
Complications in the Use of Deepithelialized Free Gingival Graft vs. Connective Tissue Graft: A One-Year Randomized Clinical Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion/Exclusion Criteria
2.3. Surgical Procedure
2.4. Post-Surgical Instructions
2.5. Index and Classification of Complications
- Epithelial cyst: chronic inflammatory lesion partially or completely delimited by tissue.
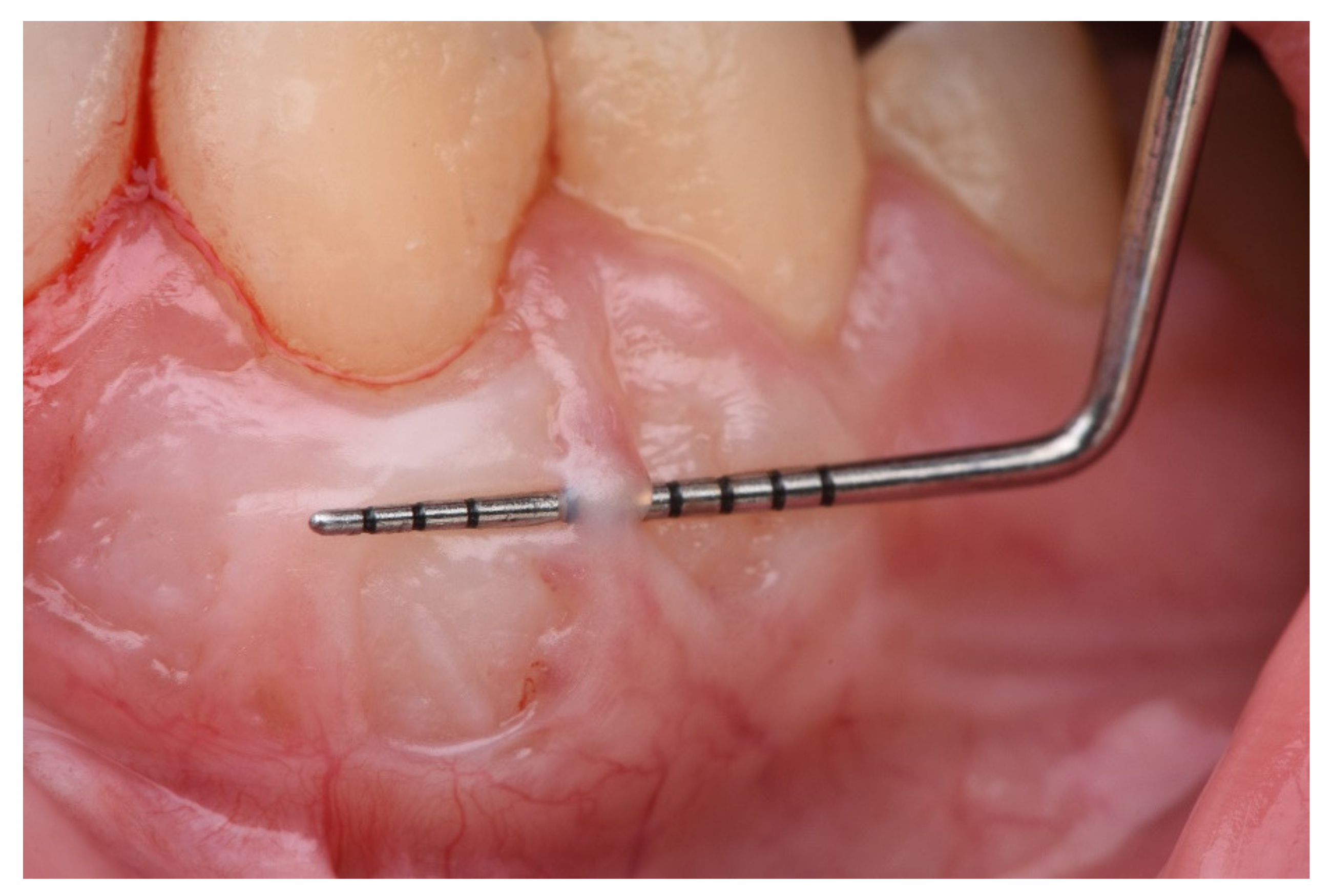
- Cul-de-sac: invagination formation, with probing depths greater than 0.5 mm (Figure 2).
- Bony exostoses: benign overgrowth of a pre-existing bone.
- Color change: aesthetic alteration compared with the appearance of the surrounding tissues.
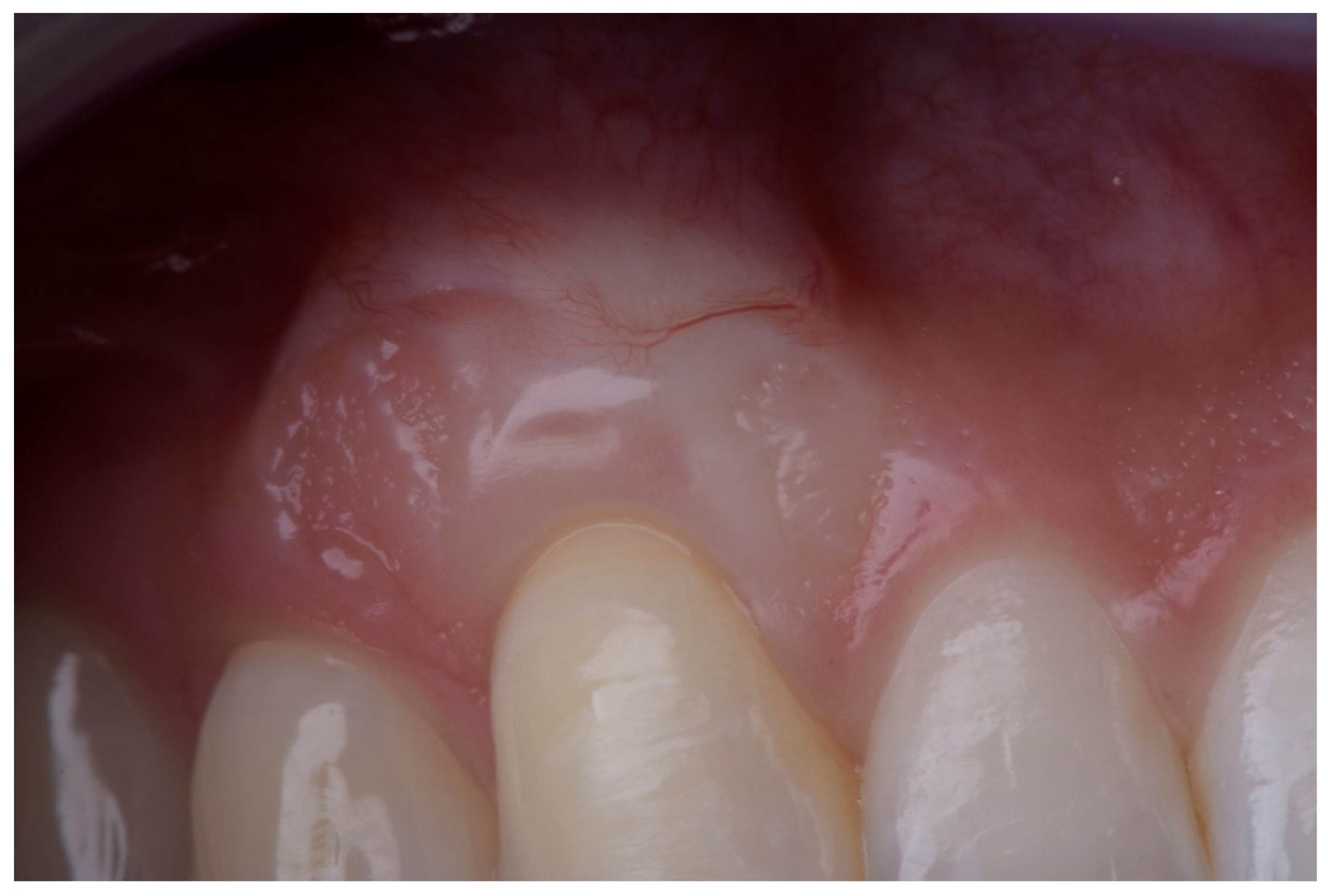
- Superficial re-epithelialization: proliferation, partial or complete, of the original superficial epithelial layer of the graft, resulting in a mucosal surface similar to the donor area creating a patch effect comparable to the ones produces in an IGL (Figure 3).
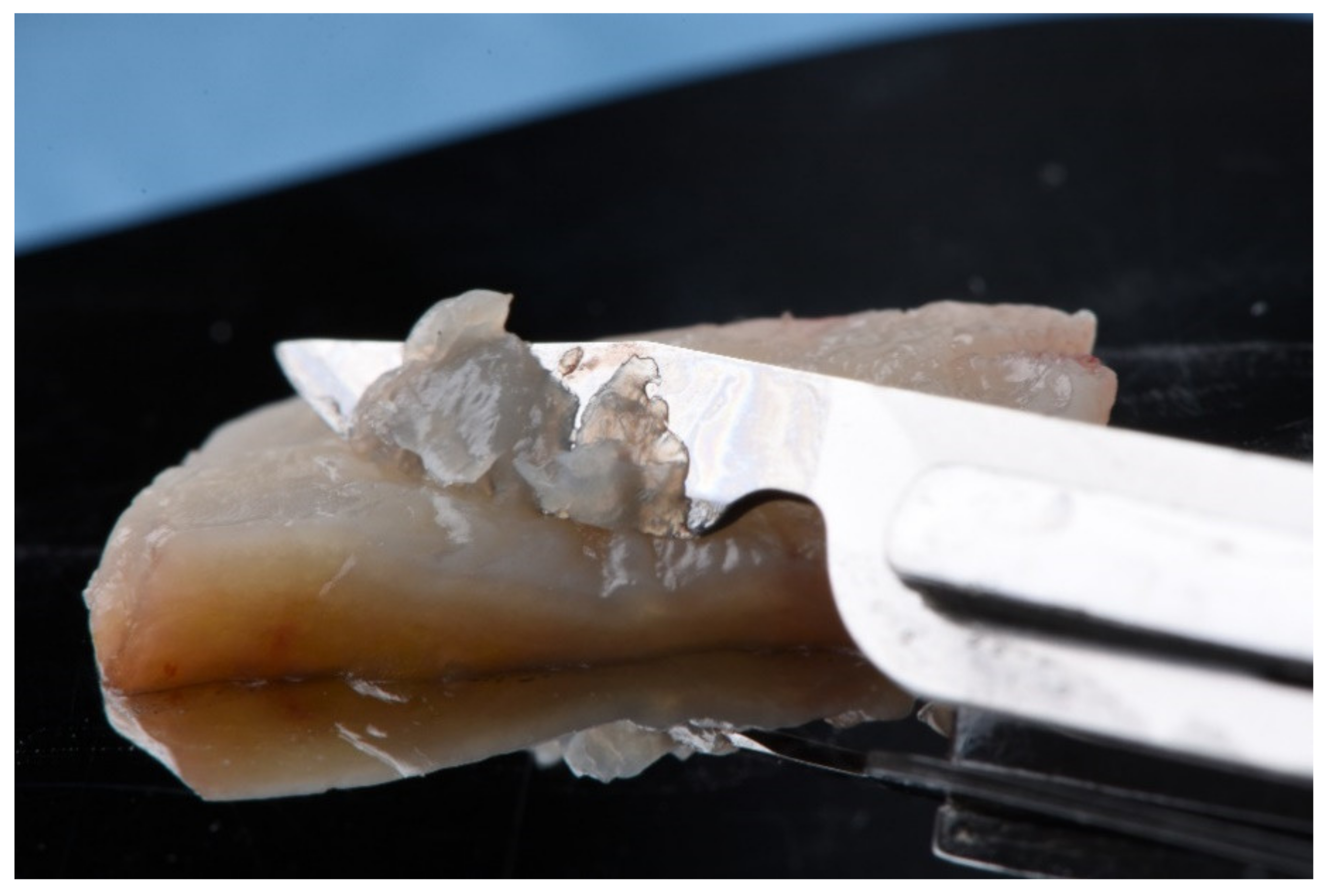
- Superficial epithelial bands: epithelial tissue located on the graft without being adhered to it (Figure 4).
- Superficial revascularization: proliferation of multiple blood vessels modifying the superficial aesthetics of the graft. (Figure 5).
- The re-epithelialization of the graft; it substantially modifies the aesthetics.
- The presence of epithelial bands; for being non-adhered retentive areas.
- The presence of cul-de-sac; retentive and aesthetic effect.
- The presence of epithelial cysts.
- Bone exostoses.
2.6. Postoperative Controls
3. Results
3.1. Incidence of Major Complications
3.2. Incidence of Minor Complications
4. Discussion
4.1. Major Complications: Re-Epithelialization, Epithelial Bands, and Cul-de-Sac
4.2. Major Complications: Epithelial Cysts
4.3. Major Complications: Bone Exostoses
4.4. Minor Complications: Discoloration and Superficial Revascularization
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guinard, E.A.; Caffese, R.G. Treatment of localized gingival recessions. Part I. Lateral sliding flap. J. Periodontol. 1978, 49, 351. [Google Scholar] [CrossRef] [PubMed]
- Hall, W.B. The current status of mucogingival problems and their therapy. J. Periodontol. 1981, 52, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, H.C.; Atkins, J.H. Free Autogenous Grafts: III. Utilization of Grafts in the Treatment of Gingival Recession. Periodontics 1968, 6, 152–160. [Google Scholar]
- Miller, P.D. Root coverage using free soft tissue autografts following acid application. I. Technique. Int. J. Periodont. Rest. Dent. 1982, 2, 65–70. [Google Scholar]
- MilIer, P.D., Jr. Root coverage with the free gingival graft. Factors associated with incomplete coverage. J. Periodontol. 1987, 58, 674–681. [Google Scholar] [CrossRef]
- Grupe, H.; Warren, R.F. Repair of gingival defects by a sliding flap operation. J. Periodontol. 1956, 27, 92–99. [Google Scholar] [CrossRef]
- Zucchelli, G.; Marzadori, M.; Mele, M.; Stefanini, M.; Montebugnoli, L. Root coverage in molar teeth: A comparative controlled randomized clinical trial. J. Clin. Periodontol. 2012, 39, 1082–1088. [Google Scholar] [CrossRef]
- Chambrone, L.; Chambrone, D.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Can subepithelial connective tissue grafts be considered the gold standard procedure in the treatment of Miller Class I and II recession-type defects? J. Dent. 2008, 36, 659–671. [Google Scholar] [CrossRef]
- Zucchelli, G.; Marzadori, M.; Mounssif, I.; Mazzotti, C.; Stefanini, M. Coronally advanced flap + connective tissue graft techniques for the treatment of deep gingival recession in the lower incisors. A controlled randomized clinical trial. J. Clin. Periodontol. 2014, 41, 806–813. [Google Scholar] [CrossRef]
- Aroca, S.; Molnár, B.; Windisch, P.; Gera, I.; Salvi, G.E.; Nikolidakis, D.; Sculean, A. Treatment of multiple adjacent Miller class I and II gingival recessions with a Modified Coronally Advanced Tunnel (MCAT) technique and a collagen matrix or palatal connective tissue graft: A randomized, controlled clinical trial. J. Clin. Periodontol. 2013, 40, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.; Wang, H.L. Flap thickness as a Predictor of Root Coverage: A Systematic Review. J. Periodontol. 2006, 77, 1625–1634. [Google Scholar] [CrossRef]
- Wessel, J.R.; Tatakis, D.N. Patient outcomes following subepithelial connective tissue graft and free gingival graft procedures. J. Periodontol. 2008, 79, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Rotenberg, S.R.; Tatakis, D.N. Dimensional changes during early healing after a subepithelial connective tissue graft procedure. J. Periodontol. 2013, 85, 884–889. [Google Scholar] [CrossRef] [PubMed]
- Brasher, J.W.; Rees, T.D.; Boyce, W.A. Complications of free grafts of masticatory mucosa. J. Periodontol. 1975, 46, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Breault, L.G.; Billman, M.A.; Lewis, D.M. Report of a gingival “surgical cyst” developing secondarily to a subepithelial connective tissue graft. J. Periodontol. 1997, 68, 392–395. [Google Scholar] [CrossRef]
- Harris, R.J. Formation of cyst-like area after a connective tissue graft for root coverage. J Periodontol. 2002, 73, 340–345. [Google Scholar] [CrossRef]
- Escalante, M.G.; Tatakis, D.N. Gingival Cyst of the Adult as Early Sequela of Connective Tissue Grafting. Case Rep. Dent. 2015, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Ritchey, B.; Orban, B. Cysts of the gingiva. Oral. Surg. Oral. Med. Oral. Pathol. 1953, 6, 765–771. [Google Scholar] [CrossRef]
- Wei, P.C.; Geivelis, M. A gingival cul-de-sac following a root coverage procedure with a subepithelial connective tissue submerged graft. J. Periodontol. 2003, 74, 1376–1380. [Google Scholar] [CrossRef]
- Otero-Cagide, F.J.; Singer, D.L.; Hoover, J.N. Exostosis associated with autogenous gingival grafts: A report of 9 cases. J. Periodontol. 1996, 67, 611–616. [Google Scholar] [CrossRef]
- Corsair, A.J.; Iacono, V.J.; Moss, S.S. Exostosis following a subepithelial connective tissue graft. J. Int. Acad. Periodontol. 2001, 3, 38–41. [Google Scholar] [PubMed]
- Hokett, S.D.; Peacock, M.E.; Burns, W.T.; Swiec, G.D.; Cuenin, M.F. External Root Resorption Following Partial-Thickness Connective Tissue Graft Placement: A Case Report. J. Periodontol. 2002, 73, 334–339. [Google Scholar] [CrossRef]
- Carnio, J.; Camargo, P.M.; Kenney, E.B. Root resorption associated with a subepithelial connective tissue graft for root coverage: Clinical and histologic report of a case. Int. J. Periodontics Restor. Dent. 2003, 23, 391–398. [Google Scholar]
- Cizza, N.; Migues, D. Progressive root resorption associated with the treatment of deep gingival recession. A clinical case. Int. J. Periodontics Restor. Dent. 2010, 30, 619–625. [Google Scholar] [PubMed]
- Gluckman, H.; Du Toit, J.; Pontes, C.C.; Hille, J. Hyperplastic Response Following Soft Tissue Augmentation in the Esthetic Zone. Clinical Advances in Periodontics. Clin. Adv. Periodontics. 2019, 9, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Parashis, A.O.; Tatakis, D.N. Subepithelial Connective Tissue Graft for Root Coverage: A Case Report of an Unusual Late Complication of Epithelial Origin. J. Periodontol. 2007, 78, 2051–2056. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Mele, M.; Mazzotti, C.; Marzadori, M.; Montebugnoli, L.; De Sanctis, M. Coronally advanced flap with and without vertical releasing incisions for the treatment of multiple gingival recessions: A comparative controlled randomized clinical trial. J. Periodontol. 2009, 80, 1083–1094. [Google Scholar] [CrossRef] [PubMed]
- Alberto de Castro, L.; Franco Vêncio, E.; Francisco Mendonça, E. Epithelial Inclusion Cyst After. Free Gingival Graft: A Case Report. Int. J. Periodontics Restor. Dent. 2007, 27, 465–469. [Google Scholar]
- Pack, A.R.C.; Gaudie, W.M.; Jennings, A.M. Bony exostosis as a sequela to free gingival grafting: Two case reports. J. Periodontol. 1991, 62, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Czuszak, C.A.; Tolson, G.E.; Kudryk, V.L.; Hanson, B.S.; Billman, M.A. Development of an exostosis following a free gingival graft: Case report. J. Periodontol. 1996, 67, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Efeoglu, A.; Demirel, K. A further report of bony exostosis occurring as a sequela to free gingival grafts. Periodontal Clin. Investig. 1994, 16, 20–22. [Google Scholar]
- Echeverria, J.J.; Montero, M.; Abad, D.; Gay, C. Exostosis following a free gingival graft. J. Clin. Periodontol. 2002, 29, 474–477. [Google Scholar] [CrossRef]
- Goyal, L.; Gupta, N.D.; Gupta, N.; Chawla, K. Free Gingival Graft as a Single Step Procedure for Treatment of Mandibular Miller Class I and II Recession Defects. World J. Plast. Surg. 2019, 8, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Raoofi, S.; Asadinejad, S.M.; Khorshidi, H. Evaluation of color and width of attached gingiva gain in two surgical techniques: Free gingival graft and connective tissue graft covered by thin mucosal flap, a clinical trial. J. Dent. (Shiraz) 2019, 20, 224–231. [Google Scholar] [CrossRef]
- Maia, V.T.G.; Kahn, S.; De Souza, A.B.; Fernandes, G.V.D.O. De-Epithelialized Connective Tissue Graft and the Reminiscent Epithelial Content after Harvested by the Harris’ Technique: A Histological and Morphometrical Case Series. Clin. Adv. Periodontics. 2021. [Google Scholar] [CrossRef] [PubMed]
- MilIer, P.D., Jr. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Di Domenico, M.; Pinto, F.; Quagliuolo, L.; Contaldo, M.; Settembre, G.; Romano, A.; Coppola, M.; Ferati, K.; Bexheti-Ferati, A.; Sciarra, A.; et al. The Role of Oxidative Stress and Hormones in Controlling Obesity. Front. Endocrinol. 2019, 10, 540. [Google Scholar] [CrossRef] [Green Version]
- Hurzeler, M.B.; Weng, D. A single incision technique to harvest subepithelial connective tissue grafts from palate. Int. J. Periodontics Restor. Dent. 1999, 19, 279–287. [Google Scholar]
- Holbrook, T.; Ochsenbein, C. Complete coverage of the denuded root surface with a one-stage gingival graft. Int. J. Periodontics Restor. Dent. 1983, 3, 8–27. [Google Scholar]
- Roman, A.; Soanca, A.; Campian, R.; Cioban, C.; Balazsi, R. Postoperative Complications Following Gingival Grafts: A Prospective Cohort Study. Appl. Med. Inform. 2011, 4, 19–26. [Google Scholar]
- Griffin, T.J.; Cheung, W.S.; Zavras, A.I.; Damoulis, P.D. Postoperative Complications Following Gingival Augmentation Procedures. J. Periodontol. 2006, 77, 2070–2079. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, R.; Mizutani, K.; Lin, T.; Kakizaki, S.; Mimata, A.; Watanabe, K.; Saito, N.; Meinzer, W.; Iwata, T.; Izumi, Y.; et al. Ex Vivo Evaluation of Gingival Ablation with Various Laser Systems and Electroscalpel. Photobiomodulation Photomedicin Laser Surg. 2020, 38, 364–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshino, H.; Hasuike, A.; Sanjo, N.; Sato, D.; Kubota, T.; Nagashima, H.; Sato, S. CO2 Laser De-epithelization Technique for Subepithelial Connective Tissue Graft: A Study of 21 Recessions. In Vivo 2020, 34, 869–875. [Google Scholar] [CrossRef] [Green Version]
- Gursoy, H.; Yarimoglu, E.; Kuru, B.; Ozkan Karaca, E.; Ince Kuka, G. Evaluation of the Effects of Er:YAG Laser for the De-Epithelialization of the Palatal Graft in the Treatment of Multiple Gingival Recessions: A Randomized Clinical Trial. Photobiomodulation Photomedicine Laser Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Capparé, P.; Teté, G.; Romanos, G.E.; Nagni, M.; Sannino, G.; Gherlone, E.F. The ’All-on-four’ protocol in HIV-positive patients: A prospective, longitudinal 7-year clinical study. Int. J. Oral. Implantol. (Berl.) 2019, 12, 501–510. [Google Scholar]
- Cairo, F.; Nieri, M.; Cattabriga, M.; Cortellini, P.; De Paoli, S.; De Sanctis, M.; Fonzar, A.; Francetti, L.; Merli, M.; Rasperini, G.; et al. Root coverage esthetic score after treatment of gingival recession: An interrater agreement multicenter study. J. Periodontol. 2010, 81, 1752–1758. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Complications | Control Group (CTG + CAF) (n = 32 Patients) | Test Group (DFGG + CAF) (n = 34 Patients) | Confidence Interval (95%) |
|---|---|---|---|
| Major | |||
| Reepithelialization | 0 (0%) | 5 (15.6%) | [3.03–28.07%] p = 0.023 |
| Cul de Sac | 0 (0%) | 5 (15.6%) | [3.03–28.07%] p = 0.023 |
| Epithelial bands | 0 (0%) | 5 (15.6%) | [3.03–28.07%] p = 0.023 |
| Cysts | 0 (0%) | 0 (0%) | - |
| Exostoses | 0 (0%) | 0 (0%) | - |
| Minor | |||
| Revascularization | 2 (5.9%) | 10 (31.3%) | [1.259–22.409%] p = 0.01 |
| Discoloration | 5 (14.7%) | 15 (46.9%) | [11.21–53.19%] p = 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ripoll, S.; Fernández de Velasco-Tarilonte, Á.; Bullón, B.; Ríos-Carrasco, B.; Fernández-Palacín, A. Complications in the Use of Deepithelialized Free Gingival Graft vs. Connective Tissue Graft: A One-Year Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 4504. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094504
Ripoll S, Fernández de Velasco-Tarilonte Á, Bullón B, Ríos-Carrasco B, Fernández-Palacín A. Complications in the Use of Deepithelialized Free Gingival Graft vs. Connective Tissue Graft: A One-Year Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2021; 18(9):4504. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094504
Chicago/Turabian StyleRipoll, Silvestre, Ángela Fernández de Velasco-Tarilonte, Beatriz Bullón, Blanca Ríos-Carrasco, and Ana Fernández-Palacín. 2021. "Complications in the Use of Deepithelialized Free Gingival Graft vs. Connective Tissue Graft: A One-Year Randomized Clinical Trial" International Journal of Environmental Research and Public Health 18, no. 9: 4504. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094504