23.3 | 74 | 12.6 | |
| Yes | 964 | 82.0 | 452 | 76.7 | 512 | 87.4 | |
| FP discussion with male partner | <0.001 | ||||||
| No | 328 | 27.7 | 130 | 21.9 | 198 | 33.5 | |
| Yes | 550 | 46.5 | 326 | 55.0 | 224 | 37.9 | |
| Don’t want | 306 | 25.8 | 137 | 23.1 | 169 | 28.6 | |
| Discuss FP with Community Health Workers | 0.82 | ||||||
| No | 1082 | 91.4 | 543 | 91.6 | 539 | 91.2 | |
| Yes | 102 | 8.6 | 50 | 8.4 | 52 | 8.8 | |
| Discuss FP with health Facility worker | 0.82 | ||||||
| No | 751 | 63.4 | 422 | 71.2 | 329 | 55.7 | |
| Yes | 433 | 36.6 | 171 | 28.8 | 262 | 44.3 | |
| FP Counselling at ANC | <0.001 | ||||||
| No | 444 | 37.6 | 258 | 43.6 | 186 | 31.5 | |
| Yes | 738 | 62.4 | 334 | 56.4 | 404 | 68.5 | |
| Parity | 0.00 | ||||||
| 1 | 246 | 20.8 | 101 | 17.0 | 145 | 24.5 | |
| 2 to 4 | 544 | 46.0 | 276 | 46.5 | 268 | 45.4 | |
| 5+ | 394 | 33.3 | 216 | 36.4 | 178 | 30.1 | |
| State of being in union | 0.75 | ||||||
| In-union | 1004 | 87.5 | 499 | 87.9 | 505 | 87.2 | |
| Not in-union | 143 | 12.5 | 69 | 12.2 | 74 | 12.8 | |
| Education Status | 0.012 | ||||||
| No education | 234 | 19.8 | 101 | 17.0 | 133 | 22.5 | |
| Primary and above | 950 | 80.2 | 492 | 83.0 | 458 | 77.5 | |
| Age category | 0.07 | ||||||
| 15–24 | 496 | 41.9 | 255 | 43.0 | 241 | 40.8 | |
| 25–34 | 512 | 43.2 | 239 | 40.3 | 273 | 46.2 | |
| 35+ | 176 | 14.9 | 99 | 16.7 | 77 | 13.0 | |
| Decision making on health care | 0.20 | ||||||
| Women alone | 175 | 14.9 | 94 | 15.9 | 81 | 13.8 | |
| Jointly | 581 | 49.4 | 276 | 46.8 | 305 | 56.9 | |
| Male partner alone/others alone | 421 | 37.8 | 220 | 37.3 | 201 | 34.2 | |
References
- WHO/Jhpiego Postnatal Care for Mothers and Newborns Highlights from the World Health Organization 2013 Guidelines. In Postnatal Care Guidel; WHO: Geneva, Switzerland, 2015; pp. 1–8.
- Sedgh, G.; Singh, S.; Hussain, R. Intended and unintended pregnancies worldwide in 2012 and recent trends. Stud. Fam. Plann. 2014, 45, 301–314. [Google Scholar] [CrossRef] [Green Version]
- Cleland, J.; Bernstein, S.; Ezeh, A.; Faundes, A.; Glasier, A.; Innis, J. Family planning: The unfinished agenda. Lancet 2006, 368, 1810–1827. [Google Scholar] [CrossRef]
- WHO. Postnatal Care of the Mother and Newborn 2013; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Ross, J.A.; Winfrey, W.L. Contraceptive Use, Intention to Use and Unmet Need during the Extended Postpartum Period. Int. Fam. Plan. Perspect. 2001, 27, 20. [Google Scholar] [CrossRef]
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC); Ministry of Health (MoH); National Bureau of Statistics (NBS); Office of Chief Government Statistician (OCGS); ICF. 2016 Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015-16. Dar es Salaam, Tanzania, and Rockville, MD, USA, 2016. Available online: www.nbs.go.tz (accessed on 9 February 2021).
- National Bureau of Statistics (NBS) and ICF Macro. Tanzania Demographic and Health Survey 2010. Natl. Bur. Stat. Dar es Salaam, Tanzania ICF Macro Calverton, Maryland, USA 2011. pp. 1–482. Available online: www.nbs.go.tz (accessed on 9 February 2021).
- National Bureau of Statistics (NBS). Tanzania in Figures 2018. Dodoma. 2019. Available online: www.nbs.go.tz (accessed on 9 February 2021).
- Moreland, S.; Talbird, S.; U.S. Agency for International Development (USAID). Achieving the Millennium Development Goals: The Contribution of Fulfilling the Unmet Need for Family Planning; USAID: Washington DC, USA, 2006. [Google Scholar]
- Ministry of Health Community Development Gender Elderly and Children (MoHCDGEC) Tanzania. National Family Planning Costed Implementation Plan 2019–2023; MOHCDGEC: Dar es Salaam, Tanzania, 2019. [Google Scholar]
- WHO. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Do, M.; Hotchkiss, D. Relationships between antenatal and postnatal care and post-partum modern contraceptive use: Evidence from population surveys in Kenya and Zambia. BMC Health Serv. Res. 2013, 13, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Agha, S.; Williams, E. Does the antenatal care visit represent a missed opportunity for increasing contraceptive use in Pakistan? An analysis of household survey data from Sindh province. Health Policy Plan. 2016, 31, 325–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keogh, S.C.; Urassa, M.; Kumogola, Y.; Kalongoji, S.; Kimaro, D.; Zaba, B. Postpartum Contraception in Northern Tanzania: Patterns of Use, Relationship to Antenatal Intentions, and Impact of Antenatal Counseling. Stud. Fam. Plann. 2015, 46, 405–422. [Google Scholar] [CrossRef]
- Vural, F.; Vural, B.; Cakıroglu, Y. The effect of combined antenatal and postnatal counselling on postpartum modern contraceptive use: Prospective case-control study in Kocaeli, Turkey. J. Clin. Diagn. Res. 2016, 10, QC04–QC07. [Google Scholar] [CrossRef] [PubMed]
- Dona, A.; Abera, M.; Alemu, T.; Hawaria, D. Timely initiation of postpartum contraceptive utilization and associated factors among women of child bearing age in Aroressa District, Southern Ethiopia: A community based cross-sectional study. BMC Public Health 2018, 18, 1100. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, M.; Gilles, K.; Shattuck, D.; Kerner, B.; Guest, G. Changes in couples’ communication as a result of a male-involvement family planning intervention. J. Health Commun. 2012, 17, 802–819. [Google Scholar] [CrossRef]
- Osuafor, G.N.; Maputle, S.M.; Ayiga, N. Corrigendum: Factors related to married or cohabiting women’s decision to use modern contraceptive methods in Mafikeng, South Africa. Afr. J. Prim. Health Care Fam. Med. 2018, 10, 1998. [Google Scholar] [CrossRef] [Green Version]
- Babalola, S.; Oyenubi, O.; Speizer, I.S.; Cobb, L.; Akiode, A.; Odeku, M. Factors affecting the achievement of fertility intentions in urban Nigeria: Analysis of longitudinal data. BMC Public Health 2017, 17, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassa, M.; Abajobir, A.A.; Gedefaw, M. Level of male involvement and associated factors in family planning services utilization among married men in Debremarkos town, Northwest Ethiopia. BMC Int. Health Hum. Rights 2014, 14, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Khan, R.N.J.; Hashim, S.M.; Nawi, A.M.; Siraj, H.H. Factors associated with ever used of modern contraception among married men attending a primary healthcare clinic. Med. J. Malays. 2018, 73, 301–306. [Google Scholar]
- Kamal, N. The influence of husbands on contraceptive use by Bangladeshi women. Health Policy Plan. 2000, 15, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Abraha, T.H.; Belay, H.S.; Welay, G.M. Intentions on contraception use and its associated factors among postpartum women in Aksum town, Tigray region, northern Ethiopia: A community-based cross- sectional study. Reprod. Health 2018, 15, 188. [Google Scholar] [CrossRef]
- Asaolu, I.O.; Okafor, C.T.; Ehiri, J.C.; Dreifuss, H.M.; Ehiri, J.E. Association between Measures of Women’s Empowerment and Use of Modern Contraceptives: An Analysis of Nigeria’s Demographic and Health Surveys. Front. Public Health 2017, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Mboane, R.; Bhatta, M.P. Influence of a husband’s healthcare decision making role on a woman’s intention to use contraceptives among Mozambican women. Reprod. Health 2015, 12, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Mosha, I.; Ruben, R.; Kakoko, D. Family planning decisions, perceptions and gender dynamics among couples in Mwanza, Tanzania: A qualitative study. BMC Public Health 2013, 13, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuler, S.R.; Rottach, E.; Mukiri, P. Gender norms and family planning decision-making in Tanzania: A qualitative study. J. Public Health Afr. 2011, 2, 102–107. [Google Scholar] [CrossRef] [Green Version]
- Sundararajan, R.; Yoder, L.M.; Kihunrwa, A.; Aristide, C.; Kalluvya, S.E.; Downs, D.J.; Mwakisole, A.H.; Downs, J.A. How gender and religion impact uptake of family planning: Results from a qualitative study in Northwestern Tanzania. BMC Women’s Health 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Srikanthan, A.; Reid, R.L. Religious and Cultural Influences on Contraception. J. Obstet. Gynaecol. Can. 2008, 30, 129–137. [Google Scholar] [CrossRef]
- Abdi, B.; Okal, J.; Serour, G.; Temmerman, M. “Children are a blessing from God”—A qualitative study exploring the socio-cultural factors influencing contraceptive use in two Muslim communities in Kenya. Reprod. Health 2020, 17, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabagenyi, A.; Reid, A.; Ntozi, J.; Atuyambe, L. Socio-cultural inhibitors to use of modern contraceptive techniques in rural Uganda: A qualitative study. Pan Afr. Med. J. 2016, 25, 78. [Google Scholar] [CrossRef] [PubMed]
- De Vargas Nunes Coll, C.; Ewerling, F.; Hellwig, F.; De Barros, A.J.D. Contraception in adolescence: The influence of parity and marital status on contraceptive use in 73 low-and middle-income countries. Reprod. Health 2019, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Apanga, P.A.; Kumbeni, M.T.; Ayamga, E.A.; Ulanja, M.B.; Akparibo, R. Prevalence and factors associated with modern contraceptive use among women of reproductive age in 20 African countries: A large population-based study. BMJ Open 2020, 10, 1–12. [Google Scholar] [CrossRef]
- Mekonnen, W.; Worku, A. Determinants of low family planning use and high unmet need in Butajira District, South Central Ethiopia. Reprod. Health 2011, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kanma-Okafor, O.J.; Asuquo, E.J.I.M.; Balogun, M.R.A.O. Utilisation and Preferences of Family Planning Services among Women in Ikosi-Isheri, Kosofe Local Government Area, Lagos, Nigeria. Niger. Postgrad Med. J. 2019, 26, 182–188. [Google Scholar] [CrossRef]
- Agadjanian, V.; Hayford, S.R.; Luz, L.; Yao, J. Bridging user and provider perspectives: Family planning access and utilization in rural Mozambique. Int. J. Gynecol. Obstet. 2015, 130, e47–e51. [Google Scholar] [CrossRef] [Green Version]
- Schultz, C.; Larrea, N.; Celada, M.; Heinrichs, G. A Qualitative Assessment of Community Attitudes and Barriers to Family Planning Use in the Trifinio Region of Southwest Guatemala. Matern. Child Health J. 2018, 22, 461–466. [Google Scholar] [CrossRef]
- Semachew Kasa, A.; Tarekegn, M.; Embiale, N. Knowledge, attitude and practice towards family planning among reproductive age women in a resource limited settings of Northwest Ethiopia. BMC Res. Notes 2018, 11, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Mustafa, G.; Azmat, S.K.; Hameed, W.; Ali, S.; Ishaque, M.; Hussain, W.; Ahmed, A.; Munroe, E. Family Planning Knowledge, Attitudes, and Practices among Married Men and Women in Rural Areas of Pakistan: Findings from a Qualitative Need Assessment Study. Int. J. Reprod. Med. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabagenyi, A.; Jennings, L.; Reid, A.; Nalwadda, G.; Ntozi, J.; Atuyambe, L. Barriers to male involvement in contraceptive uptake and reproductive health services: A qualitative study of men and women’s perceptions in two rural districts in Uganda. Reprod. Health 2014, 11, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spagnoletti, B.R.M.; Bennett, L.R.; Kermode, M.; Wilopo, S.A. “I wanted to enjoy our marriage first... but I got pregnant right away”: A qualitative study of family planning understandings and decisions of women in urban Yogyakarta, Indonesia. BMC Pregnancy Childbirth 2018, 18, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Izugbara, C.; Ibisomi, L.; Ezeh, A.C.; Mandara, M. Gendered interests and poor spousal contraceptive communication in Islamic northern Nigeria. J. Fam. Plan. Reprod. Health Care 2010, 36, 219–224. [Google Scholar] [CrossRef] [Green Version]
- Mansor, M.; San, S.O.; Abdullah, K.L. Prevalence of Family Planning Practices among Women Influenced by Husband’s Socio Demography and Decision Making. J. Sains Kesihat. Malays. 2015, 13, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Bishanga, D.R.; Massenga, J.; Mwanamsangu, A.H.; Kim, Y.M.; Eorge, J.; Kapologwe, N.A.; Zoungrana, J.; Rwegasira, M.; Kols, A.; Hill, K.; et al. Women’s experience of facility-based childbirth care and receipt of an early postnatal check for herself and her newborn in Northwestern Tanzania. Int. J. Environ. Res. Public Health 2019, 16, 481. [Google Scholar] [CrossRef] [Green Version]
- Jhpiego, ICF/Macro International Inc.; John Snow Inc. Save the Children. Maternal and Child Survival Program (MCSP); Year 1 Implementation Plan June 2014–September 2015; Jhpiego: Dar es Salaam, Tanzania, 2015. [Google Scholar]
- Bishanga, D.R.; Drake, M.; Kim, Y.M.; Mwanamsangu, A.H.; Makuwani, A.M.; Zoungrana, J.; Lemwayi, R.; Rijken, M.J.; Stekelenburg, J. Factors associated with institutional delivery: Findings from a cross-sectional study in Mara and Kagera regions in Tanzania. PLoS ONE 2018, 13, e0209672. [Google Scholar] [CrossRef] [PubMed]
- United States Agency for International Development (USAID) Bureau for Global Health. Child Survival and Health Grants Program; USAID: Washington, DC, USA, 2002; p. 192. [Google Scholar]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Shahidul Islam, M.; Shafiul Alam, M.; Mahedi Hasan, M. Inter-spousal communication on family planning and its effect on contraceptive use and method choice in Bangladesh. Asian Soc. Sci. 2014, 10, 189–201. [Google Scholar] [CrossRef]
- Do, M.; Kurimoto, N. Women’s empowerment and choice of contraceptive methods in selected African countries. Int. Perspect. Sex. Reprod. Health 2012, 38, 23–33. [Google Scholar] [CrossRef]
- Wolff, B.; Blanc, A.K.; Ssekamatte-Ssebuliba, J. The Role of Couple Negotiation in Unmet Need for Contraception and the Decision to Stop Childbearing in Uganda. Stud. Fam. Plann. 2000, 31, 124–137. [Google Scholar] [CrossRef]
- Rizkianti, A.; Afifah, T.; Saptarini, I.; Rakhmadi, M.F. Women’s decision-making autonomy in the household and the use of maternal health services: An Indonesian case study. Midwifery 2020, 90, 102816. [Google Scholar] [CrossRef] [PubMed]
- Ghose, B.; Feng, D.; Tang, S.; Yaya, S.; He, Z.; Udenigwe, O.; Ghosh, S.; Feng, Z. Women’s decision-making autonomy and utilisation of maternal healthcare services: Results from the Bangladesh Demographic and Health Survey. BMJ Open 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ameyaw, E.K.; Tanle, A.; Kissah-Korsah, K.; Amo-Adjei, J. Women’s Health Decision-Making Autonomy and Skilled Birth Attendance in Ghana. Int. J. Reprod. Med. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.M.; Kols, A.; Mwarogo, P.; Awasum, D. Differences in counseling men and women: Family planning in Kenya. Patient Educ. Couns. 2000, 39, 37–47. [Google Scholar] [CrossRef]
- Wegner, M.N.; Landry, E.; Wilkinson, D.; Tzanis, J. Men as Partners in Reproductive Health: From Issues to Action. Int. Fam. Plan. Perspect. 1998, 24, 38–42. [Google Scholar] [CrossRef]
- Bustamante-Forest, R.; Giarratano, G. Changing men’s involvement in reproductive health and family planning. Nurs. Clin. N. Am. 2004, 39, 301–318. [Google Scholar] [CrossRef]
- Kejela, G. The Role of Male Involvement in Modern Family Planning Utilization and Associated Factors in Arba Minch Town, Gamo Gofa Zone, Ethiopia. Eur. J. Prev. Med. 2017, 5, 39. [Google Scholar] [CrossRef] [Green Version]
- Barber, S.L. Family Planning Advice and Postpartum Contraceptive Use Among Low-Income Women in Mexico. Int. Fam. Plan. Perspect. 2007, 33, 6–12. [Google Scholar] [CrossRef]
- Frumence, G.; Goodman, M.; Chebet, J.J.; Mosha, I.; Bishanga, D.; Chitama, D.; Winch, P.J.; Killewo, J.; Baqui, A.H. Factors affecting early identification of pregnant women by community health workers in Morogoro, Tanzania. BMC Public Health 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Mazzei, A.; Ingabire, R.; Mukamuyango, J.; Nyombayire, J.; Sinabamenye, R.; Bayingana, R.; Parker, R.; Tichacek, A.; Easter, S.R.; Karita, E.; et al. Community health worker promotions increase uptake of long-acting reversible contraception in Rwanda. Reprod. Health 2019, 16, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, M.I.; Johns, N.E.; Quinn, A.K.; Boyce, S.C.; Fatouma, I.A.; Oumarou, A.O.; Sani, A.; Silverman, J.G. Can community health workers increase modern contraceptive use among young married women? A cross-sectional study in rural Niger. Reprod. Health 2019, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lutalo, T.; Kigozi, G.; Kimera, E.; Serwadda, D.; Wawer, M.J.; Zabin, L.S.; Gray, R.H. A randomized community trial of enhanced family planning outreach in Rakai, Uganda. Stud. Fam. Plann. 2010, 41, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Tappis, H.; Kazi, A.; Hameed, W.; Dahar, Z.; Ali, A.; Agha, S. The role of quality health services and discussion about birth spacing in postpartum contraceptive use in Sindh, Pakistan: A multilevel analysis. PLoS ONE 2015, 10, e0139628. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Social Welfare (MOHSW). National Family Planning Guidelines and Standards; Ministry of Health and Social Welfare (MOHSW): Dar es Salaam, Tanzania, 2013. [Google Scholar]
- Belda, S.S.; Haile, M.T.; Melku, A.T.; Tololu, A.K. Modern contraceptive utilization and associated factors among married pastoralist women in Bale eco-region, Bale Zone, South East Ethiopia. BMC Health Serv. Res. 2017, 17, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakew, Y.; Reda, A.A.; Tamene, H.; Benedict, S.; Deribe, K. Geographical variation and factors influencing modern contraceptive use among married women in Ethiopia: Evidence from a national population based survey. Reprod. Health 2013, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medhanyie, A.; Spigt, M.; Kifle, Y.; Schaay, N.; Sanders, D.; Blanco, R. The role of health extension workers in improving utilization of maternal health services in rural areas in Ethiopia: A cross sectional study. BMC Health Serv. Res. 2012, 12, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabagenyi, A.; Ndugga, P.; Wandera, S.O.; Kwagala, B. Modern contraceptive use among sexually active men in Uganda: Does discussion with a health worker matter? BMC Public Health 2014, 14, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puri, M.C.; Maharjan, M.; Pearson, E.; Pradhan, E.; Dhungel, Y.; Khadka, A.; Shah, I.H. Delivering postpartum family planning services in Nepal: Are providers supportive? BMC Health Serv. Res. 2018, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- LeFevre, A.; Mpembeni, R.; Kilewo, C.; Yang, A.; An, S.; Mohan, D.; Mosha, I.; Besana, G.; Lipingu, C.; Callaghan-Koru, J.; et al. Program assessment of efforts to improve the quality of postpartum counselling in health centers in Morogoro region, Tanzania. BMC Pregnancy Childbirth 2018, 18, 1–13. [Google Scholar] [CrossRef]

| Variable | n | % |
|---|---|---|
| Age * | ||
| 15–24 | 496 | 41.9 |
| 25–34 | 512 | 43.2 |
| 35+ | 176 | 14.9 |
| Education * | ||
| No education | 234 | 19.8 |
| Primary and above | 950 | 80.2 |
| State of being in union with male Partner * | ||
| Not in union | 143 | 12.1 |
| In union | 1004 | 84.8 |
| Parity * | ||
| 1 | 246 | 20.8 |
| 2–4 | 544 | 45.9 |
| 5+ | 394 | 33.3 |
| Maternity Care Utilization | ||
| Antenatal care attendance * | ||
| Never | 68 | 5.7 |
| 1–3 visits | 485 | 41.0 |
| 4+ visits | 631 | 53.3 |
| Family planning counselling during antenatal care ** | ||
| No | 444 | 37.5 |
| Yes | 738 | 62.3 |
| Discussed family planning with community health worker * | ||
| No | 1082 | 91.4 |
| Yes | 102 | 8.6 |
| Discussed family planning with facility based health worker * | ||
| No | 751 | 63.4 |
| Yes | 433 | 36.6 |
| Partner accompany to ANC ** | ||
| No | 497 | 42.0 |
| Yes | 680 | 57.4 |
| Partner participated in family planning counselling ** | ||
| No | 1064 | 89.9 |
| Yes | 120 | 10.1 |
| Knowledge On Family Planning | ||
| Being able to mention at least one family planning method * | ||
| Not able to mention any method | 211 | 17.8 |
| Mentioned at least one method | 964 | 81.4 |
| Exposure to media * | ||
| No exposure to tv, radio & newspapers | 291 | 24.6 |
| Exposed to at least one media source | 659 | 55.7 |
| Gender Related Factors | ||
| Discuss family planning with partner ** | ||
| No | 553 | 46.7 |
| Yes | 328 | 27.7 |
| Opted not to disclose whether they discussed or not | 303 | 25.6 |
| Need husband/partner’s approval to use family planning ** | ||
| No | 248 | 21.0 |
| Yes | 929 | 78.5 |
| Decision-making in healthcare * | ||
| Woman alone | 175 | 14.8 |
| Jointly | 581 | 49.1 |
| Male partner alone/others alone | 421 | 35.6 |
| Variable | Family Planning Use | Bivariate | Multivariate | ||
|---|---|---|---|---|---|
| Yes | % | OR (95% CI) | p-Value | aOR (95% CI) | |
| Age | |||||
| 15–24 | 155 | 31.3 | 1 | 1 | |
| 25–34 | 176 | 34.4 | 1.17(0.88–1.54) | 0.29 | 1.34 (0.91–1.99) |
| 35+ | 47 | 26.7 | 0.78 (0.51–1.17) | 0.23 | 0.91 (0.53–1.58) |
| Education | |||||
| No education | 56 | 23.9 | 1 | 1 | |
| Primary and above | 322 | 33.9 | 1.52 (1.06–2.19) | 0.02 | 1.66 (1.01–2.73) |
| State of being in union/or not * | |||||
| Not in union | 37 | 25.9 | 1 | 1 | |
| In union | 335 | 33.4 | 1.61 (1.04–2.47) | 0.03 | 1.86 (1.02–3.42) |
| Region | |||||
| Mara | 150 | 25.3 | 1 | 1 | |
| Kagera | 228 | 38.6 | 1.96(1.34–2.89) | 0.001 | 1.65 (0.89–3.04) |
| Parity | |||||
| 1 | 72 | 29.3 | 1 | ||
| 2–4 | 188 | 34.6 | 1.31 (0.92–1.87) | 0.13 | |
| 5+ | 118 | 30.0 | 1.11 (0.76–1.62) | 0.58 | |
| Antenatal care attendance | |||||
| Never | 24 | 35.3 | 1 | ||
| 1–3 | 137 | 28.3 | 0.83 (0.47–1.47) | 0.53 | |
| 4+ | 217 | 34.4 | 1.05 (0.60–1.83) | 0.88 | |
| Family planning counseling during antenatal care * | |||||
| No | 84 | 18.9 | 1 | 1 | |
| Yes | 293 | 39.7 | 3.01 (2.22–4.09) | <0.001 | 2.68 (1.78–4.05) |
| Discussed family planning with community health worker | |||||
| No | 317 | 29.3 | 1 | 1 | |
| Yes | 61 | 59.8 | 3.42 (2.18–5.38) | <0.001 | 4.59 (2.53–8.33) |
| Discussed family planning with facility health worker | |||||
| No | 167 | 22.2 | 1 | 1 | |
| Yes | 211 | 48.7 | 3.88 (2.91–5.18) | <0.001 | 1.93 (1.29–2.90) |
| Partner company to antenatal care * | |||||
| No | 129 | 26 | 1 | 1 | |
| Yes | 245 | 36 | 1.43 (1.08–1.89) | 0.01 | 1.26 (0.84–1.90) |
| Partner participated in family planning counseling | |||||
| No | 307 | 28.9 | 1 | 1 | |
| Yes | 71 | 59.2 | 4.03 (2.62–6.19) | <0.001 | 0.97 (0.56–1.67) |
| Being able to mention at least one family planning method | |||||
| Not able to mention any family planning method | 50 | 23.7 | 1 | 1 | |
| Mentioned at least one family planning method | 328 | 34.0 | 1.63 (1.12–2.37) | 0.01 | 1.10 (0.66–1.83) |
| Exposure to media * | |||||
| No exposure to tv, radio & newspapers | 85 | 29.2 | 1 | ||
| Exposed to atleast one media source | 237 | 36.0 | 1.19 (0.85–1.66) | 0.32 | |
| Discussed family planning with partner | |||||
| No | 63 | 11.4 | 1 | 1 | |
| Yes | 119 | 36.3 | 3.72 (2.52–5.49) | <0.001 | 3.22 (1.99–5.21) |
| Opted not to disclose | 196 | 64.7 | 27.51 (17.53–43.17) | <0.001 | 24.19 (13.62–42.95) |
| Need husband/partner approval to * use family planning | |||||
| No | 67 | 27 | 1 | ||
| Yes | 307 | 33.1 | 1.25 (0.89–1.74) | 0.20 | |
| Decision-making in healthcare * | |||||
| Woman alone | 126 | 33.7 | 1 | ||
| Jointly | 86 | 23.0 | 0.97 (0.67–1.41) | 0.87 | |
| Male partner alone/others alone | 162 | 43.3 | 1.01 (0.73–1.40) | 0.94 | |
| Random effects | |||||
| (ςu)2 | 0.94 | ||||
| ICC | 0.23 | ||||
| Model fitness | |||||
| Likelihood value | −448.67 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massenga, J.; Noronha, R.; Awadhi, B.; Bishanga, D.R.; Safari, O.; Njonge, L.; Kim, Y.-M.; Roosmalen, J.v.; van den Akker, T. Family Planning Uptake in Kagera and Mara Regions in Tanzania: A Cross-Sectional Community Survey. Int. J. Environ. Res. Public Health 2021, 18, 1651. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041651
Massenga J, Noronha R, Awadhi B, Bishanga DR, Safari O, Njonge L, Kim Y-M, Roosmalen Jv, van den Akker T. Family Planning Uptake in Kagera and Mara Regions in Tanzania: A Cross-Sectional Community Survey. International Journal of Environmental Research and Public Health. 2021; 18(4):1651. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041651
Chicago/Turabian StyleMassenga, Joseph, Rita Noronha, Bayoum Awadhi, Dunstan R. Bishanga, Oliva Safari, Lusekelo Njonge, Young-Mi Kim, Jos van Roosmalen, and Thomas van den Akker. 2021. "Family Planning Uptake in Kagera and Mara Regions in Tanzania: A Cross-Sectional Community Survey" International Journal of Environmental Research and Public Health 18, no. 4: 1651. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041651