
Assessing Fluorosis Incidence in Areas with Low Fluoride Content in the Drinking Water, Fluorotic Enamel Architecture, and Composition Alterations

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population Study
2.2. Qualification for the Study
2.3. In Vitro Analysis of Extracted Human Teeth
2.3.1. A Quantitative Analysis of Total Protein Content in Tooth Enamel
2.3.2. Determination of Fluoride Content in Tooth Enamel
2.3.3. Scanning Electron Microscopy (SEM)
2.4. Statistical Analysis
2.4.1. Sample Size Calculation
2.4.2. Experimental Groups Comparison
3. Results
3.1. Findings of the Population Study
3.2. In Vitro Studies of Extracted Teeth Enamel
3.2.1. Quantitative Analysis of Total Protein in Tooth Enamel
3.2.2. Fluoride Content in Tooth Enamel
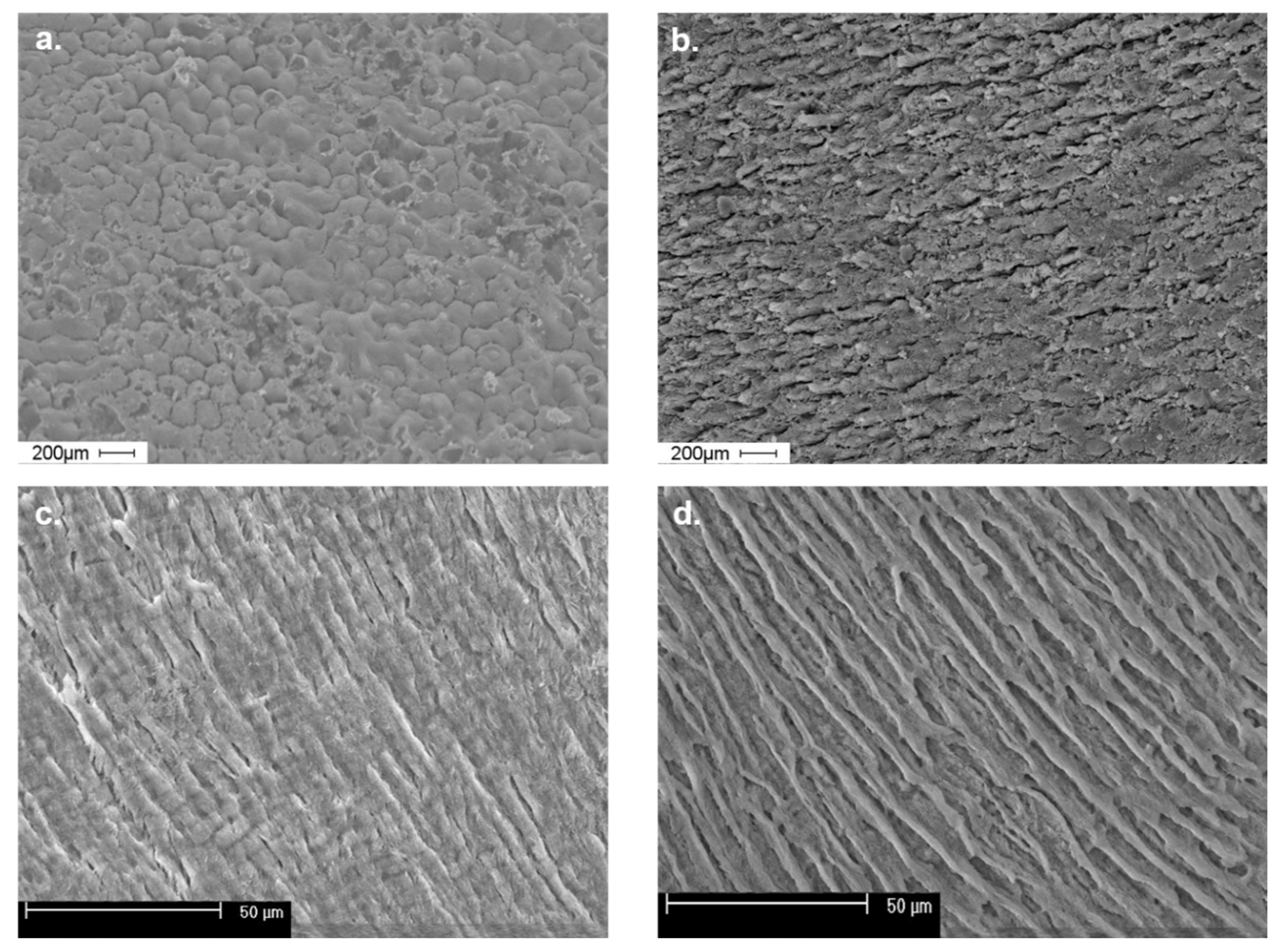
3.2.3. Findings of the SEM Examination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Commission Directorate General for Health and Consumers. Critical Review of Any New Evidence on the Hazard Profile, Health Effects, and Human Exposure to Fluoride and the Fluoridating Agents of Drinking Water; Publications Office: Luxemburg, 2010. [Google Scholar]
- O’Mullane, D.M.; Baez, R.J.; Jones, S.; Lennon, M.A.; Petersen, P.E.; Rugg-Gunn, A.J.; Whelton, H.; Whitford, G.M. Fluoride and Oral Health. Community Dent. Health 2016, 33, 69–99. [Google Scholar]
- Kerdoun, M.A.; Bouaziz, H.; Adjaine, O.E.K.; Mekhloufi, S.; Bechki, Z.; Belkhalfa, H. Fluoride Concentration in Bottled Drinking Water from a Fluoride Endemic Area: A Market-Based Survey. Clin. Nutr. ESPEN 2021, 46, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Ciosek, Ż.; Kot, K.; Kosik-Bogacka, D.; Łanocha-Arendarczyk, N.; Rotter, I. The Effects of Calcium, Magnesium, Phosphorus, Fluoride, and Lead on Bone Tissue. Biomolecules 2021, 11, 506. [Google Scholar] [CrossRef] [PubMed]
- Cossellu, G.; Lanteri, V.; Butera, A.; Laffi, N.; Merlini, A.; Farronato, G. Timing Considerations on the Shear Bond Strength of Orthodontic Brackets after Topical Fluoride Varnish Applications. J. Orthodont. Sci. 2017, 6, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M. Fluoride and bone metabolism. Clin. Calcium 2007, 17, 217–223. [Google Scholar]
- Solanki, Y.S.; Agarwal, M.; Gupta, A.B.; Gupta, S.; Shukla, P. Fluoride Occurrences, Health Problems, Detection, and Remediation Methods for Drinking Water: A Comprehensive Review. Sci. Total Environ. 2022, 807, 150601. [Google Scholar] [CrossRef]
- Petersen, P.E.; Ogawa, H. Prevention of Dental Caries through the Use of Fluoride—The WHO Approach. Community Dent. Health 2016, 33, 66–68. [Google Scholar]
- Deciphering the Interaction of a Macrocyclic Tetranuclear Zn(II) Complex with Biomimicking Surfactant: A Case Study Using Cetyltrimethylammonium Bromide. Biointerface Res. Appl. Chem. 2021, 12, 2462–2472. [CrossRef]
- Nor, N.A.M.; Chadwick, B.L.; Farnell, D.J.; Chestnutt, I.G. The Impact of Stopping or Reducing the Level of Fluoride in Public Water Supplies on Dental Fluorosis: A Systematic Review. Rev. Environ. Health 2020, 35, 419–426. [Google Scholar]
- Sunkari, E.D.; Adams, S.J.; Okyere, M.B.; Bhattacharya, P. Groundwater Fluoride Contamination in Ghana and the Associated Human Health Risks: Any Sustainable Mitigation Measures to Curtail the Long Term Hazards? Groundw. Sustain. Dev. 2022, 16, 100715. [Google Scholar] [CrossRef]
- Keesari, T.; Pant, D.; Roy, A.; Sinha, U.K.; Jaryal, A.; Singh, M.; Jain, S.K. Fluoride Geochemistry and Exposure Risk through Groundwater Sources in Northeastern Parts of Rajasthan, India. Arch. Environ. Contam. Toxicol. 2021, 80, 294–307. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Kiss, L.; Mei, H.; Remete, A.M.; Ponikvar-Svet, M.; Sedgwick, D.M.; Roman, R.; Fustero, S.; Moriwaki, H.; Soloshonok, V.A. Chemical Aspects of Human and Environmental Overload with Fluorine. Chem. Rev. 2021, 121, 4678–4742. [Google Scholar] [CrossRef] [PubMed]
- Rajendiran, M.; Trivedi, H.M.; Chen, D.; Gajendrareddy, P.; Chen, L. Recent Development of Active Ingredients in Mouthwashes and Toothpastes for Periodontal Diseases. Molecules 2021, 26, 2001. [Google Scholar] [CrossRef] [PubMed]
- Kumaran, B.; Watson, T. Thermal Build-up, Decay and Retention Responses to Local Therapeutic Application of 448 KHz Capacitive Resistive Monopolar Radiofrequency: A Prospective Randomised Crossover Study in Healthy Adults. Int. J. Hyperth. 2015, 31, 883–895. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.-G.; Kang, L.; Wu, G. Fluorosis Increases the Risk of Postmenopausal Osteoporosis by Stimulating Interferon γ. Biochem. Biophys. Res. Commun. 2016, 479, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Guo, X.; Sun, Q.; Shan, Z.; Teng, W. Effects of Excess Fluoride and Iodide on Thyroid Function and Morphology. Biol. Trace Elem. Res. 2016, 170, 382–389. [Google Scholar] [CrossRef]
- Nagendra, A.H.; Bose, B.; Shenoy, P.S. Recent Advances in Cellular Effects of Fluoride: An Update on Its Signalling Pathway and Targeted Therapeutic Approaches. Mol. Biol. Rep. 2021, 48, 5661–5673. [Google Scholar] [CrossRef]
- Dean, H.T. Classification of Mottled Enamel Diagnosis. J. Am. Dent. Assoc. (1922) 1934, 21, 1421–1426. [Google Scholar] [CrossRef]
- Wright, J.T.; Chen, S.C.; Hall, K.I.; Yamauchi, M.; Bawden, J.W. Protein Characterization of Fluorosed Human Enamel. J. Dent. Res. 1996, 75, 1936–1941. [Google Scholar] [CrossRef]
- Hubbard, M.J.; Perez, V.A.; Ganss, B. 100 Years of Chalky Teeth Research: From Pioneering Histopathology to Social Good. Front. Dent. Med. 2021, 1, 25. [Google Scholar] [CrossRef]
- Kim, S.J. Structural Characterization and Amelotin-Mediated Mineralization of Enamel Lesions in Molar-Incisor Hypomineralization. Ph.D. Thesis, University of Toronto, Toronto, ON, Canada, 2021. [Google Scholar]
- Suckling, G.W.; Nelson, D.G.; Patel, M.J. Macroscopic and Scanning Electron Microscopic Appearance and Hardness Values of Developmental Defects in Human Permanent Tooth Enamel. Adv. Dent. Res. 1989, 3, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Społeczeństwo|Wielkopolskie Regionalne Obserwatorium Terytorialne. Available online: https://wrot.umww.pl/kapital-ludzki-i-spoleczny/ (accessed on 2 June 2022).
- Kalkulator Doboru Próby. Available online: https://www.naukowiec.org/dobor.html (accessed on 19 April 2022).
- Social Science Statistics. Available online: https://www.socscistatistics.com/ (accessed on 31 May 2022).
- Yonezawa, D.; Yagi, M. Effect of a School-Based Fluoride Mouth-Rinsing Programme on Dental Caries. Int. Dent. J. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi, F.; Mahvi, A.H.; Hosseini, M.; Nedjat, S.; Nodehi, R.N.; Kharazifard, M.J.; Parvizishad, M.; Cheraghi, Z. The Prevalence of Dental Fluorosis and Exposure to Fluoride in Drinking Water: A Systematic Review. J. Dent. Res. Dent. Clin. Dent. Prospects 2016, 10, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Koh, D.-C.; Chae, G.-T.; Kee, W.-S.; Ko, K.-S. Integrated Assessment of Major Element Geochemistry and Geological Setting of Traditional Natural Mineral Water Sources in South Korea at the National Scale. J. Hydrol. 2021, 598, 126249. [Google Scholar] [CrossRef]
- Gebretsadik, H.G. Prevalence of Dental Fluorosis among 12–15 Years Old School Children in Zeway, Oromia Region, Ethiopia. Orapuh J. 2021, 2, e823. [Google Scholar]
- Ferreira, M.L.G.; Cury, J.A.; Machado, C.P.; Tabchoury, T.H.U.; Fujimaki, M. Assessment of Public Water Supply Fluoridation of the 15th Regional Health of Paraná. R. Saúde Públ. Paraná 2021, 4, 53–66. [Google Scholar] [CrossRef]
- Cabral, R.N.; Leal, S.C.; de Bernardino, Í.M.; Soviero, V.L.V.M.; Nyvad, B. Caries Lesion Transition Patterns of Schoolchildren in a Fluoridated Community in Brazil. Clin. Oral Investig. 2022, 26, 689–695. [Google Scholar] [CrossRef]
- Stephen, K.W.; Macpherson, L.M.D.; Gilmour, W.H.; Stuart, R.A.M.; Merrett, M.C.W. A Blind Caries and Fluorosis Prevalence Study of School-Children in Naturally Fluoridated and Nonfluoridated Townships of Morayshire, Scotland. Community Dent. Oral Epidemiol. 2002, 30, 70–79. [Google Scholar] [CrossRef]
- Wang, N.J.; Gropen, A.M.; Ogaard, B. Risk Factors Associated with Fluorosis in a Non-Fluoridated Population in Norway. Community Dent. Oral Epidemiol. 1997, 25, 396–401. [Google Scholar] [CrossRef]
- Thomas, N.; Kay, E.; Witton, R.; Quinn, C. Comparison of a Full Arch Digital Photographic Assessment of Caries Prevalence in 5-Year-Old Children to an Established Visual Assessment Method: A Cross-Sectional Study. BDJ Open 2021, 7, 32. [Google Scholar] [CrossRef]
- Habiyakare, T.; Schurer, J.M.; Poole, B.; Murcott, S.; Migabo, B.; Mardochee, B.; Amuguni, J.H.; Morgan, J.P. Dental Fluorosis among People and Livestock Living on Gihaya Island in Lake Kivu, Rwanda. One Health Outlook 2021, 3, 23. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A.; James, W.P.T. Diet and Dental Caries: The Pivotal Role of Free Sugars Reemphasized. J. Dent. Res. 2015, 94, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Tabari, E.D.; Ellwood, R.; Rugg-Gunn, A.J.; Evans, D.J.; Davies, R.M. Dental Fluorosis in Permanent Incisor Teeth in Relation to Water Fluoridation, Social Deprivation and Toothpaste Use in Infancy. Br. Dent. J. 2000, 189, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Bowen, W.H. Fluorosis: Is It Really a Problem? J. Am. Dent. Assoc. 2002, 133, 1405–1407. [Google Scholar] [CrossRef] [PubMed]
- Ruan, J.P.; Bårdsen, A.; Astrøm, A.N.; Huang, R.Z.; Wang, Z.L.; Bjorvatn, K. Dental Fluorosis in Children in Areas with Fluoride-Polluted Air, High-Fluoride Water, and Low-Fluoride Water as Well as Low-Fluoride Air: A Study of Deciduous and Permanent Teeth in the Shaanxi Province, China. Acta Odontol. Scand. 2007, 65, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Machiulskiene, V.; Baelum, V.; Fejerskov, O.; Nyvad, B. Prevalence and Extent of Dental Caries, Dental Fluorosis, and Developmental Enamel Defects in Lithuanian Teenage Populations with Different Fluoride Exposures. Eur. J. Oral Sci. 2009, 117, 154–160. [Google Scholar] [CrossRef]
- Indermitte, E.; Saava, A.; Karro, E. Reducing Exposure to High Fluoride Drinking Water in Estonia-a Countrywide Study. Int. J. Environ. Res. Public Health 2014, 11, 3132–3142. [Google Scholar] [CrossRef]
- Waugh, D.T.; Potter, W.; Limeback, H.; Godfrey, M. Risk Assessment of Fluoride Intake from Tea in the Republic of Ireland and Its Implications for Public Health and Water Fluoridation. Int. J. Environ. Res. Public Health 2016, 13, 259. [Google Scholar] [CrossRef]
- Ha, D.H.; Spencer, A.J.; Moynihan, P.; Thomson, W.M.; Do, L.G. Excess Risk of Dental Caries from Higher Free Sugars Intake Combined with Low Exposure to Water Fluoridation. J. Dent. Res. 2021, 100, 1243–1250. [Google Scholar] [CrossRef]
- Stangvaltaite-Mouhat, L.; Puriene, A.; Stankeviciene, I.; Aleksejūnienė, J. Fluoride in the Drinking Water and Dental Caries Experience by Tooth Surface Susceptibility among Adults. BMC Oral Health 2021, 21, 234. [Google Scholar] [CrossRef]
- Jairoun, A.A.; Al-Hemyari, S.S.; Shahwan, M.; Jairoun, O.; Zyoud, S.H. Analysis of Fluoride Concentration in Toothpastes in the United Arab Emirates: Closing the Gap between Local Regulation and Practice. Cosmetics 2021, 8, 113. [Google Scholar] [CrossRef]
- Ha, D.H.; Crocombe, L.A.; Khan, S.; Do, L.G. The Impact of Different Determinants on the Dental Caries Experience of Children Living in Australia Rural and Urban Areas. Community Dent. Oral Epidemiol. 2021, 49, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Haider, A.; Khadatkar, P.; Suresh, S.; Arisutha, S.; Verma, S. Fluorides-Foundation for Healthy Teeth: A Dental Perspectives. J. Sol-Gel Sci. Technol. 2021, 100, 375–387. [Google Scholar] [CrossRef]
- Momeni, A.; Neuhäuser, A.; Renner, N.; Heinzel-Gutenbrunner, M.; Abou-Fidah, J.; Rasch, K.; Kröplin, M.; Fejerskov, O.; Pieper, K. Prevalence of Dental Fluorosis in German Schoolchildren in Areas with Different Preventive Programmes. Caries Res. 2007, 41, 437–444. [Google Scholar] [CrossRef]
- Paiva, S.M.; Lima, Y.B.O.; Cury, J.A. Fluoride Intake by Brazilian Children from Two Communities with Fluoridated Water. Community Dent. Oral Epidemiol. 2003, 31, 184–191. [Google Scholar] [CrossRef]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental Caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Gallo, S.; Lelli, M.; Tarterini, F.; Giglia, F.; Scribante, A. SEM/EDS Evaluation of the Mineral Deposition on a Polymeric Composite Resin of a Toothpaste Containing Biomimetic Zn-Carbonate Hydroxyapatite (MicroRepair®) in Oral Environment: A Randomized Clinical Trial. Polymers 2021, 13, 2740. [Google Scholar] [CrossRef]
- Saldarriaga, A.; Rojas-Gualdrón, D.F.; Restrepo, M.; Bussaneli, D.G.; Fragelli, C.; de Cássia Loiola Cordeiro, R.; Santos-Pinto, L.; Jeremias, F. Clinical Changes in the Severity of Dental Fluorosis: A Longitudinal Evaluation. BMC Oral Health 2021, 21, 366. [Google Scholar] [CrossRef]
- Dong, H.; Yang, X.; Zhang, S.; Wang, X.; Guo, C.; Zhang, X.; Ma, J.; Niu, P.; Chen, T. Associations of Low Level of Fluoride Exposure with Dental Fluorosis among U.S. Children and Adolescents, NHANES 2015–2016. Ecotoxicol. Environ. Saf. 2021, 221, 112439. [Google Scholar] [CrossRef]
- Jullien, S. Prophylaxis of Caries with Fluoride for Children under Five Years. BMC Pediatr. 2021, 21, 351. [Google Scholar] [CrossRef]
- Suzuki, M.; Ikeda, A.; Bartlett, J.D. Sirt1 Overexpression Suppresses Fluoride-Induced P53 Acetylation to Alleviate Fluoride Toxicity in Ameloblasts Responsible for Enamel Formation. Arch. Toxicol. 2018, 92, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Gao, Y.; Wang, C.; Zhao, L.; Sun, D. Excessive Fluoride Induces Endoplasmic Reticulum Stress and Interferes Enamel Proteinases Secretion. Environ. Toxicol. 2013, 28, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Martignon, S.; Bartlett, D.; Manton, D.J.; Martinez-Mier, E.A.; Splieth, C.; Avila, V. Epidemiology of Erosive Tooth Wear, Dental Fluorosis and Molar Incisor Hypomineralization in the American Continent. Caries Res. 2021, 55, 1–11. [Google Scholar] [CrossRef]
- Li, Q.; Shen, J.; Qin, T.; Zhou, G.; Li, Y.; Chen, Z.; Li, M. A Qualitative and Comprehensive Analysis of Caries Susceptibility for Dental Fluorosis Patients. Antibiotics 2021, 10, 1047. [Google Scholar] [CrossRef]
- Ostalska-Nowicka, D.; Paszyńska, E.; Dmitrzak-Węglarz, M.; Neyman-Bartkowiak, A.; Rabiega, A.; Zachwieja, J.; Nowicki, M. Dental Caries-Related Primary Hypertension in Children and Adolescents: Cross-Sectional Study. Oral Dis. 2021, 27, 1822–1833. [Google Scholar] [CrossRef]
- Jha, P.K.; Tripathi, P. Arsenic and Fluoride Contamination in Groundwater: A Review of Global Scenarios with Special Reference to India. Groundw. Sustain. Dev. 2021, 13, 100576. [Google Scholar] [CrossRef]
- Aoba, T.; Fejerskov, O. Dental Fluorosis: Chemistry and Biology. Crit. Rev. Oral Biol. Med. 2002, 13, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Public Health. Available online: https://ec.europa.eu/health/index_en (accessed on 1 June 2022).
- Hong, L.; Levy, S.M.; Warren, J.J.; Broffitt, B.; Cavanaugh, J. Fluoride Intake Levels in Relation to Fluorosis Development in Permanent Maxillary Central Incisors and First Molars. Caries Res. 2006, 40, 494–500. [Google Scholar] [CrossRef]
- Mohabatpour, F.; Chen, X.; Papagerakis, S.; Papagerakis, P. Novel Trends, Challenges and New Perspectives for Enamel Repair and Regeneration to Treat Dental Defects. Biomater. Sci. 2022. Advance Article. Available online: https://0-pubs-rsc-org.brum.beds.ac.uk/en/content/articlelanding/2022/bm/d2bm00072e/unauth (accessed on 1 June 2022). [CrossRef]
- Gelli, R.; Ridi, F.; Baglioni, P. The Importance of Being Amorphous: Calcium and Magnesium Phosphates in the Human Body. Adv. Colloid Interface Sci. 2019, 269, 219–235. [Google Scholar] [CrossRef]
- Moreira, K.M.; Bertassoni, L.E.; Davies, R.P.; Joia, F.; Höfling, J.F.; Nascimento, F.D.; Puppin-Rontani, R.M. Impact of Biomineralization on Resin/Biomineralized Dentin Bond Longevity in a Minimally Invasive Approach: An “in Vitro” 18-Month Follow-Up. Dent. Mater. 2021, 37, e276–e289. [Google Scholar] [CrossRef] [PubMed]
- Burwell, A.K.; Litkowski, L.J.; Greenspan, D.C. Calcium Sodium Phosphosilicate (NovaMin®): Remineralization Potential. Adv. Dent. Res. 2009, 21, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Nebu, P. State of the Art Enamel Remineralization Systems: The Next Frontier in Caries Management. Caries Res. 2019, 53, 284–295. Available online: https://www.karger.com/Article/Abstract/493031 (accessed on 1 June 2022).
- Biria, M.; Rezvani, Y.; Roodgarian, R.; Rabbani, A.; Iranparvar, P. Antibacterial Effect of an Herbal Toothpaste Containing Bamboo Salt: A Randomized Double-Blinded Controlled Clinical Trial. BMC Oral Health 2022, 22, 193. [Google Scholar] [CrossRef]
- Delbem, A.C.B.; Pessan, J.P. Alternatives to Enhance the Anticaries Effects of Fluoride. In Pediatric Restorative Dentistry; Springer: Cham, Switzerland, 2019; Available online: https://0-link-springer-com.brum.beds.ac.uk/chapter/10.1007/978-3-319-93426-6_6 (accessed on 2 June 2022).
- Soneta, S.P.; Hugar, S.M.; Hallikerimath, S.; Gokhale, N.; Joshi, R.S.; Uppin, C. A Comparative Evaluation of Remineralizing Potential of Commonly Used Fluoridated Toothpaste, Herbal Toothpaste, Toothpaste with Zinc Hydroxyapatite, and Toothpaste with Calcium Sucrose Phosphate in Children: A Scanning Electronic Microscopic Study. Int. J. Clin. Pediatr. Dent. 2022, 15, S158–S163. [Google Scholar] [CrossRef]
- Chang, H.; Lee, J. Formulating a Vitamin D Delivery Toothpaste Using a Penetration Promotor. J. Int. Res. Med. Pharm. Sci. 2020, 15, 20–31. Available online: https://www.ikppress.org/index.php/JIRMEPS/article/view/5472 (accessed on 2 June 2022).


{kind=link}
| Severity of Fluorosis * | Number of Cases in Groups with Different Severity Level * n (%) | |
|---|---|---|
| 0 | 607 (87.2%) | |
| 1 | 12 (1.7%) | Total groups 1–3: 89 (12.8%) |
| 2 | 56 (8.1%) | |
| 3 | 21 (3.0%) | |
| 4 | n.o. | |
| 5 | n.o. | |
| Total number of study participants: | 696 | |
| Group | n | Mean ± SD (mg/g) | p-Value |
|---|---|---|---|
| I | 10 | 28.12 ± 1.75 | * p = 0.002 |
| II | 10 | 32.08 ± 2.12 | ** p = 0.914 |
| III | 10 | 33.01 ± 3.12 | *** p < 0.001 |
| Group | n | Mean ± SD (mg/g) | p-Value |
|---|---|---|---|
| I | 10 | 0.81 ± 0.10 | * p < 0.001 |
| II | 10 | 1.17 ± 0.13 | ** p = 0.221 |
| III | 10 | 1.24 ± 0.22 | *** p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strużycka, I.; Olszewska, A.; Bogusławska-Kapała, A.; Hryhorowicz, S.; Kaczmarek-Ryś, M.; Grabarek, B.O.; Staszkiewicz, R.; Kuciel-Polczak, I.; Czajka-Jakubowska, A. Assessing Fluorosis Incidence in Areas with Low Fluoride Content in the Drinking Water, Fluorotic Enamel Architecture, and Composition Alterations. Int. J. Environ. Res. Public Health 2022, 19, 7153. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127153
Strużycka I, Olszewska A, Bogusławska-Kapała A, Hryhorowicz S, Kaczmarek-Ryś M, Grabarek BO, Staszkiewicz R, Kuciel-Polczak I, Czajka-Jakubowska A. Assessing Fluorosis Incidence in Areas with Low Fluoride Content in the Drinking Water, Fluorotic Enamel Architecture, and Composition Alterations. International Journal of Environmental Research and Public Health. 2022; 19(12):7153. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127153
Chicago/Turabian StyleStrużycka, Izabela, Aneta Olszewska, Agnieszka Bogusławska-Kapała, Szymon Hryhorowicz, Marta Kaczmarek-Ryś, Beniamin Oskar Grabarek, Rafał Staszkiewicz, Izabela Kuciel-Polczak, and Agata Czajka-Jakubowska. 2022. "Assessing Fluorosis Incidence in Areas with Low Fluoride Content in the Drinking Water, Fluorotic Enamel Architecture, and Composition Alterations" International Journal of Environmental Research and Public Health 19, no. 12: 7153. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127153