
Impact of High-Intensity Interval Training on Body Composition and Depressive Symptoms in Adults under Home Confinement

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedeures
2.3. Research Design
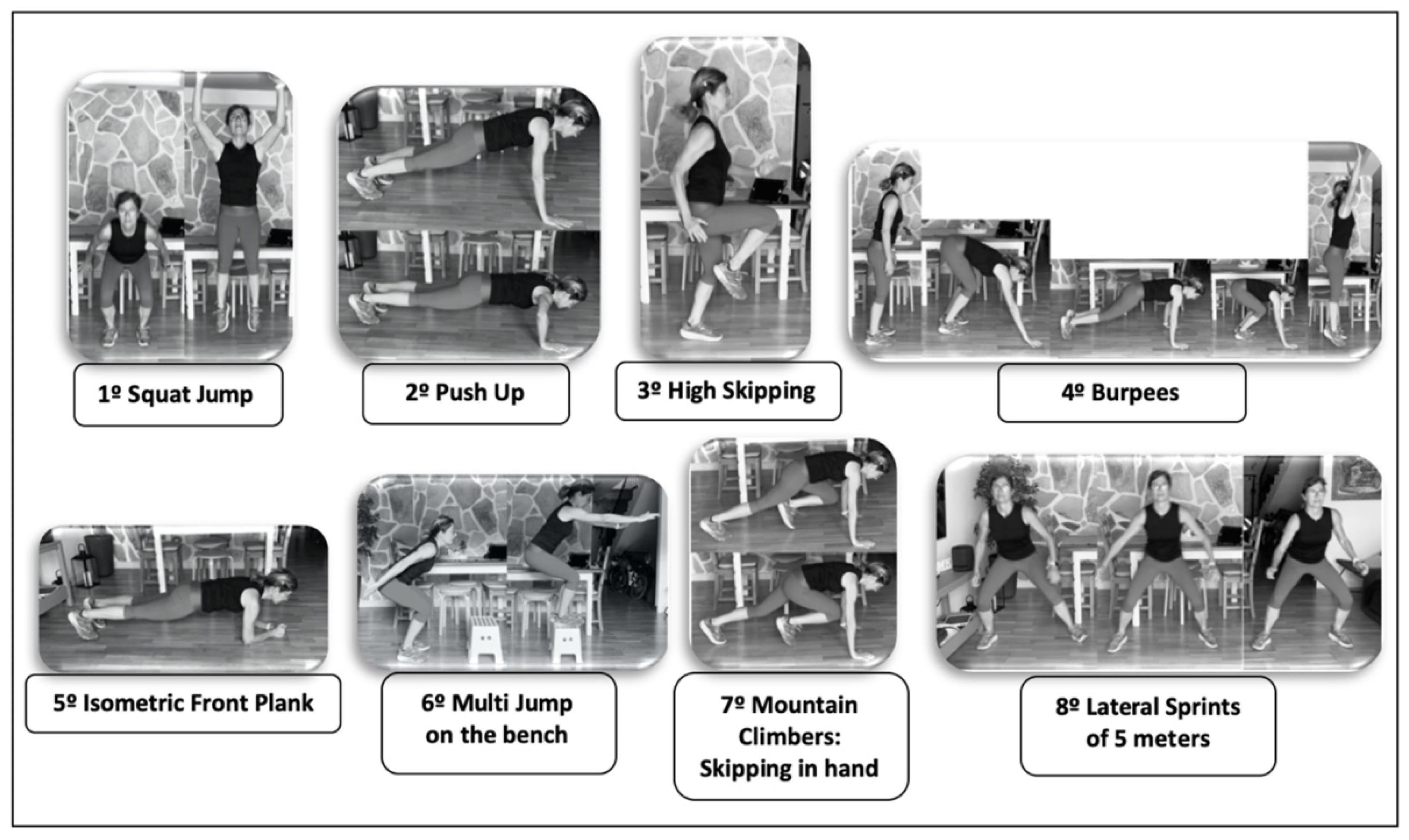
HIIT Training
2.4. Statistical Analysis
3. Results
3.1. Body Composition
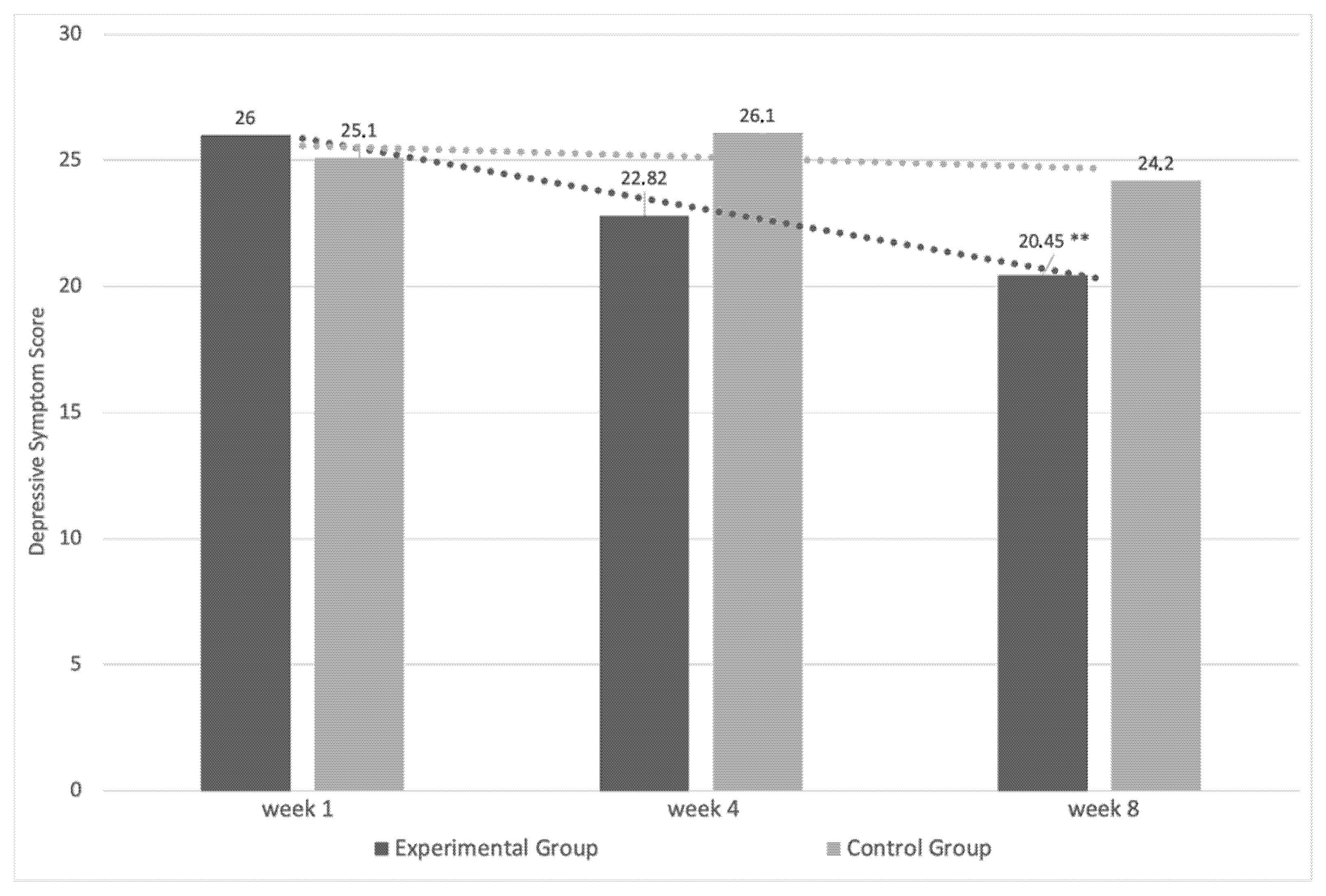
3.2. Depressive Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Scarmozzino, F.; Visioli, F. COVID-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Neill, E.; Meyer, D.; Toh, W.L.; Van Rheenen, T.E.; Phillipou, A.; Tan, E.J.; Rossell, S.L. Alcohol use in Australia during the early days of the COVID-19 pandemic: Initial results from the COLLATE project. Psychiatry Clin. Neurosci. 2020, 74, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Jacob, L.; Yakkundi, A.; McDermott, D.; Armstrong, N.C.; Barnett, Y.; López-Sánchez, G.F.; Martin, S.; Butler, L.; A Tully, M. Correlates of symptoms of anxiety and depression and mental wellbeing associated with COVID-19: A cross-sectional study of UK-based respondents. Psychiatry Res. 2020, 291, 113138. [Google Scholar] [CrossRef] [PubMed]
- Troyer, E.A.; Kohn, J.N.; Hong, S. Are we facing a crashing wave of neuropsychiatric sequelae of COVID-19? Neuropsychiatric symptoms and potential immunologic mechanisms. Brain Behav. Immun. 2020, 87, 34–39. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Martínez-Amat, A.; Cruz-Díaz, D.; Pérez-López, F.R. Osteosarcopenic obesity and fall prevention strategies. Maturitas 2015, 80, 126–132. [Google Scholar] [CrossRef]
- Michell, V.; Samaria, C.; Rudy, N.J.; Danyela, V.; Dantas, E. Effects of a concurrent physical exercise program on aerobic power and body composition in adults. J. Sports Med. Phys. Fitness. 2014, 54, 441–446. [Google Scholar] [PubMed]
- Ferreira, F.C.; De Medeiros, A.I.; Nicioli, C.; Nunes, J.E.D.; Shiguemoto, G.E.; Prestes, J.; Verzola, R.M.M.; Baldissera, V.; Perez, S.E.D.A. Circuit resistance training in sedentary women: Body composition and serum cyto-kine levels. Appl. Physiol. Nutr. Metab. 2010, 35, 163–171. [Google Scholar] [CrossRef]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A. Association between physical exercise and mental health in 1·2 million individuals in the USA between 2011 and 2015: A cross-sectional study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Weston, K.S.; Wisløff, U.; Coombes, J.S. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Br. J. Sports Med. 2014, 48, 1227–1234. [Google Scholar] [CrossRef]
- Alonso-Fernandez, D.; Fernández-Rodríguez, R.; Gutiérrez-Sánchez, A. Effect of a HIIT programme vs. Extensive Continuous Training on Inexperienced Individuals. Apunts Educació Física i Esports 2017, 130, 84–94. [Google Scholar] [CrossRef]
- Maillard, F.; Pereira, B.; Boisseau, N. Effect of High-Intensity Interval Training on Total, Abdominal and Visceral Fat Mass: A Meta-Analysis. Sports Med. 2018, 48, 269–288. [Google Scholar] [CrossRef]
- Alonso-Fernández, D.; Fernández-Rodríguez, R.; Taboada-Iglesias, Y.; Gutiérrez-Sánchez, Á. Impact of a HIIT protocol on body composition and VO2max in adolescents. Sci. Sports 2019, 34, 341–347. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-La-O, A.; Jurado-Fasoli, L.; Ruiz, J.R.; Castillo, M.J.; Gutiérrez, Á. Effects of different exercise training programs on body composition: A randomized control trial. Scand. J. Med. Sci. Sports 2019, 29, 968–979. [Google Scholar] [CrossRef] [PubMed]
- Dupuit, M.; Rance, M.; Morel, C.; Bouillon, P.; Pereira, B.; Bonnet, A.; Maillard, F.; Duclos, M.; Boisseau, N. Moderate-Intensity Continuous Training or High-Intensity Interval Training with or without Resistance Training for Altering Body Composition in Postmenopausal Women. Med. Sci. Sports Exerc. 2020, 52, 736–745. [Google Scholar] [CrossRef]
- Bartlett, D.B.; Willis, L.H.; Slentz, C.A.; Hoselton, A.; Kelly, L.; Huebner, J.L.; Kraus, V.B.; Moss, J.; Muehlbauer, M.J.; Spielmann, G.; et al. Ten weeks of high-intensity interval walk training is associated with reduced disease activity and improved innate immune function in older adults with rheumatoid arthritis: A pilot study. Arthritis Res. Ther. 2018, 20, 127. [Google Scholar] [CrossRef] [Green Version]
- Dorneles, G.P.; Da Silva, I.; Boeira, M.C.; Valentini, D.; Fonseca, S.G.; Lago, P.D.; Peres, A.; Romão, P.R.T. Cardiorespiratory fitness modulates the proportions of monocytes and T helper subsets in lean and obese men. Scand. J. Med. Sci. Sports 2019, 29, 1755–1765. [Google Scholar] [CrossRef]
- Reljic, D.; Lampe, D.; Wolf, F.; Zopf, Y.; Herrmann, H.J.; Fischer, J. Prevalence and predictors of dropout from high-intensity interval training in sedentary individuals: A meta-analysis. Scand. J. Med. Sci. Sports 2019, 29, 1288–1304. [Google Scholar] [CrossRef]
- Kikuchi, N.; Nakazato, K. Low-load bench press and push-up induce similar muscle hypertrophy and strength gain. J. Exerc. Sci. Fit. 2017, 15, 37–42. [Google Scholar] [CrossRef]
- Heymsfield, S.B. Tanita Institute Contract Study. Algorithm Development for Estimating Visceral Fat Rating. Ph.D. Thesis, Columbia University College of Physicians and Surgeons, New York, NY, USA, 2004. [Google Scholar]
- Cecchini, J.A.; Fernandez-Río, J.; Mendez-Gimenez, A. Physical activity, approach and avoidance temperament and depressive symptoms. Kinesiology 2019, 51, 60–69. [Google Scholar] [CrossRef] [Green Version]
- Kandel, D.B.; Davies, M. Epidemiology of depressive mood in adolescents: An empirical study. Arch. Gen. Psychiatry 1982, 39, 1205–1212. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.S.; Patten, C.A.; Gillin, J.C.; Kaplan, R.M.; Pierce, J.P. Cigarette smoking predicts development of depressive symptoms among U.S. adolescents. Ann. Behav. Med. 1997, 19, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Halliday, T.M.; Davy, B.M.; Clark, A.G.; Baugh, M.E.; Hedrick, V.E.; Marinik, E.L.; Flack, K.D.; Savla, J.; Winett, S.; Winett, R.A. Dietary Intake Modification in Response to a Participation in a Resistance Training Program for Sedentary Older Adults with Prediabetes: Findings from the Resist Diabetes Study. Eat. Behav. 2014, 15, 379–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabata, I.; Nishimura, K.; Kouzaki, M.; Hirai, Y.; Ogita, F.; Miyachi, M.; Yamamoto, K. Effects of moderate-intensity endurance and high-intensity intermittent training on anaerobic capacity and VO2max. Med. Sci. Sports Exerc. 1996, 28, 1327–1330. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- López-Moreno, M.; López, M.; Miguel, M.; Garcés-Rimón, M. Physical and Psychological Effects Related to Food Habits and Lifestyle Changes Derived from COVID-19 Home Confinement in the Spanish Population. Nutrients 2020, 12, 3445. [Google Scholar] [CrossRef]
- Rodríguez-Larrad, A.; Mañas, A.; Labayen, I.; González-Gross, M.; Espin, A.; Aznar, S.; Serrano-Sánchez, J.A.; Vera-Garcia, F.J.; González-Lamuño, D.; Ara, I.; et al. Impact of COVID-19 Confinement on Physical Activity and Sedentary Behaviour in Spanish University Students: Role of Gender. Int. J. Environ. Res. Public Health 2021, 18, 369. [Google Scholar] [CrossRef]
- Pérez-Rodrigo, C.; Gianzo Citores, M.; Hervás Bárbara, G.; Ruiz-Litago, F.; Casis Sáenz, L.; Arija, V.; López-Sobaler, A.M.; Martínez de Victoria, E.; Ortega, R.M.; Partearroyo, T.; et al. Patterns of Change in Dietary Habits and Physical Activity during Lockdown in Spain Due to the COVID-19 Pandemic. Nutrients 2021, 13, 300. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Wang, M.; Baker, J.S.; Quan, W.; Shen, S.; Fekete, G.; Gu, Y. A Preventive Role of Exercise Across the Coronavirus 2 (SARS-CoV-2) Pandemic. Front. Physiol. 2020, 11, 572718. [Google Scholar] [CrossRef]
- De Paula, C.C.; Machado, S.; Costa, G.D.C.T.; Sales, M.M.; Miranda, T.G.; Barsanulfo, S.R.; Murillo-Rodriguez, E.; Budde, H.; Filho, A.S.S. High intensity interval training (HIIT) as a viable alternative to induce the prevention of respiratory diseases: A point of view of exercise immunology during COVID-19 outbreak. Res. Soc. Dev. 2020, 9, e7069109186. [Google Scholar] [CrossRef]
- Souza, D.; Coswig, V.; De Lira, C.A.B.; Gentil, P. H″IT″ting the Barriers for Exercising during Social Isolation. Biology 2020, 9, 245. [Google Scholar] [CrossRef] [PubMed]
- Borrega-Mouquinho, Y.; Sánchez-Gómez, J.; Fuentes-García, J.P.; Collado-Mateo, D.; Villafaina, S. Effects of high-intensity interval training and moderate-intensity training on stress, depression, anxiety, and resilience in healthy adults during coronavirus disease 2019 confinement: A randomized controlled trial. Front. Psychol. 2021, 12, 643069. [Google Scholar] [CrossRef] [PubMed]
- Soylu, Y.; Arslan, E.; Sogut, M.; Kilit, B.; Clemente, F. Effects of self-paced high-intensity interval training and moderate-intensity continuous training on the physical performance and psychophysiological responses in recreationally active young adults. Biol. Sport 2021, 38, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.; Van Den Berg, R.; Ward, R.E.; Keech, A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 635–646. [Google Scholar] [CrossRef]
- Nybo, L.; Sundstrup, E.; Jakobsen, M.D.; Mohr, M.; Hornstrup, T.; Simonsen, L.; Bülow, J.; Randers, M.B.; Nielsen, J.J.; Aagaard, P.; et al. High-intensity training versus traditional exercise interventions for promoting health. Med. Sci. Sports Exerc. 2010, 42, 1951–1958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Violant-Holz, V.; Gallego-Jiménez, M.G.; González-González, C.S.; Muñoz-Violant, S.; Rodríguez, M.J.; Sansano-Nadal, O.; Guerra-Balic, M. Psychological Health and Physical Activity Levels during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9419. [Google Scholar] [CrossRef]
- Méndez-Giménez, A.; Cecchini, J.A.; Fernández-Río, J.; Carriedo, A. Physical Activity and Prevention of Depressive Symptoms in the Spanish Population during Confinement due to COVID-19. Psicothema 2021, 33, 111–117. [Google Scholar] [CrossRef]
- Currier, D.; Lindner, R.; Spittal, M.J.; Cvetkovski, S.; Pirkis, J.; English, D.R. Physical activity and depression in men: Increased activity duration and intensity associated with lower likelihood of current depression. J. Affect. Disord. 2020, 260, 426–431. [Google Scholar] [CrossRef]
- Harvey, S.B.; Øverland, S.; Hatch, S.L.; Wessely, S.; Mykletun, A.; Hotopf, M. Exercise and the prevention of depression: Results of the HUNT cohort study. Am. J. Psychiatry 2018, 175, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Mammen, G.; Faulkner, G. Physical activity and the prevention of depression: A systematic review of prospective studies. Am. J. Prev. Med. 2013, 45, 649–657. [Google Scholar] [CrossRef]
- Arslan, E.; Can, S.; Demirkan, E. Effect of short-term aerobic and combined training program on body composition, lipids profile and psychological health in premenopausal women. Sci. Sports 2017, 32, 106–113. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group | N | Age (Years Old) | Weight (kg) | Height (cm) | |||
|---|---|---|---|---|---|---|---|
| EG | 11 | 34.4 | 4.9 | 72.56 | 12.26 | 170 | 10 |
| CG | 10 | 36.5 | 6.4 | 70.56 | 11.02 | 172 | 11 |
| “Tabata” Blocks | Min. Break between Blocks | Nº Exercises/Session | Nº Sessions per Week | HIIT Minutes per Week | |
|---|---|---|---|---|---|
| Weeks 1 and 2 | 2 | 2.5 | 16 | 2 | 16 |
| Week 3 | 3 | 2 | 24 | 2 | 24 |
| Weeks 4 and 5 | 3 | 2 | 24 | 3 | 36 |
| Weeks 6 and 7 | 3 | 1 | 24 | 3 | 36 |
| Week 8 | 4 | 2 | 32 | 3 | 48 |
| EG (n = 11) | CG (n = 10) | |||||
|---|---|---|---|---|---|---|
| Variables | M1 | M2 | % Change | M1 | M2 | % Change |
| Kcal/day | 2149.1 ± 413 | 2203.3 ± 511 | 2.51 | 2228.8 ± 488 | 2335.6 ± 402 | 4.81 |
| Proteins/day (%) | 18 ± 4 | 17 ± 3 | −1 | 17 ± 2 | 17 ± 3 | 0 |
| Lipids/day (%) | 39 ± 5 | 41 ± 6 | 2 | 40 ± 7 | 43 ± 5 | 3 |
| Carbohydrates/day (%) | 43 ± 7 | 42 ± 5 | −1 | 43 ± 8 | 40 ± 7 | −3 |
| GE (n = 11) | GC (n = 10) | |||||
|---|---|---|---|---|---|---|
| Variables | M1 | M2 | % Change | M1 | M2 | % Change |
| Weight (kg) | 72.56 ± 12.26 | 71.84 ± 11.77 | −0.99 | 70.56 ± 11.02 | 72.44 ± 11.53 | 2.66 * |
| BMI (kg/m2) | 24.54 ± 2.74 | 24.32 ± 2.68 | −0.89 | 23.84 ± 1.86 | 24.51 ± 2.26 | 2.81 * |
| FM (%) | 24.09 ± 4.31 | 22.98 ± 3.82 | −4.61 * | 25.20 ± 3.98 | 27.31 ± 4.21 | 8.37 ** |
| FM (kg) | 17.75 ± 5.16 | 16.81 ± 4.73 | −5.29 * | 18.01 ± 5.02 | 20.07 ± 5.71 | 11.43 * |
| FBMI (kg/m2) | 5.99 ± 1.59 | 5.67 ± 1.43 | −5.34 * | 6.06 ± 1.34 | 6.75 ± 1.54 | 11.38 ** |
| LM (kg) | 54.81 ± 7.94 | 55.04 ± 7.63 | 0.42 | 52.55 ± 6.85 | 52.37 ± 6.61 | −0.34 |
| LBMI (kg/m2) | 18.56 ± 1.35 | 18.66 ± 1.42 | 0.54 | 17.78 ± 0.85 | 17.75 ± 1.09 | −0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Fernández, D.; Fernández-Rodríguez, R.; Taboada-Iglesias, Y.; Gutiérrez-Sánchez, Á. Impact of High-Intensity Interval Training on Body Composition and Depressive Symptoms in Adults under Home Confinement. Int. J. Environ. Res. Public Health 2022, 19, 6145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106145
Alonso-Fernández D, Fernández-Rodríguez R, Taboada-Iglesias Y, Gutiérrez-Sánchez Á. Impact of High-Intensity Interval Training on Body Composition and Depressive Symptoms in Adults under Home Confinement. International Journal of Environmental Research and Public Health. 2022; 19(10):6145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106145
Chicago/Turabian StyleAlonso-Fernández, Diego, Rosana Fernández-Rodríguez, Yaiza Taboada-Iglesias, and Águeda Gutiérrez-Sánchez. 2022. "Impact of High-Intensity Interval Training on Body Composition and Depressive Symptoms in Adults under Home Confinement" International Journal of Environmental Research and Public Health 19, no. 10: 6145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106145