
Air Pollution Exposure and the Relative Risk of Sudden Sensorineural Hearing Loss in Taipei

 , , , and
, , , and 
Abstract
:1. Introduction
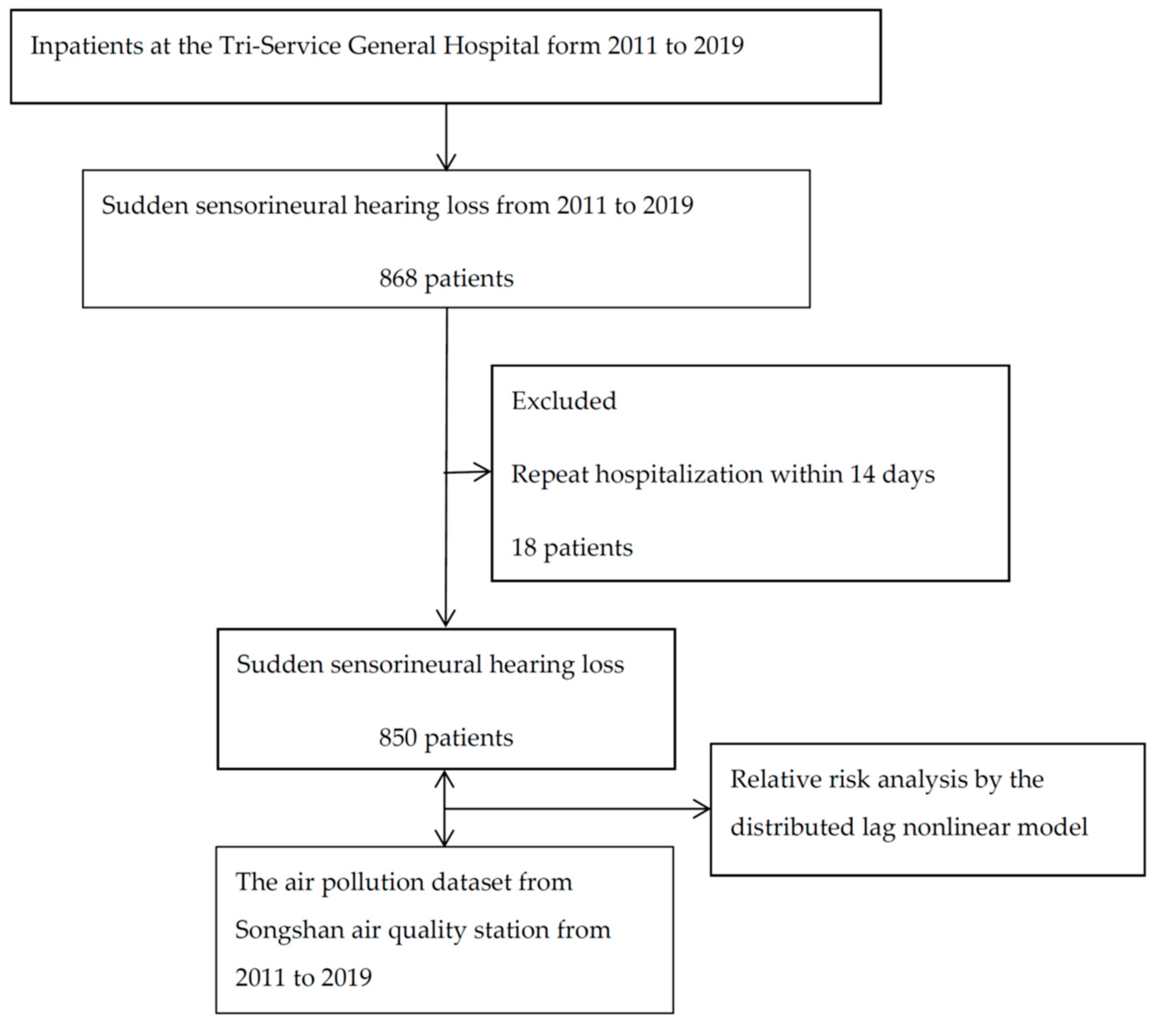
2. Materials and Methods
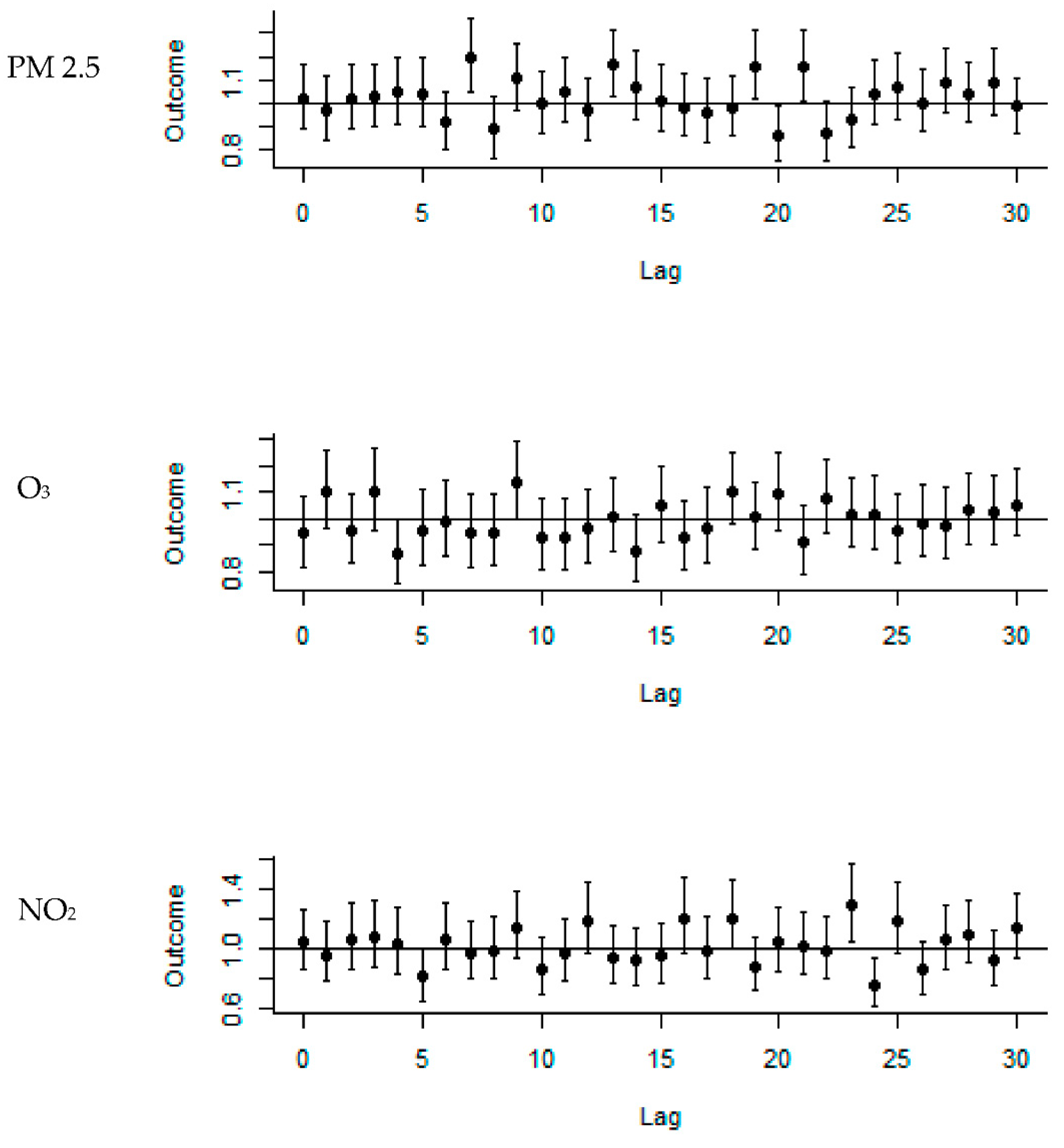
3. Results
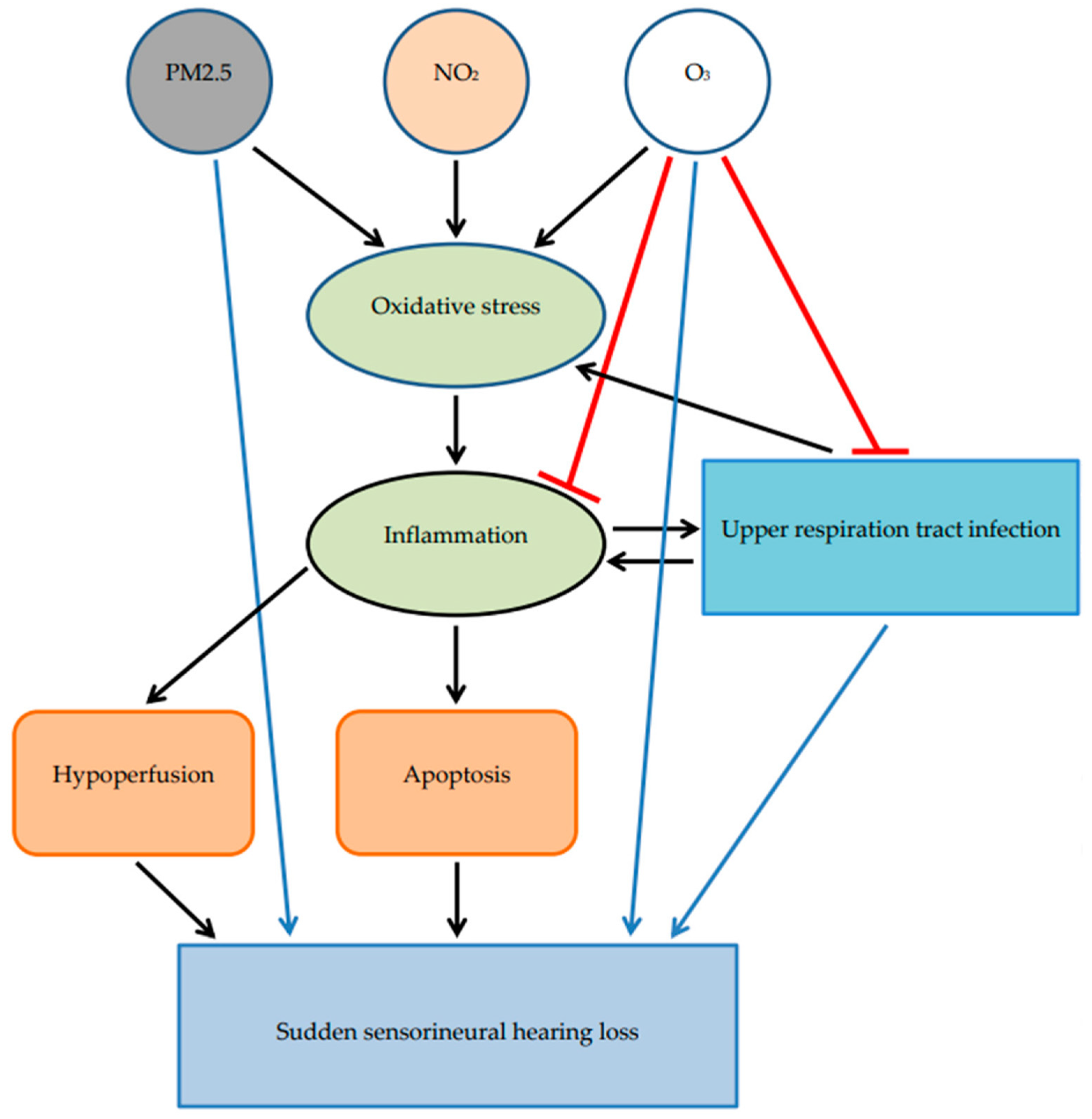
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, S.H.; Kim, S.-J.; Im, H.; Kim, T.-H.; Song, J.-J.; Chae, S.-W. A trend in sudden sensorineural hearing loss: Data from a population-based study. Audiol. Neurotol. 2017, 22, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, M.; Heman-Ackah, S.E.; Shaikh, J.A.; Roehm, P.C. Sudden sensorineural hearing loss: A review of diagnosis, treatment, and prognosis. Trends Amplif. 2011, 15, 91–105. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.K.; Lin, J.R.; Atashband, S.; Irvine, R.A.; Westerberg, B.D. Systematic review of the evidence for the etiology of adult sudden sensorineural hearing loss. Laryngoscope 2010, 120, 1011–1021. [Google Scholar] [CrossRef] [PubMed]
- Alexander, T.H.; Harris, J.P. Incidence of sudden sensorineural hearing loss. Otol. Neurotol. 2013, 34, 1586–1589. [Google Scholar] [CrossRef]
- Chandrasekhar, S.S.; Tsai Do, B.S.; Schwartz, S.R.; Bontempo, L.J.; Faucett, E.A.; Finestone, S.A.; Hollingsworth, D.B.; Kelley, D.M.; Kmucha, S.T.; Moonis, G. Clinical practice guideline: Sudden hearing loss (update). Otolaryngol. Head Neck Surg. 2019, 161 (Suppl. 1), S1–S45. [Google Scholar] [CrossRef] [Green Version]
- Young, Y.-H. Contemporary review of the causes and differential diagnosis of sudden sensorineural hearing loss. Int. J. Audiol. 2020, 59, 243–253. [Google Scholar] [CrossRef]
- Vidale, S.; Campana, C. Ambient air pollution and cardiovascular diseases: From bench to bedside. Eur. J. Prev. Cardiol. 2018, 25, 818–825. [Google Scholar] [CrossRef]
- Simkovich, S.M.; Goodman, D.; Roa, C.; Crocker, M.E.; Gianella, G.E.; Kirenga, B.J.; Wise, R.A.; Checkley, W. The health and social implications of household air pollution and respiratory diseases. NPJ Prim. Care Respir. Med. 2019, 29, 12. [Google Scholar] [CrossRef]
- Pope, I.I.I.C.A.; Coleman, N.; Pond, Z.A.; Burnett, R.T. Fine particulate air pollution and human mortality: 25+ years of cohort studies. Environ. Res. 2020, 183, 108924. [Google Scholar] [CrossRef]
- Lee, H.M.; Kim, M.S.; Kim, D.J.; Uhm, T.W.; Yi, S.B.; Han, J.H.; Lee, I.W. Effects of meteorological factor and air pollution on sudden sensorineural hearing loss using the health claims data in Busan, Republic of Korea. Am. J. Otolaryngol. 2019, 40, 393–399. [Google Scholar] [CrossRef]
- Tsai, S.C.-S.; Hsu, Y.-C.; Lai, J.-N.; Chou, R.-H.; Fan, H.-C.; Lin, F.C.-F.; Zhang, R.; Lin, C.-L.; Chang, K.-H. Long-term exposure to air pollution and the risk of developing sudden sensorineural hearing loss. J. Transl. Med. 2021, 19, 424. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.G.; Min, C.; Kim, S.Y. Air pollution increases the risk of SSNHL: A nested case-control study using meteorological data and national sample cohort data. Sci. Rep. 2019, 9, 8270. [Google Scholar] [CrossRef] [PubMed]
- Taiwanese Environmental Protection Administration. The Air Pollution Data; Taiwanese Environmental Protection Administration: Taipei, Taiwan, 2020. Available online: https://airtw.epa.gov.tw/CHT/Query/His_Data.aspx (accessed on 1 April 2021).
- Gasparrini, A.; Armstrong, B.; Gasparrini, M.A. Package ‘dlnm’; London, UK, 2021; Available online: https://CRAN.R-project.org/package=dlnm (accessed on 1 April 2021).
- Taipei City Statistical Inquiry System. The Number of Motor Vehicle in Taipei; Taipei, Taiwan. 2021. Available online: https://statdb.dbas.gov.taipei/pxweb2007-tp/dialog/statfile9.asp (accessed on 1 April 2021).
- Lehner, C.; Gehwolf, R.; Tempfer, H.; Krizbai, I.; Hennig, B.; Bauer, H.-C.; Bauer, H. Oxidative stress and blood–brain barrier dysfunction under particular consideration of matrix metalloproteinases. Antioxid. Redox Signal. 2011, 15, 1305–1323. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Gonzalez, S. The role of mitochondrial oxidative stress in hearing loss. Neurol. Disord. 2017, 1, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Capaccio, P.; Pignataro, L.; Gaini, L.M.; Sigismund, P.E.; Novembrino, C.; De Giuseppe, R.; Uva, V.; Tripodi, A.; Bamonti, F. Unbalanced oxidative status in idiopathic sudden sensorineural hearing loss. Eur. Arch. Oto-Rhino-Laryngol. 2012, 269, 449–453. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; Leray, E.; Heydarpour, P.; Torres-Jardón, R.; Reis, J. Air pollution, a rising environmental risk factor for cognition, neuroinflammation and neurodegeneration: The clinical impact on children and beyond. Rev. Neurol. 2016, 172, 69–80. [Google Scholar] [CrossRef]
- Arpornchayanon, W.; Canis, M.; Ihler, F.; Settevendemie, C.; Strieth, S. TNF-α inhibition using etanercept prevents noise-induced hearing loss by improvement of cochlear blood flow in vivo. Int. J. Audiol. 2013, 52, 545–552. [Google Scholar] [CrossRef]
- Sahin, C.; Varim, C.; Karacaer, C. Investigation of neutrophil-to-lymphocyte ratio and red cell distribution width in sudden senseurineural hearing loss. Int. J. Adv. Med. 2019, 6, 424–428. [Google Scholar] [CrossRef]
- Del Zoppo, G.; Ginis, I.; Hallenbeck, J.M.; Iadecola, C.; Wang, X.; Feuerstein, G.Z. Inflammation and stroke: Putative role for cytokines, adhesion molecules and Inos in brain response to ischemia. Brain Pathol. 2000, 10, 95–112. [Google Scholar] [CrossRef]
- Ma, J.-H.; Song, S.-H.; Guo, M.; Zhou, J.; Liu, F.; Peng, L.; Fu, Z.-R. Long-term exposure to PM2.5 lowers influenza virus resistance via down-regulating pulmonary macrophage Kdm6a and mediates histones modification in IL-6 and IFN-β promoter regions. Biochem. Biophys. Res. Commun. 2017, 493, 1122–1128. [Google Scholar] [CrossRef]
- Nenna, R.; Evangelisti, M.; Frassanito, A.; Scagnolari, C.; Pierangeli, A.; Antonelli, G.; Nicolai, A.; Arima, S.; Moretti, C.; Papoff, P. Respiratory syncytial virus bronchiolitis, weather conditions and air pollution in an Italian urban area: An observational study. Environ. Res. 2017, 158, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Su, W.; Wu, X.; Geng, X.; Zhao, X.; Liu, Q.; Liu, T. The short-term effects of air pollutants on influenza-like illness in Jinan, China. BMC Public Health 2019, 19, 1319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boda, E.; Rigamonti, A.E.; Bollati, V. Understanding the effects of air pollution on neurogenesis and gliogenesis in the growing and adult brain. Curr. Opin. Pharmacol. 2020, 50, 61–66. [Google Scholar] [CrossRef]
- Lin, Y.-K.; Chang, C.-K.; Chang, S.-C.; Chen, P.-S.; Lin, C.; Wang, Y.-C. Temperature, nitrogen dioxide, circulating respiratory viruses and acute upper respiratory infections among children in Taipei, Taiwan: A population-based study. Environ. Res. 2013, 120, 109–118. [Google Scholar] [CrossRef]
- Stieb, D.M.; Shutt, R.; Kauri, L.M.; Roth, G.; Szyszkowicz, M.; Dobbin, N.A.; Chen, L.; Rigden, M.; Van Ryswyk, K.; Kulka, R. Cardiorespiratory effects of air pollution in a panel study of winter outdoor physical activity in older adults. J. Occup. Environ. Med. 2018, 60, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Shabani, S. A mechanistic view on the neurotoxic effects of air pollution on central nervous system: Risk for autism and neurodegenerative diseases. Environ. Sci. Pollut. Res. 2021, 28, 6349–6373. [Google Scholar] [CrossRef]
- Van Reeth, K. Cytokines in the pathogenesis of influenza. Vet. Microbiol. 2000, 74, 109–116. [Google Scholar] [CrossRef]
- Cheng, C.-G.; Chien, W.-C.; Lin, H.-C.; Lin, H.-C.; Chung, C.-H.; Cheng, C.-A. Hearing impairment in young and middle-aged septicemia survivors. Medicine 2020, 99, e21050. [Google Scholar] [CrossRef]
- Shao, I.Y.; Elkind, M.S.; Boehme, A.K. Risk factors for stroke in patients with sepsis and bloodstream infections. Stroke 2019, 50, 1046–1051. [Google Scholar] [CrossRef]
- Chen, X.; Fu, Y.-Y.; Zhang, T.-Y. Role of viral infection in sudden hearing loss. J. Int. Med. Res. 2019, 47, 2865–2872. [Google Scholar] [CrossRef] [Green Version]
- Xie, W.; Dai, Q.; Liu, J.; Liu, Y.; Hellström, S.; Duan, M. Analysis of clinical and laboratory findings of idiopathic sudden sensorineural hearing loss. Sci. Rep. 2020, 10, 6057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taiwanese Center of Disease Control. The Received Rate of Influzena Vaccine in Taiwan; Taiwanese Center of Disease Control: Taipei, Taiwan, 2021. Available online: https://www.cdc.gov.tw/Category/MPage/JNTC9qza3F_rgt9sRHqV2Q (accessed on 1 April 2021).
- Tsai, Y.-W.; Huang, W.-F.; Wen, Y.-W.; Chen, P.-F. The relationship between influenza vaccination and outpatient visits for upper respiratory infection by the elderly in Taiwan. Value Health 2007, 10, 117–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.-H.; Chang, Y.-Y.; Kuo, S.-C.; Chen, Y.-T. Influenza vaccination and secondary prevention of cardiovascular disease among Taiwanese elders-A propensity score-matched follow-up study. PLoS ONE 2019, 14, e0219172. [Google Scholar]
- Lee, K.K.; Miller, M.R.; Shah, A.S. Air pollution and stroke. J. Stroke 2018, 20, 2. [Google Scholar] [CrossRef] [Green Version]
- Tsuzuki, N.; Wasano, K.; Oishi, N.; Hentona, K.; Shimanuki, M.; Nishiyama, T.; Hiraga, Y.; Shinden, S.; Ogawa, K. Severe sudden sensorineural hearing loss related to risk of stroke and atherosclerosis. Sci. Rep. 2021, 11, 20204. [Google Scholar] [CrossRef]
- Mustafić, H.; Jabre, P.; Caussin, C.; Murad, M.H.; Escolano, S.; Tafflet, M.; Périer, M.-C.; Marijon, E.; Vernerey, D.; Empana, J.-P. Main air pollutants and myocardial infarction: A systematic review and meta-analysis. JAMA 2012, 307, 713–721. [Google Scholar] [CrossRef]
- Chang, K.-H.; Tsai, S.C.-S.; Lee, C.-Y.; Chou, R.-H.; Fan, H.-C.; Lin, F.C.-F.; Lin, C.-L.; Hsu, Y.-C. Increased risk of sensorineural hearing loss as a result of exposure to air pollution. Int. J. Environ. Res. Public Health 2020, 17, 1969. [Google Scholar] [CrossRef] [Green Version]
- Ho, C.-H.; Tan, T.-Y.; Hwang, C.-F.; Lin, W.-C.; Wu, C.-N.; Yang, C.-H. Association of carotid intima-media thickness with the risk of sudden sensorineural hearing loss. PeerJ 2020, 8, e9276. [Google Scholar] [CrossRef]
- Mohammadi, M.; Taziki Balajelini, M.H.; Rajabi, A. Migraine and risk of sudden sensorineural hearing loss: A systematic review and meta-analysis. Laryngoscope Investig. Otolaryngol. 2020, 5, 1089–1095. [Google Scholar] [CrossRef]
- Tsai, Y.-T.; Chang, I.-J.; Hsu, C.-M.; Yang, Y.-H.; Liu, C.-Y.; Tsai, M.-S.; Chang, G.-H.; Lee, Y.-C.; Huang, E.I.; Lin, M.-H. Association between Sudden Sensorineural Hearing Loss and Preexisting Thyroid Diseases: A Nationwide Case-Control Study in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 834. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Pollutant | Mean ± Standard Deviation | 25% | 50% | 75% | Minimum | Maximum |
|---|---|---|---|---|---|---|
| PM2.5 (ppm) | 18 ± 10.64 | 12 | 18 | 26 | 2 | 85 |
| PM10 (ppm) | 36.57 ± 18.15 | 24 | 36.57 | 45 | 5 | 147 |
| O3 (ppm) | 25.6 ± 10.39 | 19.2 | 25.6 | 32.8 | 2.8 | 90 |
| NO2 (ppb) | 19.83 ± 7.26 | 15.86 | 19.83 | 24.26 | 2.38 | 65.63 |
| SO2 (ppb) | 2.6 ± 1.54 | 1.9 | 2.6 | 3.6 | 0.2 | 20.8 |
| CO (ppm) | 0.46 ± 0.2 | 0.37 | 0.46 | 0.58 | 0.08 | 2.63 |
| Air temperature (°C) | 23.79 ± 5.55 | 19.03 | 23.79 | 28.48 | 5.5 | 33.3 |
| Relative Humidity (%) | 73.42 ± 9.54 | 66.34 | 73.42 | 81 | 24.57 | 95.01 |
| PM2.5 | PM10 | O3 | NO2 | SO2 | CO | Temperature | RH | |
|---|---|---|---|---|---|---|---|---|
| PM2.5 | 0.843 *** | 0.233 *** | 0.520 *** | 0.441 *** | 0.557 *** | −0.127 *** | −0.222 *** | |
| PM10 | 0.843 *** | 0.348 *** | 0.451 *** | 0.384 *** | 0.473 *** | −0.186 *** | −0.359 *** | |
| O3 | 0.233 *** | 0.348 *** | −0.126 *** | 0.001 | −0.187 *** | −0.173 *** | −0.266 *** | |
| NO2 | 0.52 *** | 0.451 *** | −0.126 ** | 0.456 *** | 0.859 *** | −0.273 *** | 0.117 *** | |
| SO2 | 0.441 *** | 0.384 *** | 0.001 | 0.456 *** | 0.333 *** | 0.174 *** | −0.157 *** | |
| CO | 0.557 *** | 0.473 *** | −0.187 *** | 0.859 *** | 0.333 *** | −0.167 *** | 0.103 *** | |
| Temperature | −0.127 *** | −0.186 *** | −0.173 *** | −0.273 *** | 0.174 *** | −0.167 *** | −0.254 *** | |
| Relative Humidity | −0.222 *** | −0.359 *** | −0.266 *** | 0.117 *** | −0.157 *** | 0.103 *** | −0.254 *** | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, C.-G.; Chen, Y.-H.; Yen, S.-Y.; Lin, H.-C.; Lin, H.-C.; Chou, K.-R.; Cheng, C.-A. Air Pollution Exposure and the Relative Risk of Sudden Sensorineural Hearing Loss in Taipei. Int. J. Environ. Res. Public Health 2022, 19, 6144. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106144
Cheng C-G, Chen Y-H, Yen S-Y, Lin H-C, Lin H-C, Chou K-R, Cheng C-A. Air Pollution Exposure and the Relative Risk of Sudden Sensorineural Hearing Loss in Taipei. International Journal of Environmental Research and Public Health. 2022; 19(10):6144. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106144
Chicago/Turabian StyleCheng, Chun-Gu, Yu-Hsuan Chen, Shang-Yih Yen, Hui-Chen Lin, Hung-Che Lin, Kuei-Ru Chou, and Chun-An Cheng. 2022. "Air Pollution Exposure and the Relative Risk of Sudden Sensorineural Hearing Loss in Taipei" International Journal of Environmental Research and Public Health 19, no. 10: 6144. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106144