
Association between Fathers’ Use of Heated Tobacco Products and Urinary Cotinine Concentrations in Their Spouses and Children

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measurement
2.2.1. Questionnaire for SHS Exposure and Definitions
2.2.2. Determination of Urinary Total Nicotine Metabolites
2.2.3. LC/MS/MS System
Apparatus
Sample Preparation
Creatinine Assay
2.3. Ethical Considerations
2.4. Data Analysis
3. Results
3.1. Study Population Characteristics
3.2. SHS Exposure in Spouses and Children from Fathers Defined by Urinary Levels of TNMs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Strobe Statement
References
- Heated Tobacco Products (HTPs) Information Sheet, 2nd ed.; World Health Organization (WHO): Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/WHO-HEP-HPR-2020.2 (accessed on 31 December 2021).
- WHO Study Group on Tobacco Product Regulation: Report on the Scientific Basis of Tobacco Product Regulation: Eighth Report of a WHO Study Group. Available online: https://www.who.int/publications/i/item/9789240022720 (accessed on 6 December 2021).
- Tabuchi, T.; Gallus, S.; Shinozaki, T.; Nakaya, T.; Kunugita, N.; Colwell, B. Heat-not-burn tobacco product use in Japan: Its prevalence, predictors and perceived symptoms from exposure to secondhand heat-not-burn tobacco aerosol. Tob. Control 2018, 27, e25–e33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hori, A.; Tabuchi, T.; Kunugita, N. Rapid increase in heated tobacco product (HTP) use from 2015 to 2019: From the Japan ‘Society and New Tobacco’ Internet Survey (JASTIS). Tob. Control 2020, 30, 474–475. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health and Nutrition. The National Health and Nutrition. Available online: https://www.mhlw.go.jp/stf/newpage_14156.html (accessed on 6 December 2021).
- World Health Organization. WHO Report on the Global Tobacco Epidemic, 2021: Addressing New and Emerging Products. 27 July 2021. Available online: https://www.who.int/publications/i/item/9789240032095 (accessed on 31 December 2021).
- World Health Organization. International Agency for Research on Cancer (IARC). IARC Handbook of Cancer Prevention vol.14.. 2011. Available online: https://handbooks.iarc.fr (accessed on 31 December 2021).
- Ministry of Health. Outline of the Act on the Partial Revision of the Health Promotion Act (No.78 of 2108). Available online: https://www.mhlw.go.jp/english/policy/health-medical/health/dl/201904kenko.pdf (accessed on 6 December 2021).
- Sansone, G.; Fong, G.T.; Meng, G.; Craig, L.V.; Xu, S.S.; Quah, A.C.K.; Ouimet, J.; Mochizuki, Y.; Yoshimi, I.; Tabuchi, T. Secondhand Smoke Exposure in Public Places and Support for Smoke-Free Laws in Japan: Findings from the 2018 ITC Japan Survey. Int. J. Environ. Res. Public Health 2020, 17, 979–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekki, K.; Inaba, Y.; Uchiyama, S.; Kunugita, N. Comparison of Chemicals in Mainstream Smoke in Heat-not-burn Tobacco and Combustion Cigarettes. J. UOEH 2017, 39, 201–207. [Google Scholar] [CrossRef] [Green Version]
- Torres, S.; Merino, C.; Paton, B.; Correig, X.; Ramírez, N. Biomarkers of Exposure to Secondhand and Thirdhand Tobacco Smoke: Recent Advances and Future Perspectives. Int. J. Environ. Res. Public Health 2018, 15, 2693–2718. [Google Scholar] [CrossRef] [Green Version]
- Levine, H.; Berman, T.; Goldsmith, R.; Göen, T.; Spungen, J.; Novack, L.; Amitai, Y.; Shohat, T.; Grotto, I. Exposure to tobacco smoke based on urinary cotinine levels among Israeli smoking and nonsmoking adults: A cross-sectional analysis of the first Israeli human biomonitoring study. BMC Public Health 2013, 13, 1241–1249. [Google Scholar] [CrossRef] [Green Version]
- Benowitz, N.L. Biomarkers of environmental tobacco exposure. Environ. Health Perspect. 1999, 107, 349–355. [Google Scholar]
- Schick, S.F.; Blount, B.C.; Jacob, P., 3rd; Saliba, N.A.; Bernert, J.T.; Hellani, A.E.; Jatlow, P.; Pappas, R.S.; Wang, L.; Foulds, J.; et al. Biomarkers of exposure to new and emerging tobacco delivery products. Am. J. Phisiol. Lung Cell Mol. Physiol. 2017, 313, L425–L452. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Yang, M.; Huang, Z.; Tian, L.; Niu, L.; Xiao, S. Urinary cotinine concentrations in preschool children showed positive associations with smoking fathers. Acta Paediatr. 2017, 106, 67–73. [Google Scholar] [CrossRef]
- De Jesús, V.R.; Bhandari, D.; Zhang, L.; Reese, C.; Capella, K.; Tevis, D.; Zhu, W.; Del Valle-Pinero, A.Y.; Lagaud, G.; Chang, J.T.; et al. Urinary Biomarkers of Exposure to Volatile Organic Compounds from the Population Assessment of Tobacco and Health Study Wave 1 (2013–2014). Int. J. Environ. Res. Public Health 2020, 17, 5408. [Google Scholar] [CrossRef]
- Park, M.-B. Living with parents who smoke predicts levels of toxicant exposure in children. Sci. Rep. 2020, 10, 11173. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.H.; Na Jang, B.; Kang, S.H.; Joo, J.H.; Park, E.-C. Association between parents’ smoking status and tobacco exposure in school-age children: Assessment using major urine biomarkers. Sci. Rep. 2021, 11, 4536. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Hashemi, S.; Han, W.; Song, Y.; Lim, Y. Exposure and Risk Assessment of Second- and Third-Hand Tobacco Smoke Using Urinary Cotinine Levels in South Korea. Int. J. Environ. Res. Public Health 2022, 19, 3746. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Feng, J.; Sosnoff, C.S.; Bernert, J.T.; Blount, B.C.; Li, Y.; Del Valle-Pinero, A.Y.; Kimmel, H.L.; van Bemmel, D.M.; Rutt, S.M.; Crespo-Barreto, J.; et al. Urinary Nicotine Metabolites and Self-Reported Tobacco Use Among Adults in the Population Assessment of Tabacco and Health (PATH) Study, 2013–2014. Nicotine Tob. Res. 2022, 24, 768–777. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Jacob, P.; Fong, I.; Gupta, S. Nicotine metabolic profile in man: Comparison of cigarette smoking and transdermal nicotine. J. Pharmacol. Exp. Ther. 1994, 68, 296–303. [Google Scholar]
- Tutka, P.; Mosiewicz, J.; Wielosz, M. Pharmacokinetics and metabolism of nicotine. Pharmacol. Rep. 2005, 57, 143–153. [Google Scholar]
- Benowitz, N.L.; Hukkanen, J.; Jacob, P., III. Nicotine chemistry, metabolism, kinetics and biomarkers. Handb. Exp. Pharmacol. 2009, 192, 29–60. [Google Scholar] [CrossRef] [Green Version]
- Hukkanen, J.; Jacob, P., III; Benowitz, N.L. Metabolism and Disposition Kinetics of Nicotine. Pharmacol. Rev. 2005, 57, 79–115. [Google Scholar] [CrossRef] [Green Version]
- Miller, E.I.; Norris, H.K.; Rollins, D.E.; Tiffany, S.T.; Wilkins, D.G. A novel validated procedure for the determination of nicotine, eight nicotine metabolites and two minor tobacco alkaloids in human plasma or urine by solid-phase extraction coupled with liquid chromatography-electrospray ionization-tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2010, 878, 725–737. [Google Scholar] [CrossRef] [Green Version]
- Benowitz, N.L.; Helen, G.S.; Nardone, N.; Cox, L.S.; Jacob, P. Urine Metabolites for Estimating Daily Intake of Nicotine From Cigarette Smoking. Nicotine Tob. Res. 2020, 22, 288–292. [Google Scholar] [CrossRef]
- Imura, Y.; Tabuchi, T. Exposure to Secondhand Heated-Tobacco-Product Aerosol May Cause Similar Incidence of Asthma Attack and Chest Pain to Secondhand Cigarette Exposure: The JASTIS 2019 Study. Int. J. Environ. Res. Public Health 2021, 18, 1766. [Google Scholar] [CrossRef] [PubMed]
- Gravely, S.; Fong, G.T.; Sutanto, E.; Loewen, R.; Ouimet, J.; Xu, S.S.; Quah, A.C.K.; Thompson, M.E.; Boudreau, C.; Li, G.; et al. Perceptions of harmfulness of heated tobacco products compared to combustible cigarettes among adult smokers in Japan: Findings from the 2018 ITC Japan survey. J. Environ. Res. Public Health 2020, 17, 2394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohmomo, H.; Harada, S.; Komaki, S.; Ono, K.; Sutoh, Y.; Otomo, R.; Umekage, S.; Hachiya, T.; Katanoda, K.; Takebayashi, T.; et al. DNA methylation abnormalities and altered whole transcriptome profiles after switching from combustible tobacco smoking to heated tobacco products. Cancer Epidemiol. Biomark. Prev. 2021, 25, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, S.; Noguchi, M.; Takagi, N.; Hayashida, H.; Inaba, Y.; Ogura, H.; Kunugita, N. Simple Determination of Gaseous and Particulate Compounds Generated from Heated Tobacco Products. Chem. Res. Toxicol. 2018, 31, 585–593. [Google Scholar] [CrossRef]
- Simonavicius, E.; McNeill, A.; Shahab, L.; Brose, L.S. Heat-not-burn tobacco products: A systematic literature review. Tob. Control 2018, 28, 582–594. [Google Scholar] [CrossRef]
- St Helen, G.; Jacob Iii, P.; Nardone, N.; Benowitz, N.L. IQOS: Examination of Philip Morris International’s claim of reduced exposure. Tob. Control 2018, 27, s30–s36. [Google Scholar] [CrossRef]
- Suyama, K.; Kozu, R.; Tanaka, T.; Ishimatsu, Y.; Sawai, T. Exposure to environmental tobacco smoke from husband more strongly impacts on the airway obstruction of nonsmoking women. Int. J. Chronic Obstr. Pulm. Dis. 2017, 13, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Parro, J.; Aceituno, P.; Droppelmann, A.; Mesías, S.; Muñoz, C.; Marchetti, N.; Iglesias, V. Secondhand tobacco smoke exposure and pulmonary function: A cross-sectional study among non-smoking employees of bar and restaurants in Santiago, Chile. BMJ Open 2018, 7, e017811. [Google Scholar] [CrossRef]
- Igarashi, A.; Aida, J.; Kusama, T.; Tabuchi, T.; Tsuboya, T.; Sugiyama, K.; Yamamoto, T.; Osaka, K. Heated tobacco products have reached younger or more affluent people in Japan. J. Epidemiol. 2021, 31, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Johansson, A.; Halling, A.; Hermansson, G.; Ludvigsson, A.J. Assessment of smoking behaviors in the home and their influence on children’s passive smoking: Development of a questionnaire. Ann. Epidemiol. 2005, 15, 453–459. [Google Scholar] [CrossRef]
- Wang, L.; Bernert, J.T.; Benowitz, N.L.; Feng, J.; Jacob, P., III; McGahee, E.; Caudill, S.P.; Scherer, G.; Scherer, M.; Pluym, N.; et al. Collaborative Method Performance Study of the Measurement of Nicotine, its Metabolites, and Total Nicotine Equivalents in Human Urine. Cancer Epidemiol. Biomark. Prev. 2018, 27, 1083–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenvbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Pool, C.; Schlesselman, J.; Egger, M. STROBE Initiative. Epidemiology 2007, 18, 805–835. [Google Scholar]


{kind=link}
| (1) “Have you smoked during the time with your spouse?” (yes/no) for the father |
| (2) “Have you smoked during the time with your children?” (yes/no) for the father |
| (3) “Has your husband smoked during the time with you?” (yes/no) for the spouse |
| (4) “Has your father smoked during the time with you?” (yes/no) for the children |
| Definition of SHS exposure |
| For spouses, if the participant answered “yes” in response to questions (1) or (3), their spouses were classified as being exposed to SHS. |
| For children, if the participant answered “yes” in response to questions (2) or (4), their children were classified as being exposed to SHS. |
| SHS Exposure Status from Fathers | |||||
|---|---|---|---|---|---|
| Characteristics | Total Participants (41 Families) | Fathers Who Only Smoke Combustion Cigarettes (9 Families) | Fathers Who Only Use HTPs (22 Families) | Fathers Who Are Never-Smokers and Non-Users (10 Families) | p-Value |
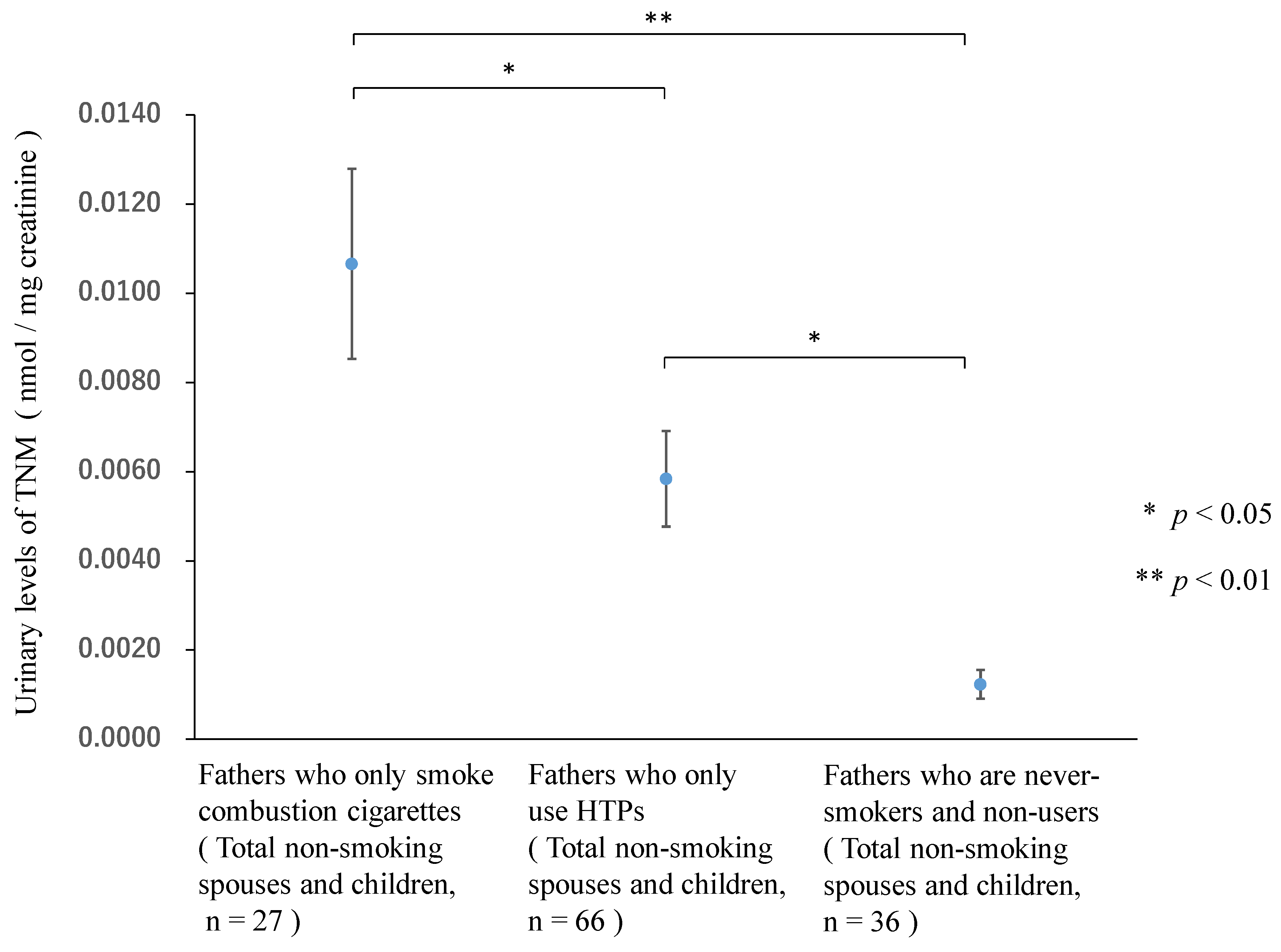
| Total non-smoking spouses and children | n = 129 | n = 27 | n = 66 | n = 36 | |
| Age, years, M (SD) | 18.1 (14.1) | 18.8 (14.5) | 18.3 (14.3) | 17.3 (13.5) | 0.93 |
| Male, n (%) | 43 | 7 | 23 | 13 | |
| Female, n (%) | 86 | 20 | 43 | 23 | 0.28 |
| Non-smoking spouses | n = 41 | n = 9 | n = 22 | n = 10 | |
| Age, years, M (SD) | 37.6 (6.0) | 37.7 (7.5) | 37.5 (6.3) | 37.7 (4.4) | 0.99 |
| Female, n (%) | 41 (100) | 9 (100) | 22(100) | 10 (100) | |
| Non-smoking children | n = 88 | n = 18 | n = 44 | n = 26 | |
| Age, years, M (SD) | 9.1 (4.4) | 9.3 (4.8) | 8.8 (3.9) | 9.4 (4.9) | 0.83 |
| Male, n (%) | 43 (48.9) | 7 (38.9) | 23 (52.3) | 13 (50.0) | |
| Female, n (%) | 45 (51.1) | 11 (61.1) | 21 (47.7) | 13 (50.0) | |
| SHS Exposure Status from Fathers | |||||
|---|---|---|---|---|---|
| Characteristics | Total Participants (41 Families) | Fathers Who Only Smoke Combustion Cigarettes, (9 Families) | Fathers Who Only Use HTPs, (22 Families) | Fathers Who Are Never-Smokers and Non-Users, (10 Families) | p-Value |
| Total non-smoking spouses and children TNM, nmol/mg creatinine, M (SE) | n = 129 | n = 27 | n = 66 | n = 36 | |
| 0.0107 (0.0021) ** | 0.0058 (0.0011) * | 0.0012 (0.0003) | <0.001 | ||
| SHS exposure, Yes | n = 15 | n = 49 | n = 0 | ||
| 0.0107 (0.0025) ** | 0.0063 (0.0014) * | <0.001 | |||
| SHS exposure, No | n = 12 | n = 17 | n = 36 | ||
| 0.0106 (0.0038) ** | 0.0045 (0.0015) | 0.0012 (0.0003) | <0.001 | ||
| Non-smoking spouses TNM, nmol/mg creatinine, M (SE) | n = 41 | n = 9 | n = 22 | n = 10 | |
| 0.0083 (0.0035) * | 0.0027 (0.0005) | 0.0010 (0.0004) | 0.01 | ||
| SHS exposure, Yes | n = 6 | n = 19 | n = 0 | ||
| 0.0087 (0.0052) * | 0.0029 (0.0006) | 0.028 | |||
| SHS exposure, No | n = 3 | n = 3 | n = 10 | ||
| 0.0074 (0.0034) ** | 0.0018 (0.0009) | 0.0010 (0.0004) | 0.008 | ||
| Non-smoking children TNM, nmol/mg creatinine, M (SE) | n = 88 | n = 18 | n = 44 | n = 26 | |
| 0.0119 (0.0027) ** | 0.0074 (0.0015) * | 0.0013 (0.0004) | <0.001 | ||
| SHS exposure, Yes | n = 9 | n = 30 | n = 0 | ||
| 0.0121 (0.0024) ** | 0.0084 (0.0021) * | 0.001 | |||
| SHS exposure, No | n = 9 | n = 14 | n = 26 | ||
| 0.0116 (0.0050) ** | 0.0051 (0.0017) | 0.0013 (0.0004) | 0.003 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onoue, A.; Inaba, Y.; Machida, K.; Samukawa, T.; Inoue, H.; Kurosawa, H.; Ogata, H.; Kunugita, N.; Omori, H. Association between Fathers’ Use of Heated Tobacco Products and Urinary Cotinine Concentrations in Their Spouses and Children. Int. J. Environ. Res. Public Health 2022, 19, 6275. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106275
Onoue A, Inaba Y, Machida K, Samukawa T, Inoue H, Kurosawa H, Ogata H, Kunugita N, Omori H. Association between Fathers’ Use of Heated Tobacco Products and Urinary Cotinine Concentrations in Their Spouses and Children. International Journal of Environmental Research and Public Health. 2022; 19(10):6275. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106275
Chicago/Turabian StyleOnoue, Ayumi, Yohei Inaba, Kentaro Machida, Takuya Samukawa, Hiromasa Inoue, Hajime Kurosawa, Hiromitsu Ogata, Naoki Kunugita, and Hisamitsu Omori. 2022. "Association between Fathers’ Use of Heated Tobacco Products and Urinary Cotinine Concentrations in Their Spouses and Children" International Journal of Environmental Research and Public Health 19, no. 10: 6275. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106275