
Foot Pain and Morphofunctional Foot Disorders in Patients with Rheumatoid Arthritis: A Multicenter Cross-Sectional Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measurements
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Moreira, E.; Jones, A.; Oliveira, H.; Jennings, F.; Fernandes, A.; Natour, J. Effectiveness of insole use in rheumatoid feet: A randomized controlled trial. Scand. J. Rheumatol. 2016, 45, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Novak, P.; Burger, H.; Tomsic, M.; Marincek, C.; Vidmar, G. Influence of foot orthoses on plantar pressures, foot pain and walking ability of rheumatoid arthritis patients—A randomised controlled study. Disabil. Rehabil. 2009, 31, 638–645. [Google Scholar] [CrossRef]
- Bagherzadeh Cham, M.; Ghasemi, M.S.; Forogh, B.; Sanjari, M.A.; Zabihi Yeganeh, M.; Eshraghi, A. Effect of rocker shoes on pain, disability and activity limitation in patients with rheumatoid arthritis. Prosthet. Orthot. Int. 2013, 38, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Cuesta-Calleja, R.; Polo-García, A.; González-Fernández, M.L. Evidencia cientifica del tratamiento ortopodologico en pie afectado por artritis reumatoide. Rev. Int. Cienc. Podol. 2018, 12, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Otter, S.J.; Lucas, K.; Springett, K.; Moore, A.; Davies, K.; Young, A.; Walker-Bone, K. Comparison of foot pain and foot care among rheumatoid arthritis patients taking and not taking anti-TNFalpha therapy: An epidemiological study. Rheumatol. Int. 2011, 31, 1515–1519. [Google Scholar] [CrossRef]
- Mochizuki, T.; Yano, K.; Ikari, K.; Hiroshima, R.; Ishibashi, M.; Okazaki, K. Relationship of callosities of the forefoot with foot deformity, Health Assessment Questionnaire Disability Index, and joint damage score in patients with rheumatoid arthritis. Mod. Rheumatol. 2020, 30, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Wilson, O.; Hewlett, S.; Woodburn, J.; Pollock, J.; Kirwan, J. Prevalence, impact and care of foot problems in people with rheumatoid arthritis: Results from a United Kingdom based cross-sectional survey. J. Foot Ankle Res. 2017, 10, 1–11. [Google Scholar] [CrossRef]
- Biz, C.; Favero, L.; Stecco, C.; Aldegheri, R. Hypermobility of the first ray in ballet dancer. Muscles Ligaments Tendons J. 2012, 2, 282–288. [Google Scholar] [PubMed]
- Riskowski, J.; Dufour, A.B.; Hannan, M.T. Arthritis, foot pain and shoe wear: Current musculoskeletal research on feet. Curr. Opin. Rheumatol. 2011, 23, 148–155. [Google Scholar] [CrossRef]
- Santos, D.; Cameron-Fiddes, V. Effects of Off-the-Shelf Foot Orthoses on Plantar Foot Pressures in Patients with Early Rheumatoid Arthritis. J. Am. Podiatr. Med. Assoc. 2014, 104, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Barn, R.; Brandon, M.; Rafferty, D.; Sturrock, R.D.; Steultjens, M.; Turner, D.E.; Woodburn, J. Kinematic, kinetic and electromyographic response to customized foot orthoses in patients with tibialis posterior tenosynovitis, pes plano valgus and rheumatoid arthritis. Rheumatology 2014, 53, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Gatt, A.; Formosa, C.; Otter, S. Foot orthoses in the management of chronic subtalar and talo crural joint pain in rheumatoid arthritis. Foot 2016, 27, 27–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenten-Diepenmaat, M.; Leeden Van Der, M.; Vliet Vlieland, T.; Roorda, L.D.; Dekker, J.; Gijon-Nogueron, G.; Ramos-Petersen, L.; Garcia-Mayor, S.; Morales-Asencio, J.M. HPR the effectiveness of therapeutic footwear in patients with rheumatoid arthritis: A systematic review and meta-analysis. Ann. Rheum. Dis. 2017, 76, 1486. [Google Scholar]
- Rome, K.; Clark, H.; Gray, J.; McMeekin, P.; Plant, M.; Dixon, J. Clinical effectiveness and cost-effectiveness of foot orthoses for people with established rheumatoid arthritis: An exploratory clinical trial. Scand. J. Rheumatol. 2017, 46, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenten-Diepenmaat, M.; Dekker, J.; Steenbergen, M.; Huybrechts, E.; Roorda, L.D.; van Schaardenburg, D.; Bus, S.A.; van der Leeden, M. In-shoe plantar pressure measurements for the evaluation and adaptation of foot orthoses in patients with rheumatoid arthritis: A proof of concept study. Gait Posture 2016, 45, 45–50. [Google Scholar] [CrossRef]
- Santos, D. The Effects of off-the-Shelf Foot Orthoses on the Quality of Life of Patients Diagnosed with Early Rheumatoid Arthritis. Clin. Res. Foot Ankle 2015, 3, 1. [Google Scholar] [CrossRef]
- Reina-Bueno, M.; Vázquez-Bautista, M.d.C.; Pérez-García, S.; Rosende-Bautista, C.; Sáez-Díaz, A.; Munuera-Martínez, P.V. Effectiveness of custom-made foot orthoses in patients with rheumatoid arthritis: A randomized controlled trial. Clin. Rehabil. 2019, 33, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Reina-Bueno, M.; Ballesteros-Mora, M.; Rodríguez-Moreno, I.; Vázquez-Bautista, C.; Pérez-García, S.; Rosende-Bautista, C.; Munuera-Martínez, P.V. Efecto de las ortesis plantares hechas a medidas versus placebo en pacientes con artritis reumatoide: Ensayo clínico aleatorizado. Estudio piloto. Rev. Española Podol. 2018, 29, 64–69. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef]
- Redmond, A.C.; Crosbie, J.; Ouvrier, R.A. Development and validation of a novel rating system for scoring standing foot posture: The Foot Posture Index. Clin. Biomech. 2006, 21, 89–98. [Google Scholar] [CrossRef]
- Garrow, A.P.; Papageorgiou, A.; Silman, A.J.; Thomas, E.; Jayson, M.I.; Macfarlane, G.J. The grading of hallux valgus. The Manchester Scale. J. Am. Podiatr. Med. Assoc. 2001, 91, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Reina, M.; Lafuente, G.; Munuera, P.V. Effect of custom-made foot orthoses in female hallux valgus after one-year follow up. Prosthet Orthot Int. 2013, 37, 113–119. [Google Scholar] [CrossRef] [Green Version]
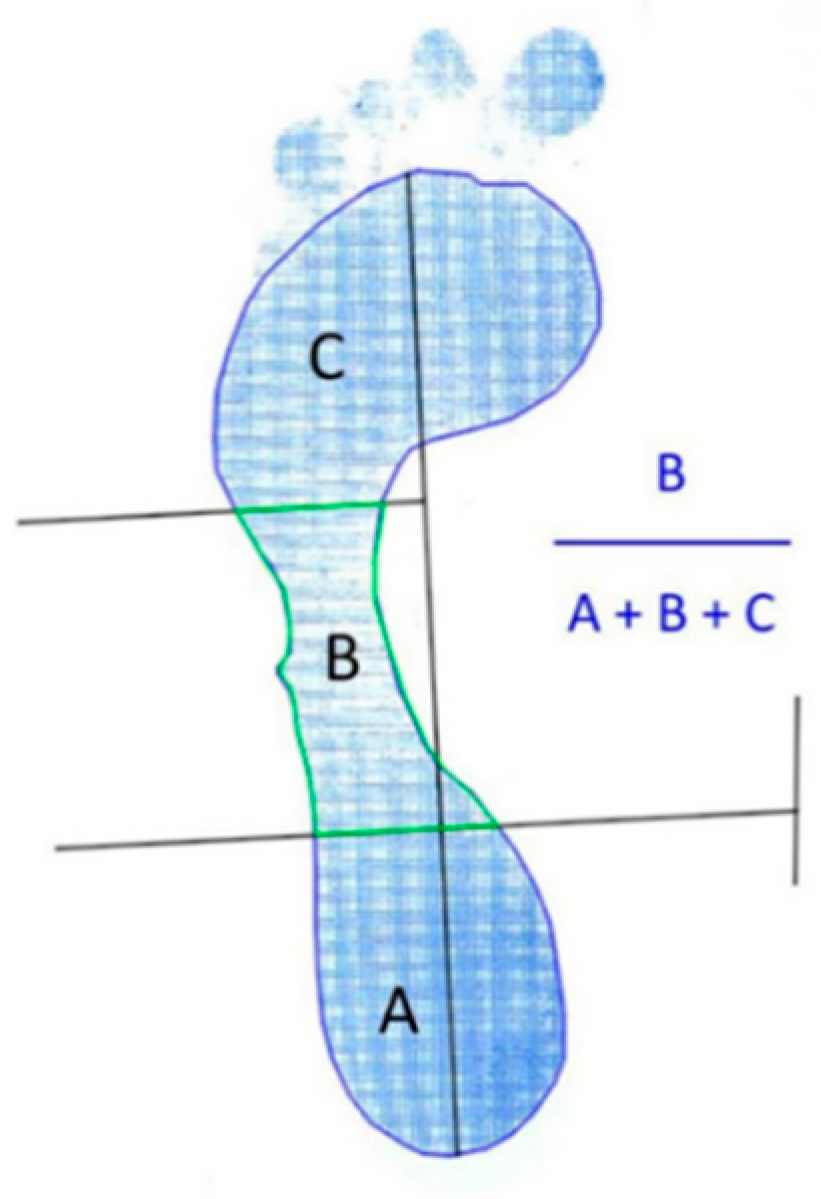
- Cavanagh, P.R.; Rodgers, M. Technical Note the Arch Index: A Useful Measure. J. Biomech. Biomech. 1987, 20, 547–551. [Google Scholar] [CrossRef]
- Landorf, K.B.; Radford, J.A. Minimal important difference: Values for the Foot Health Status Questionnaire, Foot Function Index and Visual Analogue Scale. Foot 2008, 18, 15–19. [Google Scholar] [CrossRef]
- Paez-Moguer, J.; Budiman-Mak, E.; Cuesta-Vargas, A.I. Cross-cultural adaptation and validation of the Foot Function Index to Spanish. Foot Ankle Surg. 2014, 20, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Gijon-Nogueron, G.; Ndosi, M.; Luque-Suarez, A.; Alcacer-Pitarch, B.; Munuera, P.V.; Garrow, A.; Redmond, A.C. Cross-cultural adaptation and validation of the Manchester Foot Pain and Disability Index into Spanish. Qual. Life Res. 2014, 23, 571–579. [Google Scholar] [CrossRef]
- Biscontini, D.; Bartoloni Bocci, E.; Gerli, R. Analysis of Foot Structural Damage in Rheumatoid Arthritis: Clinical Evaluation by Validated Measures and Serological Correlations. Reumatismo 2009, 61, 48–53. [Google Scholar] [CrossRef] [Green Version]
- González-Fernández, M.L.; Valor, L.; Morales-Lozano, R.; Hernández-Flórez, D.; López-Longo, F.J.; Martínez, D.; González, C.M.; Monteagudo, I.; Martínez-Barrio, J.; Garrido, J.; et al. To what extent is foot pain related to biomechanical changes and ultrasound-detected abnormalities in rheumatoid arthritis? Clin. Exp. Rheumatol. 2016, 34, 480–488. [Google Scholar]
- Redmond, A.C.; Crane, Y.Z.; Menz, H.B. Normative values for the Foot Posture Index. J. Foot Ankle Res. 2008, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Pita-Fernandez, S.; Gonzalez-Martin, C.; Aalonso-Tajes, F.; Seoane-Pillado, T.; Pertega-Diaz, S.; Perez-Garcia, S.; Seijo-Bestilleiro, R.; Balboa-Barreiro, V. Flat foot in a random population and its impact on quality of life and functionality. J. Clin. Diagn. Res. 2017, 11, 22–27. [Google Scholar] [CrossRef]
- Bal, A.; Aydog, E.; Aydog, S.T.; Cakci, A. Foot deformities in rheumatoid arthritis and relevance of foot function index. Clin. Rheumatol. 2006, 25, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Göksel Karatepe, A.; GüNaydin, R.; Adibelli, Z.H.; Kaya, T.; DuruöZ, E. Foot deformities in patients with rheumatoid arthritis: The relationship with foot functions. Int. J. Rheum. Dis. 2010, 13, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Villarraga, A.; Bayona, J.; Zuluaga, N.; Mejia, S.; Hincapie, M.E.; Anaya, J.M. The impact of rheumatoid foot on disability in Colombian patients with rheumatoid arthritis. BMC Musculoskelet. Disord. 2009, 10, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Stolt, M.; Suhonen, R.; Leino-Kilpi, H. Foot health in patients with rheumatoid arthritis—A scoping review. Rheumatol. Int. 2017, 37, 1413–1422. [Google Scholar] [CrossRef]
- Nix, S.; Smith, M.; Vicenzino, B. Prevalence of hallux valgus in the general population: A systematic review and meta-analysis. J. Foot Ankle Res. 2010, 3, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valero-Salas, J.; Palomo-Toucedo, I.C.; Munuera-Martínez, P.V. El Hallux Abductus Valgus. In El primer Radio: Biomecánica y Ortopodología; Munuera-Martínez, P.V., Ed.; Exa Editores: Santander, UK, 2012; pp. 155–187. [Google Scholar]
- De Andrade, A.P.; Inoue, E.N.; Nisihara, R.; Skare, T.L. Foot function in rheumatoid arthritis patients: A cross-sectional study. Clin. Rheumatol. 2018, 37, 3427–3430. [Google Scholar] [CrossRef]
- Carter, K.; Lahiri, M.; Cheung, P.P.; Santosa, A.; Rome, K. Prevalence of foot problems in people with inflammatory arthritis in Singapore. J. Foot Ankle Res. 2016, 9, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Morpeth, T.; Brenton-Rule, A.; Carroll, M.; Frecklington, M.; Rome, K. Fear of falling and foot pain, impairment and disability in rheumatoid arthritis: A case-control study. Clin. Rheumatol. 2016, 35, 887–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, S.; Carroll, M.; Brenton-Rule, A.; Keys, M.; Bell, L.; Dalbeth, N.; Rome, K. Region-specific foot pain and plantar pressure in people with rheumatoid arthritis: A cross-sectional study. Clin. Biomech. 2018, 55, 14–17. [Google Scholar] [CrossRef]
- Singh, D.; Biz, C.; Corradin, M.; Favero, L. Comparison of dorsal and dorsomedial displacement in evaluation of first ray hypermobility in feet with and without hallux valgus. Foot Ankle Surg. 2016, 22, 120–124. [Google Scholar] [CrossRef]
- Van Riel, P.L.C.M.; Renskers, L. The Disease Activity Score (DAS) and the Disease Activity Score using 28 joint counts (DAS28) in the management of rheumatoid arthritis. Clin. Exp. Rheumatol. 2016, 34, 40–44. [Google Scholar]
- Fuhrmann, R.A.; Rippel, W.; Traub, A. Konservative Therapie des Hallux-valgus-Syndroms: Was kann man mit Schienen und Einlagen erreichen? Orthopade 2017, 46, 395–401. [Google Scholar] [CrossRef]
- Stukenborg-Colsman, C. Hallux valgus: Konservative und operative Therapie. Orthopade 2017, 46, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zirngibl, B.; Grifka, J.; Baier, C.; Götz, J. Hallux valgus: Ätiologie, diagnostische und therapeutische Prinzipien. Orthopade 2017, 46, 283–296. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Foot Characteristics | n (%) | Mean ± Standard Deviation |
|---|---|---|
| Hallux valgus (right foot) | Mild = 17 (29.8) Moderate = 11 (19.3) Severe = 6 (10.5) TOTAL = 34 (59.6) | |
| Hallux valgus (left foot) | Mild = 17 (29.8) Moderate = 9 (15.8) Severe = 5 (8.8) TOTAL = 31 (54.4) | |
| Toe deformities | 48 (85.7) | |
| Arch Index (right foot) | Normal = 12 (21.1) Low arched = 39 (68.4) High arched = 6 (10.5) | 0.27 ± 0.00 |
| Arch Index (left foot) | Normal = 12 (21.1) Low arched = 38 (66.7) High arched = 7 (12.3) | 0.27 ± 0.00 |
| FPI (right foot) | Normal = 21 (36.8) Pronated = 21 (36.8) Highly pronated = 9 (15.8) Supinated = 3 (5.3) Highly supinated = 3 (5.3) | 5.21 ± 0.56 |
| FPI (left foot) | Normal = 21 (36.8) Pronated = 22 (38.6) Highly pronated = 9 (15.8) Supinated = 3 (5.3) Highly supinated = 2 (3.5) | 5.28 ± 0.54 |
| Variables | Mean ± Standard Deviation |
|---|---|
| Visual Analogue Scale | 6.17 ± 0.33 |
| Days with foot pain | 5.64 ± 0.31 |
| FFI (pain) | 65.80 ± 2.52 |
| FFI (disability) | 56.07 ± 3.68 |
| FFI (activity limitation) | 16.26 ± 2.69 |
| FFI total | 51.26 ± 2.57 |
| MFPDI (function) | 12.10 ± 0.64 |
| MFPDI (personal appearance) | 1.22 ± 0.19 |
| MFPDI (pain) | 6.50 ± 0.33 |
| MFPDI (work) | 2.38 ± 0.21 |
| MFPDI total | 22.19 ± 1.10 |
| Variables | ≤10 Years n = 27 (47.4%) | >10 Years n = 30 (52.6%) | p |
|---|---|---|---|
| Visual analogue scale | 6.6 ± 2.0 | 6.6 ± 2.8 | 0.659 |
| Days with foot pain | 5.5 ± 2.3 | 5.8 ± 2.1 | 0.619 |
| Toe deformities | 20 (41.7%) | 28 (58.3%) | 0.085 * |
| Arch index (right foot) | 0.25 ± 0.03 | 0.30 ± 0.05 | 0.056 * |
| Arch index (left foot) | 0.27 ± 0.05 | 0.27 ± 0.05 | 0.173 |
| FPI (right foot) | 6.9 ± 5.4 | 7.6 ± 3.9 | 0.191 |
| FPI (left foot) | 7.1 ± 5.1 | 7.2 ± 3.9 | 0.260 |
| FFI (Pain) | 65.5 ± 18.2 | 66.1 ± 20.1 | 0.898 |
| FFI (Disability) | 54.9 ± 26.2 | 57.1 ± 29.7 | 0.763 |
| FFI (Functional limitation) | 14.3 ± 18.1 | 23.7 ± 21.4 | 0.079 * |
| FFI (Total) | 49.6 ± 18.6 | 52.8 ± 20.3 | 0.544 |
| MFPDI (function) | 11.4 ± 4.9) | 12.7 ± 4.8 | 0.310 |
| MFPDI (personal appearance) | 1.1 ± 1.5 | 1.4 ± 1.5 | 0.459 |
| MFPDI (pain) | 6.7 ± 2.8 | 6.3 ± 2.3 | 0.588 |
| MFPDI (work) | 2.3 ± 4.7 | 2.5 ± 1.6 | 0.583 |
| MFPDI (Total) | 21.8 ± 9.0 | 22.5 ± 7.8 | 0.748 |
| Outcomes | Years with RA | Multivariate | |||||
|---|---|---|---|---|---|---|---|
| ≤10 Years | >10 Years | p | OR | p | |||
| n = 27 (47.4%) | n = 30 (52.6%) | ||||||
| n | % | n | % | ||||
| Toe deformities | 21 | 77.8 | 28 | 93.3 | 0.095 * | ||
| Manchester Scale for hallux valgus (right foot) | 0.182 | ||||||
| A | 14 | 51.9 | 8 | 27.6 | |||
| B | 7 | 25.9 | 10 | 34.5 | |||
| C | 5 | 18.5 | 6 | 20.7 | |||
| D | 1 | 3.7 | 5 | 17.2 | |||
| Manchester Scale for hallux valgus (left foot) | 0.344 | ||||||
| A | 15 | 55.6 | 11 | 36.7 | |||
| B | 8 | 29.6 | 9 | 30 | |||
| C | 3 | 11.1 | 6 | 20 | |||
| D | 1 | 3.7 | 4 | 13.3 | |||
| Hallux valgus (yes or not) # | 13 | 48.1 | 21 | 72.4 | 0.056 * | 4.9 (1.2–19.7) | 0.024 ** |
| Arch index (right foot) | 0.140 * | ||||||
| Low arch | 15 | 55.6 | 24 | 80 | 0.095 *** | ||
| High arch | 4 | 14.8 | 2 | 6.7 | 0.29 | ||
| Normal arch | 8 | 29.6 | 4 | 13.3 | Ref. | ||
| Arch index (left foot) | 0.816 | ||||||
| Low arch | 17 | 63 | 21 | 70 | |||
| High arch | 4 | 14.8 | 3 | 10 | |||
| Normal arch | 6 | 22.2 | 6 | 20 | |||
| FPI right foot | 0.088 * | ||||||
| Normal | 7 | 25.9 | 14 | 46.7 | |||
| Pronated | 15 | 55.6 | 15 | 50 | |||
| Supinated | 5 | 18.5 | 1 | 3.3 | |||
| FPI left foot | 0.134 * | ||||||
| Normal | 7 | 25.9 | 14 | 46.7 | Ref. | ||
| Pronated | 16 | 59.3 | 15 | 50 | 0.056 *** | ||
| Supinated | 4 | 14.8 | 1 | 3.3 | 0.066 *** | ||
| Mean ± SD; Median (IQR) | Mean ± SD; Median (IQR) | ||||||
| Visual analogue scale | 6.0 ± 2.5; 6 (5–7) | 6.3 ± 2.6; 6.5 (4.8–8.3) | 0.699 | ||||
| Days with foot pain | 5.5 ± 2.3; 7 (3.8–7) | 5.8 ± 2.1; 7 (4.8–7) | 0.594 | ||||
| FFI (Pain) | 65.5 ± 18.2; 66.7 (52.2–84.3) | 66.1 ± 20.1; 71.3 (54–81.2) | 0.565 | ||||
| FFI (Disability) | 54.9 ± 26.2; 55.6 (28.9–80) | 57.1 ± 29.7; 66.7 (32.5–80) | 0.643 | ||||
| FFI (Functional limitation) | 14.3 ± 18.1; 12 (0–16) | 23.7 ± 21.4; 18.8 (9.4–34.5) | 0.050 * | ||||
| FFI (Total) | 49.6 ± 18.6; 52.2 (35.7–66.2) | 52.8 ± 20.3; 57.7 (39.1–64.6) | 0.31 | ||||
| MFPDI (function) | 11.4 ± 4.9; 12 (8–15) | 12.7 ± 4.8; 13.5 (9–17) | 0.31 | ||||
| MFPDI (personal appearance) | 1.1 ± 1.5; 0 (0–2) | 1.4 ± 1.5; 1 (0–2.3) | 0.378 | ||||
| MFPDI (pain) | 6.7 ± 2.8; 7 (6–9) | 6.3 ± 2.3; 6 (4–8) | 0.472 | ||||
| MFPDI (work) | 2.3 ± 4.7; 2 (1–4) | 2.5 ± 1.6; 2.5 (1.5–4) | 0.582 | ||||
| MFPDI (Total) | 21.8 ± 9.0; 23 (13–30) | 22.5 ± 7.8; 22 (18.5–30) | 0.923 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reina-Bueno, M.; Munuera-Martínez, P.V.; Pérez-García, S.; Vázquez-Bautista, M.d.C.; Domínguez-Maldonado, G.; Palomo-Toucedo, I.C. Foot Pain and Morphofunctional Foot Disorders in Patients with Rheumatoid Arthritis: A Multicenter Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5042. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095042
Reina-Bueno M, Munuera-Martínez PV, Pérez-García S, Vázquez-Bautista MdC, Domínguez-Maldonado G, Palomo-Toucedo IC. Foot Pain and Morphofunctional Foot Disorders in Patients with Rheumatoid Arthritis: A Multicenter Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(9):5042. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095042
Chicago/Turabian StyleReina-Bueno, María, Pedro V. Munuera-Martínez, Sergio Pérez-García, María del Carmen Vázquez-Bautista, Gabriel Domínguez-Maldonado, and Inmaculada C. Palomo-Toucedo. 2021. "Foot Pain and Morphofunctional Foot Disorders in Patients with Rheumatoid Arthritis: A Multicenter Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 9: 5042. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095042