
Respiratory Infections Following Earthquake-Induced Tsunamis: Transmission Risk Factors and Lessons Learned for Disaster Risk Management


Abstract
:1. Introduction
2. Methods
Search Strategy
3. Results
3.1. Study Selection
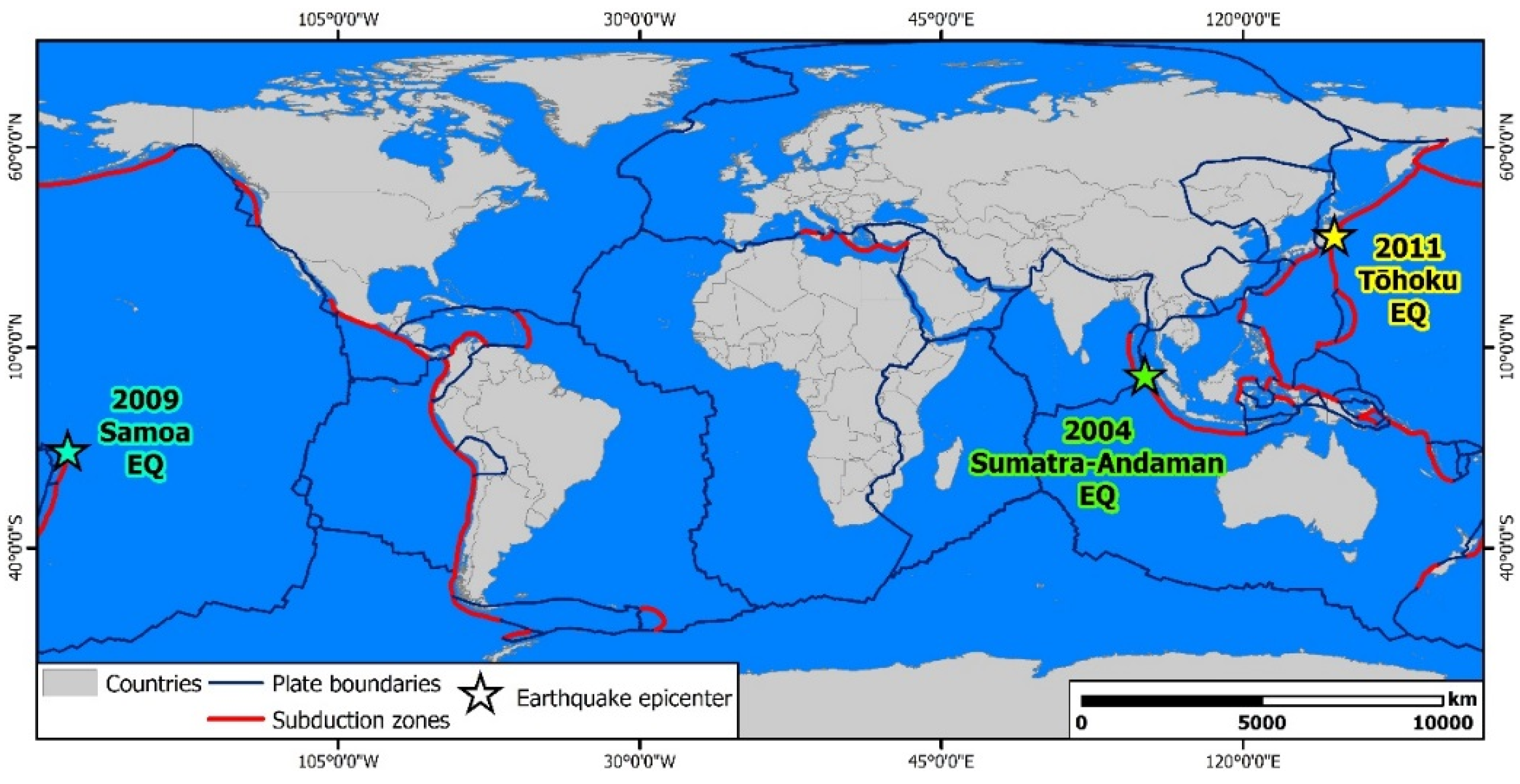
3.2. The Studied Tsunami
3.2.1. The 2004 Indian Ocean Tsunami
3.2.2. The 2009 Samoa Tsunami
3.2.3. The 2011 Great East Japan Tsunami
3.3. Respiratory Infectious Diseases Following Earthquake-Induced Tsunami
3.3.1. Tsunami Lung

{kind=link}
{kind=link}
| Source | Tsunami | Patients | Clinical Presentation—Causative Pathogens |
|---|---|---|---|
| [11] | 1 | 37 patients | Aspiration pneumonia (n = 17), pneumothorax (n = 7), pneumomediastinum (n = 3), B. pseudomallei (n = 2) |
| [29] | 1 | Epidemic peak of admitted pneumonia, tsunami lung was present in many survivors from the Asian tsunami | |
| [30] | 1 |
| Upper respiratory tract infections (mild cough, sore throat), some due to aspiration of sea water |
| [31] | 1 | 17-year-old female | Pneumonia and hemiparesis (hydropneumothorax and brain abscesses) |
| [32] | 1 | 26 tsunami victims | Pneumothorax/pneumomediastinum (n = 5), bacterial pneumonia (n = 18) Aerobic gram negative bacteria (n ≤ 9) and B.pseudomallei(n = 2), 2 deaths |
| [33] | 1 |
|
|
| [34] | 1 | 6 patients | Melioidosis, B. pseudomallei |
| [35] | 1 | 47 year old Finnish male | Melioidosis, B. pseudomallei |
| [36] | 1 | 17 German patients (10 females, 7 males) | Severe large-scale soft-tissue damage: highly resistant bacterial species, fungi and moulds Pneumonitis and pneumonia: multiply resistant Acinetobacter baumanii (n = 3), multiply resistant Enterococcus faecium, sensitive to glycopeptides only, K. pneumoniae, intermediate sensitive to amikacin only, MRSA, sensitive to fosfomycin, rifampicin, linezolid and glycopeptides only, and S. maltophilia, sensitive to quinolones only) Sinusitis (n = 3-multiply resistant A. baumanii, intermediate sensitive to ampicillin/sulbactam only, E. faecium, sensitive to glycopeptides only, and C. albicans, n = 1-A. fumigatus) |
| [37] | 1 | 72-year-old Italian female | Melioidosis, B. pseudomallei |
| [38] | 1 |
|
|
| [40] | 1 | 35-year-old male | Tsunami sinusitis (A. veronii, K. pneumoniae, E. coli, A. hydrophila, P. mirabilis) |
| [44] | 1 | 4 patients | Melioidosis, B. pseudomallei |
| [45] | 1 |
|
|
| [47] | 1 | 3 patients | Tsunami lung, Pseudallescheria boydii |
| [27] | 2 | 29 patients | Aspiration pneumonia (Streptococcus spp., Pseudomonas aeruginosa, Citrobacter spp., Proteus spp., Klebsiella spp., Pantoea spp., Enterobacter spp.) |
| [41] | 3 | 74-year-old male | Aspiration pneumonia and pleural empyema (Streptococcus sanguinis, S. mitis) |
| [42] | 3 | 31-year-old female | Tsunami sinusitis (Pseudomonas aeruginosa, Proteus vulgaris, Escherichia coli) |
| [28] | 3 | 3 female patients | Severe lung disorders (S. maltophilia, Legionella pneumophila, Burkholderia cepacia, and P. aeruginosa), 3 deaths |
| [48] | 3 | 59-year-old Japanese female | Lung and brain abscesses, S. apiospermum |
| [49] | 3 | 45-year-old male | Tsunami lung, vertebral osteomyelitis (S. apiospermum) |
| [50] | 3 | 73-year-old female | Pneumonia (E. coli), fungal sinusitis and meningitis |
| [52] | 3 | 68-year-old Japanese female | Tsunami lung, S. aurantiacum |
| [53] | 3 | 68-year-old female | Pneumonia (A. fumigatus) |
3.3.2. Acute Respiratory Infections
- Bacterial pneumonia
- Legionellosis
- Influenza infection
- Measles
- Tuberculosis
| Source | Tsunami | Patients | Clinical Presentation—Causative Pathogens |
|---|---|---|---|
| [55] | 1 | 37,492 ARIs cases (WHO) during first five months after the tsunami | The highest percentage of ARI cases occurred within 2 months after the 2004 tsunami. |
| [57] | 1 | 4710 patients in southern Sri Lanka | 1374 (29.2%) patients: trauma-related illnesses 1310 (27.8%) patients: ARIS |
| [68] | 1 | 324 internally displaced persons in 3 different tsunami disaster evacuation camps of Sri Lanka | ARIs caused by various types of H. influenza and S. pneumoniae were prevalent and some of them, including resistant isolates, were potentially transmitted from person to person in tsunami disaster evacuation camps in Sri Lanka. |
| [80] | 1 | 101 measles cases | Measles virus circulated in Cuddalore district following the tsunami, although there was no association between the two events. |
| [82] | 1 | 35 measles cases | The cluster occurred in a susceptible community living in unplanned and crowded camps in Aceh Utara district, Indonesia |
| [85] | 1 | 2 patients | Multiple infection (tuberculosis and melioidosis) |
| [56] | 3 | 1167 patients, 6 shelters | Outbreaks of ARI and acute gastroenteritis occurred in evacuation shelters. |
| [58] | 3 | 7439 patients from 44 shelters | Increased ARI incidence rate in crowded shelters |
| [61] | 3 | 322 patients with respiratory diseases (11 March–9 May 2011), 99 and 105 patients (corresponding periods in 2009 and 2010) | Increase in the absolute numbers of admissions was highest for pneumonia, followed by acute exacerbation of chronic obstructive pulmonary disease (AE-COPD) and asthma attacks |
| [62] | 3 | 17 individuals | Pneumonia in older refugees (possible causes: impaired oral hygiene, frequent aspiration, undernutrition, cold temperatures under unfavorable circumstances) |
| [63] | 3 | 1577 patients | Pneumonia comprised 43% of cases (Streptococcus pneumoniae, Moraxella catarrhalis, Haemophilusinfluenzae) |
| [64] | 3 | inpatients in respiratory medicine departments of regional core hospitals in Miyagi Prefecture | The number of patients diagnosed with CAP was 2.2 times greater in 2011 than in 2010 |
| [65] | 3 | A total of 550 pneumonia hospitalizations were identified, including 325 during the pre-disaster period and 225 cases during the post-disaster period. | A marked increase in the incidence of pneumonia was observed during the 3-month period following the disaster. Leading causative pathogens: S. pneumoniae, H. influenzae and K.pneumoniae. The positivity of H.influenzae increased by 4-fold after 11 March, especially among patients from evacuation shelters. |
| [66] | 3 | 6603 participants died of pneumonia during 1 year after the earthquake. | An earthquake increased the risk of pneumonia death and tsunami additionally increased the risk. |
| [67] | 3 | 49 adults with pneumonia (controls): within 6 weeks before the earthquake 172 adults with community-acquired or health care-associated pneumonia: within the 9 weeks after the earthquake | The number of patients with pneumonia peaked in the first 3 weeks after the earthquake, followed by a gradual decrease starting from 4 weeks after the earthquake. H. influenzae and M. catarrhalis were more predominant than S. pneumoniae |
| [70] | 3 | 75-year-old female | Pulmonary co-infection with Legionella and multiple antibiotic-resistant E. coli |
| [71] | 3 |
| Severe pneumonia potentially caused by L. pneumophila, 2 deaths |
| [73] | 3 |
| An outbreak of influenza A (H3N2) occurred in the ECs after the Great East Japan Earthquake of 2011 |
| [77] | 3 |
| Two post-tsunami outbreaks of influenza A in evacuation centers in Miyagi Prefecture, Japan |
| [78] | 3 | 277 samples tested for influenza virus from Sendai City and evacuation centers in Miyagi Prefecture | Influenza A (H3N2) (n = 112 cases), influenza A (H1N1) 2009 (n = 1 case), influenza B (n = 92 cases) |
| [79] | 3 | 15 individuals found positive for Influenza A in the Kesennuma City General Gymnasium (K-Wave) | The design of the K-wave gymnasium and the separation of evacuees from the patients prevented any further spreading of the influenza epidemic |
| [83] | 3 | 93 pulmonary TB patients (tsunami-affected areas 25, non-tsunami areas 68) | Risk factors for prognosis of TB after the earthquake: advanced age, low serum albumin level, functional status at admission, and oxygen requirement. Most of the cases with pulmonary TB experienced reactivation of latent TB infection |
| [84] | 3 | Monitoring of TB and LTBI patients in coastal and inland shelters of Northern Miyagi Prefecture, Japan | The numbers of TB patients and of patients with LTBI significantly increased in the post-disaster period, especially among evacuees staying in crowded shelters in coastal regions of Northern Miyagi Prefecture |
4. Risk Factors for Emergence and Transmission of RIs and Lessons Learned for Disaster Risk Management
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ward, S.N. Landslide tsunami. J. Geophys. Res. Space Phys. 2001, 106, 11201–11215. [Google Scholar] [CrossRef] [Green Version]
- Helal, M.; Mehanna, M. Tsunamis from nature to physics. Chaos Solitons Fractals 2008, 36, 787–796. [Google Scholar] [CrossRef]
- Sugawara, D.; Minoura, K.; Imamura, F. Tsunamis and Tsunami Sedimentology; Elsevier BV: Amsterdam, The Netherlands, 2008; pp. 9–49. [Google Scholar]
- Bryant, E. Tsunami: The Underrated Hazard, 2nd ed.; Springer Praxis Books: Chichester, UK, 2008. [Google Scholar]
- Reicherter, K. Tsunamis as Paleoseismic Indicators. In Encyclopedia of Earthquake Engineering; J.B. Metzler: Stuttgart, Germany, 2015; pp. 3786–3796. [Google Scholar]
- Kumaraguru, A.K.; Jayakumar, K.; Wilson, J.J.; Ramakritinan, C.M. Impact of the tsunami of 26 December 2004 on the coral reef environment of Gulf of Mannar and Palk Bay in the southeast coast of India. Curr. Sci. 2005, 89, 1729–1741. [Google Scholar]
- Meilianda, E.; Dohmen-Janssen, C.M.; Maathuis, B.H.P.; Hulscher, S.J.M.H.; Mulder, J.P.M. Beach Morphology at Banda Aceh, Indonesia in Response to the Tsunami on 26 December 2004. Coast. Sediments 2007, 1019–1032. [Google Scholar] [CrossRef]
- Goff, J.R.; Lane, E.; Arnold, J. The tsunami geomorphology of coastal dunes. Nat. Hazards Earth Syst. Sci. 2009, 9, 847–854. [Google Scholar] [CrossRef] [Green Version]
- Lekkas, E.L.; Andreadakis, E.; Kostaki, I.; Kapourani, E. A Proposal for a New Integrated Tsunami Intensity Scale (ITIS-2012). Bull. Seism. Soc. Am. 2013, 103, 1493–1502. [Google Scholar] [CrossRef]
- Costa, P.J.M.; Andrade, C.; Dawson, S. Geological Recognition of Onshore Tsunami Deposits. In Coastal Wetlands: Alteration and Remediation; Springer Science and Business Media LLC: Berlin/Heidelgberg, Germany, 2014; Volume 8, pp. 3–32. [Google Scholar]
- Kongsaengdao, S.; Bunnag, S.; Siriwiwattnakul, N. Treatment of survivors after the tsunami. N. Engl. J. Med. 2005, 352, 2654–2655. [Google Scholar] [CrossRef]
- Lim, P.L. Wound infections in tsunami survivors: A commentary. Ann. Acad. Med. Singap. 2005, 34, 582–585. [Google Scholar]
- Keim, M. Cyclones, tsunamis, and human health: The key role of preparedness. Oceanography 2006, 19, 40–49. [Google Scholar] [CrossRef]
- Keim, M.E. Health-related impacts of Tsunami disasters. Reg. Airpt. 2013, 1, 139–154. [Google Scholar] [CrossRef]
- Rubonis, A.V.; Bickman, L. Psychological impairment in the wake of disaster: The disaster–psychopathology relationship. Psychol. Bull. 1991, 109, 384–399. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for South-East Asia (2005). WHO Framework for Mental Health and Psychosocial Support After the Tsunami; WHO Regional Office for South-East Asia: New Delhi, India, 2005. [Google Scholar]
- Kouadio, I.K.; Aljunid, S.; Kamigaki, T.; Hammad, K.; Oshitani, H. Infectious diseases following natural disasters: Prevention and control measures. Expert Rev. Anti-Infect. 2012, 10, 95–104. [Google Scholar] [CrossRef]
- World Health Organization. Communicable Diseases Following Natural Disasters–Risk Assessment and Priority Interventions. Pro-gramme on Disease Control in Humanitarian Emergencies Communicable Diseases Cluster; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Lay, T.; Kanamori, H.; Ammon, C.J.; Nettles, M.; Ward, S.N.; Aster, R.C.; Beck, S.L.; Bilek, S.L.; Brudzinski, M.R.; Butler, R.; et al. The great sumatra-andaman earthquake of 26 December 2004. Science 2005, 308, 1127–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammon, C.J.; Ji, C.; Thio, H.-K.; Robinson, D.; Ni, S.; Hjorleifsdottir, V.; Kanamori, H.; Lay, T.; Das, S.; Helmberger, D.; et al. Rupture Process of the 2004 Sumatra-Andaman Earthquake. Science 2005, 308, 1133–1139. [Google Scholar] [CrossRef] [Green Version]
- Okal, E.A.; Fritz, H.M.; Synolakis, C.E.; Borrero, J.C.; Weiss, R.; Lynett, P.J.; Titov, V.V.; Foteinis, S.; Jaffe, B.E.; Liu, P.L.-F.; et al. field survey of the samoa tsunami of 29 September 2009. Seism. Res. Lett. 2010, 81, 577–591. [Google Scholar] [CrossRef]
- Baldridge, S.; Fritz, H.; Synolakis, C.; Borrero, J.; Okal, E.; Weiss, R.; Lynett, P.; Titov, V.; Jaffe, B.; Foteinis, S.; et al. Learning from Earthquakes—Samoa Earthquake and Tsunami of September 29, 2009. EERI Spec. Earthq. Rep. 2011, 107, 1–8. [Google Scholar]
- Ito, T.; Ozawa, K.; Watanabe, T.; Sagiya, T. Slip distribution of the 2011 off the Pacific coast of Tohoku Earthquake inferred from geodetic data. Earth. Planets. Space. 2011, 63, 627–630. [Google Scholar] [CrossRef] [Green Version]
- Lekkas, E.; Andreadakis, E.; Alexoudi, V.; Kapourani, E.; Kostaki, I. The Mw = 9.0 Tohoku Japan Earthquake (March 11, 2011) Tsunami Impact on Structures and Infrastructure. In Proceedings of the 15th Word Conference on Earthquake Engineering, Lisboa, Portugal, 24–28 September 2012. [Google Scholar]
- National Police Agency of Japan. Damage Situation and Police Countermeasures Associated with 2011 Tohoku District-Off the Pacific Ocean Earthquake. Emergency Disaster Countermeasures Headquarters. 2016. Available online: https://reliefweb.int/report/japan/japan-damage-situation-and-police-countermeasures-associated-2011tohoku-district (accessed on 2 November 2020).
- Noji, E.K. The public health consequences of disasters. Prehospital Disaster Med. 2000, 15, 21–31. [Google Scholar] [CrossRef]
- Leong-Nowell, T.A.; Leavai, F.; Ah Ching, L.; Fiu, L.; Wyber, R.; Nisbet, M.; Jones, D.; Blackmore, T.; Ioane-Cleverley, Τ. As-piration pneumonia and challenges following the Samoa Tsunami in 2009. N. Z. Med. J. 2012, 125, 70–78. [Google Scholar] [PubMed]
- Inoue, Y.; Fujino, Y.; Onodera, M.; Kikuchi, S.; Shozushima, T.; Ogino, N.; Mori, K.; Oikawa, H.; Koeda, Y.; Ueda, H.; et al. Tsunami lung. J. Anesth. 2012, 26, 246–249. [Google Scholar] [CrossRef]
- Wiwanitkit, V. Emerging of admitted pneumonia after tsunami in phuket, Thailand. Can. Respir. J. 2005, 12, 224. [Google Scholar] [CrossRef]
- Fan, S.W. Clinical cases seen in tsunami hit Banda Aceh: From a primary health care perspective. Ann. Acad. Med. Singap. 2006, 35, 54–59. [Google Scholar] [PubMed]
- Kao, A.Y.; Munandar, R.; Ferrara, S.L.; Systrom, D.M.; Sheridan, R.L.; Cash, S.S.; Ryan, E.T. Case 19-2005. New Engl. J. Med. 2005, 352, 2628–2636. [Google Scholar] [CrossRef]
- Kateruttanakul, P.; Paovilai, W.; Kongsaengdao, S.; Bunnag, S.; Atipornwanich, K.; Siriwatanakul, N. Respiratory complication of tsunami victims in Phuket and Phang-Nga. J. Med. Assoc. Thai. 2005, 88, 754–758. [Google Scholar]
- Yorsaengrat, W.; Chungpaibulpatana, J.; Tunki, B.; Pauvilai, W.; Kititornkul, S.; Suntong, B. Respiratory complication of tsu-nami diaster victims in Vachira Phuket Hospital. J. Med. Assoc. Thai 2006, 89, 518–521. [Google Scholar] [PubMed]
- Chierakul, W.; Winothai, W.; Wattanawaitunechai, C.; Wuthiekanun, V.; Rugtaengan, T.; Rattanalertnavee, J.; Jitpratoom, P.; Chaowagul, W.; Singhasivanon, P.; White, N.J.; et al. Melioidosis in 6 tsunami survivors in Southern Thailand. Clin. Infect. Dis. 2005, 41, 982–990. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, T.; Vaara, M. Burkholderia pseudomallei infections in Finnish tourists injured by the December 2004 tsunami in Thailand. Wkly. Releases 2005, 10, 2656. [Google Scholar] [CrossRef] [PubMed]
- Maegele, M.; Gregor, S.; Yuecel, N.; Simanski, C.; Paffrath, T.; Rixen, D.; Heiss, M.M.; Rudroff, C.; Saad, S.; Perbix, W.; et al. One year ago not business as usual: Wound management, infection and psychoemotional control during tertiary medical care following the 2004 Tsunami disaster in southeast Asia. Crit. Care 2006, 10, R50. [Google Scholar] [CrossRef] [Green Version]
- Ciervo, A.; Mattei, R.; Cassone, A. Melioidosis in an italian tourist injured by the tsunami in Thailand. J. Chemother. 2006, 18, 443–444. [Google Scholar] [CrossRef]
- Garzoni, C.; Emonet, S.; Legout, L.; Benedict, R.; Hoffmeyer, P.; Bernard, L.; Garbino, J. Atypical infections in tsunami survivors. Emerg. Infect. Dis. 2005, 11, 1591–1593. [Google Scholar] [CrossRef]
- Masur, H.; Murray, P. Tsunami disaster and infection: Beware what pathogens the transport delivers to your intensive care unit!*. Crit. Care Med. 2005, 33, 1179–1180. [Google Scholar] [CrossRef] [PubMed]
- Limchawalit, K.; Suchato, C. Tsunami sinusitis. New Engl. J. Med. 2005, 352, e23. [Google Scholar] [CrossRef]
- Ota, H.; Kawai, H. An unusual case of pleural empyema in a tsunami survivor. Asian Cardiovasc. Thorac. Ann. 2012, 20, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Baba, S.; Kondo, K.; Kanaya, K.; Suzukawa, K.; Sato, T.; Kurata, H.; Hiruma, T.; Fujita, H.; Yahagi, N.; Yamasoba, T. Tsunami sinusitis. Lancet 2011, 378, 1116. [Google Scholar] [CrossRef]
- White, N. Melioidosis. Lancet 2003, 361, 1715–1722. [Google Scholar] [CrossRef]
- Athan, E.; Allworth, A.M.; Engler, C.; Bastian, I.; Cheng, A.C. Melioidosis in Tsunami Survivors. Emerg. Infect. Dis. 2005, 11, 1638–1639. [Google Scholar] [CrossRef]
- Allworth, A.M. Tsunami lung: A necrotising pneumonia in survivors of the Asian tsunami. Med. J. Aust. 2005, 182, 364. [Google Scholar] [CrossRef]
- Wuthiekanun, V.; Chierakul, W.; Rattanalertnavee, J.; Langa, S.; Sirodom, D.; Wattanawaitunechai, C.; Winothai, W.; White, N.J.; Day, N.; Peacock, S.J. Serological evidence for increased human exposure to burkholderia pseudomallei following the tsunami in Southern Thailand. J. Clin. Microbiol. 2006, 44, 239–240. [Google Scholar] [CrossRef] [Green Version]
- Tintelnot, K.; Wagner, N.; Seibold, M.; De Hoog, G.S.; Horré, R. Re-identification of clinical isolates of the Pseudallescheria boydii-complex involved in near-drowning. Mycoses 2008, 51, 11–16. [Google Scholar] [CrossRef]
- Nakamura, Y.; Utsumi, Y.; Suzuki, N.; Nakajima, Y.; Murata, O.; Sasaki, N.; Nitanai, H.; Nagashima, H.; Miyamoto, S.; Yaegashi, J.; et al. Multiple Scedosporium apiospermum abscesses in a woman survivor of a tsunami in northeastern Japan: A case report. J. Med. Case Rep. 2011, 5, 526. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, J.; Yoshimoto, M.; Takebayashi, T.; Ida, K.; Tanimoto, K.; Yamashita, T. atypical fungal vertebral osteomyelitis in a tsunami survivor of the great East Japan earthquake. Spine 2014, 39, E739–E742. [Google Scholar] [CrossRef]
- Igusa, R.; Narumi, S.; Murakami, K.; Kitawaki, Y.; Tamii, T.; Kato, M.; Sato, M.; Tsuboi, M.; Ota, K. Escherichia coli Pneumonia in combination with fungal sinusitis and meningitis in a tsunami survivor after the great East Japan earthquake. Tohoku J. Exp. Med. 2012, 227, 179–184. [Google Scholar] [CrossRef] [Green Version]
- Chaney, S.; Gopalan, R.; Berggren, R.E. Pulmonary Pseudallescheria boydii infection with cutaneous zygomycosis after near drowning. South Med. J. 2004, 97, 683–687. [Google Scholar] [CrossRef]
- Nakamura, Y.; Suzuki, N.; Nakajima, Y.; Utsumi, Y.; Murata, O.; Nagashima, H.; Saito, H.; Sasaki, N.; Fujimura, I.; Ogino, Y.; et al. Scedosporium aurantiacum brain abscess after near-drowning in a survivor of a tsunami in Japan. Respir. Investig. 2013, 51, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, Y.; Tagami, T.; Kusakabe, T.; Kido, N.; Kawaguchi, T.; Omura, M.; Tosa, R. Disseminated Aspergillosis associated with tsunami Lung. Respir. Care 2012, 57, 1674–1678. [Google Scholar] [CrossRef] [PubMed]
- Bellos, A.; Mulholland, K.; O’Brien, K.L.; A Qazi, S.; Gayer, M.; Checchi, F. The burden of acute respiratory infections in crisis-affected populations: A systematic review. Confl. Health 2010, 4, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guha-Sapir, D.; Van Panhuis, W.G. Health impact of the 2004 Andaman Nicobar earthquake and tsunami in Indonesia. Prehospital Disaster Med. 2009, 24, 493–499. [Google Scholar] [CrossRef] [Green Version]
- Kawano, T.; Hasegawa, K.; Watase, H.; Morita, H.; Yamamura, O. Infectious disease frequency among evacuees at shelters after the great Eastern Japan earthquake and tsunami: A retrospective study. Disaster Med. Public Health Prep. 2014, 8, 58–64. [Google Scholar] [CrossRef]
- Lim, J.H.; Yoon, D.; Jung, G.; Kim, W.J.; Lee, H.-C.S. Medical needs of tsunami disaster refugee camps. Fam. Med. 2005, 37, 422–428. [Google Scholar]
- Kawano, T.; Tsugawa, Y.; Nishiyama, K.; Morita, H.; Yamamura, O.; Hasegawa, K. Shelter crowding and increased incidence of acute respiratory infection in evacuees following the Great Eastern Japan earthquake and tsunami. Epidemiol. Infect. 2015, 144, 787–795. [Google Scholar] [CrossRef] [Green Version]
- Keim, M.E. The public health impact of tsunami disasters. Am. J. Disaster Med. 2011, 6, 341–349. [Google Scholar] [CrossRef]
- Tamiya, N.; Noguchi, H.; Nishi, A.; Reich, M.R.; Ikegami, N.; Hashimoto, H.; Shibuya, K.; Kawachi, I.; Campbell, J.C. Population ageing and wellbeing: Lessons from Japan’s long-term care insurance policy. Lancet 2011, 378, 1183–1192. [Google Scholar] [CrossRef]
- Yamanda, S.; Hanagama, M.; Kobayashi, S.; Satou, H.; Tokuda, S.; Niu, K.; Yanai, M. The impact of the 2011 Great East Japan Earthquake on hospitalisation for respiratory disease in a rapidly aging society: A retrospective descriptive and cross-sectional study at the disaster base hospital in Ishinomaki. BMJ Open 2013, 3, e000865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, M.; Uwano, C.; Ohrui, T.; Ebihara, T.; Yamasaki, M.; Asamura, T.; Tomita, N.; Kosaka, Y.; Furukawa, K.; Arai, H. Shelter-Acquired pneumonia after a catastrophic earthquake in Japan. J. Am. Geriatr. Soc. 2011, 59, 1968–1970. [Google Scholar] [CrossRef]
- Aoyagi, T.; Yamada, M.; Kunishima, H.; Tokuda, K.; Yano, H.; Ishibashi, N.; Hatta, M.; Endo, S.; Arai, K.; Inomata, S.; et al. Characteristics of infectious diseases in hospitalized patients during the early phase after the 2011 great East Japan earthquake. Chest 2013, 143, 349–356. [Google Scholar] [CrossRef]
- Ohkouchi, S.; Shibuya, R.; Yanai, M.; Kikuchi, Y.; Ichinose, M.; Nukiwa, T. Deterioration in regional health status after the acute phase of a great disaster: Respiratory physicians’ experiences of the Great East Japan earthquake. Respir. Investig. 2013, 51, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Daito, H.; Suzuki, M.; Shiihara, J.; E Kilgore, P.; Ohtomo, H.; Morimoto, K.; Ishida, M.; Kamigaki, T.; Oshitani, H.; Hashizume, M.; et al. Impact of the Tohoku earthquake and tsunami on pneumonia hospitalisations and mortality among adults in northern Miyagi, Japan: A multicentre observational study. Thorax 2013, 68, 544–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibata, Y.; Ojima, T.; Tomata, Y.; Okada, E.; Nakamura, M.; Kawado, M.; Hashimoto, S. Characteristics of pneumonia deaths after an earthquake and tsunami: An ecological study of 5.7 million participants in 131 municipalities, Japan. BMJ Open 2016, 6, e009190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, H.; Fujimura, S.; Ubukata, S.; Sato, E.; Shoji, M.; Utagawa, M.; Kikuchi, T.; Watanabe, A. Pneumonia after earthquake, Japan, 2011. Emerg. Infect. Dis. 2012, 18, 1909–1911. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Batuwanthudawe, R.; Thevanesam, V.; Kaji, C.; Qin, L.; Nishikiori, N.; Saito, W.; Saito, M.; Watanabe, K.; Oishi, K.; et al. Possible prevalence and transmission of acute respiratory tract infections caused by streptococcus pneumoniae and haemophilus influenzae among the internally displaced persons in tsunami disaster evacuation camps of Sri Lanka. Intern. Med. 2007, 46, 1395–1402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunha, B.; Burillo, A.; Bouza, E. Legionnaires’ disease. Lancet 2016, 387, 376–385. [Google Scholar] [CrossRef]
- Ebisawa, K.; Yamada, N.; Okada, S.; Suzuki, Y.; Satoh, A.; Kobayashi, M.; Morikawa, N. Combined legionella and escherichia coli lung infection after a tsunami disaster. Intern. Med. 2011, 50, 2233–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakadate, T.; Nakamura, Y.; Yamauchii, K.; Endo, S. Two cases of severe pneumonia after the 2011 Great East Japan earthquake. West. Pac. Surveill. Response J. 2012, 3, 75–78. [Google Scholar] [CrossRef] [Green Version]
- Waring, S.C.; Brown, B.J. The threat of communicable diseases following natural disasters: A public health response. Disaster Manag. Response 2005, 3, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Kamigaki, T.; Seino, J.; Tohma, K.; Nukiwa-Soma, N.; Otani, K.; Oshitani, H. Investigation of an Influenza A (H3N2) outbreak in evacuation centres following the Great East Japan earthquake, 2011. BMC Public Health 2014, 14, 34. [Google Scholar] [CrossRef] [Green Version]
- Simonsen, L.; Clarke, M.J.; Williamson, G.D.; Stroup, D.F.; Arden, N.H.; Schonberger, L.B. The impact of influenza epidemics on mortality: Introducing a severity index. Am. J. Public Health 1997, 87, 1944–1950. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Goldstein, E.; Ho, L.M.; Yang, L.; Nishiura, H.; Wu, J.T.; Ip, D.K.M.; Chuang, S.-K.; Tsang, T.; Cowling, B.J. Excess mortality associated with influenza a and b virus in Hong Kong, 1998–2009. J. Infect. Dis. 2012, 206, 1862–1871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemaitre, M.; Carrat, F.; Rey, G.; Miller, M.; Simonsen, L.; Viboud, C. Mortality burden of the 2009 A/H1N1 influenza pandemic in France: Comparison to seasonal influenza and the A/H3N2 pandemic. PLoS ONE 2012, 7, e45051. [Google Scholar] [CrossRef]
- Hatta, M.; Endo, S.; Tokuda, K.; Kunishima, H.; Arai, K.; Yano, H.; Ishibashi, N.; Aoyagi, T.; Yamada, M.; Inomata, S.; et al. Post-Tsunami outbreaks of influenza in evacuation centers in Miyagi Prefecture, Japan. Clin. Infect. Dis. 2011, 54, 5–7. [Google Scholar] [CrossRef] [Green Version]
- Tohma, K.; Suzuki, A.; Otani, K.; Okamoto, M.; Nukiwa, N.; Kamigaki, T.; Kawamura, K.; Nakagawa, H.; Oshitani, H. Monitoring of influenza viruses in the aftermath of the Great East Japan earthquake. Jpn. J. Infect. Dis. 2012, 65, 542–544. [Google Scholar] [CrossRef] [Green Version]
- Namiki, J.; Kohsaka, S.; Ui, R. Influenza epidemic after the 2011 great East Japan earthquake and tsunami. Disaster Med. Public Health Prep. 2013, 7, 124–126. [Google Scholar] [CrossRef] [Green Version]
- Mohan, A.; Murhekar, M.V.; Wairgkar, N.S.; Hutin, Y.J.; Gupte, M.D. Measles transmission following the tsunami in a population with a high one-dose vaccination coverage, Tamil Nadu, India 2004–2005. BMC Infect. Dis. 2006, 6, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uçkay, I.; Sax, H.; Harbarth, S.; Bernard, L.; Pittet, D. Multi-resistant infections in repatriated patients after natural disasters: Lessons learned from the 2004 tsunami for hospital infection control. J. Hosp. Infect. 2008, 68, 1–8. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization & United Nations Children’s Fund (UNICEF). WHO-UNICEF Joint Statement: Reducing Measles Mortality in Emergencies. World Health Organization, 2004. Available online: https://apps.who.int/iris/handle/10665/68744 (accessed on 27 October 2020).
- Kanamori, H.; Hatakeyama, T.; Uchiyama, B.; Weber, D.J.; Takeuchi, M.; Endo, S.; Hirakata, Y.; Kaku, M. Clinical and molecular epidemiological features of tuberculosis after the 2011 Japan earthquake and tsunami. Int. J. Tuberc. Lung Dis. 2016, 20, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, M.; Takahashi, T.; Ohuchi, M.; Terui, Y.; Kiryu, K.; Shikano, K. Increasing incidence of tuberculosis infection in the coastal Region of Northern Miyagi after the great East Japan earthquake. Tohoku J. Exp. Med. 2016, 238, 187–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Othman, N.; Ismail, I.H.; Yip, R.; Zainuddin, Z.; Kasim, S.M.; Isa, R.; Noh, L.M. Infections in post-tsunami victims. Pediatr. Infect. Dis. J. 2007, 26, 960–961. [Google Scholar] [CrossRef] [PubMed]
- Pio, A.; Kirkwood, B.R.; Gove, S. Avoiding Hypothermia, an Intervention to Prevent Morbidity and Mortality From Pneumonia in Young Children. Pediatr. Infect. Dis. J. 2010, 29, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Laupland, K.B.; Zahar, J.-R.; Adrie, C.; Minet, C.; Vésin, A.; Goldgran-Toledano, D.; Azoulay, E.; Garrouste-Orgeas, M.; Cohen, Y.; Schwebel, C.; et al. Severe hypothermia increases the risk for intensive care unit-acquired infection. Clin. Infect. Dis. 2012, 54, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.G.; Nievergelt, C.M.; O’Connor, D.T. Biomarkers of PTSD: Neuropeptides and immune signaling. Neuropharmacology 2012, 62, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Luft, B.J.; Schechter, C.; Kotov, R.; Broihier, J.; Reissman, D.; Guerrera, K.; Udasin, I.; Moline, J.; Harrison, D.; Friedman-Jimenez, G.; et al. Exposure, probable PTSD and lower respiratory illness among World Trade Center rescue, recovery and clean-up workers. Psychol. Med. 2011, 42, 1069–1079. [Google Scholar] [CrossRef] [Green Version]
- Yano, H.; Suetake, M.; Kuga, A.; Irinoda, K.; Okamoto, R.; Kobayashi, T.; Inoue, M. Pulsed-Field gel electrophoresis analysis of nasopharyngeal flora in children attending a day care center. J. Clin. Microbiol. 2000, 38, 625–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoshino, K.; Watanabe, H.; Sugita, R.; Asoh, N.; Ntabaguzi, S.A.; Watanabe, K.; Oishi, K.; Nagatake, T. High rate of transmission of Penicillin-Resistant Streptococcus pneumoniae between parents and children. J. Clin. Microbiol. 2002, 40, 4357–4359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, H.; Hoshino, K.; Sugita, R.; Asoh, N.; Oishi, K.; Nagatake, T.; Watanabe, K. Possible high rate of transmission of Nontypeable Haemophilus influenzae, including -lactamase-negative ampicillin-resistant strains, between children and their parents. J. Clin. Microbiol. 2004, 42, 362–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.J.; Lee, S.H.; Kim, Y.E.; Cho, Y.J.; Jeong, Y.Y.; Kim, H.C.; Lee, J.D.; Kim, J.R.; Hwang, Y.S.; Kim, H.J.; et al. Risk factors for latent tuberculosis infection in close contacts of active tuberculosis patients in South Korea: A prospective cohort study. BMC Infect. Dis. 2014, 14, 566. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mavrouli, M.; Mavroulis, S.; Lekkas, E.; Tsakris, A. Respiratory Infections Following Earthquake-Induced Tsunamis: Transmission Risk Factors and Lessons Learned for Disaster Risk Management. Int. J. Environ. Res. Public Health 2021, 18, 4952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094952
Mavrouli M, Mavroulis S, Lekkas E, Tsakris A. Respiratory Infections Following Earthquake-Induced Tsunamis: Transmission Risk Factors and Lessons Learned for Disaster Risk Management. International Journal of Environmental Research and Public Health. 2021; 18(9):4952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094952
Chicago/Turabian StyleMavrouli, Maria, Spyridon Mavroulis, Efthymios Lekkas, and Athanassios Tsakris. 2021. "Respiratory Infections Following Earthquake-Induced Tsunamis: Transmission Risk Factors and Lessons Learned for Disaster Risk Management" International Journal of Environmental Research and Public Health 18, no. 9: 4952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094952