
The National ReferAll Database: An Open Dataset of Exercise Referral Schemes Across the UK

 , ,
, ,
Abstract
:1. Background
2. Materials and Methods
2.1. Global Data Protection Regulation
2.2. Data Preparation and Cleaning
3. Description of the Dataset
3.1. Scheme and Referral Characteristics
3.2. Outcome Measures
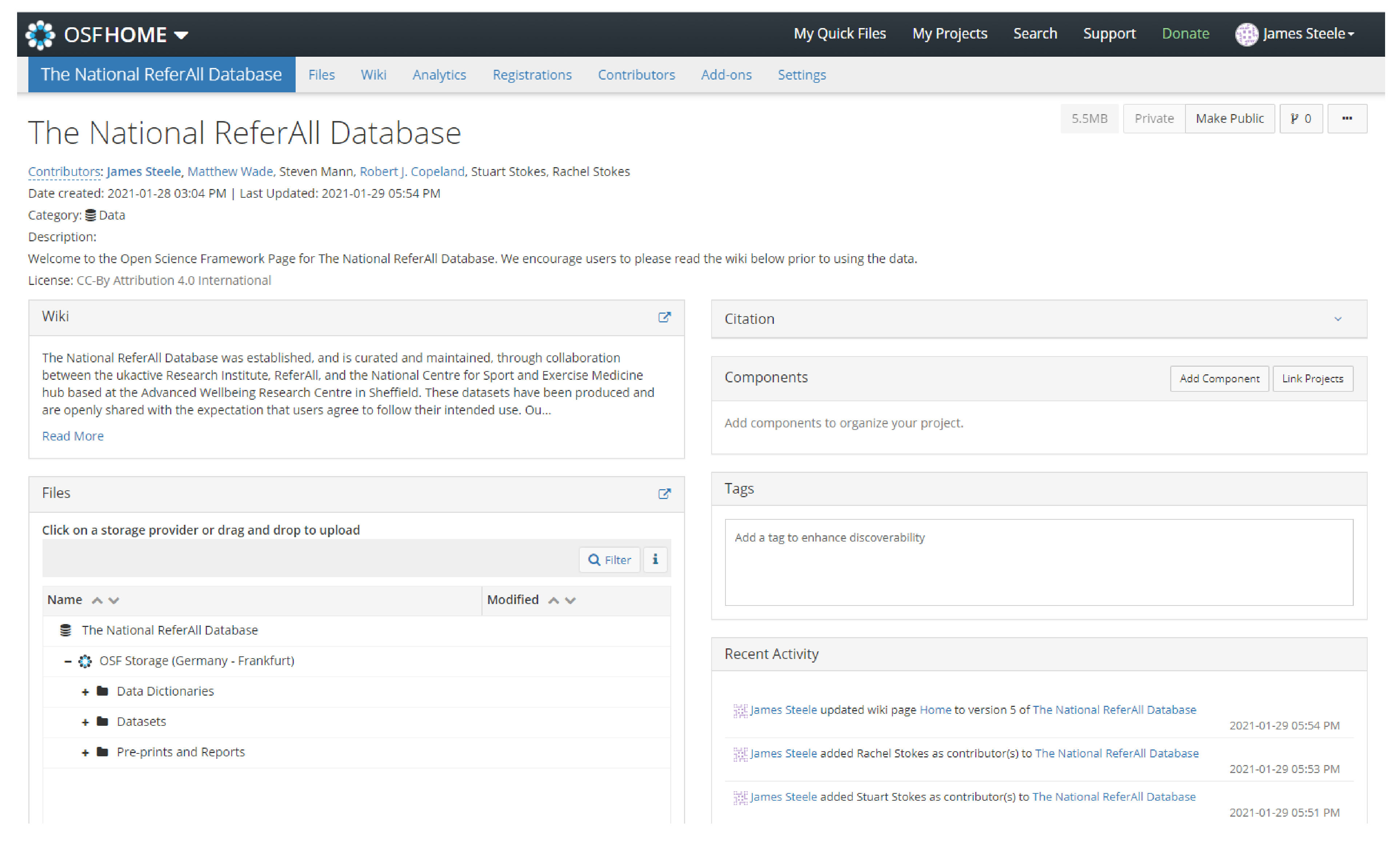
3.3. Open Science Framework Hosting
- Create a dedicated project page to manage research you intend to conduct using The National ReferAll Database datasets. Here, you should host any wider materials, additional data (or note with attribution the relevant version of The National ReferAll Database datasets being used), and any analysis code used;
- Develop proposed research questions or hypotheses to test after initially considering the data dictionaries and then prepare appropriate analysis plans to publicly pre-register on this project page. If not pre-registering, ensure that you report your analysis as purely exploratory;
- Report the results of any analysis first by pre-prints with an open licence through an appropriate pre-print server (e.g., https://osf.io/preprints/sportrxiv/, accessed on 21 April 2021) including links to any subsequent publications in other outlets (i.e., peer-reviewed journal articles).
4. Discussion
5. Conclusions
- Academics and researchers who have expressed interest in the existing data, in addition to plans to enhance the database, and what additional data might be needed to answer key research questions relating to this area;
- Policy makers and stakeholders from key organisations who have expressed interest in the resource and findings generated from it to inform strategy, policy, and investment in this area;
- Practitioners who work within this area who have also expressed interest in the findings generated in order to help guide their practice.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Physical Activity: Exercise Referral Schemes; National Institute for Health and Care Excellence (NICE): London, UK, 2014.
- Pavey, T.G.; Fox, K.; Hillsdon, M.; Anokye, N.; Campbell, J.; Foster, C.; Green, C.; Moxham, T.; Mutrie, N.; Searle, J.; et al. Effect of Exercise Referral Schemes in Primary Care on Physical Activity and Improving Health Outcomes: Systematic Review and Meta-analysis. BMJ 2011, 343, d6462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duda, J.; Williams, G.; Ntoumanis, N.; Daley, A.; Eves, F.; Mutrie, N.; Rouse, P.; Lodhia, R.; Blamey, R.; Jolly, K. Effects of a Standard Provision vs. an Autonomy Supportive Exercise Referral Programme on Physical Activity, Quality of Life and Well-being Indicators: A Cluster Randomised Controlled Trial. Int. J. Behav. Nutr. Phys. Act 2014, 11, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugdill, L.; Graham, R.C.; McNair, F. Exercise Referral: The Public Health Panacea for Physical Activity Promotion? A Critical Perspective of Exercise Referral Schemes; Their Development and Evaluation. Ergonomics 2005, 48, 1390–1410. [Google Scholar] [CrossRef] [PubMed]
- Rowley, N.; Mann, S.; Steele, J.; Horton, E.; Jimenez, A. The Effects of Exercise Referral Schemes in the United Kingdom in Those with Cardiovascular, Mental Health, and Musculoskeletal Disorders: An Updated Systematic Review. BMC Public Health 2018, 18, 949. [Google Scholar] [CrossRef] [Green Version]
- Orrow, G.; Kinmonth, A.-L.; Sanderson, S.; Sutton, S. Effectiveness of Physical Activity Promotion Based in Primary Care: Systematic Review and Meta-analysis of Randomised Controlled Trials. BMJ 2012, 344, e1389. [Google Scholar] [CrossRef] [Green Version]
- Henderson, H.E.; Evans, A.B.; Allen-Collinson, J.; Siriwardena, N.A. The ‘Wild and Wooly’ World of Exercise Referral Schemes: Contested Interpretations of an Exercise as Medicine Programme. Qual. Res. Sport Exerc. Health 2018, 10, 505–523. [Google Scholar] [CrossRef]
- Beedie, C.; Mann, S.; Jimenez, A.; Kennedy, L.; Lane, A.M.; Domone, S.; Wilson, S.; Whyte, G. Death by Effectiveness: Exercise as Medicine Caught in the Efficacy Trap. Br. J. Sports Med. 2016, 50, 323–324. [Google Scholar] [CrossRef] [Green Version]
- Raghupathi, W.; Raghupathi, V. Big Data Analytics in Healthcare: Promise and Potential. Health Inf. Sci. Syst. 2014, 2, 3. [Google Scholar] [CrossRef]
- Chen, Y.; Wu, J.; Haschler, I.; Majeed, A.; Chen, T.; Wetter, T. Academic Impact of a Public Electronic Health Database: Biobliometric Analysis of Studies Using Thegeneral Practice Research Database. PLoS ONE 2011, 6, e21404. [Google Scholar] [CrossRef]
- Morgan, K.; Rahman, M.; Moore, G. Patterning in Patient Referral to and Uptake of a National Exercise Referral Scheme (NERS) in Wales from 2008 to 2017: A Data Linkage Study. Int. J. Environ. Res. Public Health 2020, 17, 3942. [Google Scholar] [CrossRef]
- Physical Activity: Exercise Referral Schemes; National Institute for Health and Care Excellence (NICE): London, UK, 2018. Available online: https://www.nice.org.uk/guidance/ph54/resources/physical-activity-exercise-referral-schemes-pdf-1996418406085 (accessed on 21 April 2021).
- Wade, M.; Mann, S.; Copeland, R.; Batterham, A.; Steele, J. Effect of Exercise Referral Schemes upon Health and Wellbeing: Initial Observational Insights Using Individual Patient Data Meta-analysis from The National ReferrAll Database. J. Epidemiol. Commun. Health 2020, 74, 32–41. [Google Scholar] [CrossRef] [Green Version]
- Oliver, E.J.; Kasim, A.; Dodds-Reynolds, C.; Vallis, D. Community-based Exercise Prescription: Modelling Inequalities in Engagement and Completion Using the National Referral Database. In Proceedings of the Scottish Physical Activity Connections 2019, Edinburgh, UK, 6 November 2019. [Google Scholar]
- Rowley, N.; Steele, J.; Wade, M.; Copeland, R.; Mann, S.; Horton, E.; Jimenez, A. Are Exercise Referral Schemes Effective in Increasing Physical Activity Levels? Observational Findings Using Individual Patient Data Meta-analysis from The National ReferAll Database. J. Phys. Act. Health 2020, 17, 621–631. [Google Scholar] [CrossRef]
- Rocher, L.; Hendrickx, J.; de Montjoye, Y. Estimating the Success of Re-identificatinos in Incomplete Datasets Using Generative Models. Nat. Commun. 2019, 10, 3069. [Google Scholar] [CrossRef]
- Van den Broeck, J.; Cunningham, S.A.; Eeckels, R.; Herbst, K. Data Cleaning: Detecting, Diagnosing, and Editing Data Abnormalities. PLoS Med. 2005, 2, e267. [Google Scholar] [CrossRef] [Green Version]
- IPAQ Group. IPAQ Scoring Protocol. 2005. Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 21 April 2021).
- Milton, K.; Engeli, A.; Townsend, N.; Coombes, E.; Jones, A. The Seleciton of a Project Level Measure of Physical Activity; Sport England: London, UK, 2017. [Google Scholar]
- EuroQol. EQ-5D-5L | About. 2017. Available online: https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/ (accessed on 21 April 2021).
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Welch, S. Internal Construct Validity of the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS): A Rasch Analysis Using Data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Kroll, T.; Kehn, M.; Ho, P.; Groah, S. The SCI Exercise Self-Efficacy Scale (ESES): Development and Psychmetric Properties. Int. J. Behav. Nutr. Phys. Act 2007, 4, 34. [Google Scholar] [CrossRef] [Green Version]
- Hilton, C.; Trigg, R.; Minniti, A. Improving the Psychological Evaluation of Exercise Referral: Psychometric Properties of the Exercise Referral Quality of Life Scale. Health Psychol. Open 2015, 7, 1–12. [Google Scholar] [CrossRef] [Green Version]
- UK Biobank. Available online: https://biobank.ndph.ox.ac.uk/ukb/index.cgi (accessed on 21 April 2021).
- An, P.; Rice, T.; Gagnon, J.; Borecki, I.B.; Pérusse, L.; Leon, A.S.; Skinner, J.S.; Wilmore, J.H.; Bouchard, C.; Rao, D.C. Familial Aggregation of Resting Blood Pressure and Heart Rate in a Sedentary Population: The Heritage Family Study. Am. J. Hypertens. 1999, 12, 264–270. [Google Scholar] [CrossRef] [Green Version]
- Sun, W.; Cai, Z.; Li, Y.; Liu, F.; Fang, S.; Wang, G. Data Processing and Text Mining Technologies on Electronic Medical Recrds: A Review. J. Healthc. Eng. 2018, 20, 4302425. [Google Scholar]
- Silage, J.; Robinson, D. Text Mining with R; O’Reilly: Sebastopol, CA, USA, 2017. [Google Scholar]
- Foster, E.D.; Deardorff, A. Open Science Framework (OSF). J. Med. Libr. Assoc. 2017, 105, 203–206. [Google Scholar]
- Baro, E.; Degoul, S.; Beuscart, R.; Chazard, E. Toward a Literature-driven Definition of Big Data in Healthcare. BioMed Res. Int. 2015, 9, 639021. [Google Scholar] [CrossRef]
- Hanson, C.L.; Oliver, E.J.; Dodds-Reynolds, C.J.; Pearsons, A.; Kelly, P. A Modified Delphi Study to Gain Consensus for a Taxonomy to Report and Classify Physical Actvity Referral Schemes (PARS). Int. J. Behav. Nutr. Phys. Act 2020, 17, 158. [Google Scholar] [CrossRef]
- Borrelli, B. The Assessment, Monitoring, and Enhancement of Treatment Fidelity in Public Health Clinical Trials. J. Public. Health Dent. 2011, 71, S52–S63. [Google Scholar] [CrossRef] [Green Version]
- Buckley, B.J.R.; Thijssen, D.H.J.; Murphy, R.C.; Graves, L.E.F.; Whyte, G.; Gillison, F.B.; Crone, D.; Wilson, P.M.; Watson, P.M. Making a Move in Exercise Referral: Co-development of a Physical Activity Referral Scheme. J. Public Health 2018, 40, e586–e593. [Google Scholar]
- Bickerdike, L.; Booth, A.; Wilson, P.M.; Farley, K.; Wright, K. Social Prescribing: Less Rhetoric and More Reality. A Systematic Review of the Evidence. BMJ Open 2017, 7, e013384. [Google Scholar] [CrossRef]
- The NHS Long Term Plan; NHS: London, UK, 2019. Available online: https://www.longtermplan.nhs.uk/publication/nhs-long-term-plan/ (accessed on 21 April 2021).
- Moffat, S.; Steer, S.; Lawson, S.; Penn, L.; O’Brien, N. Link Worker Social Prescribing to Improve Health and Well-being for People with Long-term Conditions: Qualitative Study of Service Used Perceptions. BMJ Open 2017, 7, e015203. [Google Scholar] [CrossRef] [Green Version]
- Coote, J.H.; Joyner, M.J. Is Precision Medicine the Route to a Healthy World? Lancet 2015, 385, P1617. [Google Scholar]
- Leff, D.R.; Yang, G. Big Data for Precision Medicine. Engineering 2015, 1, 277–279. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, G.; Williamson, P.; Batterham, A.M. Issues in the Determination of ‘Responders’ and ‘Non-responders’ in Physiological Research. Exp. Physiol. 2019, 104, 1215–1225. [Google Scholar] [CrossRef] [PubMed]
- Bertotti, M.; Frostrick, C.; Hutt, P.; Sohanpal, R.; Carnes, D. A Realist Evaluation of Social Prescribing: An Exploration into the Context and Mechanisms Underpinning a Pathway Linking Primary Care with the Voluntary Sector. Prim. Health Care Res. Dev. 2018, 19, 232–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Lang, I.; Byng, R.; Garside, R. What Appraoches to Social Prescribing Work, for Whom, and in What Circumstances? A Realist Review. Health Soc. Care Commun. 2019, 28, 309–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khushnal, A.; Nichols, S.; Carroll, S.; Abt, G.; Ingle, L. Insufficient Exercise Intensity for Clinical Benefit? Monitoring and Quantification of a Commuity-based Phase III Cardiac Rehabilitation Programme: A United Kingdom Perspective. PLoS ONE 2019, 14, e0217654. [Google Scholar]
- Ibeggazene, S.; Moore, C.; Tsakirides, C.; Swainson, M.; Ipsoglou, T.; Birch, K. UK Cardiac Rehabilitation for for Purpose? A Community-based Observational Cohort Study. BMJ Open 2020, 10, e037980. [Google Scholar] [CrossRef]
- Shore, C.B.; Hubbard, G.; Gorely, T.; Polson, R.; Hunter, A.; Galloway, S.D. Insufficient Reporting of Factors Associated with Exercise Referral Scheme Uptake, Attendance, and Adherence: A Systematic Review of Reviews. J. Phys. Act Health 2019, 16, 667–676. [Google Scholar] [CrossRef]
- Eynon, M.; Foad, J.; Downey, J.; Bowmer, Y.; Mills, H. Assessing the Psychosocial Factors Associated with Adherence to Exercise Referral Schemes: A Systematic Review. Scand. J. Med. Sci. Sports 2019, 29, 638–650. [Google Scholar] [CrossRef]
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R.; Beck, B.; Bennell, K.; Brosseau, L.; Costa, L.; Cramp, F.; Feehan, E.C.L.; et al. Consensus on Exercise Reporting Template (CERT): Modified delphi study. Phys. Ther. 2016, 96, 1514–1524. [Google Scholar] [CrossRef]
- Rowley, N.; Steele, J.; Mann, S.; Jimenez, A.; Horton, E. Delivery Approaches within Exercise Referrral Schemes: A Survey of Current Practice in England. J. Phys. Act Health 2021, 18, 357–373. [Google Scholar] [CrossRef]
- Large Simple Trials Now and Looking Forward. In Large Simple Trials and Knowledge Generation in a Learning Health System: Workshop Summary; Roundtable on Value and Science-Driven Health Care; Forum on Drug Discovery, Development, and Translation; Board on Health Sciences Policy; Institute of Medicine; National Academies Press: Washington, DC, USA, 2013. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK201271/ (accessed on 21 April 2021).
- Stiglic, G.; Kocbek, P.; Fijacko, N.; Sheikh, A.; Pajnkihar, M. Challenges Associated with Missing Data in Electronic Health Records: A Case Study of a Risk Prediction Model for Diabetes Using Data from Slovenian Primary Care. Health Inform. J. 2019, 25, 951–959. [Google Scholar] [CrossRef]
- Groenwold, R.H.H. Informative Missingness in Electronic Health Record Systems: The Curse of Knowing. Diagn. Progn. Res. 2020, 4, 8. [Google Scholar]
- Taylor, A.; Taylor, R.S.; Ingram, W.; Fean, S.G.; Jolly, K.; Mutrie, N.; Lambert, J.; Yardley, L.; Streeter, A.; Greaves, C.; et al. Randomised Controlled Trial of an Augmented Exercise Referral Scheme Using Web-based Behavioural Support for Inactive Adults with Chronic Health Conditions: The E-coacER Trial. Br. J. Sports Med. 2021, 55, 444–450. [Google Scholar]
- A Connected Society: A Stratgegy for Tackling Loneliness–Laying the Foudnations for Change; DDCMS; HM Government: London, UK, 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/750909/6.4882_DCMS_Loneliness_Strategy_web_Update.pdf (accessed on 21 April 2021).


{kind=link}
| Variable | Measurement and Units | Range | Source |
|---|---|---|---|
| International Physical Activity Questionnaire—Short Form | MET/Minutes and Categorical | Standard cleaning and analysis procedures for the IPAQ were followed | [18] |
| Short Active Lives | Days Per Week and Minutes Per Week and Categorical | Standard cleaning and analysis procedures for the Short Active Lives were followed | [19] |
| EQ-5D-5L | Visual Analogue Scale (0–100%) and Health Related Quality of Life (0–1) | Standard cleaning and analysis procedures for the EQ-5D-5L were followed using the crosswalk conversion value set for the UK | [20] |
| World Health Organization Well-Being Index | Total Score (0–25 pts) | Cleaned to range 0 pts to 25 pts i.e., impossible scores based on scale were removed | [21] |
| Warwick–Edinburgh Mental Wellbeing Scale | Total Score (0–70 pts) | Cleaned to range 14 pts to 70 pts i.e., impossible scores based on scale were removed | [22] |
| Short Warwick–Edinburgh Mental Wellbeing Scale | Total Score (0–35 pts) | Cleaned to range 7 pts to 35 pts i.e., impossible scores based on scale were removed | [22] |
| Exercise Self Efficacy Scale | Total Score (4–40 pts) | Cleaned to range 4 pts to 40 pts i.e., impossible scores based on scale were removed | [23] |
| Exercise Related Quality of Life Scale | Total Score (22–110 pts) | Cleaned to range 22 pts to 110 pts i.e., impossible scores based on scale were removed | [24] |
| Height | Centimetres (cm) | Cleaned to range of 122.5 cm to 205 cm | [25] |
| Weight | Kilograms (kg) | Cleaned to range of 40 kg to 180 kg | [25] |
| Body Mass Index | Kilograms Per Metre Squared (kg.m2) | Cleaned to range of 12 kg.m2 to 75 kg.m2 | [25] |
| Waist Circumference | Centimetres (cm) | Cleaned to range of 20 cm to 197 cm | [25] |
| Hip Circumference | Centimetres (cm) | Cleaned to range of 30 cm to 195 cm | [25] |
| Resting Heart Rate | Beats Per Minute (fc) | Pre/post cleaned range to 40 fc to 110 fc | [26] |
| Characteristic | N = 39,283 1 |
|---|---|
| Scheme Type | |
| Cancer Rehab | 74 (0.2%) |
| Cardiac Rehab | 416 (1.1%) |
| ESCAPE Pain | 526 (1.3%) |
| Exercise on Referral | 30,590 (78%) |
| Falls Prevention | 2366 (6.0%) |
| Physical Activity | 89 (0.2%) |
| Pulmonary Rehab | 162 (0.4%) |
| Specialist Exercise on Referral | 174 (0.4%) |
| Stroke Rehab | 54 (0.1%) |
| Swim4Health | 182 (0.5%) |
| Weight Management | 4650 (12%) |
| Scheme Length (days) | |
| 42 | 292 (0.7%) |
| 54 | 417 (1.1%) |
| 84 | 20,032 (51%) |
| 90 | 12,019 (31%) |
| 168 | 6224 (16%) |
| 175 | 299 (0.8%) |
| 42 | 292 (0.7%) |
| Referrer Organisation Type | |
| Community | 3753 (9.6%) |
| Hospital | 2580 (6.6%) |
| Housing | 5 (<0.1%) |
| Medical Centre | 6723 (17%) |
| Outreach | 2262 (5.8%) |
| Pharmacy | 70 (0.2%) |
| School | 2 (<0.1%) |
| Surgery | 23,888 (61%) |
| Referrer Type | |
| Adult Nurse | 4276 (11%) |
| Advanced Nurse Practitioner | 183 (0.5%) |
| Alcohol Liaison Nurse | 2 (<0.1%) |
| Art Therapist | 5 (<0.1%) |
| BB Nurse | 3 (<0.1%) |
| Cancer Nurse Specialist | 40 (0.1%) |
| Cardiac Nurse | 226 (0.6%) |
| Cardiac Physiologist | 35 (<0.1%) |
| Cardiac Physiotherapist | 51 (0.1%) |
| Cardiac Rehab Professional | 41 (0.1%) |
| Cardiac Sister | 25 (<0.1%) |
| Cardiologist | 4 (<0.1%) |
| Change Coach | 2 (<0.1%) |
| Clinical Nurse Specialist | 8 (<0.1%) |
| Clinical Psychologist | 9 (<0.1%) |
| Community Diabetes Team | 9 (<0.1%) |
| Community Dietitian | 11 (<0.1%) |
| Community Mental Health Worker | 102 (0.3%) |
| Community Midwife | 13 (<0.1%) |
| Community Physiotherapist | 75 (0.2%) |
| Community Psychiatric Nurse | 35 (<0.1%) |
| Consultant | 41 (0.1%) |
| Consultant Psychiatrist | 3 (<0.1%) |
| Counsellor | 64 (0.2%) |
| Critical Care Technologist | 4 (<0.1%) |
| Dietitian | 89 (0.2%) |
| Doctor | 8674 (22%) |
| Drama Therapist | 1 (<0.1%) |
| Exercise Specialist | 226 (0.6%) |
| Family Support Worker | 23 (<0.1%) |
| General Practitioner | 7985 (20%) |
| Gynaecologist | 6 (<0.1%) |
| Health Education and Promotion Officer | 72 (0.2%) |
| Health Improvement Officer | 256 (0.7%) |
| Health Improvement Practitioner | 54 (0.1%) |
| Health Professional | 5 (<0.1%) |
| Health Support Worker | 1832 (4.7%) |
| Health Trainer | 364 (0.9%) |
| Health Trainer Coordinator | 40 (0.1%) |
| Health Visitor | 14 (<0.1%) |
| Healthcare Assistant | 804 (2.0%) |
| Healthy Lifestyle Motivator | 63 (0.2%) |
| Key Worker | 6 (<0.1%) |
| Lead Nurse Diabetes | 1 (<0.1%) |
| Learning Disability Nurse | 1 (<0.1%) |
| Mental Health Nurse | 111 (0.3%) |
| Mental Health Practitioner | 42 (0.1%) |
| Mental Health Support Worker | 82 (0.2%) |
| Mental Health Worker | 52 (0.1%) |
| Midwife | 21 (<0.1%) |
| Neurosurgeon | 1 (<0.1%) |
| NHS Health Check Nurse | 4 (<0.1%) |
| Nurse | 5077 (13%) |
| Nursing Assistant | 2 (<0.1%) |
| Occupational Therapist | 123 (0.3%) |
| Orthopaedic Technician | 5 (<0.1%) |
| Other Health Professional | 667 (1.7%) |
| Paediatrician | 2 (<0.1%) |
| Paramedic | 2 (<0.1%) |
| Pharmacist | 126 (0.3%) |
| Phlebotomist | 1 (<0.1%) |
| Physiotherapist | 3281 (8.4%) |
| Physiotherapy Assistant | 97 (0.2%) |
| Podiatrist/Chiropodist | 10 (<0.1%) |
| Practice Nurse | 2445 (6.2%) |
| Prevention Worker | 17 (<0.1%) |
| Psychiatrist | 4 (<0.1%) |
| Psychologist | 26 (<0.1%) |
| Psychotherapist | 158 (0.4%) |
| Pulmonary Physio | 46 (0.1%) |
| Recovery Workers | 532 (1.4%) |
| Respiratory Physiology Technician | 1 (<0.1%) |
| Respiratory Therapist | 52 (0.1%) |
| Rheumatology Nurse | 5 (<0.1%) |
| Senior Health Trainer | 192 (0.5%) |
| Senior Physiotherapist | 142 (0.4%) |
| Social Prescriber | 14 (<0.1%) |
| Social Worker | 40 (0.1%) |
| Specialist Health Improvement Practitioner | 23 (<0.1%) |
| Staff Nurse | 30 (<0.1%) |
| Technical Instructor | 16 (<0.1%) |
| Therapy Assistant | 51 (0.1%) |
| Referral Status | |
| Completed | 15,680 (40%) |
| Intends To Participate | 518 (1.3%) |
| Left Early | 8027 (20%) |
| Not Participating | 9590 (24%) |
| Participating | 3721 (9.5%) |
| Referred | 1747 (4.4%) |
| Index of Multiple Deprivation (percentile) | 26 (14, 35) |
| Unknown | 19,250 |
| Quintile of Deprivation | |
| 1 | 6176 (19%) |
| 2 | 5859 (18%) |
| 3 | 6092 (18%) |
| 4 | 6891 (21%) |
| 5 | 8364 (25%) |
| Unknown | 5901 |
| Rural and Urban Classification (RUC11) | |
| Rural town and fringe | 2199 (6.0%) |
| Rural town and fringe in a sparse setting | 5 (<0.1%) |
| Rural village and dispersed | 1445 (4.0%) |
| Rural village and dispersed in a sparse setting | 10 (<0.1%) |
| Urban city and town | 17,947 (49%) |
| Urban major conurbation | 13,905 (38%) |
| Urban minor conurbation | 948 (2.6%) |
| Unknown | 2824 |
| Referral in Scheme Area? | |
| Yes | 38,627 (98%) |
| No | 656 (2%) |
| Ethnic Group | |
| Asian | 256 (0.7%) |
| Black | 1272 (3.2%) |
| Mixed | 203 (0.5%) |
| Other | 149 (0.4%) |
| Unknown/Withheld | 26,650 (68%) |
| White | 10,753 (27%) |
| Ethnicity | |
| African | 551 (1.4%) |
| Arab | 17 (<0.1%) |
| Bangladeshi | 20 (<0.1%) |
| British | 10,328 (26%) |
| Caribbean | 621 (1.6%) |
| Chinese | 10 (<0.1%) |
| Gypsy or Irish Traveller | 2 (<0.1%) |
| Indian | 93 (0.2%) |
| Irish | 81 (0.2%) |
| Other Asian background | 95 (0.2%) |
| Other Black background | 100 (0.3%) |
| Other Ethnic group | 132 (0.3%) |
| Other Mixed background | 68 (0.2%) |
| Other White background | 342 (0.9%) |
| Pakistani | 38 (<0.1%) |
| Unknown | 3 (<0.1%) |
| Unknown/Withheld | 26,647 (68%) |
| White and Asian | 19 (<0.1%) |
| White and Black African | 40 (0.1%) |
| White and Black Caribbean | 76 (0.2%) |
| Age at Referral (years) | 52 (39, 63) |
| Gender | |
| Female | 26,384 (67%) |
| Male | 12,795 (33%) |
| Transgender | 30 (<0.1%) |
| Unknown | 74 (0.2%) |
| Employment Status | |
| Carer | 135 (0.3%) |
| Employed full time | 429 (1.1%) |
| Employed full time/part time | 380 (1.0%) |
| Employed part time | 338 (0.9%) |
| Full-time Student | 6 (<0.1%) |
| Full time carer | 16 (<0.1%) |
| Intermediate | 59 (0.2%) |
| Long term sick/disabled | 18 (<0.1%) |
| Look after home of family | 6 (<0.1%) |
| Looking after home/family full time | 32 (<0.1%) |
| Managerial/Professional | 102 (0.3%) |
| Other | 142 (0.4%) |
| Permanently sick/disabled | 134 (0.3%) |
| Retired | 2893 (7.4%) |
| Routine & Manual | 71 (0.2%) |
| Self-employed | 73 (0.2%) |
| Sick/Disabled/Unable to Work | 83 (0.2%) |
| Student | 71 (0.2%) |
| Unemployed | 1747 (4.5%) |
| Unknown | 32,455 (83%) |
| Volunteer | 9 (<0.1%) |
| Unknown (not completed) | 84 |
| Marital Status | |
| Civil partnership | 3 (<0.1%) |
| Co-habiting | 53 (0.1%) |
| Divorced | 96 (0.2%) |
| Married | 919 (2.3%) |
| Other | 3 (<0.1%) |
| Prefer not to say | 55 (0.1%) |
| Separated | 15 (<0.1%) |
| Single | 132 (0.3%) |
| Unknown | 37,887 (96%) |
| Widowed | 120 (0.3%) |
| Sexual Orientation | |
| Bi/Bisexual | 18 (<0.1%) |
| Gay man | 2 (<0.1%) |
| Gay woman/Lesbian | 8 (<0.1%) |
| Gay/Lesbian | 19 (<0.1%) |
| Heterosexual/Straight | 2892 (7.4%) |
| Other | 6 (<0.1%) |
| Prefer not to say | 578 (1.5%) |
| Unknown | 35,760 (91%) |
| Number of Outcome Measures (times) | |
| 1 | 35,480 (90%) |
| 2 | 2061 (5.2%) |
| 3 | 1475 (3.8%) |
| 4 | 185 (0.5%) |
| 5 | 78 (0.2%) |
| 6 | 4 (<0.1%) |
| Characteristic | N = 39,283 1 |
|---|---|
| IPAQ (MET/Minutes) | 396 (0, 1386) |
| Unknown | 30,642 |
| IPAQ (Category) | |
| 1 | 5263 (61%) |
| 2 | 2330 (27%) |
| 3 | 1048 (12%) |
| Unknown | 30,642 |
| Sport England Single Item Metric (days) | |
| 0 | 2079 (35%) |
| 1 | 1060 (18%) |
| 2 | 670 (11%) |
| 3 | 578 (9.7%) |
| 4 | 316 (5.3%) |
| 5 | 373 (6.2%) |
| 6 | 126 (2.1%) |
| 7 | 787 (13%) |
| Unknown | 33,294 |
| Short Active Lives (Total Minutes) | 32 (0, 176) |
| Unknown | 38,855 |
| Short Active Lives (Category) | |
| 1 | 205 (48%) |
| 2 | 103 (24%) |
| 3 | 120 (28%) |
| Unknown | 38,855 |
| EQ-5D-5L (Visual Analogue Scale) | 50 (50, 50) |
| Unknown | 36,220 |
| EQ-5D-5L (Health Related Quality of Life) | 1.00 (0.84, 1.00) |
| Unknown | 36,220 |
| WHO-5 (%) | 56 (36, 68) |
| Unknown | 35,804 |
| WEMWBS (pts) | 49 (41, 56) |
| Unknown | 38,532 |
| SWEMWBS (pts) | 26.0 (22.0, 30.0) |
| Unknown | 35,973 |
| Weight (kg) | 86 (73, 100) |
| Unknown | 33,675 |
| Height (cm) | 167 (161, 174) |
| Unknown | 33,794 |
| Body Mass Index (kg.m2) | 30 (26, 35) |
| Unknown | 33,799 |
| Waist Circumference (cm) | 102 (90, 114) |
| Unknown | 38,548 |
| Hip Circumference (cm) | 111 (100, 120) |
| Unknown | 38,984 |
| Waist:Hip Ratio | 0.93 (0.86, 1.00) |
| Unknown | 38,985 |
| Systolic Blood Pressure (mmHg) | 130 (119, 143) |
| Unknown | 35,681 |
| Diastolic Blood Pressure (mmHg) | 81 (74, 89) |
| Unknown | 35,681 |
| Resting Heart Rate (fc) | 78 (69, 86) |
| Unknown | 35,808 |
| 30 Second Sit to Stand (n) | 4.0 (0.0, 10.0) |
| Unknown | 38,993 |
| Exercise Self Efficacy Scale (pts) | 31.0 (28.0, 35.0) |
| Unknown | 39,195 |
| Exercise Related Quality of Life (pts) | 74 (65, 82) |
| Unknown | 37,528 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steele, J.; Wade, M.; Copeland, R.J.; Stokes, S.; Stokes, R.; Mann, S. The National ReferAll Database: An Open Dataset of Exercise Referral Schemes Across the UK. Int. J. Environ. Res. Public Health 2021, 18, 4831. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094831
Steele J, Wade M, Copeland RJ, Stokes S, Stokes R, Mann S. The National ReferAll Database: An Open Dataset of Exercise Referral Schemes Across the UK. International Journal of Environmental Research and Public Health. 2021; 18(9):4831. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094831
Chicago/Turabian StyleSteele, James, Matthew Wade, Robert J. Copeland, Stuart Stokes, Rachel Stokes, and Steven Mann. 2021. "The National ReferAll Database: An Open Dataset of Exercise Referral Schemes Across the UK" International Journal of Environmental Research and Public Health 18, no. 9: 4831. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094831