
Trends and Inequalities in Overall and Abdominal Obesity by Sociodemographic Factors in Korean Adults, 1998–2018



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Overall and Abdominal Obesity
2.3. Sociodemographic Variables
2.4. Statistical Analysis
3. Results
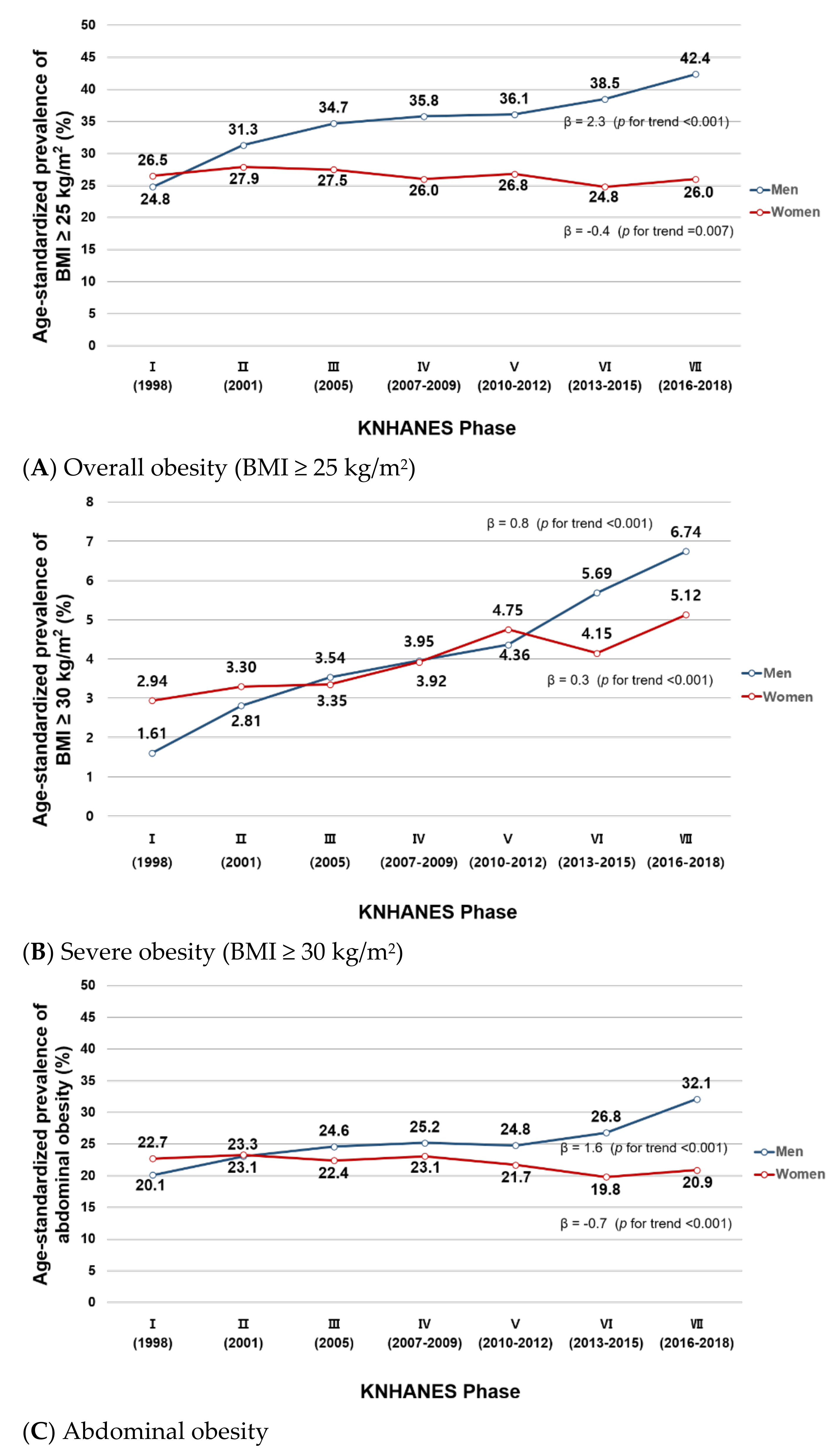
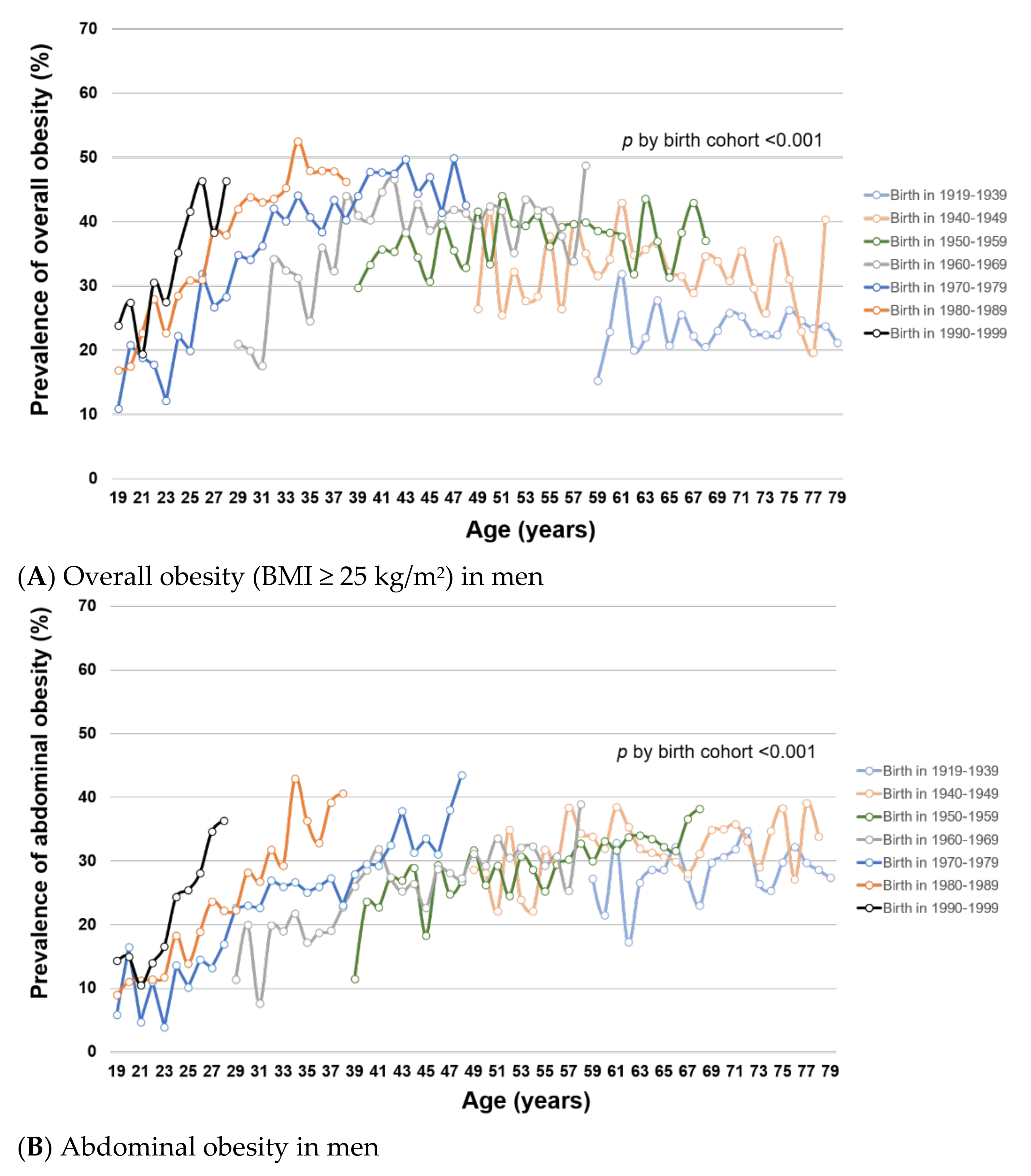
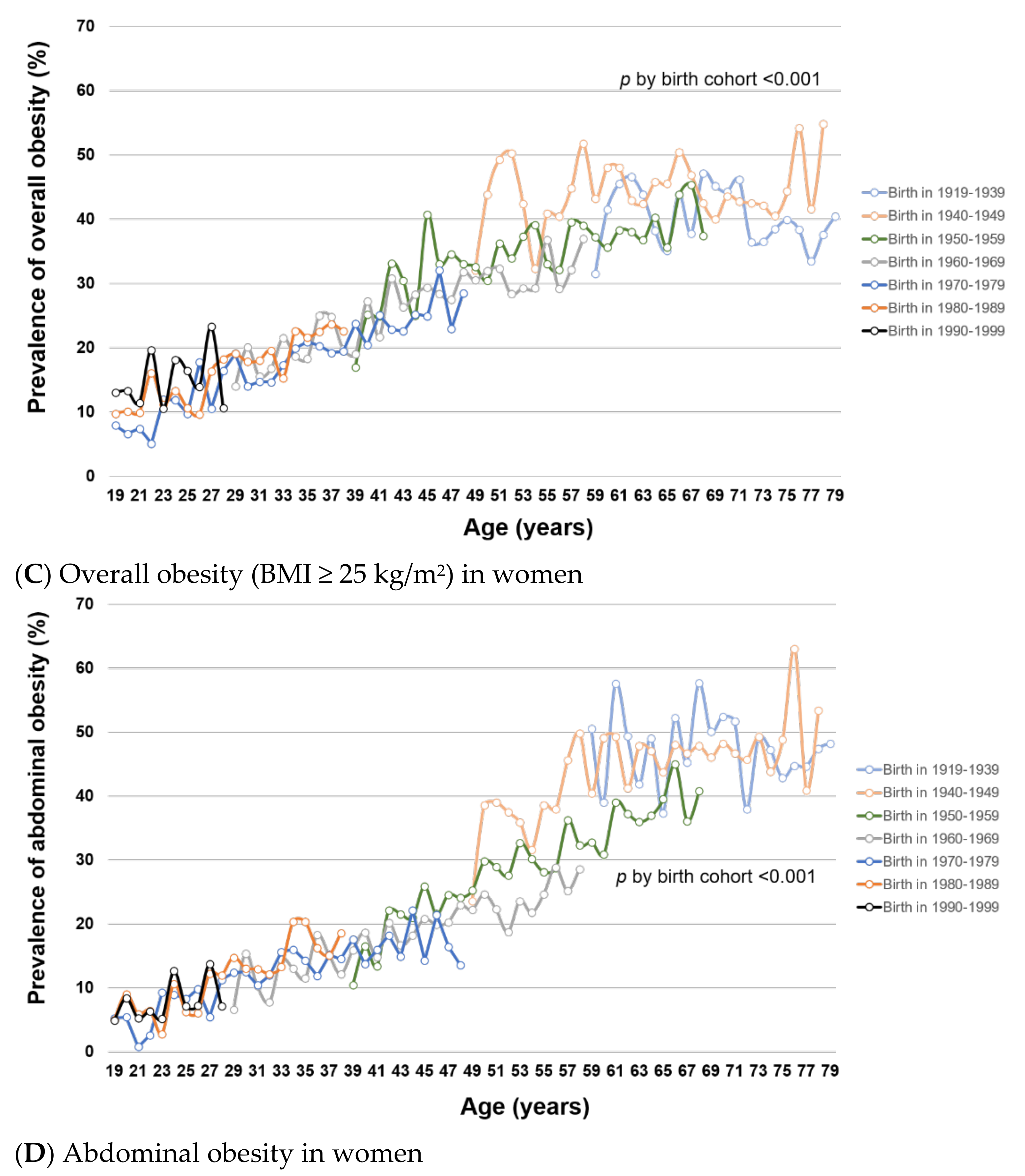
3.1. Trends of Overall and Abdominal Obesity in 1998–2018
3.2. Assocation between Socioeconoic Factors and Obesity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murphy, N.F.; MacIntyre, K.; Stewart, S.; Hart, C.L.; Hole, D.; McMurray, J.J. Long-term cardiovascular consequences of obesity: 20-year follow-up of more than 15,000 middle-aged men and women (the Renfrew-Paisley study). Eur. Heart J. 2006, 27, 96–106. [Google Scholar] [CrossRef]
- Calle, E.E.; Rodriguez, C.; Walker-Thurmond, K.; Thun, M.J. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N. Engl. J. Med. 2003, 348, 1625–1638. [Google Scholar] [CrossRef]
- Cloostermans, L.; Wendel-Vos, W.; Doornbos, G.; Howard, B.; Craig, C.L.; Kivimäki, M.; Tabak, A.G.; Jefferis, B.J.; Ronkainen, K.; Brown, W.J.; et al. Independent and combined effects of physical activity and body mass index on the development of Type 2 Diabetes—A meta-analysis of 9 prospective cohort studies. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 147. [Google Scholar] [CrossRef]
- Logue, J.; Murray, H.M.; Welsh, P.; Shepherd, J.; Packard, C.; Macfarlane, P.; Cobbe, S.; Ford, I.; Sattar, N. Obesity is associated with fatal coronary heart disease independently of traditional risk factors and deprivation. Heart 2011, 97, 564–568. [Google Scholar] [CrossRef]
- Després, J.P.; Lemieux, I. Abdominal obesity and metabolic syndrome. Nature 2006, 444, 881–887. [Google Scholar] [CrossRef]
- Park, M.H.; Falconer, C.; Viner, R.M.; Kinra, S. The impact of childhood obesity on morbidity and mortality in adulthood: A systematic review. Obes. Rev. 2012, 13, 985–1000. [Google Scholar] [CrossRef]
- Noori, N.; Hosseinpanah, F.; Nasiri, A.A.; Azizi, F. Comparison of overall obesity and abdominal adiposity in predicting chronic kidney disease incidence among adults. J. Ren. Nutr. 2009, 19, 228–237. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Flegal, K.M.; Carroll, M.D.; Kit, B.K.; Ogden, C.L. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. JAMA 2012, 307, 491–497. [Google Scholar] [CrossRef]
- Wang, Y.; Beydoun, M.A. The obesity epidemic in the United States--Gender, age, socioeconomic, racial/ethnic, and geographic characteristics: A systematic review and meta-regression analysis. Epidemiol. Rev. 2007, 29, 6–28. [Google Scholar] [CrossRef]
- Asia Pacific Cohort Studies Collaboration. The burden of overweight and obesity in the Asia-Pacific region. Obes. Rev. 2007, 8, 191–196. [Google Scholar] [CrossRef]
- Lim, H.; Lee, H.J.; Choue, R.; Wang, Y. Trends in Fast-Food and Sugar-Sweetened Beverage Consumption and Their Association with Social Environmental Status in South Korea. J. Acad. Nutr. Diet. 2018, 118, 1228–1236. [Google Scholar] [CrossRef]
- Kim, S.; Moon, S.; Popkin, B.M. The nutrition transition in South Korea. Am. J. Clin. Nutr. 2000, 71, 44–53. [Google Scholar] [CrossRef]
- Wyne, M.; Lee, M.I.N.; Moon, S.O.O. Fast-food consumption in South Korea. J. Consum. Stud. Home Econ. 2007, 18, 279–291. [Google Scholar] [CrossRef]
- Lim, S.; Shin, H.; Song, J.H.; Kwak, S.H.; Kang, S.M.; Won Yoon, J.; Choi, S.H.; Cho, S.I.; Park, K.S.; Lee, H.K.; et al. Increasing prevalence of metabolic syndrome in Korea: The Korean National Health and Nutrition Examination Survey for 1998–2007. Diabetes Care 2011, 34, 1323–1328. [Google Scholar] [CrossRef]
- Kang, H.T.; Shim, J.Y.; Lee, H.R.; Park, B.J.; Linton, J.A.; Lee, Y.J. Trends in prevalence of overweight and obesity in Korean adults, 1998–2009: The Korean National Health and Nutrition Examination Survey. J. Epidemiol. 2014, 24, 109–116. [Google Scholar] [CrossRef]
- Kim, C.S.; Ko, S.H.; Kwon, H.S.; Kim, N.H.; Kim, J.H.; Lim, S.; Choi, S.H.; Song, K.H.; Won, J.C.; Kim, D.J.; et al. Prevalence, awareness, and management of obesity in Korea: Data from the Korea national health and nutrition examination survey (1998–2011). Diabetes Metab. J. 2014, 38, 35–43. [Google Scholar] [CrossRef]
- Lim, J.; Park, H.S. Trends in the prevalence of underweight, obesity, abdominal obesity and their related lifestyle factors in Korean young adults, 1998–2012. Obes. Res. Clin. Pract. 2018, 12, 358–364. [Google Scholar] [CrossRef]
- Rhee, S.Y.; Park, S.W.; Kim, D.J.; Woo, J. Gender disparity in the secular trends for obesity prevalence in Korea: Analyses based on the KNHANES 1998–2009. Korean J. Intern. Med. 2013, 28, 29–34. [Google Scholar] [CrossRef]
- Shin, H.Y.; Kang, H.T. Recent trends in the prevalence of underweight, overweight, and obesity in Korean adults: The Korean National Health and Nutrition Examination Survey from 1998 to 2014. J. Epidemiol. 2017, 27, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Sobal, J.; Stunkard, A.J. Socioeconomic status and obesity: A review of the literature. Psychol. Bull. 1989, 105, 260–275. [Google Scholar] [CrossRef] [PubMed]
- McLaren, L. Socioeconomic status and obesity. Epidemiol. Rev. 2007, 29, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Conde, W.L.; Lu, B.; Popkin, B.M. Obesity and inequities in health in the developing world. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, NSW, Australia, 2000. [Google Scholar]
- Seo, M.H.; Lee, W.Y.; Kim, S.S.; Kang, J.H.; Kang, J.H.; Kim, K.K.; Kim, B.Y.; Kim, Y.H.; Kim, W.J.; Kim, E.M.; et al. 2018 Korean Society for the Study of Obesity Guideline for the Management of Obesity in Korea. J. Obes. Metab. Syndr. 2019, 28, 40–45. [Google Scholar] [CrossRef]
- Mueller, C.W.; Parcel, T.L. Measures of Socioeconomic Status: Alternatives and Recommendations. Child. Dev. 1981, 52, 13–30. [Google Scholar] [CrossRef]
- Baker, E.H. Socioeconomic Status, Definition. The Wiley Blackwell Encyclopedia of Health, Illness, Behavior, and Society; John Wiley & Sons, Ltd.: Chicester, UK, 2014; pp. 2210–2214. [Google Scholar]
- OECD. Framework for Integrated Analysis; OECD: Paris, France, 2013. [Google Scholar]
- Wagner, A.K.; Soumerai, S.B.; Zhang, F.; Ross-Degnan, D. Segmented regression analysis of interrupted time series studies in medication use research. J. Clin. Pharm. Ther. 2002, 27, 299–309. [Google Scholar] [CrossRef]
- Devaux, M.; Sassi, F. Social inequalities in obesity and overweight in 11 OECD countries. Eur. J. Public Health 2013, 23, 464–469. [Google Scholar] [CrossRef]
- Ogden, C.L.; Fakhouri, T.H.; Carroll, M.D.; Hales, C.M.; Fryar, C.D.; Li, X.; Freedman, D.S. Prevalence of Obesity Among Adults, by Household Income and Education—United States, 2011–2014. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 1369–1373. [Google Scholar] [CrossRef]
- Ogden, C.L.; Carroll, M.D.; Fakhouri, T.H.; Hales, C.M.; Fryar, C.D.; Li, X.; Freedman, D.S. Prevalence of Obesity Among Youths by Household Income and Education Level of Head of Household—United States 2011–2014. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 186–189. [Google Scholar] [CrossRef]
- Kim, T.H.; Park, Y.; Myung, J.; Han, E. Food price trends in South Korea through time series analysis. Public Health 2018, 165, 67–73. [Google Scholar] [CrossRef]
- Yatsuya, H.; Li, Y.; Hilawe, E.H.; Ota, A.; Wang, C.; Chiang, C.; Zhang, Y.; Uemura, M.; Osako, A.; Ozaki, Y.; et al. Global trend in overweight and obesity and its association with cardiovascular disease incidence. Circ. J. 2014, 78, 2807–2818. [Google Scholar] [CrossRef]
- Imoisili, O.E.; Sumner, A.E. Preventing Diabetes and Atherosclerosis in Sub-Saharan Africa: Should the Metabolic Syndrome Have a Role? Curr. Cardiovasc. Risk Rep. 2009, 3, 161–167. [Google Scholar] [CrossRef]
- Brewis, A.A. Stigma and the perpetuation of obesity. Soc. Sci. Med. 2014, 118, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Brewis, A.A.; Wutich, A. Explicit versus implicit fat-stigma. Am. J. Hum. Biol. 2012, 24, 332–338. [Google Scholar] [CrossRef]
- Puhl, R.M.; Heuer, C.A. Obesity stigma: Important considerations for public health. Am. J. Public Health 2010, 100, 1019–1028. [Google Scholar] [CrossRef]
- Wu, Y.K.; Berry, D.C. Impact of weight stigma on physiological and psychological health outcomes for overweight and obese adults: A systematic review. J. Adv. Nurs. 2018, 74, 1030–1042. [Google Scholar] [CrossRef]
- Brewis, A.A.; Han, S.Y.; SturtzSreetharan, C.L. Weight, gender, and depressive symptoms in South Korea. Am. J. Hum. Biol. 2017, 29. [Google Scholar] [CrossRef]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef]
- Pereira-Miranda, E.; Costa, P.R.F.; Queiroz, V.A.O.; Pereira-Santos, M.; Santana, M.L.P. Overweight and Obesity Associated with Higher Depression Prevalence in Adults: A Systematic Review and Meta-Analysis. J. Am. Coll. Nutr. 2017, 36, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Milaneschi, Y.; Simmons, W.K.; van Rossum, E.F.C.; Penninx, B.W. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef] [PubMed]
- Campos-Vazquez, R.M.; Gonzalez, E. Obesity and hiring discrimination. Econ. Hum. Biol. 2020, 37, 100850. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.S.; Latner, J.D.; Ebneter, D.; Hunter, J.A. Obesity discrimination: The role of physical appearance, personal ideology, and anti-fat prejudice. Int. J. Obes. 2013, 37, 455–460. [Google Scholar] [CrossRef]
- Puhl, R.; Brownell, K.D. Bias, discrimination, and obesity. Obes. Res. 2001, 9, 788–805. [Google Scholar] [CrossRef]
- Ahn, R.; Kim, T.H.; Han, E. The Moderation of Obesity Penalty on Job Market Outcomes by Employment Efforts. Int. J. Environ. Res. Public Health 2019, 16, 2974. [Google Scholar] [CrossRef]
- Gao, Y.; Huang, Y.; Song, F.; Dai, H.; Wang, P.; Li, H.; Zheng, H.; Dong, H.; Han, J.; Wang, Y.; et al. Urban-rural disparity of overweight/obesity distribution and its potential trend with breast cancer among Chinese women. Oncotarget 2016, 7, 56608–56618. [Google Scholar] [CrossRef]
- Lenardson, J.D.; Hansen, A.Y.; Hartley, D. Rural and Remote Food Environments and Obesity. Curr. Obes. Rep. 2015, 4, 46–53. [Google Scholar] [CrossRef]
- Trivedi, T.; Liu, J.; Probst, J.; Merchant, A.; Jhones, S.; Martin, A.B. Obesity and obesity-related behaviors among rural and urban adults in the USA. Rural Remote Health 2015, 15, 3267. [Google Scholar]
- Yun, S.; Kim, H.J.; Oh, K. Trends in energy intake among Korean adults, 1998–2015: Results from the Korea National Health and Nutrition Examination Survey. Nutr. Res. Pract. 2017, 11, 147–154. [Google Scholar] [CrossRef]
- Park, J.; Shin, A.; Lee, M.; Choi, J.; Song, M.; Kim, Y.; Lee, J.K.; Kang, D.; Choi, J.Y. Prevalence of Participating in Physical Activity From 2 Korean Surveillance Systems: KNHANES and KCHS. J. Phys. Act. Health 2018, 15, 763–773. [Google Scholar] [CrossRef]
- Kwon, Y.S.; Ju, S.Y. Trends in nutrient intakes and consumption while eating-out among Korean adults based on Korea National Health and Nutrition Examination Survey (1998–2012) data. Nutr. Res. Pract. 2014, 8, 670–678. [Google Scholar] [CrossRef]
- Kim, H.R. Policy Suggestions on Obesity Prevention Strategies and Programs. Health and Welfare Policy Forum 2010, 163, 39–49. [Google Scholar]
- Rosen, J.C.; Gross, J. Prevalence of weight reducing and weight gaining in adolescent girls and boys. Health Psychol. 1987, 6, 131–147. [Google Scholar] [CrossRef]
- Page, R.M.; Lee, C.M.; Miao, N.F. Self-perception of body weight among high school students in Taipei, Taiwan. Int. J. Adolesc. Med. Health 2005, 17, 123–136. [Google Scholar] [CrossRef]
- Jaacks, L.M.; Vandevijvere, S.; Pan, A.; McGowan, C.J.; Wallace, C.; Imamura, F.; Mozaffarian, D.; Swinburn, B.; Ezzati, M. The obesity transition: Stages of the global epidemic. Lancet Diabetes Endocrinol. 2019, 7, 231–240. [Google Scholar] [CrossRef]
- Smith, A.R.; Joiner, T.E. Examining body image discrepancies and perceived weight status in adult Japanese women. Eat. Behav. 2008, 9, 513–515. [Google Scholar] [CrossRef]
- Takimoto, H.; Yoshiike, N.; Kaneda, F.; Yoshita, K. Thinness among young Japanese women. Am. J. Public Health 2004, 94, 1592–1595. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, F.; Takimoto, H.; Yoshita, K.; Yoshiike, N. Perceived body size and desire for thinness of young Japanese women: A population-based survey. Br. J. Nutr. 2006, 96, 1154–1162. [Google Scholar] [CrossRef]
- Wardle, J.; Haase, A.M.; Steptoe, A. Body image and weight control in young adults: International comparisons in university students from 22 countries. Int. J. Obes. 2006, 30, 644–651. [Google Scholar] [CrossRef]
- Noh, J.W.; Kwon, Y.D.; Yang, Y.; Cheon, J.; Kim, J. Relationship between body image and weight status in east Asian countries: Comparison between South Korea and Taiwan. BMC Public Health 2018, 18, 814. [Google Scholar] [CrossRef] [PubMed]
- Sakamaki, R.; Amamoto, R.; Mochida, Y.; Shinfuku, N.; Toyama, K. A comparative study of food habits and body shape perception of university students in Japan and Korea. Nutr. J. 2005, 4, 31. [Google Scholar] [CrossRef]
- Lee, H.R.; Lee, H.E.; Choi, J.; Kim, J.H.; Han, H.L. Social media use, body image, and psychological well-being: A cross-cultural comparison of Korea and the United States. J. Health Commun. 2014, 19, 1343–1358. [Google Scholar] [CrossRef]
- Al-Safi, Z.A.; Polotsky, A.J. Obesity and menopause. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 548–553. [Google Scholar] [CrossRef]
- Lizcano, F.; Guzmán, G. Estrogen Deficiency and the Origin of Obesity during Menopause. Biomed. Res. Int. 2014, 2014, 757461. [Google Scholar] [CrossRef]
- Clegg, D.J. Minireview: The year in review of estrogen regulation of metabolism. Mol. Endocrinol. 2012, 26, 1957–1960. [Google Scholar] [CrossRef]
- Lovejoy, J.C. The menopause and obesity. Prim. Care 2003, 30, 317–325. [Google Scholar] [CrossRef]
- Jura, M.; Kozak, L.P. Obesity and related consequences to ageing. Age 2016, 38, 23. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhang, Y.; Jin, M.; Gu, Z.; Pei, Y.; Meng, P. Aged-Related Changes in Body Composition and Association between Body Composition with Bone Mass Density by Body Mass Index in Chinese Han Men over 50-year-old. PLoS ONE 2015, 10, e0130400. [Google Scholar] [CrossRef]
- Kaye, S.A.; Folsom, A.R.; Prineas, R.J.; Potter, J.D.; Gapstur, S.M. The association of body fat distribution with lifestyle and reproductive factors in a population study of postmenopausal women. Int. J. Obes. 1990, 14, 583–591. [Google Scholar] [CrossRef]
- Rebuffé-Scrive, M.; Eldh, J.; Hafström, L.O.; Björntorp, P. Metabolism of mammary, abdominal, and femoral adipocytes in women before and after menopause. Metabolism 1986, 35, 792–797. [Google Scholar] [CrossRef]
- Pasquali, R.; Casimirri, F.; Cantobelli, S.; Labate, A.M.; Venturoli, S.; Paradisi, R.; Zannarini, L. Insulin and androgen relationships with abdominal body fat distribution in women with and without hyperandrogenism. Horm. Res. 1993, 39, 179–187. [Google Scholar] [CrossRef]
- Ju, J.S. Nutrition in the Republic of Korea. Br. J. Nutr. 2000, 84 (Suppl. 2), S195–S198. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Prevalence of Overall Obesity (%) | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men | Women | ||||||||||||||||||
| Sociodemographic Characteristics | I (1998) | II (2001) | III (2005) | IV (07–09) | V (10–12) | VI (13–15) | VII (16–18) | Age-Adjusted β | p for Trend | I (1998) | II (2001) | III (2005) | IV (07–09) | V (10–12) | VI (13–15) | VII (16–18) | Age-Adjusted β | p for Trend | |
| Age | 19–29 years | 18.5 | 24.8 | 24.8 | 30.3 | 28.3 | 31.3 | 38.0 | 2.65 | <0.001 | 11.7 | 11.5 | 13.4 | 13.6 | 14.2 | 14.0 | 15.8 | 0.64 | 0.01 |
| 30–39 years | 27.9 | 34.4 | 38.1 | 39.4 | 41.2 | 44.9 | 47.8 | 2.94 | <0.001 | 20.4 | 19.6 | 19.0 | 16.5 | 21.5 | 18.8 | 21.0 | 0.26 | 0.29 | |
| 40–49 years | 33.5 | 38.7 | 41.1 | 40.3 | 42.9 | 42.3 | 47.1 | 1.75 | <0.001 | 29.9 | 34.1 | 29.0 | 27.2 | 29.2 | 24.5 | 26.7 | −0.97 | 0.001 | |
| 50–59 years | 27.6 | 32.2 | 41.0 | 41.6 | 34.8 | 40.8 | 41.6 | 1.45 | <0.001 | 42.5 | 40.6 | 43.1 | 38.2 | 35.1 | 33.1 | 31.2 | −2.17 | <0.001 | |
| 60–69 years | 19.9 | 26.3 | 31.0 | 32.2 | 35.2 | 35.0 | 38.1 | 2.38 | <0.001 | 38.8 | 46.2 | 47.1 | 47.0 | 43.1 | 40.3 | 38.3 | −1.31 | <0.001 | |
| 70–79 years | 8.3 | 23.7 | 27.1 | 21.1 | 26.1 | 29.0 | 31.0 | 2.64 | <0.001 | 34.7 | 36.3 | 37.3 | 39.8 | 37.6 | 42.1 | 44.5 | 1.65 | <0.001 | |
| Income | 1st Quartile | 22.2 | 31.7 | 33.7 | 35.1 | 32.0 | 37.0 | 40.9 | 2.32 | <0.001 | 25.5 | 32.0 | 29.6 | 30.5 | 33.0 | 31.9 | 33.5 | 0.45 | 0.09 |
| 2nd Quartile | 24.8 | 29.5 | 32.6 | 35.9 | 38.2 | 40.6 | 41.4 | 2.59 | <0.001 | 27.9 | 28.6 | 28.4 | 29.8 | 29.2 | 27.7 | 29.6 | −0.52 | 0.05 | |
| 3rd Quartile | 24.0 | 33.5 | 35.6 | 38.3 | 36.3 | 38.0 | 43.5 | 2.29 | <0.001 | 24.6 | 26.1 | 30.4 | 24.6 | 27.4 | 27.1 | 27.1 | −0.39 | 0.13 | |
| 4th Quartile | 28.4 | 30.8 | 37.7 | 37.1 | 38.4 | 38.8 | 42.6 | 1.91 | <0.001 | 24.1 | 24.1 | 23.8 | 24.2 | 23.3 | 21.5 | 22.4 | −1.11 | <0.001 | |
| Education | High school or less | 25.1 | 31.7 | 35.6 | 36.1 | 35.1 | 37.5 | 40.1 | 2.19 | <0.001 | 29.1 | 33.7 | 34.6 | 34.1 | 35.5 | 34.0 | 36.5 | −0.07 | 0.68 |
| College or higher | 24.8 | 31.0 | 33.9 | 36.8 | 37.7 | 38.7 | 43.6 | 2.25 | <0.001 | 11.5 | 9.7 | 12.7 | 13.2 | 15.9 | 16.0 | 18.4 | 1.00 | <0.001 | |
| Region | Seoul | 23.5 | 29.8 | 32.0 | 37.8 | 36.8 | 37.7 | 40.8 | 2.20 | <0.001 | 25.3 | 24.9 | 24.1 | 25.1 | 23.8 | 23.1 | 25.7 | −0.80 | 0.003 |
| Metro urban | 27.9 | 30.9 | 34.2 | 34.3 | 35.2 | 37.3 | 39.4 | 1.69 | <0.001 | 23.3 | 24.4 | 28.2 | 28.2 | 27.3 | 26.1 | 27.7 | −0.36 | 0.15 | |
| Non-metro urban | 25.7 | 34.0 | 35.9 | 37.6 | 37.7 | 39.9 | 43.3 | 2.23 | <0.001 | 24.1 | 27.1 | 26.2 | 27.1 | 27.8 | 27.0 | 27.4 | −0.47 | 0.04 | |
| Rural | 21.9 | 29.5 | 37.9 | 35.0 | 34.2 | 38.9 | 45.5 | 3.18 | <0.001 | 30.5 | 35.0 | 36.0 | 29.1 | 36.3 | 34.3 | 35.6 | 0.47 | 0.17 | |
| Occupation | Non-physical labor | 27.8 | 36.2 | 38.6 | 41.0 | 42.2 | 40.3 | 45.6 | 1.78 | <0.001 | 13.5 | 9.8 | 13.5 | 14.3 | 17.7 | 17.6 | 16.8 | 0.31 | 0.28 |
| Physical labor | 26.5 | 32.7 | 37.0 | 36.2 | 35.5 | 38.6 | 42.2 | 2.04 | <0.001 | 31.3 | 34.5 | 32.5 | 31.5 | 32.7 | 30.5 | 32.6 | −0.63 | 0.01 | |
| Unemployed | 19.4 | 24.4 | 27.1 | 31.2 | 30.6 | 34.2 | 36.8 | 2.57 | <0.001 | 24.6 | 27.5 | 29.5 | 28.8 | 29.5 | 28.0 | 31.3 | −0.04 | 0.82 | |
| Prevalence of Abdominal Obesity (%) | |||||||||||||||||||
| Age | 19–29 | 12.3 | 11.2 | 11.4 | 17.6 | 15.2 | 17.7 | 23.6 | 1.89 | <0.001 | 7.5 | 6.8 | 8.0 | 8.5 | 8.7 | 8.8 | 8.1 | 0.18 | 0.36 |
| 30–39 | 16.0 | 23.1 | 21.6 | 23.1 | 26.7 | 28.6 | 35.4 | 2.84 | <0.001 | 12.9 | 13.7 | 12.9 | 13.3 | 14.9 | 14.9 | 16.0 | 0.55 | 0.02 | |
| 40–49 | 27.3 | 28.6 | 26.7 | 27.6 | 26.5 | 29.3 | 34.3 | 1.15 | <0.001 | 22.8 | 21.5 | 19.0 | 20.1 | 19.4 | 16.1 | 19.9 | −0.58 | 0.03 | |
| 50–59 | 28.4 | 27.2 | 37.5 | 30.7 | 27.0 | 29.3 | 32.1 | 0.23 | 0.51 | 38.6 | 37.7 | 37.6 | 36.2 | 29.7 | 23.7 | 24.5 | −3.19 | <0.001 | |
| 60–69 | 24.0 | 26.9 | 32.7 | 32.5 | 31.6 | 29.6 | 35.7 | 1.23 | <0.05 | 44.9 | 50.2 | 47.4 | 50.5 | 45.1 | 38.6 | 38.0 | −2.38 | <0.001 | |
| 70–79 | 13.7 | 29.8 | 32.9 | 28.2 | 29.5 | 31.9 | 36.4 | 2.27 | <0.001 | 40.7 | 45.8 | 44.8 | 47.1 | 44.4 | 47.7 | 49.9 | 1.13 | 0.02 | |
| Income | 1st Quartile | 17.1 | 21.8 | 22.8 | 24.4 | 22.9 | 27.1 | 32.4 | 2.04 | <0.001 | 23.1 | 26.7 | 26.5 | 28.8 | 28.0 | 28.3 | 29.1 | 0.04 | 0.88 |
| 2nd Quartile | 19.0 | 18.6 | 24.5 | 25.8 | 25.4 | 27.6 | 32.0 | 1.85 | <0.001 | 23.2 | 23.3 | 21.1 | 26.5 | 24.6 | 21.4 | 26.0 | −0.67 | <0.05 | |
| 3rd Quartile | 18.4 | 23.3 | 24.7 | 26.4 | 24.5 | 26.9 | 32.9 | 1.60 | <0.001 | 19.8 | 21.7 | 26.2 | 20.8 | 22.6 | 20.9 | 21.2 | −0.94 | <0.001 | |
| 4th Quartile | 22.6 | 23.4 | 25.2 | 25.7 | 26.9 | 26.8 | 31.9 | 1.07 | <0.001 | 20.4 | 19.8 | 18.8 | 21.9 | 18.8 | 17.5 | 18.2 | −1.35 | <0.001 | |
| Education | High school orless | 20.1 | 22.7 | 28.3 | 27.0 | 26.3 | 28.8 | 33.2 | 1.39 | <0.001 | 25.0 | 28.4 | 29.8 | 32.1 | 31.4 | 29.4 | 33.4 | −0.54 | <0.05 |
| College or higher | 17.9 | 21.5 | 19.4 | 23.9 | 23.8 | 25.9 | 31.9 | 1.81 | <0.001 | 8.2 | 7.0 | 6.8 | 9.4 | 10.3 | 10.7 | 12.5 | 0.53 | <0.05 | |
| Region | Seoul | 19.5 | 23.7 | 23.1 | 24.6 | 22.2 | 28.8 | 33.0 | 1.65 | <0.001 | 21.7 | 21.3 | 18.6 | 21.9 | 16.7 | 16.3 | 22.6 | −1.08 | <0.001 |
| Metro urban | 20.2 | 19.9 | 26.5 | 26.1 | 27.6 | 26.4 | 29.6 | 1.06 | <0.001 | 18.7 | 21.1 | 25.2 | 25.5 | 24.3 | 21.9 | 21.6 | −1.05 | <0.001 | |
| Non-metro urban | 19.6 | 23.2 | 22.6 | 24.9 | 23.2 | 26.6 | 32.7 | 1.70 | <0.001 | 20.0 | 19.3 | 21.3 | 22.9 | 22.6 | 22.3 | 23.3 | −0.46 | 0.05 | |
| Rural | 17.9 | 22.2 | 26.0 | 26.6 | 27.9 | 27.3 | 35.8 | 2.20 | <0.001 | 27.4 | 32.8 | 28.4 | 30.5 | 32.9 | 29.3 | 31.2 | −0.07 | 0.82 | |
| Occupation | Non-physical labor | 18.8 | 24.4 | 22.0 | 27.2 | 26.6 | 28.6 | 35.4 | 2.07 | <0.001 | 7.8 | 4.9 | 7.9 | 10.0 | 12.2 | 11.3 | 11.1 | 0.14 | 0.53 |
| Physical labor | 21.0 | 23.3 | 26.2 | 25.0 | 24.7 | 26.5 | 31.4 | 1.18 | <0.001 | 25.5 | 26.3 | 27.0 | 27.8 | 27.1 | 23.4 | 26.6 | −0.95 | <0.001 | |
| Unemployed | 16.2 | 18.0 | 23.0 | 24.9 | 24.0 | 27.0 | 30.2 | 1.72 | <0.001 | 22.1 | 24.9 | 25.0 | 27.3 | 25.8 | 25.2 | 28.8 | −0.34 | 0.06 | |
| Overall Obesity | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Socioeconomic Characteristics | I (1998) | II (2001) | III (2005) | IV (2007–2009) | V (2010–2012) | VI (2013–2015) | VII (2016–2018) | ||||||||
| OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | ||
| Income | 1st Quartile | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| 2nd Quartile | 1.11 | (0.85 1.44) | 0.88 | (0.68, 1.14) | 0.96 | (0.70, 1.31) | 1.03 | (0.86, 1.22) | 1.24 | (1.03, 1.50) | 1.17 | (0.98, 1.40) | 0.99 | (0.84, 1.17) | |
| 3rd Quartile | 1.07 | (0.80, 1.44) | 1.00 | (0.77, 1.30) | 1.07 | (0.78, 1.48) | 1.12 | (0.94, 1.34) | 1.12 | (0.92, 1.36) | 0.98 | (0.83, 1.17) | 1.08 | (0.93, 1.26) | |
| 4th Quartile | 1.29 | (0.97, 1.71) | 0.89 | (0.67, 1.17) | 1.21 | (0.88, 1.67) | 1.05 | (0.87, 1.27) | 1.23 | (1.02, 1.49) | 1.06 | (0.90, 1.26) | 1.04 | (0.89, 1.22) | |
| Education | High school or less | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| College or higher | 1.04 | (0.84, 1.28) | 1.02 | (0.82, 1.28) | 1.04 | (0.78, 1.38) | 0.98 | (0.85, 1.14) | 1.04 | (0.89, 1.22) | 1.06 | (0.92, 1.22) | 1.05 | (0.92, 1.20) | |
| Region | Seoul | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Metro urban | 1.25 | (0.96, 1.63) | 1.03 | (0.76, 1.39) | 1.07 | (0.74, 1.55) | 0.86 | (0.71, 1.04) | 0.93 | (0.78, 1.10) | 0.97 | (0.81, 1.15) | 0.94 | (0.80, 1.10) | |
| Non-metro urban | 1.10 | (0.82, 1.47) | 1.16 | (0.88, 1.53) | 1.12 | (0.78, 1.61) | 0.95 | (0.80, 1.12) | 1.05 | (0.89, 1.24) | 1.08 | (0.92, 1.26) | 1.10 | (0.95, 1.26) | |
| Rural | 0.99 | (0.75, 1.32) | 0.93 | (0.69, 1.26) | 1.25 | (0.86, 1.84) | 0.90 | (0.75, 1.10) | 0.97 | (0.80, 1.19) | 1.03 | (0.84, 1.26) | 1.27 | (1.02, 1.60) | |
| Occupation | Non-physical labor | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Physical labor | 1.02 | (0.81, 1.29) | 0.87 | (0.68, 1.12) | 1.03 | (0.78, 1.35) | 0.87 | (0.73, 1.03) | 0.82 | (0.70, 0.96) | 1.01 | (0.87, 1.18) | 0.94 | (0.82, 1.08) | |
| Unemployed | 0.92 | (0.67, 1.27) | 0.71 | (0.50, 1.01) | 0.85 | (0.59, 1.22) | 0.86 | (0.70, 1.06) | 0.81 | (0.65, 0.99) | 1.06 | (0.87, 1.30) | 0.88 | (0.74, 1.06) | |
| Abdominal Obesity | |||||||||||||||
| Income | 1st Quartile | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| 2nd Quartile | 1.13 | (0.86, 1.48) | 0.82 | (0.60, 1.13) | 1.15 | (0.84, 1.59) | 1.07 | (0.88, 1.29) | 1.12 | (0.92, 1.37) | 1.02 | (0.85, 1.23) | 0.93 | (0.79, 1.10) | |
| 3rd Quartile | 1.11 | (0.84, 1.46) | 1.01 | (0.76, 1.34) | 1.14 | (0.78, 1.64) | 1.10 | (0.90, 1.35) | 1.06 | (0.86, 1.30) | 0.93 | (0.78, 1.11) | 0.98 | (0.83, 1.14) | |
| 4th Quartile | 1.30 | (1.00, 1.68) | 1.00 | (0.72, 1.37) | 1.28 | (0.91, 1.79) | 1.03 | (0.84, 1.26) | 1.22 | (0.98, 1.51) | 0.95 | (0.79, 1.13) | 0.91 | (0.76, 1.08) | |
| Education | High school or less | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| College or higher | 1.18 | (0.92, 1.51) | 1.22 | (0.97, 1.55) | 0.95 | (0.67, 1.35) | 1.06 | (0.89, 1.26) | 1.02 | (0.85, 1.22) | 1.00 | (0.85, 1.16) | 0.99 | (0.85, 1.16) | |
| Region | Seoul | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Metro urban | 1.04 | (0.78, 1.39) | 0.76 | (0.55, 1.05) | 1.18 | (0.84, 1.64) | 1.04 | (0.84, 1.30) | 1.34 | (1.09, 1.65) | 0.88 | (0.73, 1.06) | 0.86 | (0.72, 1.03) | |
| Non-metro urban | 1.00 | (0.71, 1.39) | 0.90 | (0.67, 1.23) | 0.93 | (0.68, 1.28) | 0.95 | (0.76, 1.19) | 1.11 | (0.90, 1.38) | 0.95 | (0.80, 1.13) | 1.00 | (0.85, 1.17) | |
| Rural | 0.86 | (0.62, 1.20) | 0.78 | (0.54, 1.13) | 0.97 | (0.68, 1.39) | 1.03 | (0.81, 1.31) | 1.37 | (1.08, 1.74) | 0.93 | (0.75, 1.16) | 1.14 | (0.91, 1.42) | |
| Occupation | Non-physical labor | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Physical labor | 1.18 | (0.90, 1.54) | 0.99 | (0.74, 1.33) | 1.13 | (0.79, 1.63) | 0.85 | (0.70, 1.03) | 0.86 | (0.72, 1.04) | 0.88 | (0.74, 1.04) | 0.81 | (0.69, 0.95) | |
| Unemployed | 1.10 | (0.79, 1.52) | 0.92 | (0.63, 1.36) | 1.13 | (0.74, 1.72) | 0.88 | (0.70, 1.09) | 0.96 | (0.76, 1.22) | 1.05 | (0.84, 1.30) | 0.83 | (0.69, 1.01) | |
| Overall Obesity | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Socioeconomic Characteristics | I (1998) | II (2001) | III (2005) | IV (2007–2009) | V (2010–2012) | VI (2013–2015) | VII (2016–2018) | ||||||||
| OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | ||
| Income | 1st Quartile | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| 2nd Quartile | 1.18 | (0.96, 1.45) | 0.88 | (0.68, 1.14) | 1.00 | (0.76, 1.32) | 0.94 | (0.79, 1.12) | 0.87 | (0.74, 1.01) | 0.82 | (0.71, 0.96) | 0.84 | (0.73, 0.98) | |
| 3rd Quartile | 1.00 | (0.80, 1.25) | 0.80 | (0.62, 1.04) | 1.16 | (0.90, 1.49) | 0.77 | (0.65, 0.91) | 0.84 | (0.71, 0.99) | 0.80 | (0.68, 0.93) | 0.80 | (0.68, 0.93) | |
| 4th Quartile | 0.99 | (0.78, 1.26) | 0.86 | (0.65, 1.14) | 0.86 | (0.64, 1.16) | 0.76 | (0.64, 0.91) | 0.71 | (0.60, 0.85) | 0.61 | (0.52, 0.73) | 0.66 | (0.56, 0.78) | |
| Education | High school or less | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| College or higher | 0.58 | (0.44, 0.78) | 0.43 | (0.32, 0.59) | 0.49 | (0.36, 0.67) | 0.55 | (0.45, 0.67) | 0.54 | (0.46, 0.64) | 0.62 | (0.53, 0.73) | 0.62 | (0.54, 0.72) | |
| Region | Seoul | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Metro urban | 0.89 | (0.69, 1.14) | 0.82 | (0.64, 1.06) | 1.10 | (0.83, 1.47) | 1.09 | (0.91, 1.31) | 1.17 | (0.96, 1.42) | 1.07 | (0.89, 1.28) | 0.98 | (0.84, 1.15) | |
| Non-metro urban | 0.90 | (0.73, 1.11) | 1.02 | (0.79, 1.31) | 1.06 | (0.78, 1.43) | 1.15 | (0.96, 1.38) | 1.18 | (0.99, 1.39) | 1.20 | (1.01, 1.42) | 1.00 | (0.86, 1.16) | |
| Rural | 0.90 | (0.70, 1.15) | 1.00 | (0.76, 1.32) | 1.27 | (0.88, 1.82) | 0.97 | (0.80, 1.18) | 1.40 | (1.16, 1.70) | 1.34 | (1.10, 1.63) | 1.15 | (0.94, 1.41) | |
| Occupation | Non-physical labor | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Physical labor | 1.21 | (0.85, 1.70) | 1.71 | (1.09, 2.69) | 1.14 | (0.74, 1.76) | 1.21 | (0.95, 1.55) | 1.07 | (0.86, 1.33) | 1.00 | (0.82, 1.21) | 1.37 | (1.14, 1.65) | |
| Unemployed | 1.07 | (0.76, 1.49) | 1.42 | (0.93, 2.17) | 1.25 | (0.85, 1.83) | 1.25 | (1.01, 1.54) | 1.14 | (0.93, 1.39) | 1.00 | (0.83, 1.19) | 1.41 | (1.20, 1.66) | |
| Abdominal Obesity | |||||||||||||||
| Income | 1st Quartile | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| 2nd Quartile | 1.10 | (0.89, 1.37) | 0.91 | (0.67, 1.22) | 0.77 | (0.57, 1.05) | 0.85 | (0.71, 1.01) | 0.83 | (0.71, 0.97) | 0.65 | (0.55, 0.77) | 0.87 | (0.75, 1.00) | |
| 3rd Quartile | 0.88 | (0.69, 1.12) | 0.85 | (0.65, 1.12) | 1.07 | (0.80, 1.44) | 0.64 | (0.55, 0.76) | 0.78 | (0.66, 0.92) | 0.67 | (0.57, 0.79) | 0.69 | (0.59, 0.81) | |
| 4th Quartile | 0.90 | (0.71, 1.14) | 0.89 | (0.65, 1.21) | 0.72 | (0.51, 1.00) | 0.69 | (0.58, 0.83) | 0.65 | (0.54, 0.78) | 0.54 | (0.44, 0.65) | 0.60 | (0.51, 0.71) | |
| Education | High school or less | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| College or higher | 0.69 | (0.48, 0.99) | 0.48 | (0.33, 0.69) | 0.39 | (0.25, 0.59) | 0.53 | (0.43, 0.65) | 0.53 | (0.43, 0.64) | 0.58 | (0.48, 0.70) | 0.58 | (0.50, 0.68) | |
| Region | Seoul | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Metro urban | 0.80 | (0.59, 1.07) | 0.85 | (0.64, 1.15) | 1.26 | (0.93, 1.70) | 1.13 | (0.89, 1.44) | 1.60 | (1.26, 2.03) | 1.28 | (1.04, 1.57) | 0.81 | (0.67, 0.99) | |
| Non-metro urban | 0.86 | (0.66, 1.13) | 0.81 | (0.59, 1.09) | 1.10 | (0.78, 1.54) | 1.11 | (0.87, 1.41) | 1.43 | (1.14, 1.79) | 1.46 | (1.20, 1.77) | 0.94 | (0.79, 1.11) | |
| Rural | 0.81 | (0.62, 1.05) | 1.01 | (0.71, 1.44) | 0.99 | (0.69, 1.42) | 1.16 | (0.91, 1.49) | 1.74 | (1.36, 2.22) | 1.57 | (1.25, 1.97) | 1.05 | (0.85, 1.29) | |
| Occupation | Non-physical labor | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Physical labor | 1.41 | (0.93, 2.15) | 2.11 | (1.23, 3.63) | 1.19 | (0.72, 1.98) | 1.20 | (0.94, 1.54) | 0.99 | (0.78, 1.26) | 0.98 | (0.77, 1.24) | 1.35 | (1.11, 1.65) | |
| Unemployed | 1.39 | (0.92, 2.09) | 2.00 | (1.20, 3.34) | 1.19 | (0.74, 1.92) | 1.35 | (1.07, 1.69) | 1.08 | (0.85, 1.37) | 1.12 | (0.91, 1.40) | 1.58 | (1.33, 1.88) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, H.-J.; Oh, H. Trends and Inequalities in Overall and Abdominal Obesity by Sociodemographic Factors in Korean Adults, 1998–2018. Int. J. Environ. Res. Public Health 2021, 18, 4162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084162
Jang H-J, Oh H. Trends and Inequalities in Overall and Abdominal Obesity by Sociodemographic Factors in Korean Adults, 1998–2018. International Journal of Environmental Research and Public Health. 2021; 18(8):4162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084162
Chicago/Turabian StyleJang, Ha-Jin, and Hannah Oh. 2021. "Trends and Inequalities in Overall and Abdominal Obesity by Sociodemographic Factors in Korean Adults, 1998–2018" International Journal of Environmental Research and Public Health 18, no. 8: 4162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084162