
Effectiveness of App-Based Intervention to Improve Health Status of Sedentary Middle-Aged Males and Females

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
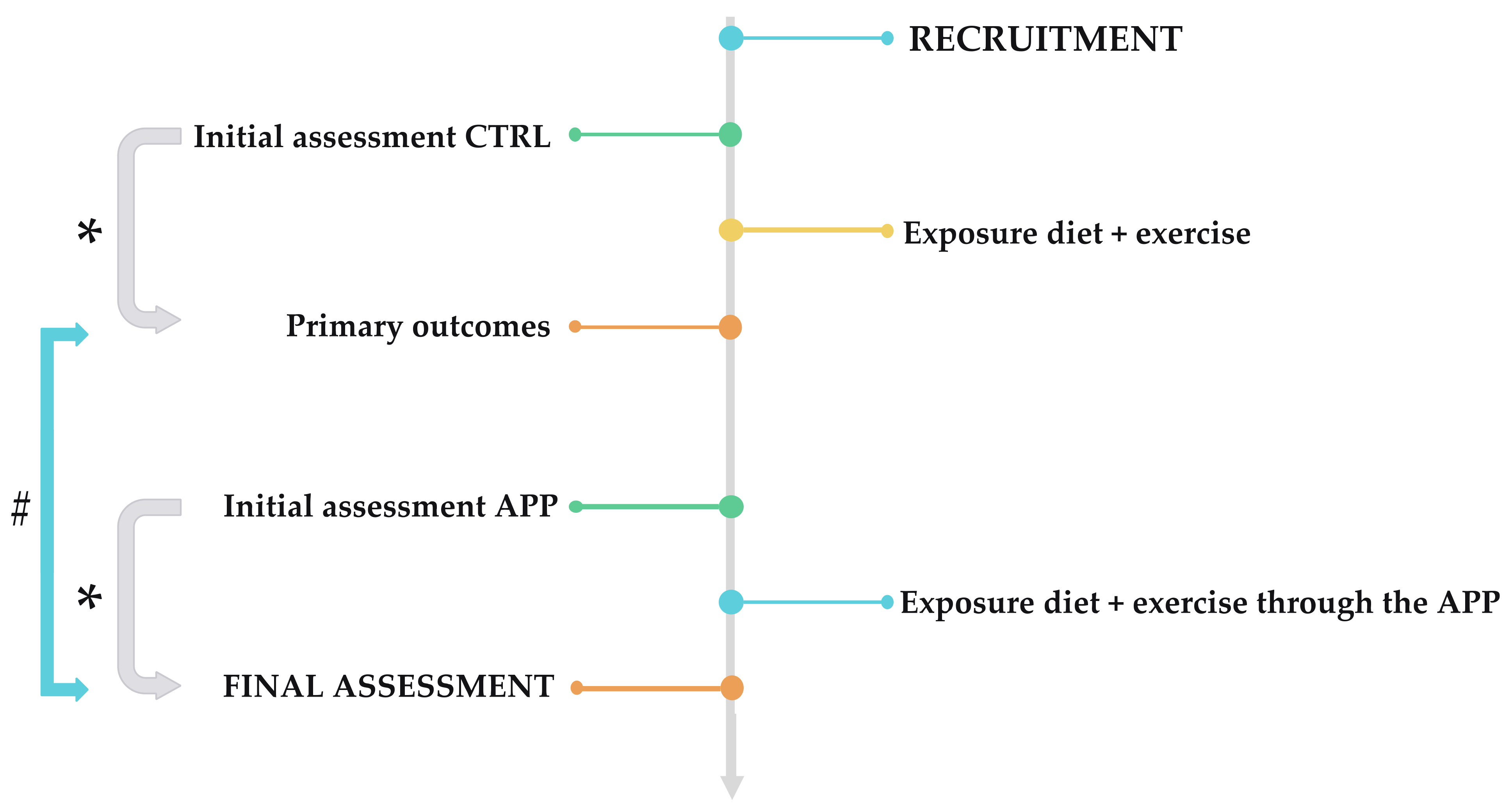
2.1. Study Design
2.2. Participants
2.3. Declarations: Ethical Approval, Consent to Participate and Consent to Publish
2.4. Intervention
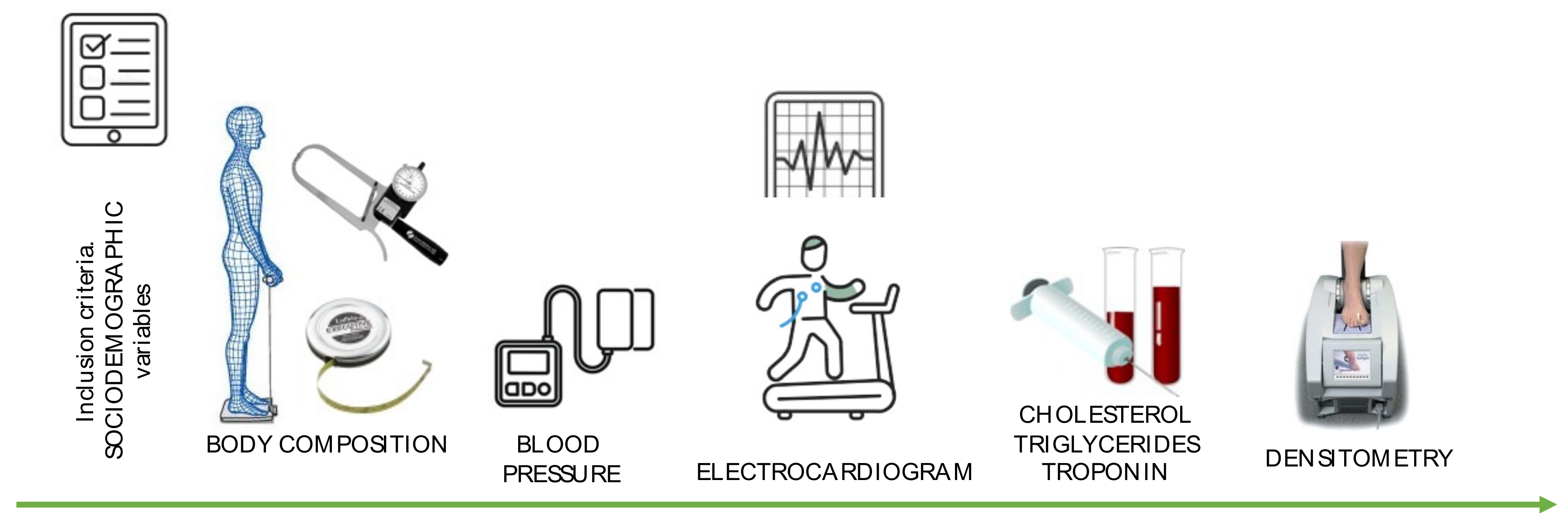
2.5. Study Variables
2.5.1. Body Composition
2.5.2. Cardiovascular Parameters
2.5.3. Bone Mineral Density
2.6. Statistical Analysis
3. Results
3.1. Socio-Demographic Data
3.2. Body Composition
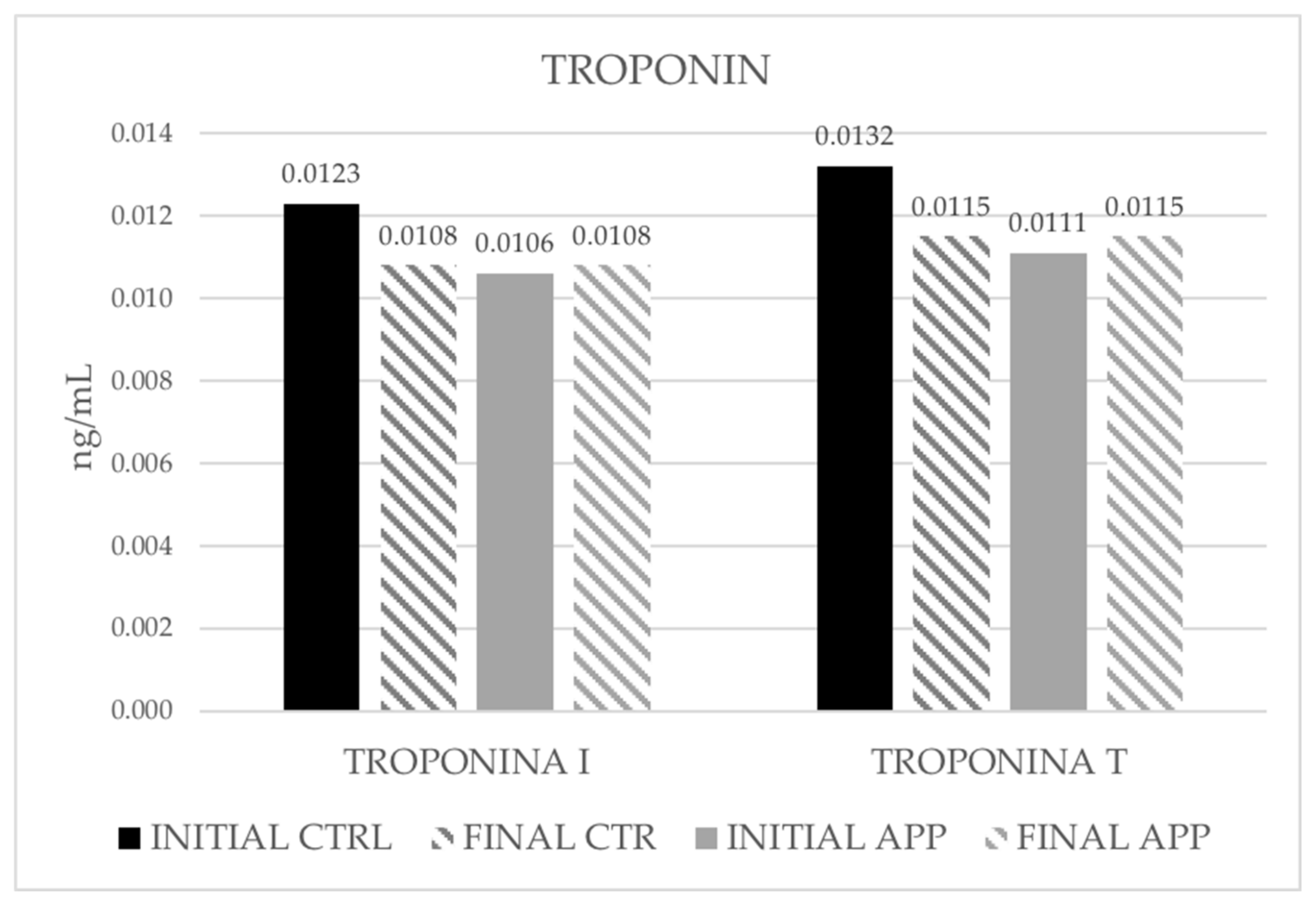
3.3. Cardiovascular Parameters
3.4. Bone Mineral Density
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 21 March 2022).
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandão, I.; Martins, M.J.; Monteiro, R. Metabolically Healthy Obesity-Heterogeneity in Definitions and Unconventional Factors. Metabolites 2020, 10, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcalde-Rabanal, J.E.; Orozco-Núñez, E.; Espinosa-Henao, O.E.; Arredondo-López, A.; Alcayde-Barranco, L. The complex scenario of obesity, diabetes and hypertension in the area of influence of primary healthcare facilities in Mexico. PLoS ONE 2018, 13, e0187028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutcher, Y.N.; Boutcher, S.H. Exercise intensity and hypertension: What’s new? J. Hum. Hypertens. 2017, 31, 157–164. [Google Scholar] [CrossRef]
- Heiston, E.M.; Eichner, N.Z.M.; Gilbertson, N.M.; Malin, S.K. Exercise improves adiposopathy, insulin sensitivity and metabolic syndrome severity independent of intensity. Exp. Physiol. 2020, 105, 632–640. [Google Scholar] [CrossRef]
- Di Daniele, N.; Noce, A.; Vidiri, M.F.; Moriconi, E.; Marrone, G.; Annicchiarico-Petruzzelli, M.; D’Urso, G.; Tesauro, M.; Rovella, V.; De Lorenzo, A.D. Impact of Mediterranean diet on metabolic syndrome, cancer and longevity. Oncotarget 2017, 8, 8947. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Dealmeida, D.; Parmanto, B. Applying a User-Centered Approach to Building a Mobile Personal Health Record App: Development and Usability Study. JMIR Mhealth Uhealth 2019, 7, e13194. [Google Scholar] [CrossRef]
- Morrison, L.G.; Hargood, C.; Lin, S.X.; Dennison, L.; Joseph, J.; Hughes, S.; Michaelides, D.T.; Johnston, D.; Johnston, M.; Michie, S.; et al. Understanding usage of a hybrid website and smartphone app for weight management: A mixed-methods study. J. Med. Internet Res. 2014, 16, e3579. [Google Scholar] [CrossRef]
- Castensøe-Seidenfaden, P.; Husted, G.R.; Teilmann, G.; Hommel, E.; Olsen, B.S.; Kensing, F. Designing a Self-Management App for Young People With Type 1 Diabetes: Methodological Challenges, Experiences, and Recommendations. JMIR Mhealth Uhealth 2017, 5, e8137. [Google Scholar] [CrossRef] [Green Version]
- Stork, M.J.; Bell, E.G.; Jung, M.E. Examining the Impact of a Mobile Health App on Functional Movement and Physical Fitness: Pilot Pragmatic Randomized Controlled Trial. JMIR Mhealth Uhealth 2021, 9, e24076. [Google Scholar] [CrossRef]
- Byambasuren, O.; Beller, E.; Hoffmann, T.; Glasziou, P. mHealth App Prescription in Australian General Practice: Pre-Post Study. JMIR Mhealth Uhealth 2020, 8, e16497. [Google Scholar] [CrossRef] [PubMed]
- Payne, H.E.; Lister, C.; West, J.H.; Bernhardt, J.M. Behavioral functionality of mobile apps in health interventions: A systematic review of the literature. JMIR Mhealth Uhealth 2015, 3, e3335. [Google Scholar] [CrossRef] [PubMed]
- Saliasi, I.; Martinon, P.; Darlington, E.; Smentek, C.; Tardivo, D.; Bourgeois, D.; Dussart, C.; Carrouel, F.; Fraticelli, L. Promoting Health via mHealth Applications Using a French Version of the Mobile App Rating Scale: Adaptation and Validation Study. JMIR Mhealth Uhealth 2021, 9, e30480. [Google Scholar] [CrossRef] [PubMed]
- Woods, L.S.; Duff, J.; Roehrer, E.; Walker, K.; Cummings, E. Patients’ Experiences of Using a Consumer mHealth App for Self-Management of Heart Failure: Mixed-Methods Study. JMIR Hum. Factors 2019, 6, e13009. [Google Scholar] [CrossRef]
- Serlachius, A.; Schache, K.; Kieser, A.; Arroll, B.; Petrie, K.; Dalbeth, N. Association Between User Engagement of a Mobile Health App for Gout and Improvements in Self-Care Behaviors: Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e15021. [Google Scholar] [CrossRef]
- Jeffrey, B.; Bagala, M.; Creighton, A.; Leavey, T.; Nicholls, S.; Wood, C.; Longman, J.; Barker, J.; Pit, S. Mobile phone applications and their use in the self-management of Type 2 Diabetes Mellitus: A qualitative study among app users and non-app users. Diabetol. Metab. Syndr. 2019, 11, 1–17. [Google Scholar] [CrossRef]
- Ernsting, C.; Stühmann, L.M.; Dombrowski, S.U.; Voigt-Antons, J.N.; Kuhlmey, A.; Gellert, P. Associations of Health App Use and Perceived Effectiveness in People With Cardiovascular Diseases and Diabetes: Population-Based Survey. JMIR Mhealth Uhealth 2019, 7, e12179. [Google Scholar] [CrossRef]
- Brindal, E.; Hendrie, G.A.; Freyne, J.; Noakes, M. A Mobile Phone App Designed to Support Weight Loss Maintenance and Well-Being (MotiMate): Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e12882. [Google Scholar] [CrossRef] [Green Version]
- Joshi, A.; Amadi, C.; Schumer, H.; Galitzdorfer, L.; Gaba, A. A human centered approach to design a diet app for patients with metabolic syndrome. Mhealth 2019, 5, 43. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Román-Viñas, B.; Sanchez-Villegas, A.; Guasch-Ferré, M.; Corella, D.; La Vecchia, C. Benefits of the Mediterranean diet: Epidemiological and molecular aspects. Mol. Aspects Med. 2019, 67, 1–55. [Google Scholar]
- Oppliger, R.A.; Case, H.S.; Horswill, C.A.; Landry, G.L.; Shelter, A.C. American College of Sports Medicine position stand. Weight loss in wrestlers. Med. Sci. Sports Exerc. 1996, 28, ix–xii. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, R.A.; Blackmon, J.R.; Jones, J.W.; Strait, G. Exercising testing in adult normal subjects and cardiac patients. Pediatrics 1963, 32, 742–756. [Google Scholar] [CrossRef]
- Loh, J.; Amanullah, M.R.; See, C.K.; Tang, H.C.; Gunasegaran, K.; Hamid, N.; Lau, J.; Lee, C.Y.; Ewe, S.H.; Ding, Z.P.; et al. Predicting premature termination of exercise during Bruce protocol stress echocardiography. Echocardiography 2021, 38, 1612–1617. [Google Scholar] [CrossRef] [PubMed]
- Lara, B.; Salinero, J.J.; Gutiérrez, J.; Areces, F.; Abián-Vicén, J.; Ruiz-Vicente, D.; Gallo-Salazar, C.; Jiménez, F.; Del Coso, J. Influence of endurance running on calcaneal bone stiffness in male and female runners. Eur. J. Appl. Physiol. 2016, 116, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Marín, F.; González-Macías, J.; Díez-Pérez, A.; Palma, S.; Delgado-Rodríguez, M. Relationship between bone quantitative ultrasound and fractures: A meta-analysis. J. Bone Miner. Res. 2006, 21, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Caballero Uribe, C.V. Evaluación de la osteoporosis mediante el ultrasonido cuantitativo de calcáneo. Rev. Esp. Enferm. Metab. Oseas 2001, 10, 65–69. [Google Scholar]
- Huh, U.; Tak, Y.J.; Song, S.; Chung, S.W.; Sung, S.M.; Lee, C.W.; Bae, M.; Ahn, H.Y. Feedback on Physical Activity Through a Wearable Device Connected to a Mobile Phone App in Patients With Metabolic Syndrome: Pilot Study. JMIR Mhealth Uhealth 2019, 7, e13381. [Google Scholar] [CrossRef]
- Debon, R.; Bellei, E.A.; Biduski, D.; Volpi, S.S.; Alves, A.L.S.; Portella, M.R.; De Marchi, A.C.B. Effects of using a mobile health application on the health conditions of patients with arterial hypertension: A pilot trial in the context of Brazil’s Family Health Strategy. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Higgins, J.P. Smartphone Applications for Patients’ Health and Fitness. Am. J. Med. 2016, 129, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Milne-Ives, M.; LamMEng, C.; de Cock, C.; van Velthoven, M.H.; Ma, E.M. Mobile Apps for Health Behavior Change in Physical Activity, Diet, Drug and Alcohol Use, and Mental Health: Systematic Review. JMIR Mhealth Uhealth 2020, 8, e17046. [Google Scholar] [CrossRef]
- Han, M.; Rhee, S.Y. Effect of Adherence to Smartphone App Use on the Long-term Effectiveness of Weight Loss in Developing and OECD Countries: Retrospective Cohort Study. JMIR Mhealth Uhealth 2021, 9, e13496. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Lee, E. Effectiveness of Mobile Health Application Use to Improve Health Behavior Changes: A Systematic Review of Randomized Controlled Trials. Healthc. Inform. Res. 2018, 24, 207–226. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
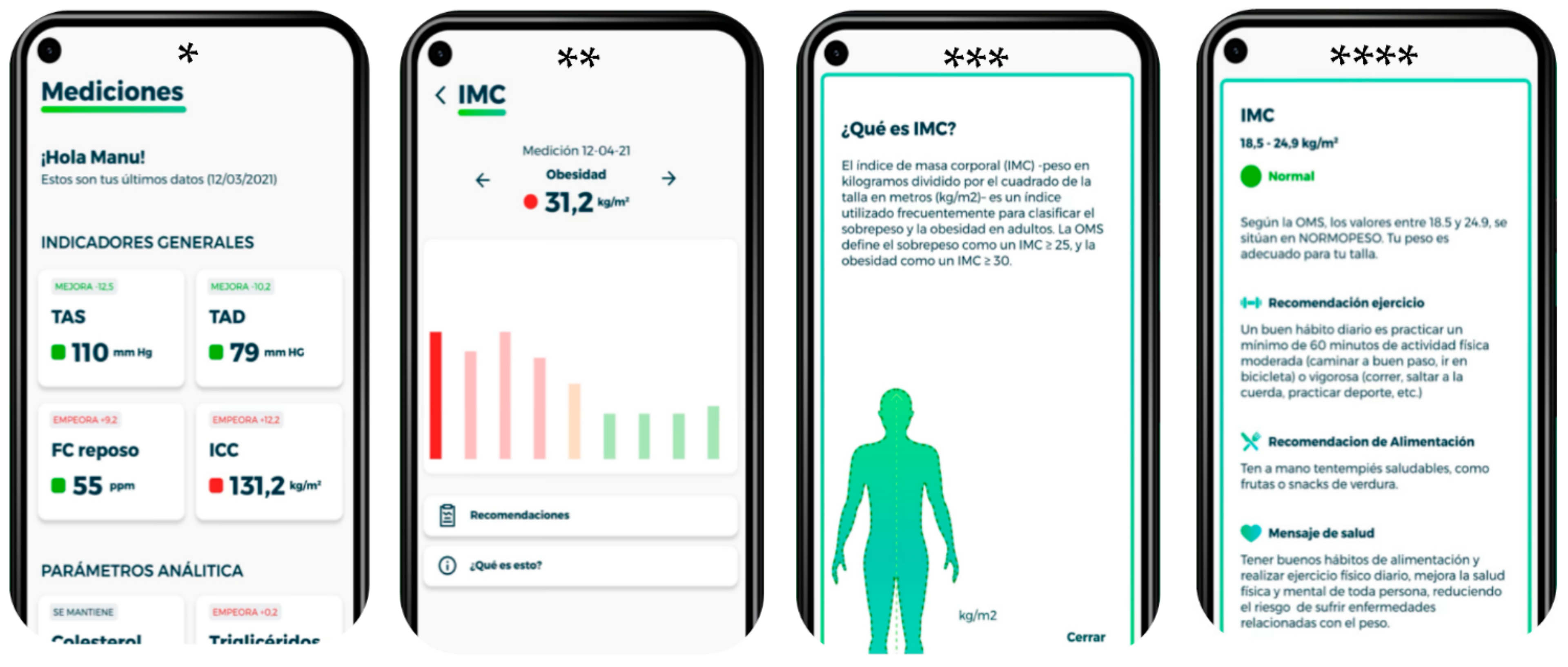
| * | Measurements. General indicators. The image shows the variables: systolic blood pressure, diastolic blood pressure, resting heart rate and waist/hip ratio. |
| ** | Once you click on one of the variables, the record of the different measurements appears (bar graph). Within the screen there is a section of recommendations and what is this? |
| *** | What is BMI? Body mass index (BMI)—weight in kilograms divided by the square of height in meters (kg/m2)—is an index frequently used to classify overweight and obesity in adults. WHO defines overweight as a BMI > 25 and obesity as a BMI > 30. |
| **** | BMI According to WHO, values between 18.5 and 24.9 are NORMAL WEIGHT. Your weight is appropriate for your size. Exercise recommendation: A good daily habit is to engage in a minimum of 60 min of moderate (brisk walking, cycling) or vigorous (running, jumping rope, sports, etc.) physical activity. Food recommendation: Have healthy snacks on hand, such as fruits or vegetable snacks. Health message: good eating habits and daily physical exercise help to improve the physical and mental health of everyone, reducing the risk of weight-related diseases. |
| Variable | Result Message | Exercise Message | Eating Message | Health Message |
|---|---|---|---|---|
| BMI (kg/m2) ≥ 25.0 | Overweight is caused by an abnormal or excessive accumulation of fat that can be detrimental to health. | Exercise helps regulate metabolism, causing an increase in metabolism by using energy reserves (glycogen and fat) to run the muscles. | A proper diet would improve your results, this is composed of a varied diet, with plenty of fruits and vegetables, avoiding processed products and alcohol. | Maintaining a healthy weight does not mean dieting. It is a lifestyle. There are simple steps you can take every day to keep your weight at healthy levels and reduce your risk of weight-related diseases and health problems. |
| Cholesterol ≥ 240 mg/dL | At this cholesterol level, the probability of suffering heart disease is twice as high as with values < 200 mg/dL. | Regular physical activity can help you control your weight and thus lower your cholesterol. | Eating foods rich in Omega 3 helps regulate total blood cholesterol. Among these foods are nuts, avocados, and oily fish. | High cholesterol affects the heart and blood vessels and increases the risk of developing cardiovascular disease. |
| Hight fat mass (%) | Your percentage of fat mass is HIGH. This increases the risk of heart disease and stroke. | Daily physical exercise has a beneficial effect on body composition. It helps to reduce skin folds, as well as the body fat index. | If you take in more calories than you burn, the excess calories are stored in your body in the form of fat cells. When the stored fat is not subsequently converted into energy, excess body fat is produced. | Excess body fat increases the risk of depression. Scientists at the University of Aarhus in Denmark conclude that excess body fat increases the chance of depression by up to 15%. |
| SBP 120–130 mmHg | Your systolic blood pressure is at HIGH values. Control these values regularly, having high blood pressure can have serious repercussions on your health. | Daily physical exercise (walking, running, cycling, swimming, etc.) for 30–60 min, 3 to 5 days a week, will help regulate your blood pressure. | Refined carbohydrates, especially sugar, can increase blood pressure. Some studies have shown that low-carbohydrate diets may help lower your levels. | There is conflicting research on smoking and high blood pressure, but what is clear is that both increase the risk of heart disease. |
| Men | Women | |||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Age | 35.38 | 7.25 | 45.00 | 8.68 |
| Height | 176.05 | 7.62 | 162.77 | 5.42 |
| CTRL | app | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial | Final | Initial | Final | Effect Time | Effect Time × Period | |||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | F | p | η2p | F | p | η2p | |
| Weight (kg) | 83.00 | 16.4 | 81.9 | 16.2 | 78.5 | 15.5 | 72.6 | 15.0 | 206.7 | < 0.001 | 0.752 | 93.4 | < 0.001 | 0.579 |
| BMI (kg/m2) | 29.00 | 4.88 | 28.6 | 4.72 | 27.5 | 4.58 | 25.4 | 4.44 | 202.9 | <0 .001 | 0.749 | 92.7 | < 0.001 | 0.577 |
| Fat mass (%) | 30.2 | 10.3 | 29.5 | 10.8 | 28.1 | 10.4 | 26.1 | 9.73 | 55.5 | <0 .001 | 0.450 | 11.4 | 0.001 | 0.143 |
| Water (%) | 50.6 | 7.05 | 51.4 | 7.57 | 53.7 | 8.07 | 57.6 | 8.84 | 120.6 | <0 .001 | 0.639 | 55.5 | < 0.001 | 0.449 |
| Visceral fat | 8.14 | 3.88 | 7.81 | 3.64 | 7.46 | 3.52 | 7.08 | 3.42 | 26.494 | < 0.001 | 0.280 | 0.108 | 0.743 | 0.002 |
| Hip (cm) | 90.5 | 11.4 | 90.2 | 10.9 | 86.1 | 11.1 | 79.9 | 10.3 | 50.5 | < 0.001 | 0.426 | 40.3 | < 0.001 | 0.372 |
| Waist (cm) | 106.0 | 11.3 | 105.0 | 9.98 | 103.0 | 9.83 | 96.2 | 10.1 | 54.4 | < 0.001 | 0.444 | 37.7 | < 0.001 | 0.357 |
| WHI | 0.858 | 0.0974 | 0.858 | 0.0945 | 0.841 | 0.0918 | 0.833 | 0.0923 | 1.73 | 0.193 | 0.025 | 2.14 | 0.148 | 0.031 |
| CTRL | app | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial | Final | Initial | Final | Effect Time | Effect Time x Period | |||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | F | p | η2p | F | p | η2p | |
| CHO (mg/dL) | 188.0 | 45.4 | 175.0 | 38.0 | 167.0 | 37.6 | 155.0 | 34.9 | 9.1 | 0.003 | 0.119 | 0.9 | 0.339 | 0.013 |
| TG (mg/dL) | 104.0 | 127.0 | 100.0 | 123.0 | 96.8 | 123.0 | 89.7 | 113.0 | 356.4 | <0 .001 | 0.344 | 0.1 | 0.799 | 0.001 |
| SBP (mmHg) | 130.0 | 19.8 | 130.0 | 17.1 | 124.0 | 17.2 | 115.0 | 15.7 | 27.1 | < 0.001 | 0.285 | 28.9 | < 0.001 | 0.298 |
| DBP (mmHg) | 83.6 | 13.2 | 83.6 | 12.6 | 79.8 | 12.6 | 74.0 | 11.5 | 17.0 | < 0.001 | 0.200 | 16.4 | <0 .001 | 0.194 |
| HR at rest | 69.6 | 14.7 | 68.7 | 12.4 | 66.5 | 12.4 | 60.8 | 11.1 | 17.3 | < 0.001 | 0.203 | 9.2 | 0.003 | 0.120 |
| HR max | 159.00 | 16.9 | 161.0 | 15.0 | 156.0 | 14.8 | 142.0 | 13.5 | 26.1 | < 0.001 | 0.278 | 45.4 | < 0.001 | 0.401 |
| CTRL | app | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial | Final | Initial | Final | Effect Time | Effect Time x Period | |||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | F | p | η2p | F | p | η2p | |
| BUA (dB/MHz) | 133.0 | 11.4 | 134.0 | 12.1 | 134.0 | 12.1 | 135.0 | 12.2 | 14.291 | <0 .001 | 0.174 | 0.335 | 0.565 | 0.005 |
| SOS (m/s) | 1647.0 | 35.9 | 1658.0 | 38.2 | 1665.0 | 38.3 | 1673.0 | 38.7 | 9.033 | 0.004 | 0.117 | 0.230 | 0.633 | 0.003 |
| STIFFNESS (A.U) | 432.0 | 15.5 | 436.0 | 16.4 | 439.0 | 16.5 | 441.0 | 16.7 | 0.416 | 0.521 | 0.006 | 2.314 | 0.133 | 0.033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Olcina, M.; Cuestas-Calero, B.J.; Miralles-Amorós, L.; Vicente-Martínez, M.; Sánchez-Sánchez, J. Effectiveness of App-Based Intervention to Improve Health Status of Sedentary Middle-Aged Males and Females. Int. J. Environ. Res. Public Health 2022, 19, 5857. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19105857
Martínez-Olcina M, Cuestas-Calero BJ, Miralles-Amorós L, Vicente-Martínez M, Sánchez-Sánchez J. Effectiveness of App-Based Intervention to Improve Health Status of Sedentary Middle-Aged Males and Females. International Journal of Environmental Research and Public Health. 2022; 19(10):5857. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19105857
Chicago/Turabian StyleMartínez-Olcina, María, Bernardo José Cuestas-Calero, Laura Miralles-Amorós, Manuel Vicente-Martínez, and Javier Sánchez-Sánchez. 2022. "Effectiveness of App-Based Intervention to Improve Health Status of Sedentary Middle-Aged Males and Females" International Journal of Environmental Research and Public Health 19, no. 10: 5857. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19105857