
Motor Functioning and Intelligence Quotient in Paediatric Survivors of a Fossa Posterior Tumor Following a Multidisciplinary Rehabilitation Program

Abstract
:1. Introduction
- (1)
- Physical functioning and the intelligence quotient (IQ) using a standardized measure and compared to normative data.
- (2)
- The progression of these aforementioned outcome values during a multidisciplinary rehabilitation program.
- (3)
- A possible difference in physical functioning and the intelligence quotient (IQ) between the different histopathological tumors (medulloblastoma, ependymoma, astrocytoma).
- (4)
- (1)
- There is no difference in the outcomes of pediatric survivors of fossa posterior tumor and normative data.
- (2)
- There is no difference in outcomes when comparing the values at the beginning and at the end of the rehabilitation.
- (3)
- The histopathological tumor has no effect on physical functioning and IQ.
- (4)
- Motor functioning is not related to cognitive functioning.
2. Materials and Methods
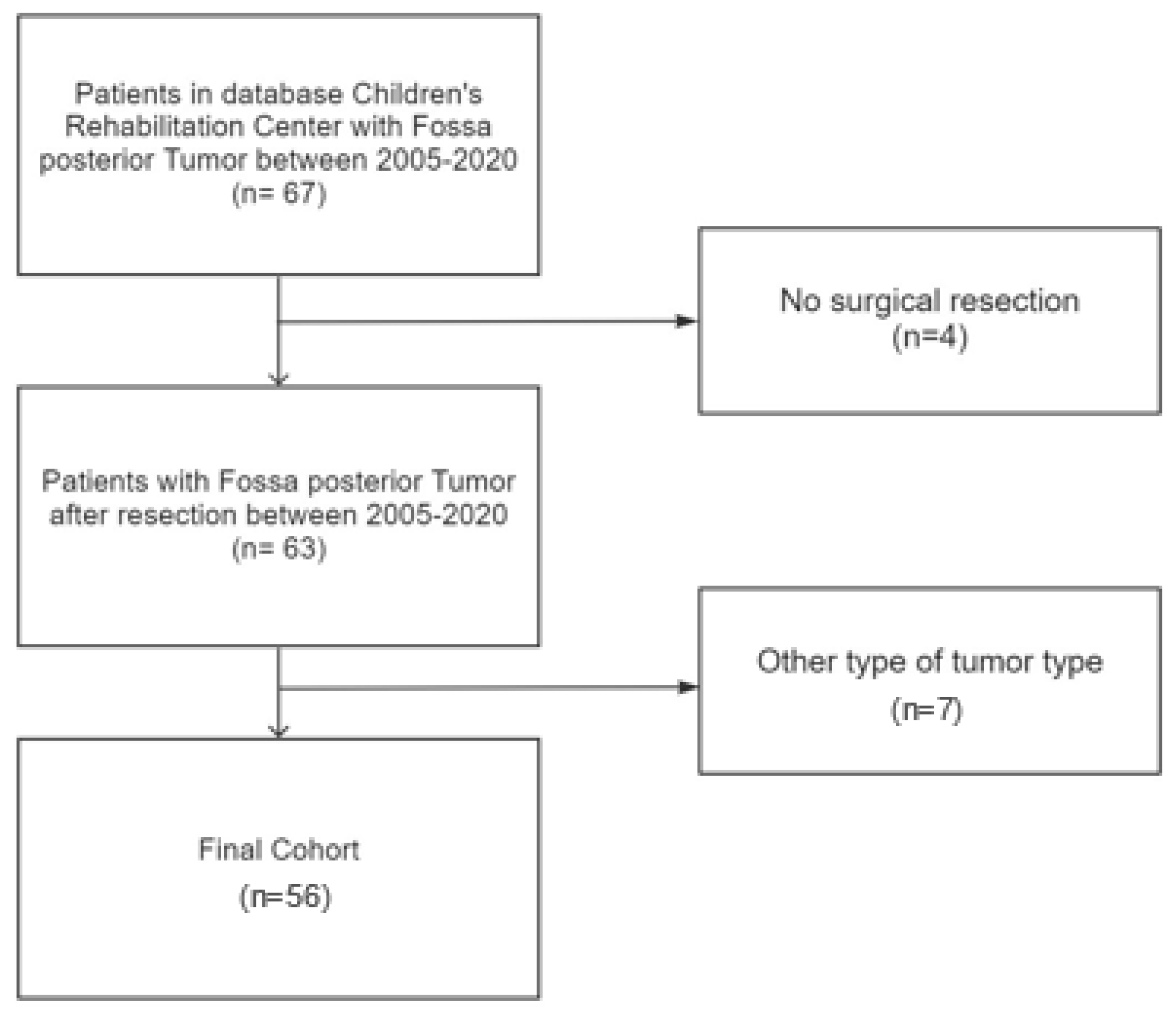
2.1. Participants
2.2. Physical Functioning
2.3. Cognitive Functioning
2.4. Statistical Analysis
3. Results
3.1. Participants
3.2. Physical Functioning
3.2.1. Balance and Range of Motion
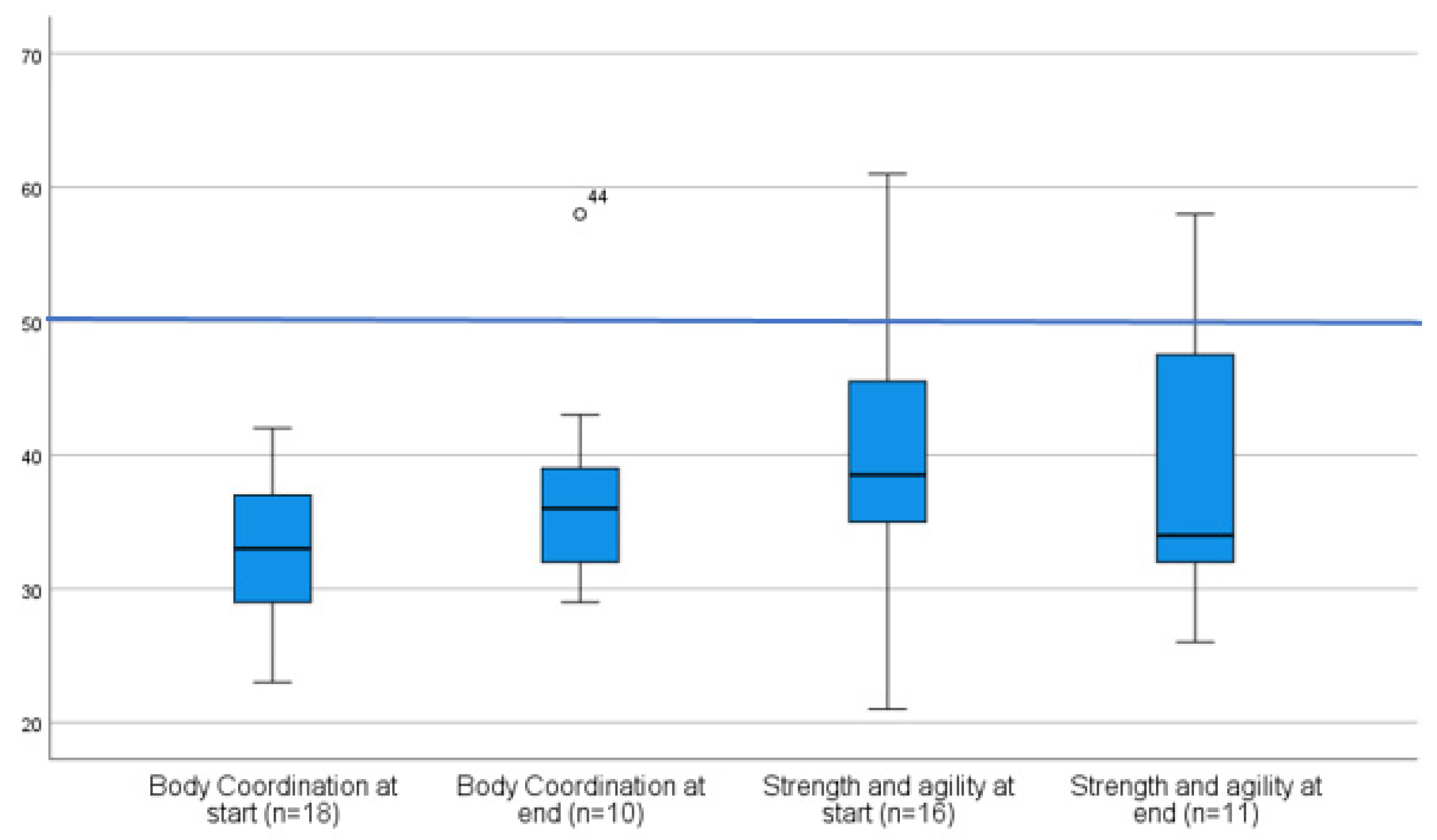
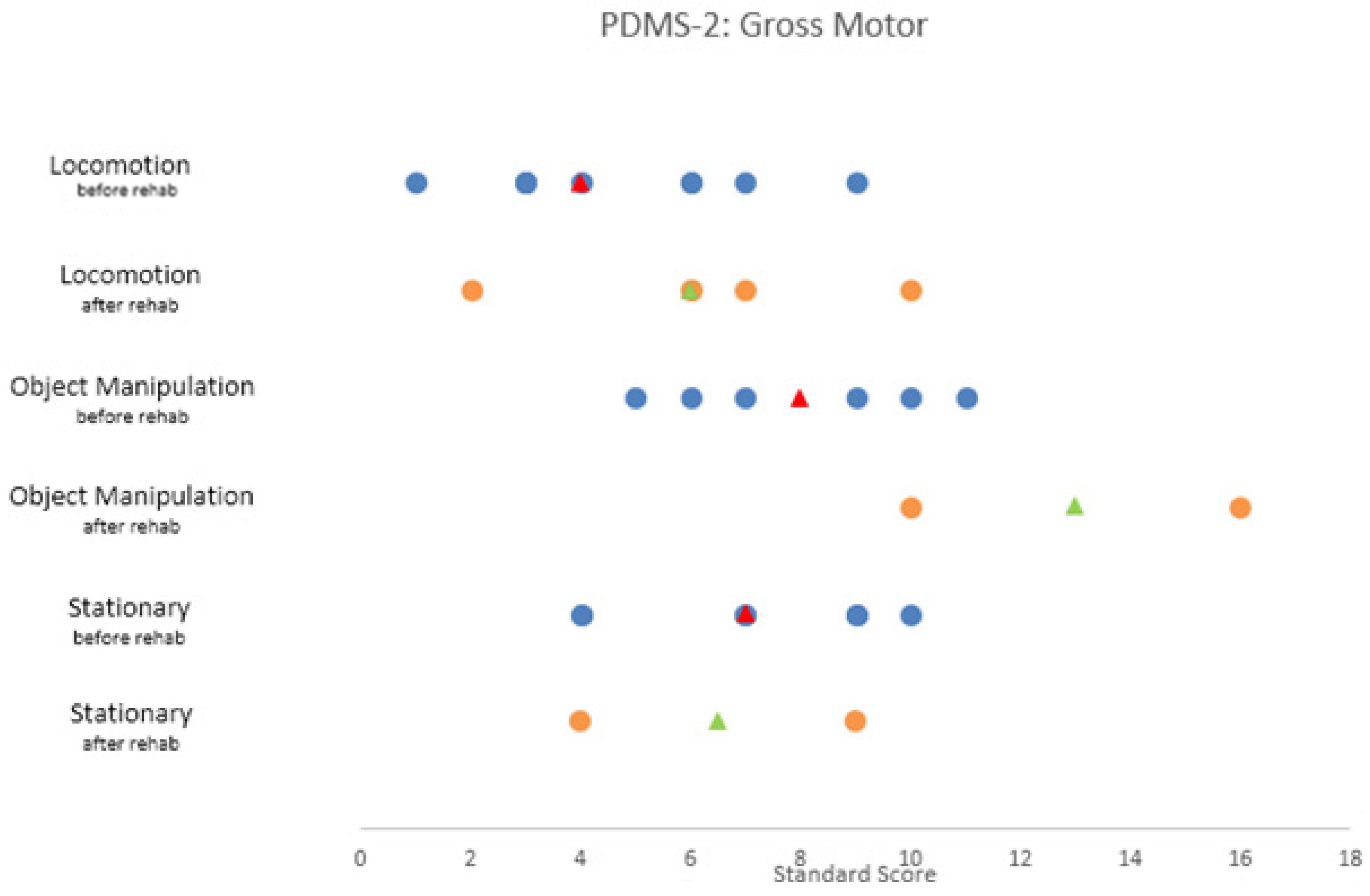
3.2.2. Gross Motor Functioning
The Bruininks–Oseretsky Test of Motor Proficiency Second Edition (BOT-2)
The Peabody Developmental Motor Scale (PDMS-2)
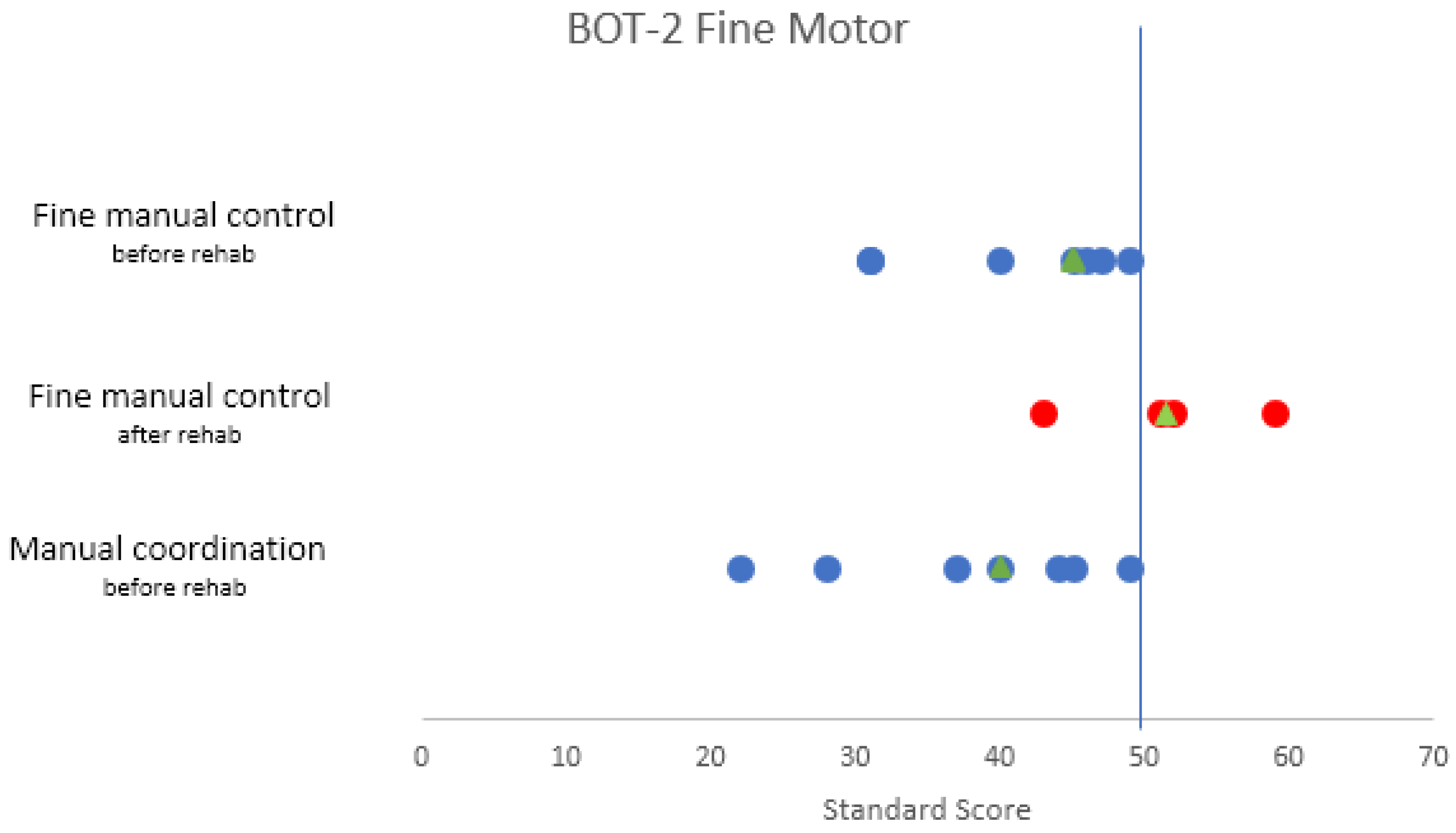
3.2.3. Fine Motor Functioning
The Bruininks–Oseretsky Test of Motor Proficiency Second Edition (BOT-2)
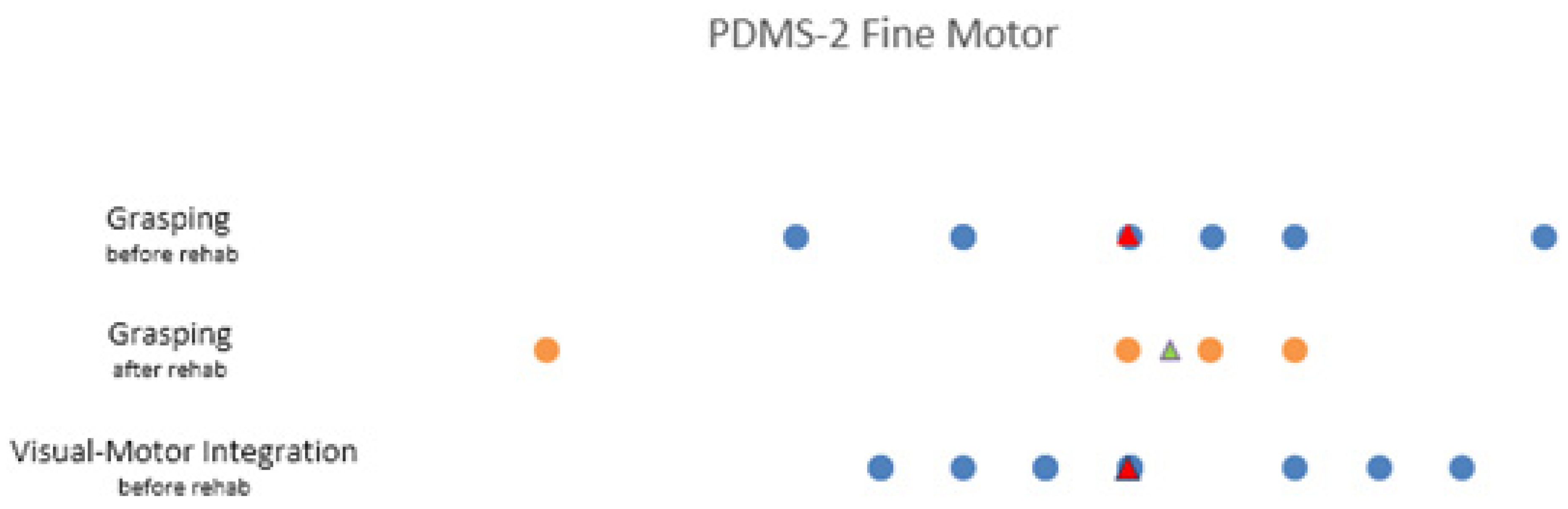
The Peabody Developmental Motor Scale (PDMS-2)
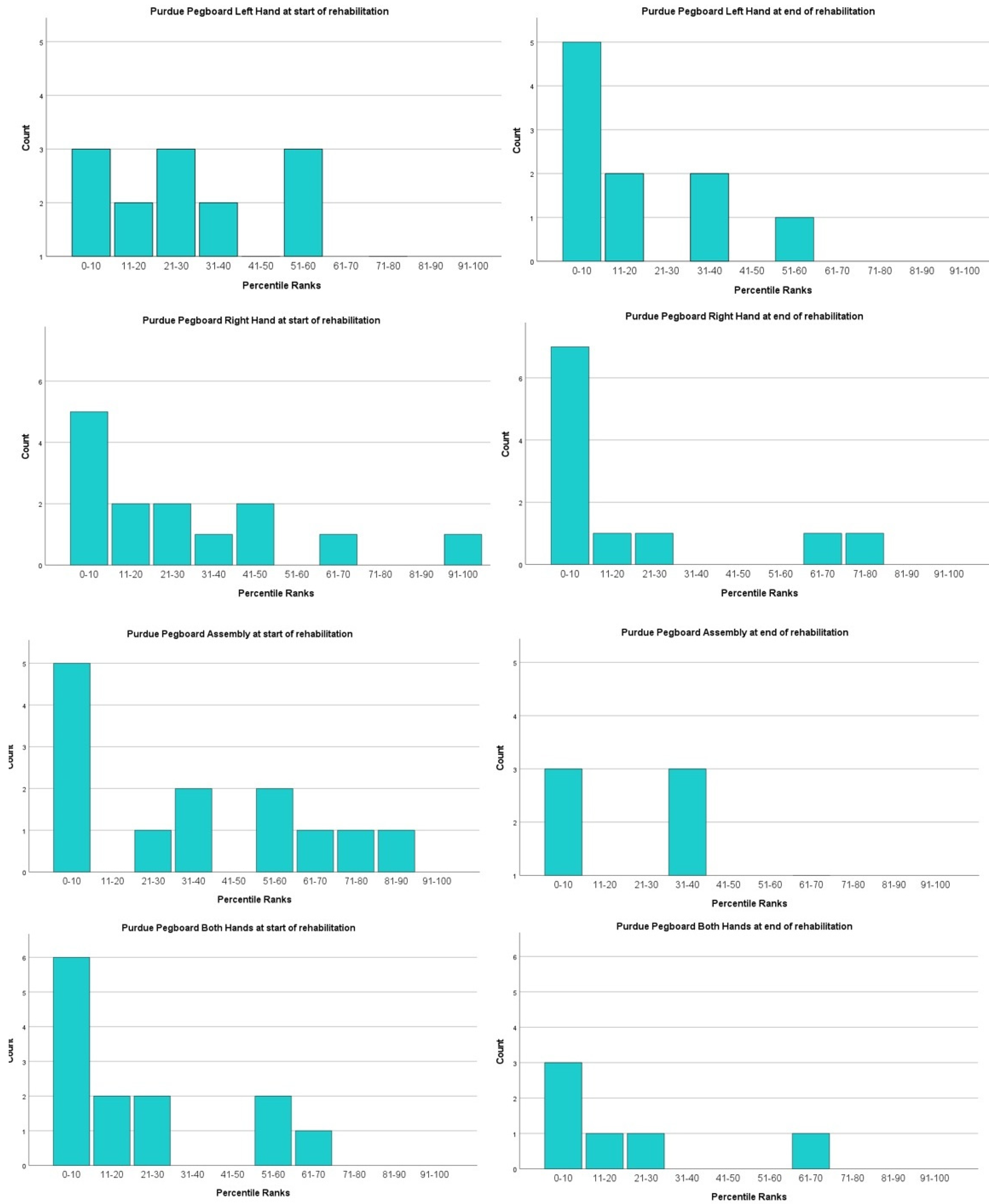
Purdue Pegboard Test (PPT)
3.3. Cognitive Functioning
3.4. Relationship between Intelligence Quotient (IQ) and Motor Functioning
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simon, M.; Hosen, I.; Gousias, K.; Rachakonda, S.; Heidenreich, B.; Gessi, M.; Schramm, J.; Hemminki, K.; Waha, A.; Kumar, R. TERT promoter mutations: A novel independent prognostic factor in primary glioblastomas. Neuro-Oncol. 2015, 17, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Williams, T.; Naushahi, M.; Bernard, A.; Campbell, R. Epidemiology of paediatric central nervous system tumors in Queensland, Australia. J. Clin. Neurosci. 2021, 92, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Alves, C.A.P.F.; Löbel, U.; Martin-Saavedra, J.S.; Toescu, S.; Tsunemi, M.H.; Teixeira, S.R.; Mankad, K.; Hargrave, D.; Jacques, T.S.; da Costa Leite, C.; et al. A diagnostic algorithm for posterior fossa tumors in children: A validation study. Am. J. Neuroradiol. 2021, 42, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Nejat, F.; El Khashab, M.; Rutka, J.T. Initial management of childhood brain tumors: Neurosurgical considerations. J. Child Neurol. 2008, 23, 1136–1148. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.D.; Fidler-Benaoudia, M.; Keegan, T.H.; Hipp, H.S.; Jemal, A.; Siegel, R.L. Cancer statistics for adolescents and young adults, 2020. CA A Cancer J. Clin. 2020, 70, 443–459. [Google Scholar] [CrossRef]
- Stensvold, E.; Krossnes, B.K.; Lundar, T.; Due-Tønnessen, B.J.; Frič, R.; Due-Tønnessen, P.; Bechensteen, A.G.; Myklebust, T.Å.; Johannesen, T.B.; Brandal, P. Outcome for children treated for medulloblastoma and supratentorial primitive neuroectodermal tumor (CNS-PNET)—A retrospective analysis spanning 40 years of treatment. Acta Oncol. 2017, 56, 698–705. [Google Scholar] [CrossRef] [Green Version]
- Gadgil, N.; Hansen, D.; Barry, J.; Chang, R.; Lam, S. Posterior fossa syndrome in children following tumor resection: Knowledge update. Surg. Neurol. Int. 2016, 7, S179–S183. [Google Scholar]
- Schmahmann, J.D. Pediatric post-operative cerebellar mutism syndrome, cerebellar cognitive affective syndrome, and posterior fossa syndrome: Historical review and proposed resolution to guide future study. Child’s Nerv. Syst. 2020, 36, 1205–1214. [Google Scholar] [CrossRef]
- Piscione, P.J.; Bouffet, E.; Mabbott, D.J.; Shams, I.; Kulkarni, A.V. Physical functioning in pediatric survivors of childhood posterior fossa brain tumors. Neuro-Oncology 2014, 16, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Dreneva, A.A.; Skvortsov, D.V. Postural balance in pediatric posterior fossa tumor survivors: Through impairments to rehabilitation possibilities. Clin. Biomech. 2020, 71, 53–58. [Google Scholar] [CrossRef]
- Lassaletta, A.; Bouffet, E.; Mabbott, D.; Kulkarni, A.V. Functional and neuropsychological late outcomes in posterior fossa tumors in children. Child’s Nerv. Syst. 2015, 31, 1877–1890. [Google Scholar] [CrossRef] [PubMed]
- Hartley, H.; Pizer, B.; Lane, S.; Sneade, C.; Williams, R.; Mallucci, C.; Bunn, L.; Kumar, R. Incidence and prognostic factors of ataxia in children with posterior fossa tumors. Neuro-Oncol. Pract. 2019, 6, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Hanzlik, E.; Woodrome, S.E.; Abdel-Baki, M.; Geller, T.J.; Elbabaa, S.K. A systematic review of neuropsychological outcomes following posterior fossa tumor surgery in children. Child’s Nerv. Syst. 2015, 31, 1869–1875. [Google Scholar] [CrossRef] [PubMed]
- Butler, R.W.; Sahler, O.J.Z.; Askins, M.A.; Alderfer, M.A.; Katz, E.R.; Phipps, S.; Noll, R.B. Interventions to improve neuropsychological functioning in childhood cancer survivors. Dev. Disabil. Res. Rev. 2008, 14, 251–258. [Google Scholar] [CrossRef]
- Forsyth, R.; Hamilton, C.; Ingram, M.; Kelly, G.; Grove, T.; Wales, L.; Gilthorpe, M.S. Demonstration of functional rehabilitation treatment effects in children and young people after severe acquired brain injury. Dev. Neurorehabilit. 2022, 25, 239–245. [Google Scholar] [CrossRef]
- Capute, A.J.; Shapiro, B.K.; Palmer, F.B.; Ross, A.W.R.C. Cognitive-Motor Interactions: The Relationship of Infant Gross Motor Attainment to IQ at 3 Years. Clin. Pediatrics 1985, 24, 671–675. [Google Scholar] [CrossRef]
- Beckung, E.; Hagberg, G.; Uldall, P.; Cans, C. Probability of walking in children with cerebral palsy in Europe. Pediatrics 2008, 121, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Deitz, J.C.; Kartin, D.; Kopp, K. Review of the Bruininks-Oseretsky Test of Motor Proficiency, Second Edition (BOT-2). Phys. Occup. Ther Pediatr. 2007, 27, 87–102. [Google Scholar] [CrossRef]
- Brown, T. Structural validity of the Bruininks-Oseretsky test of motor proficiency—Second edition brief form (BOT-2-BF). Res. Dev. Disabil. 2019, 85, 92–103. [Google Scholar] [CrossRef]
- van Hartingsveldt, M.J.; Cup, E.H.C.; Oostendorp, R.A.B. Reliability and validity of the fine motor scale of the Peabody Developmental Motor Scales-2. Occup. Ther. Int. 2005, 12, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.H.; Liao, H.F.; Hsieh, C.L. Reliability, sensitivity to change, and responsiveness of the Peabody Developmental Motor Scales-Second Edition for children with cerebral palsy. Phys. Ther. 2006, 86, 1351–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamphaus, R.W. Assessment of adolescent and adult intelligence. In Clinical Assessment of Child and Adolescent Intelligence; Springer: New York, NY, USA, 2005. [Google Scholar]
- Warschausky, S. Wechsler Preschool and Primary Scale of Intelligence. In Encyclopedia of Clinical Neuropsychology; Kreutzer, J.S., DeLuca, J., Caplan, B., Eds.; Springer: New York, NY, USA, 2011. [Google Scholar] [CrossRef]
- Rustler, V.; Hagerty, M.; Daeggelmann, J.; Marjerrison, S.; Bloch, W.; Baumann, F.T. Exercise interventions for patients with pediatric cancer during inpatient acute care: A systematic review of literature. Pediatric Blood Cancer 2017, 64, e26567. [Google Scholar] [CrossRef] [PubMed]
- Konczak, J.; Timmann, D. The effect of damage to the cerebellum on sensorimotor and cognitive function in children and adolescents. Neurosci. Biobehav. Rev. 2007, 31, 1101–1113. [Google Scholar] [CrossRef] [PubMed]
- Green, J.L.; Knight, S.J.; McCarthy, M.D.L.C. Motor functioning during and following treatment with chemotherapy for pediatric acute lymphoblastic leukemia. Pediatric Blood Cancer 2013, 60, 1261–1266. [Google Scholar] [CrossRef] [PubMed]
- Söntgerath, R.; Eckert, K. Impairments of Lower Extremity Muscle Strength and Balance in Childhood Cancer Patients and Survivors: A Systematic Review. Pediatric Hematol. Oncol. 2015, 32, 585–612. [Google Scholar] [CrossRef]
- Johnson, D.L.; McCabe, M.A.; Nicholson, H.S.; Joseph, A.L.; Getson, P.R.; Byrne, J.; Brasseux, C.; Packer, R.J.; Reaman, G. Quality of long-term survival in young children with medulloblastoma. J. Neurosurg. 1994, 80, 1004–1010. [Google Scholar] [CrossRef] [Green Version]
- Grimshaw, S.L.; Taylor, N.F.; Shields, N. The Feasibility of Physical Activity Interventions During the Intense Treatment Phase for Children and Adolescents with Cancer: A Systematic Review. Pediatric Blood Cancer 2016, 63, 1586–1593. [Google Scholar] [CrossRef]
- Goebel, A.M.; Koustenis, E.; Rueckriegel, S.M.; Pfuhlmann, L.; Brandsma, R.; Sival, D.; Skarabis, H.; Schuelke, M.; Driever, P.H. Motor function in survivors of pediatric acute lymphoblastic leukemia treated with chemotherapy-only. Eur. J. Paediatr. Neurol. 2019, 23, 304–316. [Google Scholar] [CrossRef]
- Harila-Saari, A.H.; Huuskonen, U.E.J.; Tolonen, U.; Vainionpää, L.K.; Lanning, B.M. Motor nervous pathway function is impaired after treatment of childhood acute lymphoblastic leukemia: A study with motor evoked potentials. Med. Pediatric Oncol. 2001, 36, 345–351. [Google Scholar] [CrossRef]
- Reinders-Messelink, H.; Schoemaker, M.; Snijders, T.; Göeken, L.; van den Briel, M.; Bökkerink, J.; Kamps, W. Motor performance of children during treatment for acute lymphoblastic leukemia. Med. Pediatric Oncol. 1999, 33, 545–550. [Google Scholar] [CrossRef]
- Reinders-Messelink, H.A.; Schoemaker, M.M.; Hofte, M.; Göeken, L.N.; Kingma, A.; van den Briel, M.M.; Kamps, W.A. Fine motor and handwriting problems after treatment for childhood acute lymphoblastic leukemia. Med. Pediatric Oncol. 1996, 27, 551–555. [Google Scholar] [CrossRef]
- Hockenberry, M.; Krull, K.; Moore, K.; Gregurich, M.A.; Casey, M.E.; Kaemingk, K. Longitudinal evaluation of fine motor skills in children with leukemia. J. Pediatric Hematol./Oncol. 2007, 29, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Grill, J.; Viguier, D.; Kieffer, V.; Bulteau, C.; Sainte-Rose, C.; Hartmann, O.; Kalifa, C.; Dellatolas, G. Critical risk factors for intellectual impairment in children with posterior fossa tumors: The role of cerebellar damage. J. Neurosurg. 2004, 101 (Suppl. 2), 152–158. [Google Scholar] [CrossRef] [PubMed]
- Baillieux, H.; Smet HJ de Paquier, P.F.; de Deyn, P.P.; Mariën, P. Cerebellar neurocognition: Insights into the bottom of the brain. Clin. Neurol. Neurosurg. 2008, 110, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Duffner, P.K.; Cohen, M.E.; Thomas, P. Late effects of treatment on the intelligence of children with posterior fossa tumors. Cancer 1983, 51, 233–237. [Google Scholar] [CrossRef]
- Ris, M.D.; Packer, R.; Goldwein, J.; Jones-Wallace, D.; Boyett, J.M. Intellectual outcome after reduced-dose radiation therapy plus adjuvant chemotherapy for medulloblastoma: A children’s cancer group study. J. Clin. Oncol. 2001, 19, 3470–3476. [Google Scholar] [CrossRef]
- Maddrey, A.M.; Bergeron, J.A.; Lombardo, E.R.; McDonald, N.K.; Mulne, A.F.; Barenberg, P.D.; Bowers, D.C. Neuropsychological performance and quality of life of 10 year survivors of childhood medulloblastoma. J. Neuro-Oncol. 2005, 72, 245–253. [Google Scholar] [CrossRef]
- Cahaney, C.; Stefancin, P.; Coulehan, K.; Parker, R.I.; Preston, T.; Goldstein, J.; Hogan, L.; Duong, T.Q. Anatomical brain MRI study of pediatric cancer survivors treated with chemotherapy: Correlation with behavioral measures. Magn. Reson. Imaging 2020, 72, 8–13. [Google Scholar] [CrossRef]
- Gandy, K.; Scoggins, M.A.; Jacola, L.M.; Litten, M.; Reddick, W.E.; Krull, K.R. Structural and Functional Brain Imaging in Long-Term Survivors of Childhood Acute Lymphoblastic Leukemia Treated with Chemotherapy: A Systematic Review. JNCI Cancer Spectr. 2021, 5, pkab069. [Google Scholar] [CrossRef]
- Kushner, D.S.; Amidei, C. Rehabilitation of motor dysfunction in primary brain tumor patients. Neuro-Oncol. Pract. 2015, 2, 185–191. [Google Scholar] [CrossRef] [Green Version]
- de Spéville, E.D.; Kieffer, V.; Dufour, C.; Grill, J.; Noulhiane, M.; Hertz-Pannier, L.; Chevignard, M. Neuropsychological consequences of childhood medulloblastoma and possible interventions: A review. Neurochirurgie 2021, 67, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Ospina, P.A.; Mcneely, M.L. A Scoping Review of Physical Therapy Interventions for Childhood Cancers|Physiotherapy Canada. Physiother. Can. 2019, 71, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Popernack, M.L.; Gray, N.; Reuter-Rice, K. Moderate-to-Severe Traumatic Brain Injury in Children: Complications and Rehabilitation Strategies. J. Pediatric Health Care 2015, 29, e1–e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray, M.P.; Woods, D.; Hadjikoumi, I. Early access to rehabilitation for paediatric patients with traumatic brain injury. Eur. J. Trauma Emerg. Surg. 2012, 38, 423–431. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | % | ||
|---|---|---|---|
| Tumor Histology | Ependymoma | 7 | 12.5 |
| Medulloblastoma | 28 | 50 | |
| Pilocytic Astrocytoma | 21 | 37.5 | |
| Sex | Male | 35 | 62.5 |
| Female | 21 | 37.5 | |
| Mean Age (SD) | 6.512 | 4.129 | |
| External Ventricular Drain at presentation | Yes | 38 | 67.9 |
| No | 18 | 32.1 | |
| Relapse Tumor | Yes | 23 | 41.1 |
| No | 33 | 58.9 | |
| Deceased | Yes | 11 | 19.6 |
| No | 45 | 80.4 |
| Physical Functioning Parameters | Tumor Histology | Statistical Significance (p) | |||||
|---|---|---|---|---|---|---|---|
| Medulloblastoma | Ependymoma | Pilocytic Astrocytoma | |||||
| Normal | Abnormal | Normal | Abnormal | Normal | Abnormal | ||
| Balance before rehab (n = 16) | 0% | 68.8% (11/16) | 6.3% (1/16) | 0% | 0% | 25% (4/16) | <0.001 |
| Balance after rehab (n = 8) | 0% | 50% (4/8) | 12.5% (1/8) | 0% | 25% (2/8) | 12.5% (1/8) | <0.076 |
| Mobility upper limbs before rehab (n = 47) | 44.7% (21/47) | 2.1% (1/47) | 10.6% (5/47) | 0% | 38.3% (18/47) | 4.3% (2/47) | <0.637 |
| Mobility upper limbs after rehab (n = 27) | 55.6% (15/27) | 0% | 7.4% (2/27) | 0% | 37% (10/27) | 0% | * |
| Mobility lower limbs before rehab (n = 48) | 35.4% (17/48) | 10.4% (5/48) | 10.4% (5/48) | 0% | 41.7% (20/48) | 2.1% (1/48) | <0.138 |
| Mobility lower limbs after rehab (n = 28) | 35.7% (10/28) | 21.4% (6/28) | 7.1% (2/28) | 0% | 35.7% (10/28) | 0% | <0.057 |
| IQ Score by Tumor Histology | |||||||
|---|---|---|---|---|---|---|---|
| Tumor Histology | Total IQ before Rehab | Total IQ after Rehab | Verbal IQ before Rehab | Verbal IQ after Rehab | Performance IQ before Rehab | Performance IQ after Rehab | |
| Ependymoma | Mean | 90.33 | 92.67 | 90.75 | |||
| N | 3 | 3 | 4 | ||||
| Std. Deviation | 14.295 | 12.342 | 14.431 | ||||
| Medulloblastoma | Mean | 92.31 | 82.44 | 96.07 | 88.33 | 87.23 | 80.56 |
| N | 16 | 9 | 14 | 9 | 13 | 9 | |
| Std. Deviation | 12.826 | 11.980 | 12.899 | 12.510 | 12.969 | 10.760 | |
| Pylocytic Astrocytoma | Mean | 89.25 | 89.00 | 94.50 | 74.00 | 86.30 | 101.00 |
| N | 12 | 3 | 10 | 1 | 10 | 1 | |
| Std. Deviation | 13.505 | 6.245 | 19.283 | . | 14.158 | . | |
| Total | Mean | 90.94 | 84.08 | 95.11 | 86.90 | 87.41 | 82.60 |
| N | 31 | 12 | 27 | 10 | 27 | 10 | |
| Std. Deviation | 12.842 | 10.967 | 14.998 | 12.635 | 13.162 | 12.030 | |
| BOT-2 Bodycoordination | BOT-2 Strength and Agility | PDMS-2 Locomotion | PDMS-2 Object Manipulation | PDMS-2 Stationary | ||
|---|---|---|---|---|---|---|
| Total IQ | Pearson Correlation | 0.519 | 0.317 | 0.197 | −0.346 | −0.002 |
| Sig. (2-tailed) | 0.102 | 0.372 | 0.751 | 0.775 | 0.998 | |
| N | 11 | 10 | 5 | 3 | 5 | |
| Verbal IQ | Pearson Correlation | 0.528 | 0.426 | 0.078 | −1.000 | −0.235 |
| Sig. (2-tailed) | 0.144 | 0.293 | 0.922 | . | 0.765 | |
| N | 9 | 8 | 4 | 2 | 4 | |
| Performance IQ | Pearson Correlation | 0.423 | −0.099 | 0.616 | −0.218 | 0.553 |
| Sig. (2-tailed) | 0.257 | 0.815 | 0.268 | 0.860 | 0.447 | |
| N | 9 | 8 | 5 | 3 | 4 | |
| BOT-2 Fine Manual Control | BOT-2 Manual Coordination | PDMS-2 Grasping | PDMS-2 Visual-Motor | ||
|---|---|---|---|---|---|
| Total IQ | Pearson Correlation | −0.158 | −0.099 | −1.000 | 0.064 |
| Sig. (2-tailed) | 0.899 | 0.937 | . | 0.959 | |
| N | 3 | 3 | 2 | 3 | |
| Verbal IQ | Pearson Correlation | −0.785 | −0.094 | −1.000 | 1.000 |
| Sig. (2-tailed) | 0.426 | 0.940 | . | . | |
| N | 3 | 3 | 2 | 2 | |
| Performance IQ | Pearson Correlation | 0.436 | 0.500 | . | −0.904 |
| Sig. (2-tailed) | 0.713 | 0.667 | . | 0.281 | |
| N | 3 | 3 | 2 | 3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Decock, M.; De Wilde, R.; Van der Looven, R.; Vander Linden, C. Motor Functioning and Intelligence Quotient in Paediatric Survivors of a Fossa Posterior Tumor Following a Multidisciplinary Rehabilitation Program. Int. J. Environ. Res. Public Health 2022, 19, 7083. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127083
Decock M, De Wilde R, Van der Looven R, Vander Linden C. Motor Functioning and Intelligence Quotient in Paediatric Survivors of a Fossa Posterior Tumor Following a Multidisciplinary Rehabilitation Program. International Journal of Environmental Research and Public Health. 2022; 19(12):7083. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127083
Chicago/Turabian StyleDecock, Mathieu, Robin De Wilde, Ruth Van der Looven, and Catharine Vander Linden. 2022. "Motor Functioning and Intelligence Quotient in Paediatric Survivors of a Fossa Posterior Tumor Following a Multidisciplinary Rehabilitation Program" International Journal of Environmental Research and Public Health 19, no. 12: 7083. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127083