
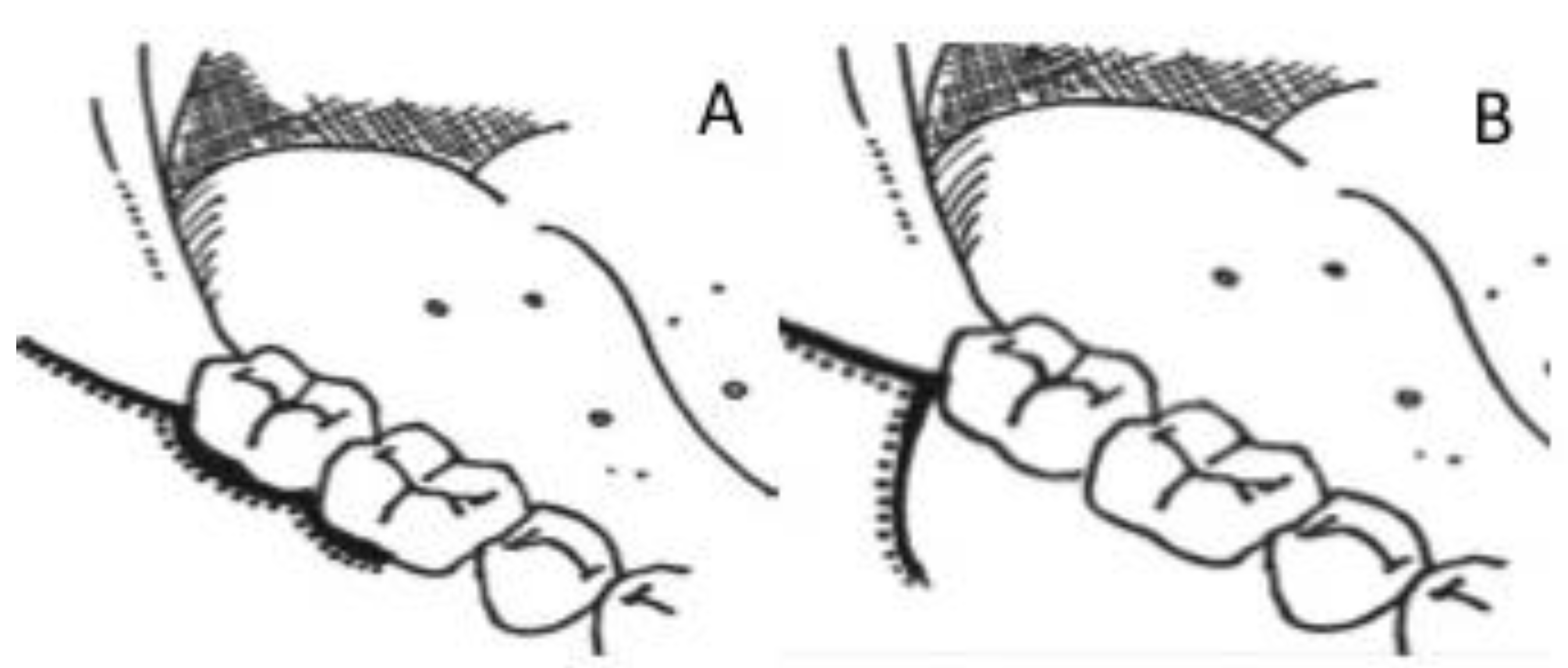
Influence of Surgical Flap Design (Envelope and Szmyd) for Removal of Impacted Mandibular Third Molars on Clinical Periodontal Parameters: A Clinical Trial


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Study Design and Participants
2.3. Questionnaire
2.4. Clinical Assessments
2.5. Surgical Procedure
2.6. Statistical Analysis
3. Results
3.1. General Characteristics of Study Participants
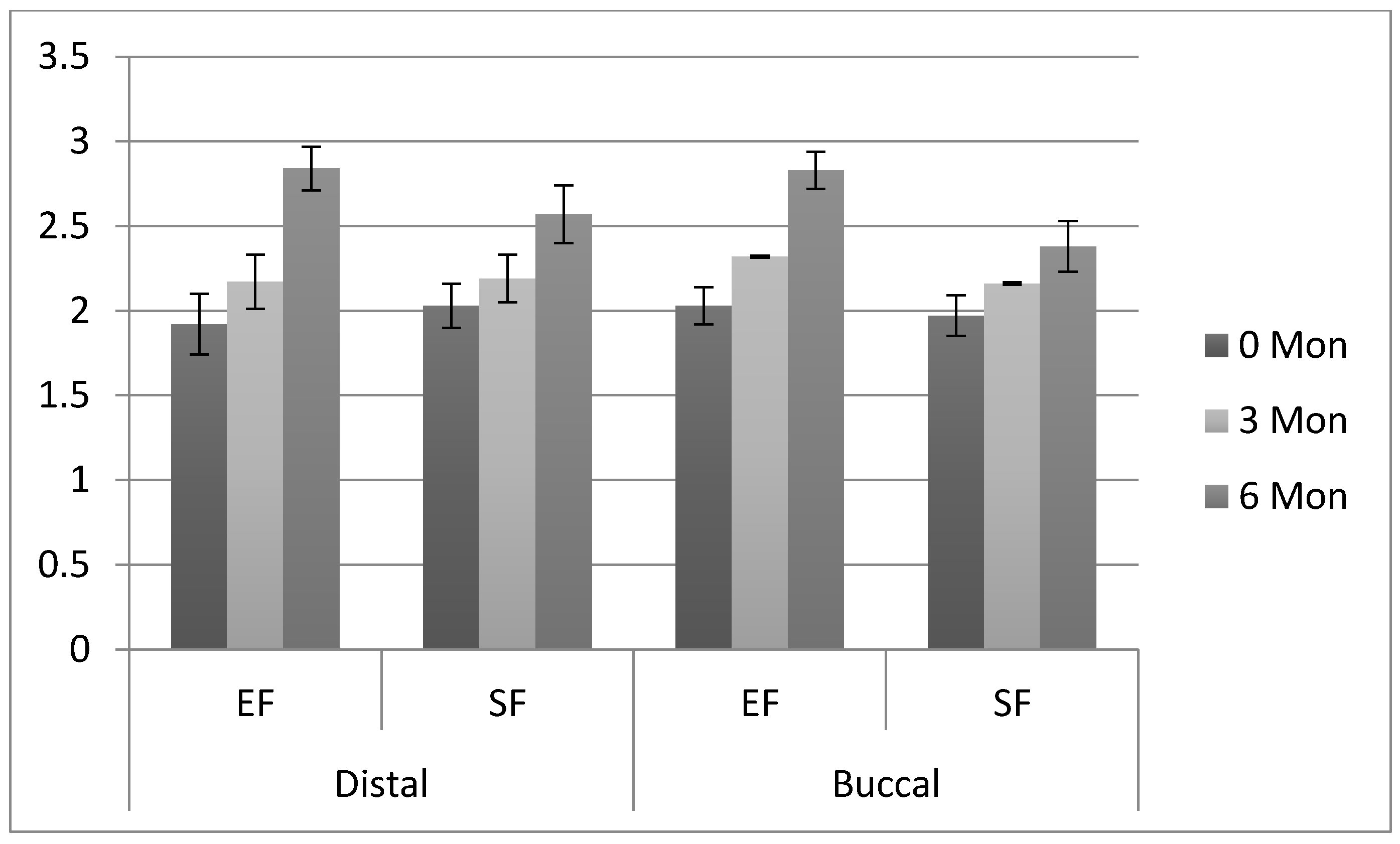
3.2. Comparison of Periodontal Parameters
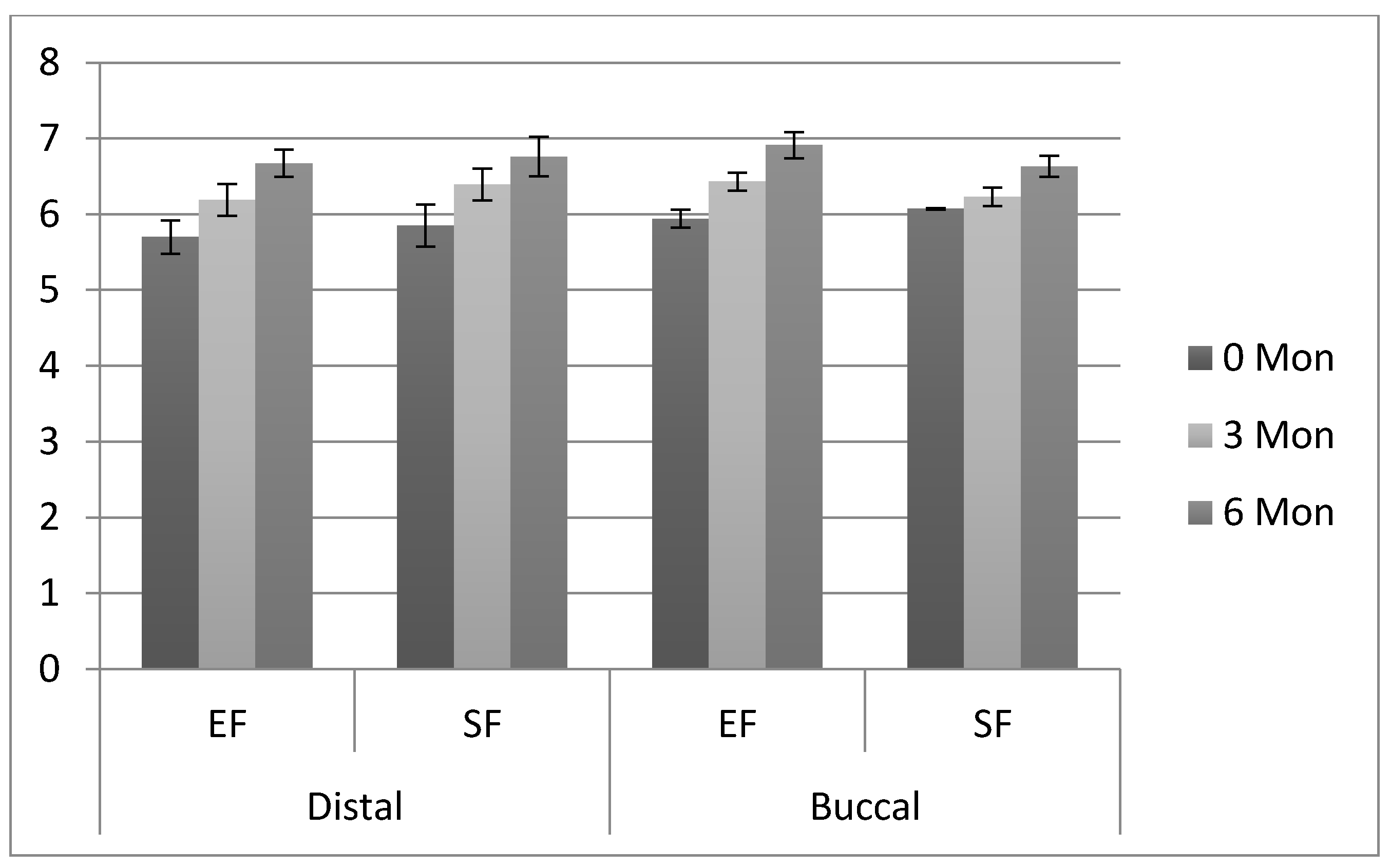
3.3. Comparison of Clinical Attachment Loss
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Dolanmaz, D.; Esen, A.; Isik, K.; Candirli, C. Effect of 2 flap designs on postoperative pain and swelling after impacted third molar surgery. Oral Surg. Oral Med. Oral Path. Oral Rad. 2013, 116, e244–e246. [Google Scholar] [CrossRef]
- Jakse, N.; Bankaoglu, V.; Wimmer, G.; Eskici, A.; Pertl, C. Primary wound healing after lower third molar surgery: Evaluation of 2 different flap designs. Oral Surg. Oral Med. Oral Path. Oral Rad. Endod. 2002, 93, 7–12. [Google Scholar] [CrossRef]
- Erdogan, Ö.; Tatlı, U.; Üstün, Y.; Damlar, I. Influence of two different flap designs on the sequelae of mandibular third molar surgery. Oral Maxfac. Surg. 2011, 15, 147. [Google Scholar] [CrossRef]
- Monaco, G.; Daprile, G.; Tavernese, L.; Corinaldesi, G.; Marchetti, C. Mandibular third molar removal in young patients: An evaluation of 2 different flap designs. J. Oral Maxfac. Surg. 2009, 67, 15–21. [Google Scholar] [CrossRef]
- Koyuncu, B.Ö.; Çetingül, E. Short-term clinical outcomes of two different flap techniques in impacted mandibular third molar surgery. Oral Surg. Oral Med. Oral Path. Oral Rad. 2013, 116, e179–e184. [Google Scholar] [CrossRef] [PubMed]
- Enrico Borgonovo, A.; Giussani, A.; Battista Grossi, G.; Maiorana, C. Evaluation of postoperative discomfort after impacted mandibular third molar surgery using three different types of flap. Quintessence Intern. 2014, 45, 21–27. [Google Scholar]
- Alqahtani, N.A.; Khaleelahmed, S.; Desai, F. Evaluation of two flap designs on the mandibular second molar after third molar extractions. J. Oral Maxillofac. Pathol. 2017, 21, 317. [Google Scholar] [PubMed] [Green Version]
- Di Nardo, D.; Mazzucchi, G.; Lollobrigida, M.; Passariello, C.; Guarnieri, R.; Galli, M.; De Biase, A.; Testarelli, L. Immediate or delayed retrieval of the displaced third molar: A review. J. Clin. Exper. Dent. 2019, 11, e55. [Google Scholar] [CrossRef]
- Yolcu, Ü.; Acar, A. Comparison of a new flap design with the routinely used triangular flap design in third molar surgery. Int. J. Oral Maxfac. Surg. 2015, 44, 1390–1397. [Google Scholar] [CrossRef]
- Briguglio, F.; Zenobio, E.G.; Isola, G.; Briguglio, R.; Briguglio, E.; Farronato, D. Complications in surgical removal of impacted mandibular third molars in relation to flap design: Clinical and statistical evaluations. Quintessence Intern. 2011, 42, 6–12. [Google Scholar]
- Rahpeyma, A.; Khajehahmadi, S.; Ilkhani, S. Wound dehiscence after wisdom tooth removal in mandibular mesioangular class IB impactions: Triangular transposition flap versus envelope flap. J. Dent. Res. Dent. Clin. Dent. Prosp. 2015, 9, 175. [Google Scholar] [CrossRef]
- Goldsmith, S.M.; De Silva, R.K.; Tong, D.C.; Love, R.M. Influence of a pedicle flap design on acute postoperative sequelae after lower third molar removal. Int. J. Oral Maxfac. Surg. 2012, 41, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Cunqueiro, M.M.; Gutwald, R.; Reichman, J.; Otero-Cepeda, X.L.; Schmelzeisen, R. Marginal flap versus paramarginal flap in impacted third molar surgery: A prospective study. Oral Surg. Oral Med. Oral Path. Oral Radiol. Endodontol. 2003, 95, 403–408. [Google Scholar] [CrossRef]
- Kugelberg, C.F. Periodontal healing two and four years after impacted lower third molar surgery: A comparative retrospective study. Int. J. Oral Maxfac. Surg. 1990, 19, 341–345. [Google Scholar] [CrossRef]
- Marciani, R.D. Complications of third molar surgery and their management. Atlas Oral Maxillofac. Surg. Clin. N. Am. 2012, 20, 233–251. [Google Scholar] [CrossRef] [PubMed]
- Osunde, O.; Adebola, R.; Omeje, U. Management of inflammatory complications in third molar surgery: A review of the literature. Afr. Health Sci. 2011, 11, 3–9. [Google Scholar]
- Wood, D.L.; Hoag, P.M.; Donnenfeld, O.W.; Rosenfeld, L.D. Alveolar crest reduction following full and partial thickness flaps. J. Periodontol. 1972, 43, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Rullo, R.; Addabbo, F.; Papaccio, G.; D’Aquino, R.; Festa, V.M. Piezoelectric device vs. conventional rotative instruments in impacted third molar surgery: Relationships between surgical difficulty and postoperative pain with histological evaluations. J. Cranio-Maxillofac. Surg. 2013, 41, e33–e38. [Google Scholar] [CrossRef]
- Bello, S.A.; Adeyemo, W.L.; Bamgbose, B.O.; Obi, E.V.; Adeyinka, A.A. Effect of age, impaction types and operative time on inflammatory tissue reactions following lower third molar surgery. Head Face Med. 2011, 7, 8. [Google Scholar] [CrossRef] [Green Version]
- Barbosa-Rebellato, N.-L.; Thomé, A.-C.; Costa-Maciel, C.; Oliveira, J.; Scariot, R. Factors associated with complications of removal of third molars: A transversal study. Med. Oral Patol. Oral Cir. Bucal. 2011, 16, e376–e380. [Google Scholar] [CrossRef]
- Malkawi, Z.; Al-Omiri, M.K.; Khraisat, A. Risk indicators of postoperative complications following surgical extraction of lower third molars. Med Princ. Pract. 2011, 20, 321–325. [Google Scholar] [CrossRef]
- Komerik, N.; Muglali, M.; Tas, B.; Selcuk, U. Difficulty of impacted mandibular third molar tooth removal: Predictive ability of senior surgeons and residents. J. Oral Maxillofac. Surg. 2014, 72, 1062-e1. [Google Scholar] [CrossRef] [PubMed]
- Lata, J.; Tiwari, A.K. Incidence of lingual nerve paraesthesia following mandibular third molar surgery. Natl. J. Maxillofac. Surg. 2012, 2, 137. [Google Scholar]
- de Santana-Santos, T.; de Souza-Santos, J.A.; Martins-Filho, P.R.; da Silva, L.C.; de Oliveira E Silva, E.D.; Gomes, A.C. Prediction of postoperative facial swelling, pain and trismus following third molar surgery based on preoperative variables. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e65–e70. [Google Scholar] [CrossRef] [PubMed]
- Cunha-Cruz, J.; Rothen, M.; Spiekerman, C.; Drangsholt, M.; McClellan, L.; Huang, G.J. Recommendations for third molar removal: A practice-based cohort study. Am. J. Public Health 2014, 104, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Sarikov, R.; Juodzbalys, G. Inferior alveolar nerve injury after mandibular third molar extraction: A literature review. J. Oral Maxillofac. Res. 2014, 5, e1. [Google Scholar] [CrossRef]
- Nguyen, E.; Grubor, D.; Chandu, A. Risk factors for permanent injury of inferior alveolar and lingual nerves during third molar surgery. J. Oral Maxillofac. Surg. 2014, 72, 2394–2401. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Tooth and Subject Characteristics | Envelope | Szmyd | Total | p-Value * |
|---|---|---|---|---|
| Gender | ||||
| Male | 17 (56.7%) | 18 (60%) | 35 (58.3%) | 0.79 |
| Female | 13 (43.3%) | 12 (40%) | 25 (41.7%) | |
| Site of impacted molar | ||||
| Right | 16 (53.3%) | 15 (50%) | 31 (51.7%) | 0.79 |
| Left | 14 (46.7%) | 15 (50%) | 29 (48.3%) | |
| Caries in 3rd molar | ||||
| Yes | 21 (70%) | 14 (46.7%) | 35 (58.3%) | 0.067 |
| No | 9 (30%) | 16 (53.3%) | 25 (41.7%) |
| Variables | Envelope Flap (Mean ± SD) | Szmyd Flap (Mean ± SD) | All Patients (Mean ± SD) | Range |
|---|---|---|---|---|
| Age (Years) | 22.50 ± 3.07 a | 23.28 ± 3.05 a | 23.22 ± 3.17 | 18–25 |
| Surgical time (minutes) | 24.27 ± 5.62 a | 25.23 ± 6.22 a | 25.18 ± 6.18 | 36–12 |
| Distal pocket Depth (mm) | 1.98 ± 0.18 a | 2.03 ± 0.13 a | 1.97 ± 0.17 | 2.40–1.5 |
| Buccal pocket depth (mm) | 2.03 ± 0.11 a | 1.97 ± 0.12 a | 2.00 ± 0.12 | 2.24–1.5 |
| Distal clinical attachment (mm) | 5.70 ± 0.22 a | 5.85 ± 0.28 a | 5.78 ± 0.26 | 6.34–5.02 |
| Buccal clinical attachment (mm) | 5.94 ± 0.12 a | 6.07 ± 0.008 a | 6.01 ± 0.12 | 6.22–5.58 |
| Distal bone level (mm) | 6.90 ± 0.56 a | 6.71 ± 0.32 a | 7.15 ± 0.23 | 7.90–6 |
| Buccal bone level (mm) | 6.79 ± 0.63 a | 6.87 ± 0.20 a | 6.83 ± 0.47 | 9.70–6.02 |
| Radiographic Finding | Envelope (n = 30) | Szmyd (n = 30) | Total (n = 60) | p-Value |
|---|---|---|---|---|
| Angulations | ||||
| Mesio-angular | 15 (50%) | 11 (36.7%) | 26 (43.3%) | 0.50 |
| Disto-angular | 2 (6.7%) | 5 (16.7%) | 7 (11.7%) | |
| Horizontal | 4 (13.3%) | 6 (20%) | 10 (16.7%) | |
| Vertical | 9 (30%) | 8 (26.7%) | 17 (28.3%) | |
| Root Pattern | ||||
| Conical | 16 (53.3%) | 9 (30%) | 25 (41.7%) | 0.17 |
| Bulbous | 7 (23.3%) | 8 (26.7%) | 15 (25%) | |
| Divergent | 0 (0%) | 2 (6.7%) | 02 (3.3%) | |
| Convergent | 7 (23.3%) | 11 (36.7%) | 18 (30%) | |
| Depth of impacted molar | ||||
| A | 24 (80%) | 27 (90%) | 51 (85%) | 0.47 |
| B | 6 (20%) | 3 (10%) | 9 (15%) | |
| C | 0 (0%) | 0 (0%) | 0 (0%) | |
| Relation with ramus of mandible | ||||
| I | 23 (76.7%) | 24 (80%) | 47 (78.3%) | 0.75 |
| II | 7 (23.3%) | 6 (20%) | 13 (21.7%) | |
| III | 0 (0%) | 0 (0%) | 0 (0%) |
| Periodontal Pocket Depth (PPD) | Flap Design | Baseline | 3rd Month | 6th Month | p-Value * |
|---|---|---|---|---|---|
| Distal | Envelope | 1.92 ± 0.18 Aa | 2.17 ± 0.16 Aa | 2.84 ± 0.13 Ab | (0 mon–3 mon) 0.094 (0 mon–6 mon) 0.007 |
| Szmyd | 2.03 ± 0.13 Ba | 2.19 ± 0.14 Aa | 2.57 ± 0.17 Bb | (0 mon–3 mon) 0.073 (0 mon–6 mon) 0.014 | |
| p-Value § | 0.012 | 0.72 | 0.0001 | ||
| Buccal | Envelope | 2.03 ± 0.11 Aa | 2.32 ± 0.006 Ab | 2.83 ± 0.11 Ac | (0 mon–3 mon) 0.033 (0 mon–6 mon) 0.016 |
| Szmyd | 1.97 ± 0.12 Aa | 2.16 ± 0.008 Bb | 2.38 ± 0.15 Bc | (0 mon–3 mon) 0.046 (0 mon–6 mon) 0.028 | |
| p-Value § | 0.051 | 0.001 | 0.001 |
| Clinical Attachment Loss (CAL) | Flap Design | Baseline | 3rd Month | 6th Month | p-Value * |
|---|---|---|---|---|---|
| Distal | Envelope | 5.70 ± 0.22 Aa | 6.19 ± 0.21 Ab | 6.67 ± 0.18 Ac | (0 mon–3 mon) 0.036 (0 mon–6 mon) 0.027 |
| Szmyd | 5.85 ± 0.28 Aa | 6.39 ± 0.21 Ab | 6.76 ± 0.26 Ac | (0 mon–3 mon) 0.020 (0 mon–6 mon) 0.017 | |
| p-Value § | 0.12 | 0.055 | 0.08 | ||
| Buccal | Envelope | 5.94 ± 0.12 Aa | 6.43 ± 0.12 Ab | 6.91 ± 0.17 Ac | (0 mon–3 mon) 0.034 (0 mon–6 mon) 0.011 |
| Szmyd | 6.07 ± 0.008 Ba | 6.23 ± 0.12 Bb | 6.63 ± 0.14 Bc | (0 mon–3 mon) 0.446 (0 mon–6 mon) 0.015 | |
| p-Value § | 0.0001 | 0.0001 | 0.0001 |
| Bone Loss | Flap Design | Baseline | 3rd Month | 6th Month | p-Value * |
|---|---|---|---|---|---|
| Distal | Envelope | 6.90 ± 0.56 Aa | 7.09 ± 0.009 Ab | 7.64 ± 0.16 Ac | 0.01 |
| Szmyd | 6.71 ± 0.32 Aa | 7.21 ± 0.29 Bb | 7.42 ± 0.38 Bc | 0.01 | |
| p-Value § | 0.11 | 0.03 | 0.006 | ||
| Buccal | Envelope | 6.79 ± 0.63 Aa | 7.39 ± 0.27 Ab | 7.90 ± 0.15 Ac | 0.001 |
| Szmyd | 6.87 ± 0.20 Aa | 7.03 ± 0.21 Bb | 7.34 ± 0.34 Bc | 0.001 | |
| p-Value § | 0.512 | 0.0005 | 0.0005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad, M.; Khan, Z.A.; Khan, T.U.; Alqutub, M.N.; Mokeem, S.A.; AlMubarak, A.M.; Haider, M.; Al-Askar, M.; Ahmed, N.; Aldahiyan, N.; et al. Influence of Surgical Flap Design (Envelope and Szmyd) for Removal of Impacted Mandibular Third Molars on Clinical Periodontal Parameters: A Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 4465. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094465
Ahmad M, Khan ZA, Khan TU, Alqutub MN, Mokeem SA, AlMubarak AM, Haider M, Al-Askar M, Ahmed N, Aldahiyan N, et al. Influence of Surgical Flap Design (Envelope and Szmyd) for Removal of Impacted Mandibular Third Molars on Clinical Periodontal Parameters: A Clinical Trial. International Journal of Environmental Research and Public Health. 2021; 18(9):4465. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094465
Chicago/Turabian StyleAhmad, Muhtada, Zafar Ali Khan, Tahir Ullah Khan, Montaser N. Alqutub, Sameer A. Mokeem, Abdulrahman M. AlMubarak, Mehmood Haider, Mansour Al-Askar, Naseer Ahmed, Nada Aldahiyan, and et al. 2021. "Influence of Surgical Flap Design (Envelope and Szmyd) for Removal of Impacted Mandibular Third Molars on Clinical Periodontal Parameters: A Clinical Trial" International Journal of Environmental Research and Public Health 18, no. 9: 4465. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094465