
Assessment of Pain-Related Fear in Indigenous Australian Populations Using the Fear of Pain Questionnaire-9 (FPQ-9)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Measures
2.2.1. EQ-5D-5L
2.2.2. Fear of Pain
2.3. Statistical Analysis
2.3.1. Power Calculation
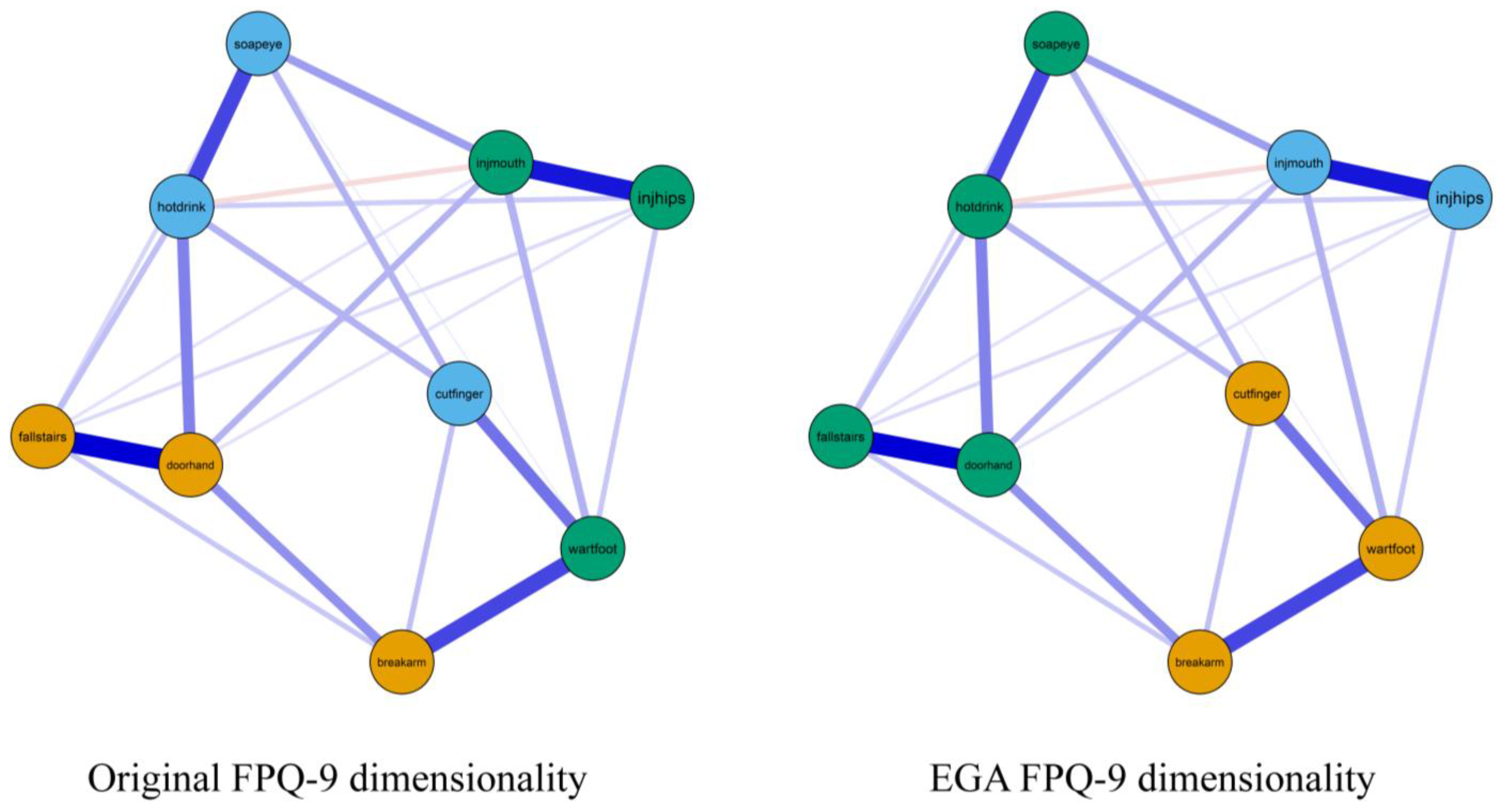
2.3.2. Network Estimation
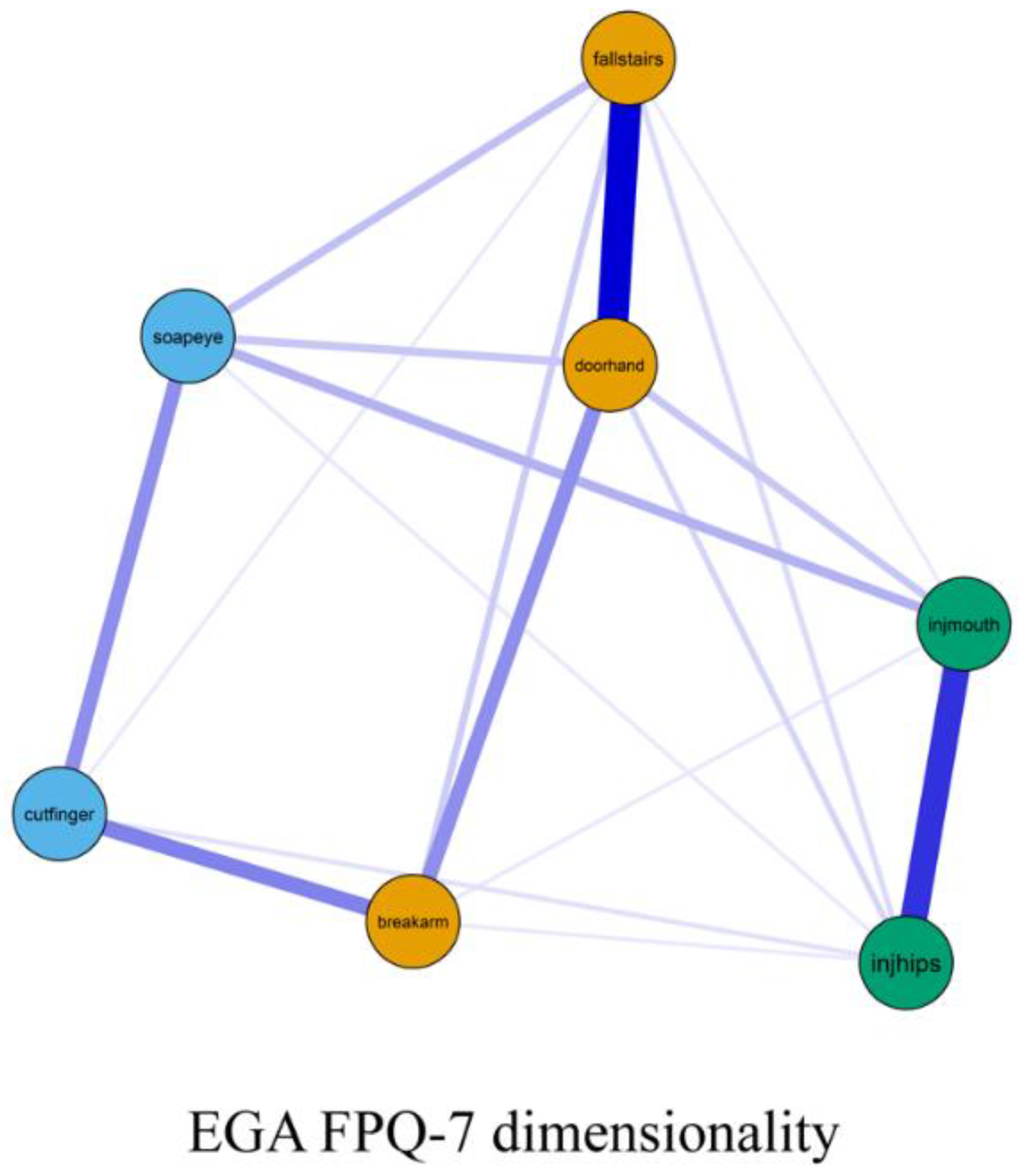
2.3.3. Exploratory Graph Analysis (EGA)
2.3.4. Model Fit
2.3.5. Internal Consistency and Reliability
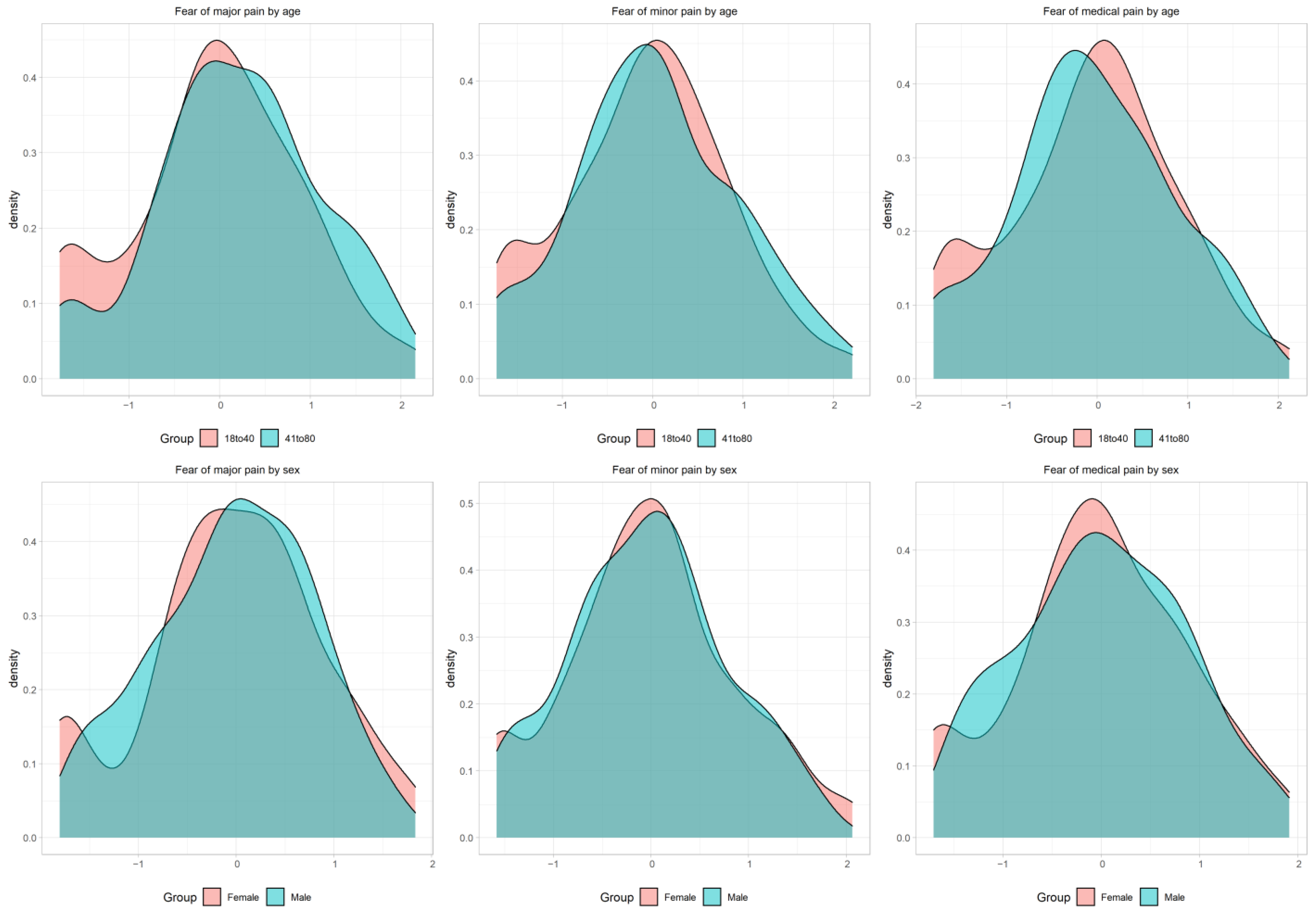
2.3.6. Measurement Invariance
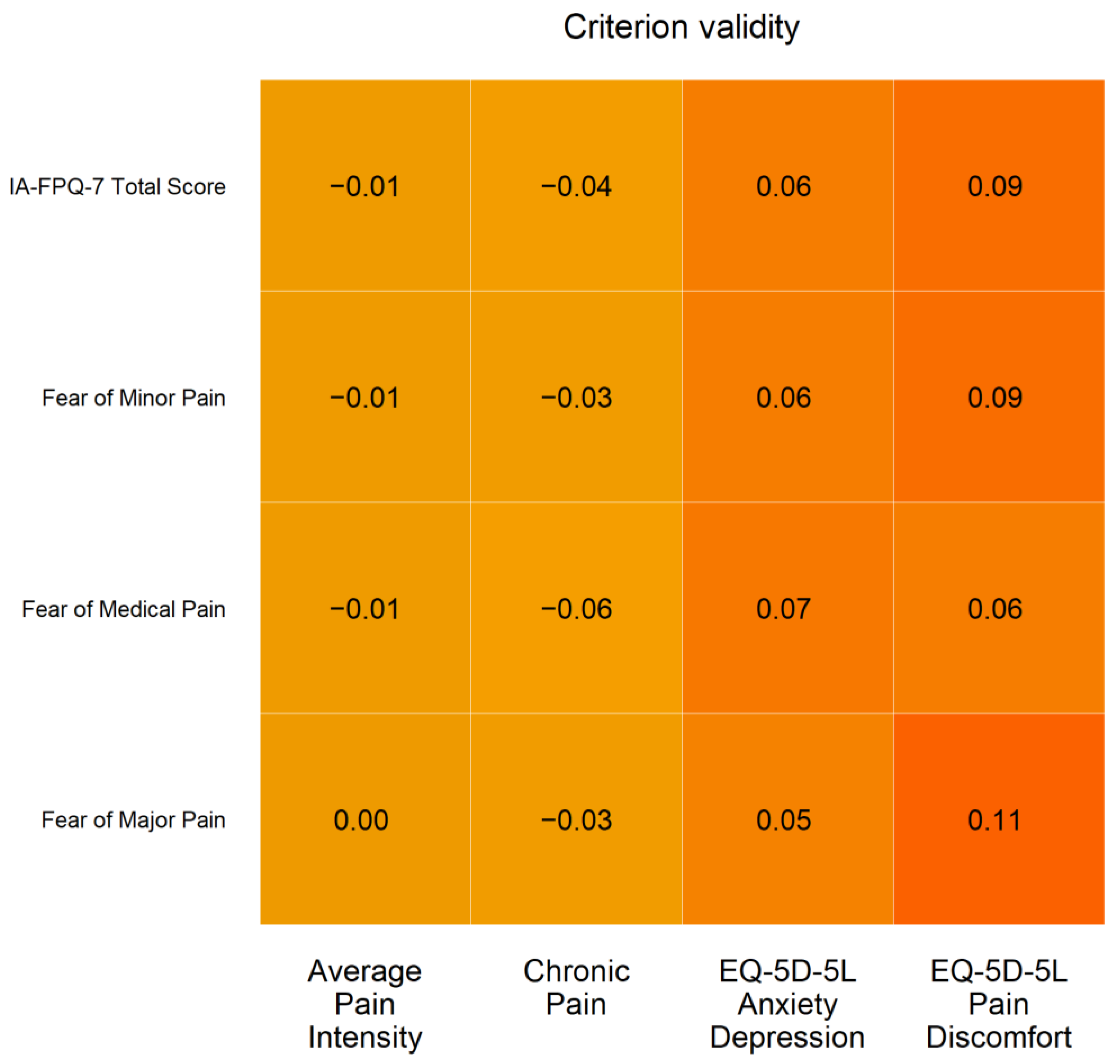
2.3.7. Criterion Validity
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Gatzounis, R.; Vlaeyen, J. Behavioural inhibition in the context of pain: Measurement and conceptual issues. Scand. J. Pain 2017, 17, 132–133. [Google Scholar] [CrossRef] [PubMed]
- Storheim, K.; Brox, J.I.; Holm, I.; Bo, K. Predictors of return to work in patients sick listed for sub-acute low back pain: A 12-month follow-up study. J. Rehabil. Med. 2005, 37, 365–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, J.A.; Franklin, G.; Fulton-Kehoe, D.; Sheppard, L.; Wickizer, T.M.; Wu, R.; Gluck, J.V.; Egan, K. Worker recovery expectations and fear-avoidance predict work disability in a population-based workers’ compensation back pain sample. Spine 2006, 31, 682–689. [Google Scholar] [CrossRef]
- Di Tella, M.; Ghiggia, A.; Testa, S.; Castelli, L.; Adenzato, M. The Fear of Pain Questionnaire: Factor structure, validity and reliability of the Italian translation. PLoS ONE 2019, 14, e0210757. [Google Scholar] [CrossRef]
- Linton, S.J.; Flink, I.K.; Vlaeyen, J.W. Understanding the etiology of chronic pain from a psychological perspective. Phys. Ther. 2018, 98, 315–324. [Google Scholar] [CrossRef]
- McNeil, D.W.; Rainwater, A.J. Development of the Fear of Pain Questionnaire—III. J. Behav. Med. 1998, 21, 389–410. [Google Scholar] [CrossRef] [PubMed]
- Mittinty, M.M.; McNeil, D.W.; Brennan, D.S.; Randall, C.L.; Mittinty, M.N.; Jamieson, L. Assessment of pain-related fear in individuals with chronic painful conditions. J. Pain Res. 2018, 11, 3071–3077. [Google Scholar] [CrossRef] [Green Version]
- Parr, J.J.; Borsa, P.A.; Fillingim, R.B.; Tillman, M.D.; Manini, T.M.; Gregory, C.M.; George, S.Z. Pain-related fear and catastrophizing predict pain intensity and disability independently using an induced muscle injury model. J. Pain 2012, 13, 370–378. [Google Scholar] [CrossRef] [Green Version]
- Topcu, S.Y.; Kostak, M.A.; Semerci, R.; Guray, O. Effect of gum chewing on pain and anxiety in Turkish children during intravenous cannulation: A randomized controlled study. J. Pediatr. Nurs. 2020, 52, e26–e32. [Google Scholar] [CrossRef]
- Solé, E.; Castarlenas, E.; Sánchez-Rodríguez, E.; Galán, S.; de la Vega, R.; Jensen, M.P.; Miró, J. The reliability and validity of the Spanish version of the Fear of Pain Questionnaire. J. Health Psychol. 2019, 24, 1134–1144. [Google Scholar] [CrossRef]
- van Wijk, A.J.; Hoogstraten, J. Dutch translation of the Fear of Pain Questionnaire: Factor structure, reliability and validity. Eur. J. Pain 2006, 10, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Albaret, M.C.; Sastre, M.T.; Cottencin, A.; Mullet, E. The Fear of Pain questionnaire: Factor structure in samples of young, middle-aged and elderly European people. Eur. J. Pain 2004, 8, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, S.; Esculpi, D.; Carvalho, A.R.; Pereira, D.R.; Torres, S.; Mercado, F.; Barbosa, F. Fear of Pain Questionnaire: Adaptação para o português europeu. Rev. Bras. Reumatol. 2016, 56, 377–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNeil, D.W.; Kennedy, S.G.; Randall, C.L.; Addicks, S.H.; Wright, C.D.; Hursey, K.G.; Vaglienti, R. Fear of Pain Questionnaire-9: Brief assessment of pain-related fear and anxiety. Eur. J. Pain 2018, 22, 39–48. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Li, S.; He, J.; Cai, D.; Dai, Y.; Feng, L.; Sun, C.; Zhu, X. Translation and Validation of Fear of Pain-9 Items into Simplified Chinese Version for Mainland China. J. Pain Res. 2021, 14, 35. [Google Scholar] [CrossRef]
- Mittinty, M.M.; McNeil, D.W.; Jamieson, L.M. Limited evidence to measure the impact of chronic pain on health outcomes of Indigenous people. J. Psychosom. Res. 2018, 107, 53. [Google Scholar] [CrossRef] [Green Version]
- Jamieson, L.M.; Garvey, G.; Hedges, J.; Leane, C.; Hill, I.; Brown, A.; Ju, X.; Sethi, S.; Order, D.; Logan, R.M.; et al. Cohort profile: Indigenous human papillomavirus and oropharyngeal squamous cell carcinoma study-a prospective longitudinal cohort. BMJ Open 2021, 11, e046928. [Google Scholar] [CrossRef]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Geisinger, K.F. Cross-cultural normative assessment: Translation and adaptation issues influencing the normative interpretation of assessment instruments. Psychol. Assess. 1994, 6, 304. [Google Scholar] [CrossRef]
- Golino, H.; Christensen, A. EGAnet: Exploratory Graph Analysis: A framework for Estimating the Number of Dimensions in Multivariate Data Using Network Psychometrics, Version 0.4; 2019. Available online: https://cran.r-project.org/web/packages/EGAnet/index.html (accessed on 1 May 2022).
- Constantin, M.A.; Schuurman, N.K.; Vermunt, J. A General Monte Carlo Method for Sample Size Analysis in the Context of Network Models. PsyArXiv. 2021. [Google Scholar] [CrossRef]
- Jorgensen, T.D.; Pornprasertmanit, S.; Schoemann, A.M.; Rosseel, Y.; Miller, P.; Quick, C. semTools: Useful Tools for Structural Equation Modelling, R Package Version 0.5-1; 2018. Available online: https://cran.r-project.org/web/packages/semTools/index.html (accessed on 1 May 2022).
- Graham, J.W. Missing data analysis: Making it work in the real world. Annu. Rev. Psychol. 2009, 60, 549–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epskamp, S.; Fried, E.I. A tutorial on regularized partial correlation networks. Psychol. Methods 2018, 23, 617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blondel, V.D.; Guillaume, J.L.; Lambiotte, R.; Lefebvre, E. Fast unfolding of communities in large networks. J. Stat. Mech. Theory Exp. 2008, 2008, P10008. [Google Scholar] [CrossRef] [Green Version]
- Christensen, A.P.; Golino, H. Estimating Factors with Psychometric Networks: A Monte Carlo Simulation Comparing Community Detection Algorithms. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Sellbom, M.; Tellegen, A. Factor analysis in psychological assessment research: Common pitfalls and recommendations. Psychol. Assess. 2019, 31, 1428. [Google Scholar] [CrossRef]
- Dunn, T.J.; Baguley, T.; Brunsden, V. From alpha to omega: A practical solution to the pervasive problem of internal consistency estimation. Br. J. Psychol. 2014, 105, 399–412. [Google Scholar] [CrossRef] [Green Version]
- Svetina, D.; Rutkowski, L.; Rutkowski, D. Multiple-group invariance with categorical outcomes using updated guidelines: An illustration using M plus and the lavaan/semtools packages. Struct. Equ. Model. 2020, 27, 111–130. [Google Scholar] [CrossRef]
- Wu, H.; Estabrook, R. Identification of confirmatory factor analysis models of different levels of invariance for ordered categorical outcomes. Psychometrika 2016, 81, 1014–1045. [Google Scholar] [CrossRef] [Green Version]
- Hancock, G.R. Effect size, power, and sample size determination for structured means modeling and MIMIC approaches to between-groups hypothesis testing of means on a single latent construct. Psychometrika 2001, 66, 373–388. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare (AIHW). Chronic Pain in Australia; AIHW: Canberra, Australia, 2020.
- Furr, R.M.; Bacharach, V.R. Psychometrics: An Introduction 2013; Sage: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Santiago, P.H.R.; Roberts, R.; Smithers, L.G.; Jamieson, L. Stress beyond coping? A Rasch analysis of the Perceived Stress Scale (PSS-14) in an Aboriginal population. PLoS ONE 2019, 14, e0216333. [Google Scholar] [CrossRef] [PubMed]
- Santiago, P.H.; Nielsen, T.; Roberts, R.; Smithers, L.G.; Jamieson, L. Sense of personal control: Can it be assessed culturally unbiased across Aboriginal and non-Aboriginal Australians? PLoS ONE 2020, 15, e0239384. [Google Scholar] [CrossRef] [PubMed]
- DeVellis, R.F. Scale Development: Theory and Applications; Sage Publications: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Lin, I.B.; Ryder, K.; Coffin, J.; Green, C.; Dalgety, E.; Scott, B.; Straker, L.M.; Smith, A.J.; O’Sullivan, P.B. Addressing disparities in low back pain care by developing culturally appropriate information for aboriginal australians: “My Back on Track, My Future”. Pain Med. 2017, 18, 2070–2080. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.; Nelson, J.; Atkinson, C. Trauma, transgenerational transfer and effects on community wellbeing. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice; Australian Institute of Health and Welfare: Canberra, Australia, 2010; pp. 135–144. [Google Scholar]
- Pointer, S.; Harrison, J.; Avefua, S. Hospitalised Injury among Aboriginal and Torres Strait Islander People 2011–2012 to 2015–2016. 2019. Available online: https://www.aihw.gov.au/reports/injury/hospitalised-injury-among-aboriginal-and-torres-st/contents/table-of-contents (accessed on 5 February 2022).
- Boufous, S.; Ivers, R.; Senserrick, T.; Martiniuk, A.; Clapham, K. Underlying Causes and Effects of Injury in Australian Aboriginal Populations: A Rapid Review; Sax Institute: Sydney, Australia, 2010. [Google Scholar]
- Green, S. Aboriginal and Torres Strait Islander Women’s Taskforce on Violence Report, 2000. Aborig. Isl. Health Work 2001, 25, 8–26. [Google Scholar]
- Hunter, E.M. Stains on the caring mantle doctors in Aboriginal Australia have a history. Med. J. Aust 1991, 155, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Mills, S.E.E.; Nicolson, K.P.; Smith, B.H. Chronic pain: A review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth 2019, 123, e273–e283. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.; Arnold, A.L.; Dunn, R.; Keeffe, J.; Taylor, H. Sampling and recruitment methodology for a national eye health survey of Indigenous Australians. Aust. N. Z. J. 2010, 34, 554–562. [Google Scholar] [CrossRef]
- Mhurchu, C.N.; Blakely, T.; Funaki-Tahifote, M.; McKerchar, C.; Wilton, J.; Chua, S.; Jiang, Y. Inclusion of indigenous and ethnic minority populations in intervention trials: Challenges and strategies in a New Zealand supermarket study. J. Epidemiol. Community Health 2009, 63, 850–855. [Google Scholar] [CrossRef]
- Borsboom, D.; Deserno, M.K.; Rhemtulla, M.; Epskamp, S.; Fried, E.I.; McNally, R.J.; Robinaugh, D.J.; Perugini, M.; Dalege, J.; Costantini, G.; et al. Network analysis of multivariate data in psychological science. Nat. Rev. Dis. Primers 2021, 1, 58. [Google Scholar] [CrossRef]
- Richiardi, L.; Pizzi, C.; Pearce, N. Commentary: Representativeness is usually not necessary and often should be avoided. Int. J. Epidemiol. 2013, 42, 1018–1022. [Google Scholar] [CrossRef] [Green Version]
- Rothman, K.J.; Gallacher, J.E.; Hatch, E.E. Why representativeness should be avoided. Int. J. Epidemiol. 2013, 42, 1012–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HPOVC Study (n = 750) | Complete Case Sample (n = 735) | |||
|---|---|---|---|---|
| N | % | N | % | |
| Age | ||||
| Mean (SD) | 40.7 (14.6) | 40.7 (14.5) | ||
| Missing | 0 | 0.0 | 0 | 0.0 |
| Sex | ||||
| Male | 234 | 31.2 | 228 | 31.0 |
| Female | 508 | 67.7 | 501 | 68.2 |
| Missing | 8 | 1.1 | 6 | 0.8 |
| Education | ||||
| High School completed | 487 | 64.9 | 480 | 65.3 |
| Technical education or university | 253 | 33.8 | 246 | 33.5 |
| Missing | 10 | 1.3 | 9 | 1.2 |
| Employment | ||||
| Employed | 193 | 25.8 | 189 | 25.7 |
| Unemployed/Benefits | 517 | 68.9 | 507 | 69.0 |
| Other/Missing | 40 | 5.3 | 39 | 5.3 |
| Access to health care card | ||||
| Yes | 161 | 21.5 | 157 | 21.3 |
| No | 551 | 73.5 | 540 | 73.5 |
| Do not know/Missing | 38 | 5.0 | 38 | 5.2 |
| χ2 | df | p-Value | RMSEA | 90% CI | CFI | TEFIvn | |
|---|---|---|---|---|---|---|---|
| One-factor structure | 311.694 | 27 | <0.001 | 0.143 | (0.129–0.158) | 0.957 | 0.000 |
| Original FPQ-9 structure | 263.929 | 24 | <0.001 | 0.139 | (0.125–0.155) | 0.964 | −1.845 |
| EGA FPQ-9 structure | 174.880 | 24 | <0.001 | 0.111 | (0.096–0.126) | 0.977 | −2.077 |
| EGA FPQ-7 structure a | 37.408 | 11 | <0.001 | 0.068 | (0.045–0.093) | 0.981 | - |
| Items | Factor Loadings | ||
|---|---|---|---|
| Fear of Major Pain | Fear of Minor Pain | Fear of Medical/Dental Pain | |
| 0.87 (0.02) | 0.00 (0.00) | 0.00 (0.00) |
| 0.88 (0.02) | 0.00 (0.00) | 0.00 (0.00) |
| 0.73 (0.03) | 0.00 (0.00) | 0.00 (0.00) |
| 0.00 (0.00) | 0.83 (0.03) | 0.00 (0.00) |
| 0.00 (0.00) | 0.77 (0.03) | 0.00 (0.00) |
| 0.00 (0.00) | 0.00 (0.00) | 0.85 (0.02) |
| 0.00 (0.00) | 0.00 (0.00) | 0.87 (0.02) |
| Factor Correlations | |||
| 0.80 (0.03) | ||
| 0.86 (0.02) | ||
| 0.84 (0.03) | ||
| Model | χ2 | df | p-Value | RMSEA | 90% CI | CFI | ∆χ2 (df) | p-Value |
|---|---|---|---|---|---|---|---|---|
| Age | ||||||||
| Configural | 53.082 | 22 | <0.001 | 0.074 | (0.049, 0.100) | 0.994 | - | - |
| Constrained Thresholds | 69.086 | 36 | 0.001 | 0.060 | (0.038, 0.081) | 0.993 | 10.31 (14) | 0.739 |
| Metric | 65.331 | 40 | 0.007 | 0.050 | (0.026, 0.071) | 0.995 | 0.61 (4) | 0.961 |
| Scalar | 77.425 | 44 | 0.001 | 0.054 | (0.038, 0.081) | 0.993 | 8.96 (4) | 0.062 |
| Sex | ||||||||
| Configural | 76.879 | 22 | <0.001 | 0.099 | (0.075, 0.124) | 0.989 | - | - |
| Constrained Thresholds | 93.578 | 36 | <0.001 | 0.079 | (0.060, 0.099) | 0.988 | 10.00 (14) | 0.762 |
| Metric | 90.535 | 40 | <0.001 | 0.070 | (0.051, 0.090) | 0.989 | 4.13 (4) | 0.389 |
| Scalar | 85.656 | 44 | <0.001 | 0.061 | (0.041, 0.080) | 0.991 | 3.47 (4) | 0.482 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mittinty, M.M.; Santiago, P.H.R.; Jamieson, L. Assessment of Pain-Related Fear in Indigenous Australian Populations Using the Fear of Pain Questionnaire-9 (FPQ-9). Int. J. Environ. Res. Public Health 2022, 19, 6256. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106256
Mittinty MM, Santiago PHR, Jamieson L. Assessment of Pain-Related Fear in Indigenous Australian Populations Using the Fear of Pain Questionnaire-9 (FPQ-9). International Journal of Environmental Research and Public Health. 2022; 19(10):6256. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106256
Chicago/Turabian StyleMittinty, Manasi Murthy, Pedro H. R. Santiago, and Lisa Jamieson. 2022. "Assessment of Pain-Related Fear in Indigenous Australian Populations Using the Fear of Pain Questionnaire-9 (FPQ-9)" International Journal of Environmental Research and Public Health 19, no. 10: 6256. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106256