
Dietary Factors Influencing the Caries Status of Adults in Karachi, Pakistan: Initial Findings

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Settings and Participants
2.3. Study Questionnaire
2.4. Food Frequency Questionnaire (FFQ)
2.5. Dental Caries Examination
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- MacHiulskiene, V.; Campus, G.; Carvalho, J.C.; Dige, I.; Ekstrand, K.R.; Jablonski-Momeni, A.; Maltz, M.; Manton, D.J.; Martignon, S.; Martinez-Mier, E.A.; et al. Terminology of Dental Caries and Dental Caries Management: Consensus Report of a Workshop Organized by ORCA and Cariology Research Group of IADR. Caries Res. 2020, 54, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar] [PubMed]
- Sheiham, A.; James, W.P.T. Diet and dental caries: The pivotal role of free sugars reemphasized. J. Dent. Res. 2015, 94, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.; Worthington, H.V.; Glenny, A.-M.; Appelbe, P.; Marinho, V.C.; Shi, X. Fluoride toothpastes of different concentrations for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Malik, A.; Qureshi, A.; Shaukat, M.S. Prevention of Dental Decay: Role of Fluoride in Dentifrices. J. Dow Univ. Health Sci. 2013, 7, 59–62. [Google Scholar]
- Tahir, M.A.; Rasheed, H. Fluoride in the drinking water of Pakistan and the possible risk of crippling fluorosis. Drink Water Eng. Sci. 2013, 6, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Dhingra, S.; Gupta, A.; Tandon, S.; Marya, C.M. Sugar clock: A primordial approach to prevent dental caries. Int. J. Clin. Pediatr. Dent. 2020, 13, 174–175. [Google Scholar]
- Marshall, T.A.; Broffitt, B.; Eichenberger-Gilmore, J.; Warren, J.J.; Cunningham, M.A.; Levy, S.M. The roles of meal, snack, and daily total food and beverage exposures on caries experience in young children. J. Public Health Dent. 2005, 65, 166–173. [Google Scholar] [CrossRef]
- Khan, A.A.; Sharea, I.; Ayma, S.; Ambreena, Q.; Inayatullah, P.; Sofia, S. Oral health in Pakistan: A situation analysis. Dev. Dent. 2004, 5, 35–44. [Google Scholar]
- Taqi, M.; Abdul Razzak, I.; Ab-Murat, N. Sugar consumption and caries occurrence among Pakistani school children. J. Pak. Med. Assoc. 2018, 68, 1483–1487. [Google Scholar]
- Dawani, N.; Nisar, N.; Khan, N.; Syed, S.; Tanweer, N. Prevalence and factors related to dental caries among pre-school children of Saddar town, Karachi Pakistan: A cross-sectional study. BMC Oral Health 2012, 12, 59. [Google Scholar] [CrossRef] [Green Version]
- Te Morenga, L.; Mallard, S.; Mann, J. Dietary sugars and body weight: Systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 2013, 346, e7492. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.; Gupta, N.; Singh, H.P. Prevalence of Dental Caries in relation to Body Mass Index, Daily Sugar Intake, and Oral Hygiene Status in 12-Year-Old School Children in Mathura City: A Pilot Study. Int. J. Pediatr. 2014, 2014, 921823. [Google Scholar] [CrossRef] [PubMed]
- Evans, E.W.; Hayes, C.; Palmer, C.A.; Bermudez, O.I.; Cohen, S.A.; Must, A. Dietary intake and severe early childhood caries in low-income, young children. J. Acad. Nutr. Diet 2013, 113, 1057–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazik, M.N.; Malde, M.K.; Ahmed, M.F.; Trovik, T.A. Correlation between caries experience in Sudanese school children and dietary habits, according to a food frequency questionnaire and a modified 24-hr recall method. Afr. J. Food Agric. Nutr. 2013, 13, 7624–7639. [Google Scholar] [CrossRef]
- Johansson, I.; Lif Holgerson, P.; Kressin, N.R.; Nunn, M.E.; Tanner, A.C. Snacking habits and caries in young children. Caries Res. 2010, 44, 421–430. [Google Scholar] [CrossRef] [Green Version]
- Perera, I.; Ekanayake, L. Relationship between dietary patterns and dental caries in Sri Lankan adolescents. Oral Health Prev. Dent. 2010, 8, 165–172. [Google Scholar] [CrossRef]
- Heller, K.E.; Burt, B.A.; Eklund, S.A. Sugared soda consumption and dental caries in the United States. J. Dent. Res. 2001, 80, 1949–1953. [Google Scholar] [CrossRef]
- Burt, B.A.; Kolker, J.L.; Sandretto, A.M.; Yuan, Y.; Sohn, W.; Ismail, A.I. Dietary patterns related to caries in a low-income adult population. Caries Res. 2006, 40, 473–480. [Google Scholar] [CrossRef] [Green Version]
- Shinga-Ishihara, C.; Nakai1, Y.; Milgrom, P.; Murakami, K.; Matsumoto-Nakano, M. Cross-cultural validity of a dietary questionnaire for studies of dental caries risk in Japanese. BMC Oral Health 2014, 14, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anzar, W.; Qureshi, A.; Afaq, A.; Kattan, H.F.; Almutairi, B.; Alzahrani, K.M.; Naseem, M.; Vohra, F.; Abduljabbar, T. Association of Dental Caries and Anthropometric Measures among Primary School Children. Children 2021, 8, 223. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.H. Sugars and dental caries. Isr. J. Dent. Sci. 1991, 2, 183–191. [Google Scholar]
- The World Health Organization. The World Oral Health Report 2020; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 20 September 2021).
- LoDolce, M.E.; Harris, J.L.; Schwartz, M.B. Sugar as part of a balanced breakfast? What cereal advertisements teach children about healthy eating. J. Health Commun. 2013, 18, 1293–1309. [Google Scholar] [CrossRef]
- Theurich, M.A.; Koletzko, B.; Grote, V. Nutritional adequacy of commercial complementary cereals in Germany. Nutrients 2020, 12, 1590. [Google Scholar] [CrossRef] [PubMed]
- Williamson, C.S. Breakfast cereals—Why all the bad press? Facts behind the headlines. Nutr. Bull. 2010, 35, 30–33. [Google Scholar] [CrossRef]
- López, R.; Smith, P.C.; Göstemeyer, G.; Schwendicke, F. Ageing, dental caries and periodontal diseases. J. Clin. Periodontol. 2017, 44, S145–S152. [Google Scholar] [CrossRef] [Green Version]
- Bernabé, E.; Sheiham, A. Age, period and cohort trends in caries of permanent teeth in four developed countries. Am. J. Public Health 2014, 104, e115–e121. [Google Scholar] [CrossRef]
- Lukacs, J.R.; Largaespada, L.L. Explaining sex differences in dental caries prevalence: Saliva, hormones, and “life-history” etiologies. Am. J. Hum. Biol. 2006, 18, 540–555. [Google Scholar] [CrossRef] [PubMed]
- Barrington, G.; Khan, S.; Kent, K.; Brennan, D.S.; Crocombe, L.A.; Bettiol, S. Obesity, dietary sugar and dental caries in Australian adults. Int. Dent. J. 2019, 69, 383–391. [Google Scholar] [CrossRef]
- Abbass, M.M.S.; AbuBakr, N.; Radwan, I.A. The potential impact of age, gender, body mass index, socioeconomic status and dietary habits on the prevalence of dental caries among Egyptian adults: A cross-sectional study. F1000Research 2019, 8, 243. [Google Scholar] [CrossRef] [Green Version]
- Watts, A.W.; Mason, S.M.; Loth, K.; Larson, N.; Neumark-Sztainer, D. Socioeconomic differences in overweight and weight-related behaviors across adolescence and young adulthood: 10-year longitudinal findings from Project EAT. Prev. Med. 2016, 87, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Shivakumar, S.; Srivastava, A.; Shivakumar, G.C. Body Mass Index and Dental Caries: Systematic Review. Int. J. Clin. Pediatric Dent. 2018, 11, 228–232. [Google Scholar]
- Holst, D.; Schuller, A.A.; Aleksejuniene, J.; Eriksen, H.M. Caries in populations—A theoretical, causal approach. Eur. J. Oral Sci. 2001, 109, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.; Manohar, B.M. Consumers’ behavior towards ready-to-eat breakfast cereals: A review and future research agenda. Educ. Psychol. 2021, 58, 656–678. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Mean ± SD/N (Percentage) | ||
|---|---|---|---|
| Age | 32.65 ± 10.49 | ||
| Gender | Male | 796 (46.12) | |
| Female | 934 (54.37) | ||
| Marital status | Single | 779 (45.43) | |
| Married | 951 (52.08) | ||
| BMI (kg/m2) | <18 | 467 (27.77) | |
| 18–22.9 | 916 (53.50) | ||
| 23–<25 | 260 (15.20) | ||
| ≥25 | 87 (5.46) | ||
| No. of children | 2 ± 1.83 | ||
| Frequency of brushing | Once daily | 495 (28.61) | |
| Twice daily | 1165 (67.34) | ||
| No brush | 70 (4.04) | ||
| Dental visits | 6 months | 240 (13.87) | |
| 12 months | 1389 (80.28) | ||
| >24 months | 101 (5.83) | ||
| Fluoride level in toothpastes (as claimed by the manufacturer) | <1100 ppm | 498 (28.78) | |
| ≥1100 ppm | 1232 (71.21) | ||
| Mean DMFT | 5.74 ± 1.86 | ||
| Mean D | 3.29 ± 1.09 | ||
| Mean F | 0.76 ± 0.56 | ||
| Mean M | 1.67 ± 1.47 | ||
| Food Items | Food Patterns | |||
|---|---|---|---|---|
| Sweet Treat | Tea Meal | Cereal | Dairy and Nut | |
| Candies (all kinds) | 0.7153 | 0.1789 | −0.1170 | −0.0708 |
| Ice cream or sherbet * | 0.5628 | −0.0471 | 0.0792 | −0.0510 |
| Bread filled with jam/fruit jam | −0.0468 | 0.8515 | 0.0733 | −0.0397 |
| Jam or jelly | 0.2364 | 0.8179 | 0.1217 | −0.0367 |
| Sugared cereal | 0.0102 | 0.1907 | 0.7211 | 0.1112 |
| Plain cereal | 0.0092 | −0.0286 | 0.6416 | 0.1587 |
| Dried fruit | 0.0449 | −0.0843 | 0.0785 | 0.6154 |
| Plain yogurt | 0.0785 | −0.1501 | 0.0824 | 0.5812 |
| Cold drinks | 0.5049 | 0.0038 | −0.1480 | −0.0525 |
| Cookies or biscuits | 0.4897 | 0.1028 | 0.3547 | 0.0949 |
| Cakes, donuts, or pies | 0.3678 | −0.1729 | 0.1916 | 0.2512 |
| Bread | −0.0660 | 0.4732 | 0.0598 | 0.3916 |
| Sugared yogurt | −0.1064 | 0.0034 | −0.0251 | 0.5295 |
| Rice | 0.2271 | −0.0967 | 0.1623 | 0.0822 |
| Cheese | 0.4555 | 0.0992 | −0.0385 | 0.0726 |
| Fresh fruit with sugar | 0.1954 | 0.0630 | 0.4156 | 0.0840 |
| Banana | −0.0684 | 0.0901 | 0.1523 | 0.4869 |
| Milk | −0.1010 | 0.1354 | −0.2002 | 0.1446 |
| Fruit juice | 0.3753 | 0.1231 | −0.0055 | 0.0401 |
| Sugar/honey in coffee/tea | 0.1293 | 0.2069 | 0.0647 | 0.0606 |
| Pudding or custard | −0.0381 | 0.2205 | 0.4144 | −0.0663 |
| Chocolates | −0.0381 | 0.2205 | 0.4144 | −0.0663 |
| Chips | 0.2763 | −0.3143 | −0.5476 | 0.2776 |
| Popcorn | −0.0272 | 0.2020 | −0.0454 | 0.3237 |
| Mithai (sweetmeat) | 0.3505 | −0.0041 | 0.0622 | 0.2026 |
| Variables | Prevalence (%) | Crude OR (95% CI) | p-Value | Adjusted OR (95% CI) ǂ | p-Value |
|---|---|---|---|---|---|
| Age | -- | 1.06 (1.02–1.09) | 0.001 * | 1.06 (0.997–1.146) | 0.060 |
| Gender | |||||
| Male | 279/796 (35%) | Reference | Reference | ||
| Female | 607/934 (65%) | 3.42 (1.48–7.89) | 0.004 * | 2.81 (0.968–8.170) | 0.057 |
| Marital Status | |||||
| Single | 296/779 (38%) | Reference | Reference | ||
| Married | 589/951 (62%) | 2.86 (1.25–6.53) | 0.013 * | 0.52 (0.0977–2.781) | 0.446 |
| BMI | -- | 1.01 (0.92–1.11) | 0.764 | 1.0 (0.8–1.12) | 0.65 |
| Frequency of Brushing | |||||
| Once daily | 495 (28) | Reference | Reference | ||
| Twice daily | 1165 (67) | 0.3 (0.2–1.9) | 0.81 | 0.2 (0.1–2.1) | 0.71 |
| No Brushing | 70 (5) | 1.1 (0.2–1.2) | 0.62 | 1.2 (0.1–1.5) | 0.51 |
| Dental Visits | |||||
| 6 months | 240 (13) | Reference | Reference | ||
| 12 months | 1389 (80) | 0.1 (0.1–1.7) | 0.56 | 0.1 (0.1–1.5) | 0.52 |
| >24 months | 101 (7) | 0.02 (0.01–1.1) | 0.73 | 0.01 (0.01–1.3) | 0.7 |
| Fluoride in Toothpastes † | |||||
| <1100 PPM | 219/498 (44%) | Reference | Reference | ||
| ≥1100 PPM | 677/1232 (55%) | 1.54 (0.60–3.93) | 0.361 | 1.55 (0.61–3.89) | 0.25 |
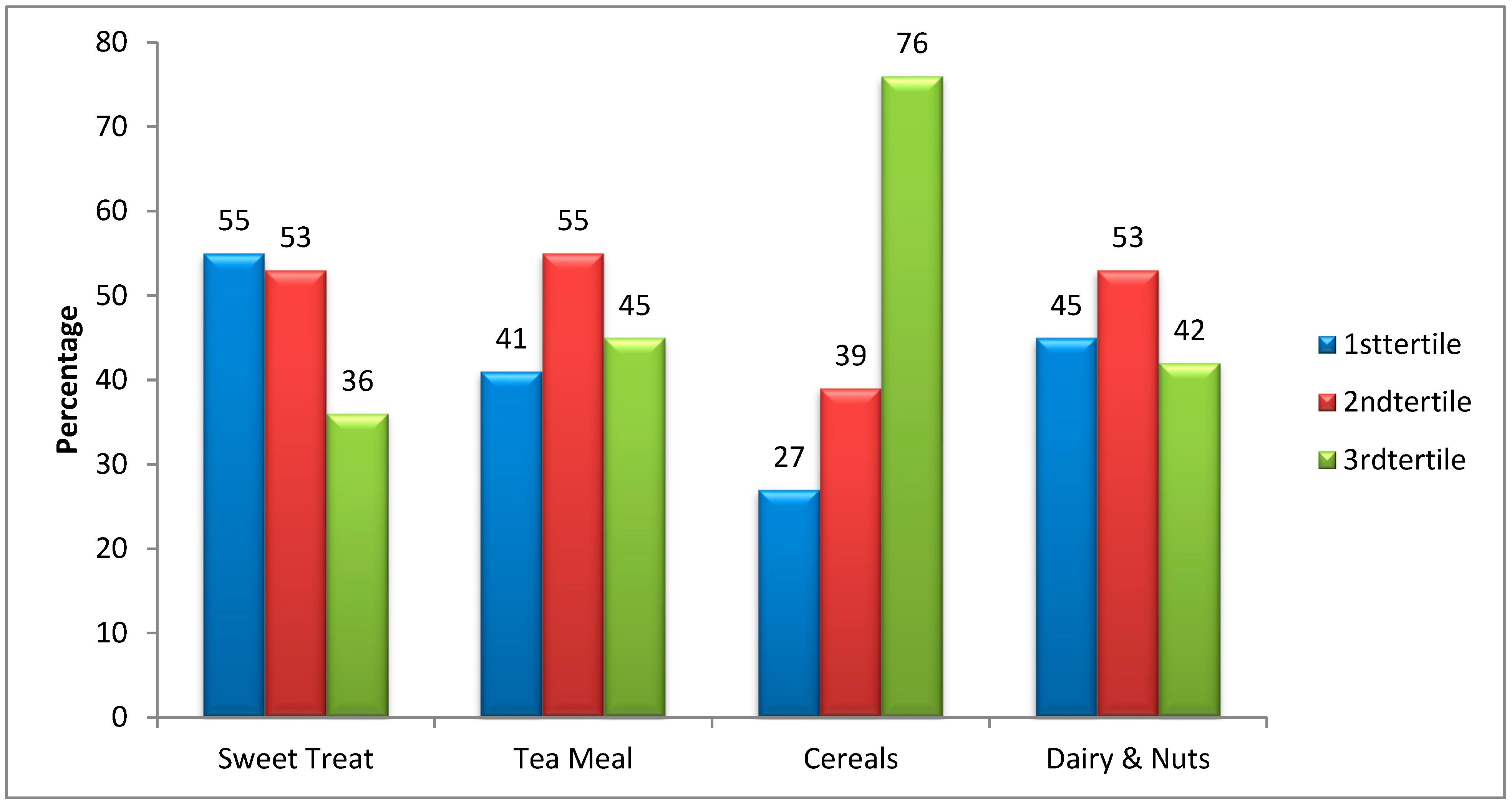
| Sweet Treat | |||||
| 1st tertile | 317/577(55%) | Reference | Reference | ||
| 2nd tertile | 305/577 (53%) | 0.85 (0.28–2.54) | 0.78 | 0.83 (0.28–2.34) | 0.68 |
| 3rd tertile | 207/576 (36%) | 0.53 (0.17–1.61) | 0.26 | 0.55 (0.16–1.78) | 0.25 |
| Tea Meal | |||||
| 1st tertile | 236/577 (41%) | Reference | Reference | ||
| 2nd tertile | 317/577 (55%) | 1.59 (0.53–4.75) | 0.406 | 1.60 (0.52–0.48) | 0.39 |
| 3rd tertile | 259/576 (45%) | 1.16 (0.39–3.49) | 0.780 | 1.18 (0.33–3.44) | 0.66 |
| Cereals | |||||
| 1st tertile | 155/577 (27%) | Reference | Reference | ||
| 2nd tertile | 225/577 (39%) | 1.69 (0.52–5.48) | 0.377 | 1.17 (0.322–4.310) | 0.803 |
| 3rd tertile | 437/576 (76%) | 9.04 (2.57–31.84) | 0.001 * | 4.36 (1.024–18.599) | 0.046 * |
| Dairy and Nuts | |||||
| 1st tertile | 259/577 (45%) | Reference | Reference | ||
| 2nd tertile | 305/577 (53%) | 1.36 (0.45–4.05) | 0.579 | 1.33 (0.41–3.39) | 0.55 |
| 3rd tertile | 241/576 (42%) | 0.85 (0.28–2.55) | 0.780 | 0.83 (0.28–2.33) | 0.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qureshi, A.; Safdar, N.F.; Qureshi, H.; AlFawaz, Y.F.; Al Ahdal, K.; Shabib, S.; Al-Aali, K.A.; Naseem, M.; Vohra, F.; Abduljabbar, T. Dietary Factors Influencing the Caries Status of Adults in Karachi, Pakistan: Initial Findings. Int. J. Environ. Res. Public Health 2022, 19, 6980. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19126980
Qureshi A, Safdar NF, Qureshi H, AlFawaz YF, Al Ahdal K, Shabib S, Al-Aali KA, Naseem M, Vohra F, Abduljabbar T. Dietary Factors Influencing the Caries Status of Adults in Karachi, Pakistan: Initial Findings. International Journal of Environmental Research and Public Health. 2022; 19(12):6980. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19126980
Chicago/Turabian StyleQureshi, Ambrina, Nilofer F. Safdar, Hina Qureshi, Yasser F. AlFawaz, Khold Al Ahdal, Sara Shabib, Khulud A. Al-Aali, Mustafa Naseem, Fahim Vohra, and Tariq Abduljabbar. 2022. "Dietary Factors Influencing the Caries Status of Adults in Karachi, Pakistan: Initial Findings" International Journal of Environmental Research and Public Health 19, no. 12: 6980. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19126980