
Screening of Patient Impairments in an Outpatient Clinic for Suspected Rare Diseases—A Cross-Sectional Study


Abstract
:1. Introduction
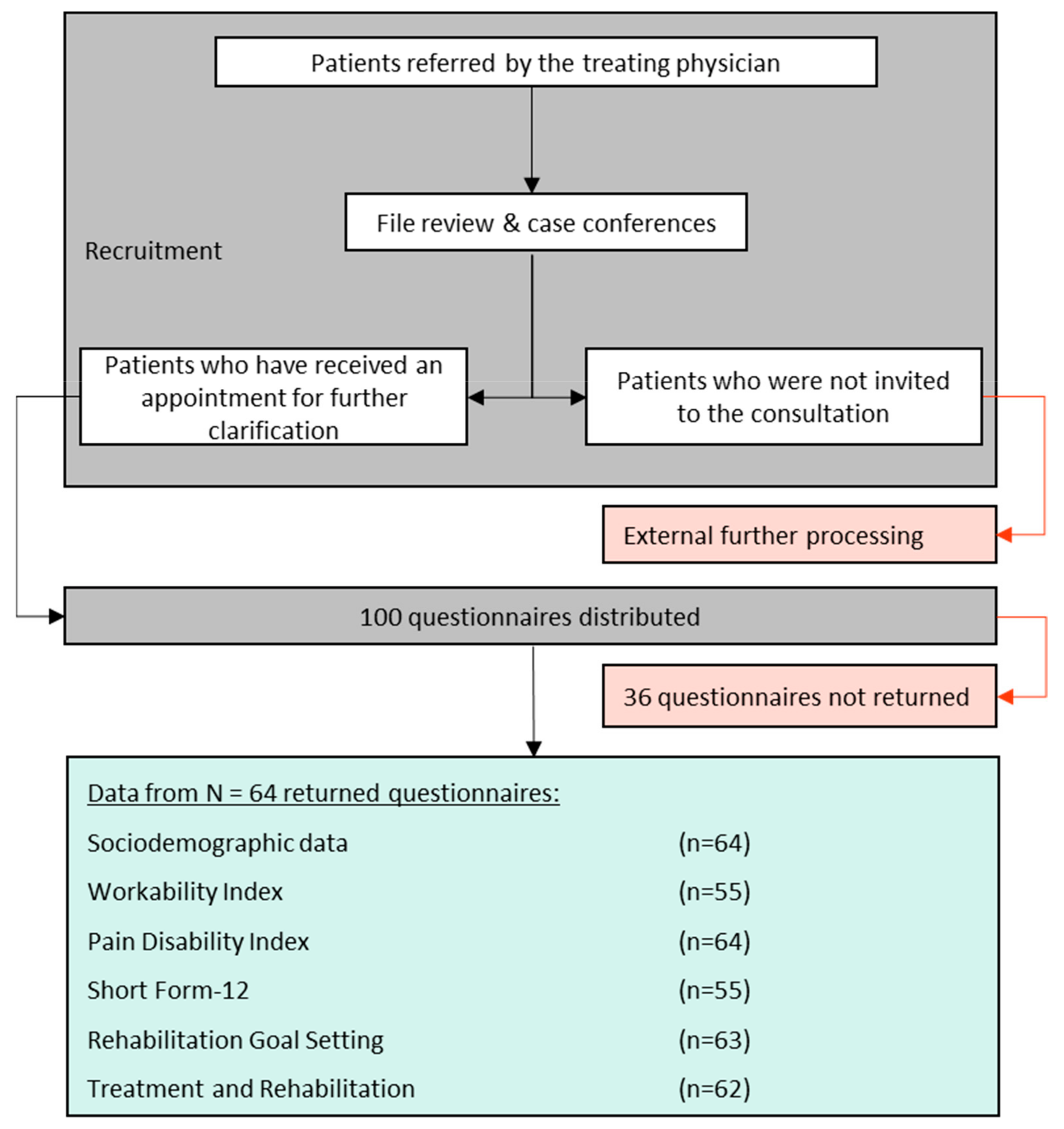
2. Materials and Methods
- Sociodemographic questions
- Rehabilitation Goal Screening (ReGoS)
- Pain Disability Index (PDI)
- Short Form-12 (SF-12)
- For patients of working age: Work Ability Index (WAI)
- Questions about previous therapies and rehabilitation
2.1. Sociodemographic Indicators
2.2. Limitations in Everyday Life Due to Impairment
2.3. Impairment Due to Pain
2.4. Health-Related Quality of Life
2.5. Work Ability Index
- –
- “critical” (7–27 points)—restoring work ability;
- –
- “moderate” (28–36 points)—improve work ability;
- –
- “good” (37–43 points)—support work ability; and
- –
- “very good” (44–49 points)—maintain work ability.
2.6. Treatments and Rehabilitation
2.7. Statistical Methods
3. Results
3.1. Sociodemographic Data
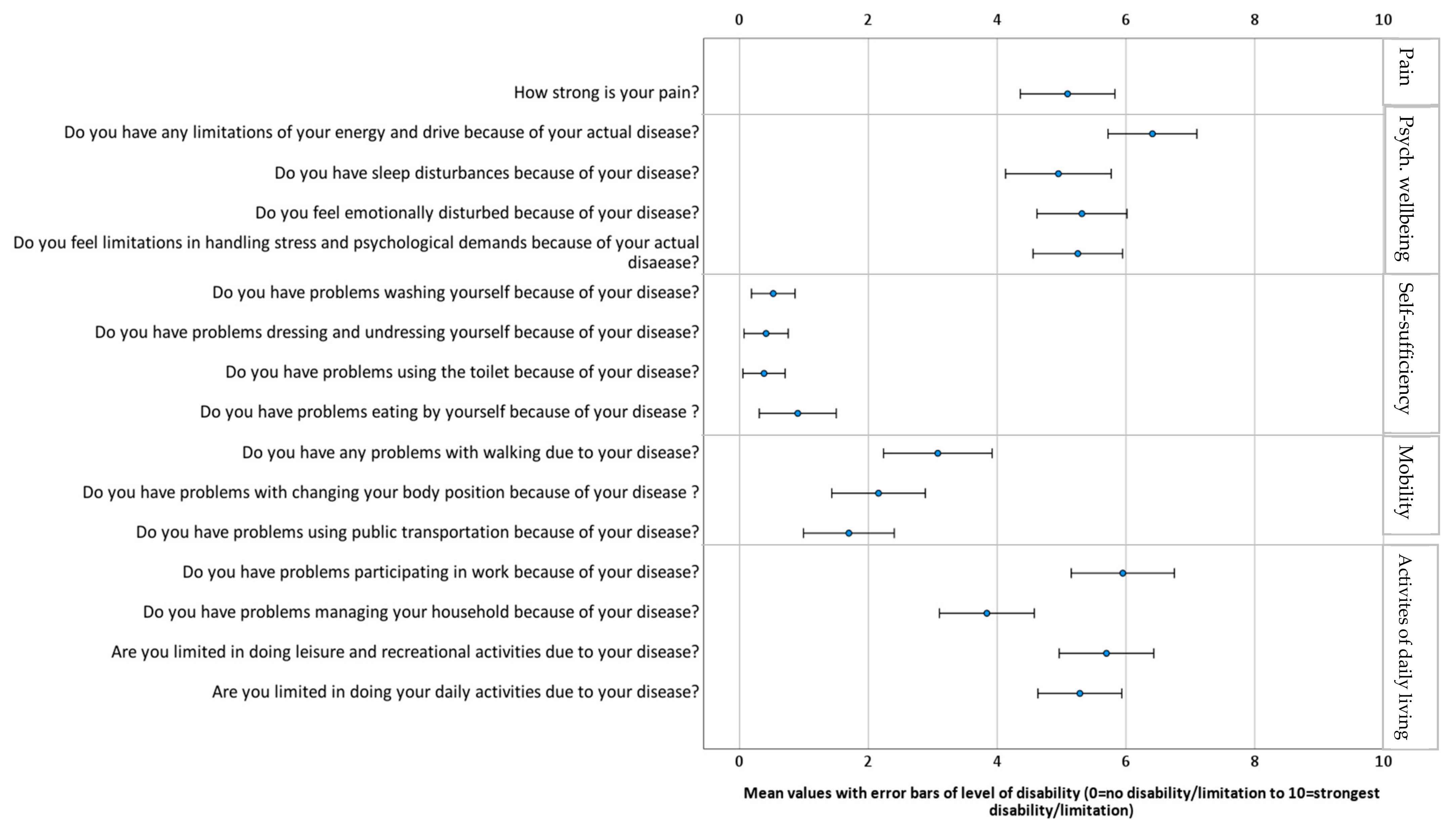
3.2. Restrictions Due to the Disease–Rehabilitation Goal Screening (ReGoS)
3.3. Workability (Work Ability Index)
3.4. Pain Disability Index (PDI)
3.5. Health-Related Quality of Life (SF-12)
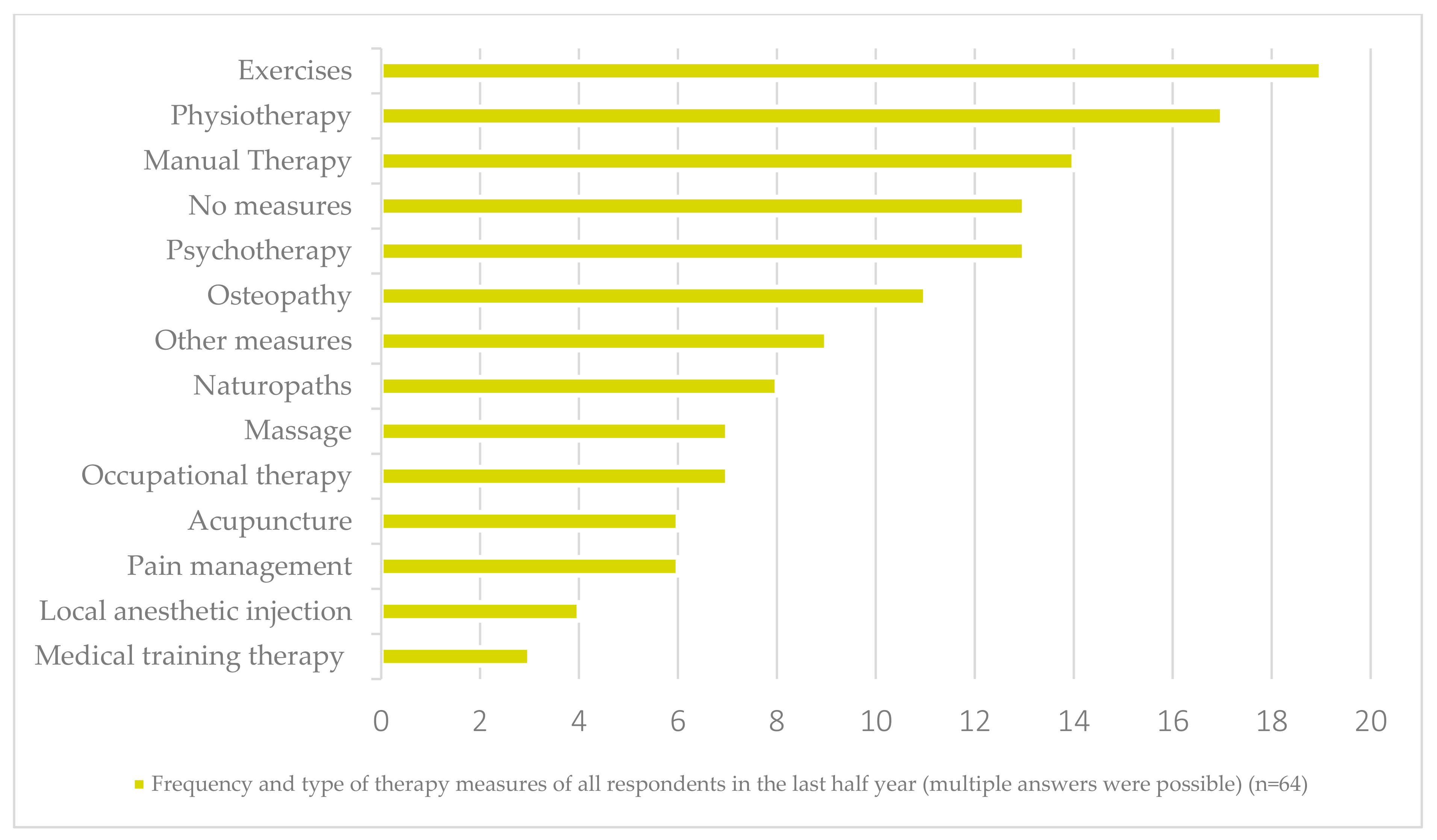
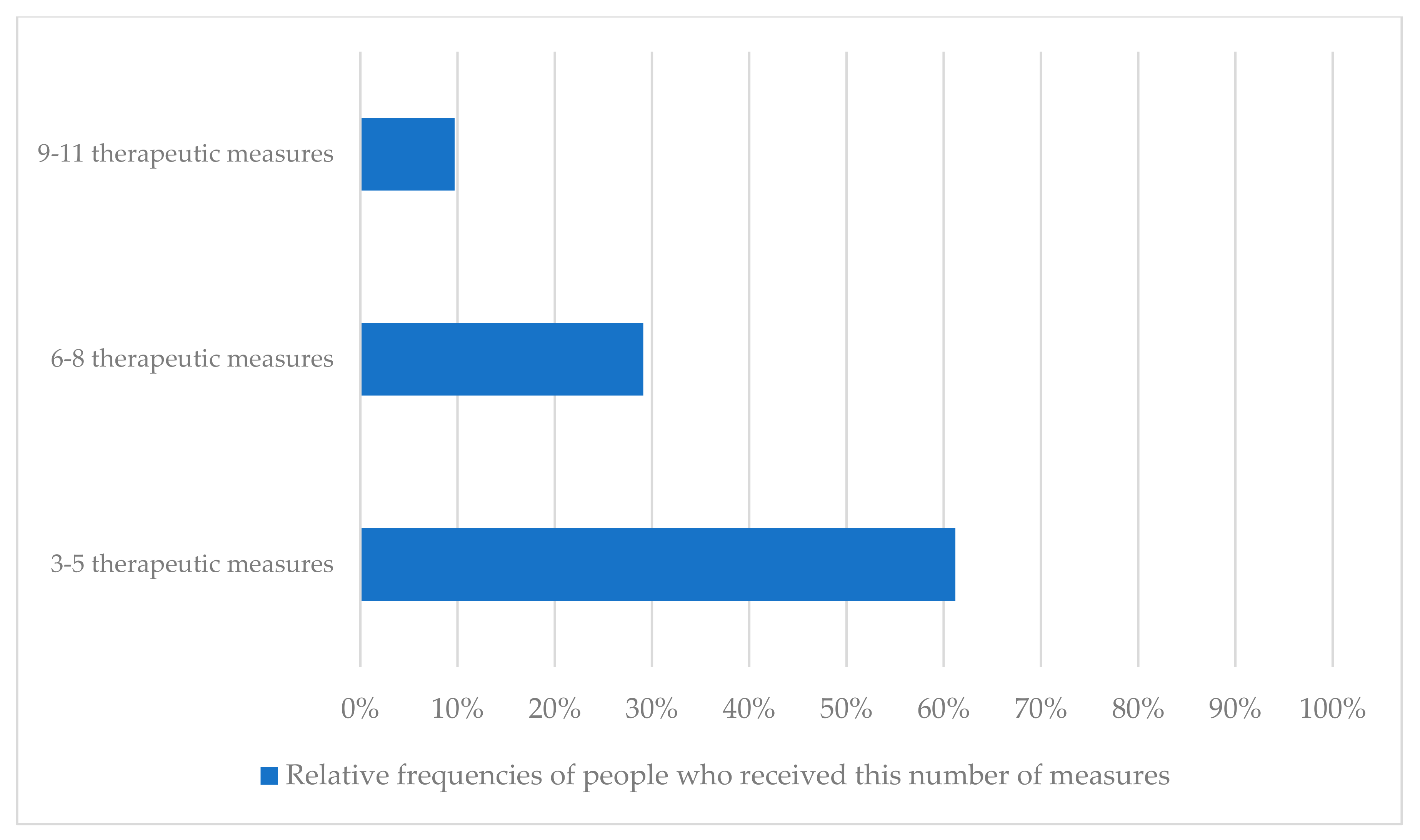
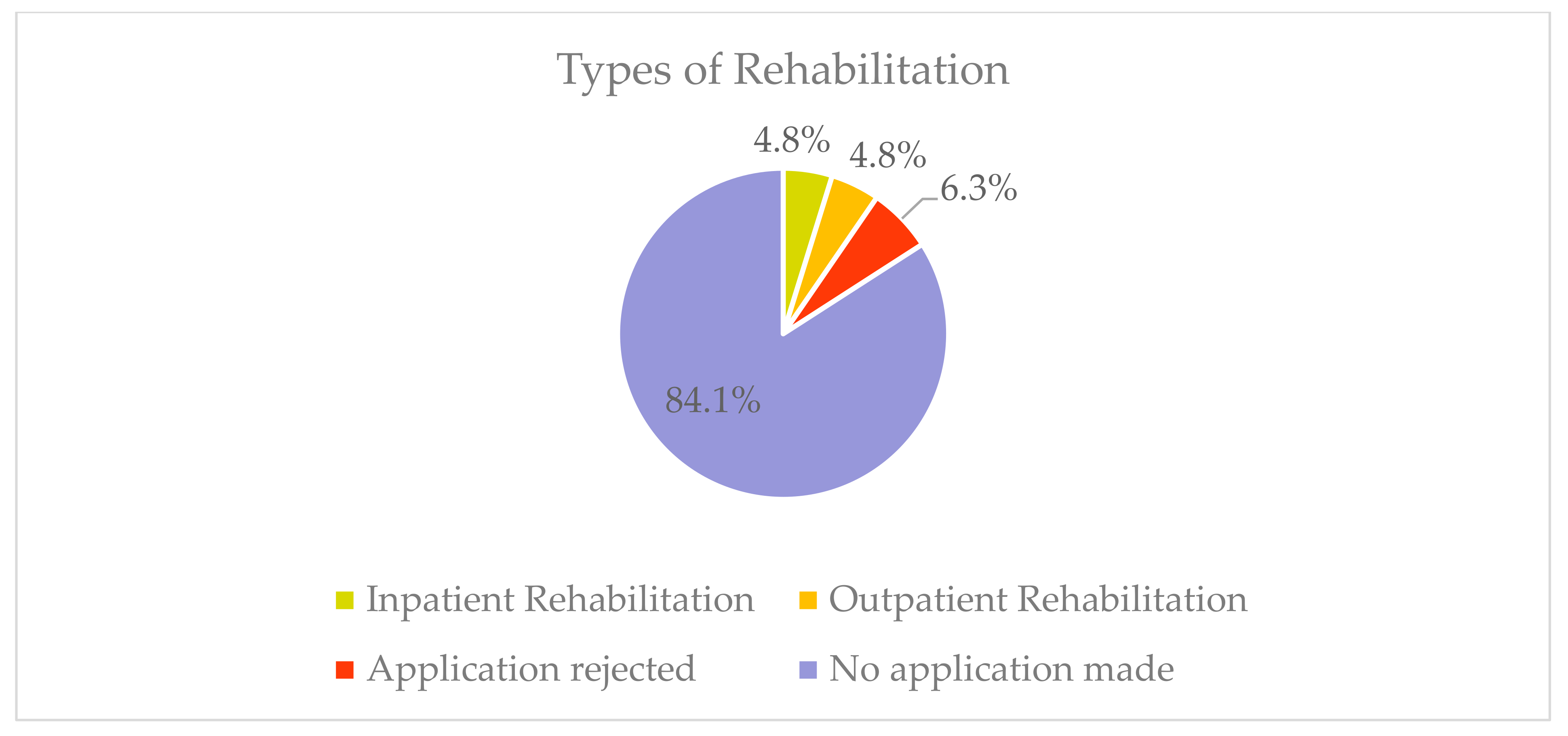
3.6. Previous Treatments and Rehabilitation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richter, T.; Nestler-Parr, S.; Babela, R.; Khan, Z.M.; Tesoro, T.; Molsen, E.; Hughes, D.A. Rare disease terminology and definitions—A systematic global review: Report of the ISPOR rare disease special interest group. Value Health 2015, 18, 906–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vrueh, R.; Baekelandt, E.R.F.; de Haan, J.M.H. Background Paper 6.19 Rare Diseases. Updated 2013. Available online: https://www.who.int/medicines/areas/priority_medicines/BP6_19Rare.pdf (accessed on 2 February 2022).
- European Commission; Consumers, Health, Agriculture and Food Executive Agency; Requena-Méndez, A. European Expert Network for Rare Communicable Diseases and Other Rare Pathologies in the Context of Mobility and Globalization (EURaDMoG); Publications Office of the EU: Luxembourg, 2020. [Google Scholar] [CrossRef]
- Shafie, A.A.; Supian, A.; Hassali, M.A.A.; Ngu, L.-H.; Thong, M.-K.; Ayob, H.; Chaiyakunapruk, N. Rare disease in Malaysia: Challenges and solutions. PLoS ONE 2020, 15, e0230850. [Google Scholar] [CrossRef] [PubMed]
- Dodel, R.; Stieber, C.; Klockgether, T. Seltene erkrankungen in der neurologie—Diagnosestellung, lebensqualität und kosten. Klinikarzt 2015, 44, 36–40. [Google Scholar] [CrossRef]
- Universitätsklinikum Frankfurt. Zentren für Seltene Enkrankungen. Updated 2021. Available online: https://www.se-atlas.de/map/zse#39 (accessed on 2 February 2022).
- Grönblad, M.; Hupli, M.; Wennerstrand, P.; Jarvinen, E.; Lukinmaa, A.; Kouri, J.-P.; Karaharju, E.O. Intercorrelation and test-retest reliability of the pain disability index (PDI) and the oswestry disability questionnaire (ODQ) and their correlation with pain intensity in low back pain patients. Clin. J. Pain 1993, 9, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J.; Tuomi, K.; Klockars, M. Changes in the work ability of active employees over an 11-year period. Scand. J. Work Environ. Health 1997, 23 (Suppl. S1), 49–57. [Google Scholar] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). A conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J. Work ability—A comprehensive concept for occupational health research and prevention. Scand. J. Work Environ. Health 2009, 35, 1–5. Available online: https://pubmed.ncbi.nlm.nih.gov/?term=Work+ability+-+a+comprehensive+concept+for+occupational+health+research+and+prevention (accessed on 31 January 2022). [CrossRef] [PubMed]
- Tuomi, K.; Ilmarinen, J.; Jahkola, A.; Katajarinne, L.; Tulkki, A. Work Ability Index, 2nd ed.; Finnish Institute of Occupational Health: Helsinki, Finland, 1998. [Google Scholar]
- Hasselhorn, H.M.; Freude, G. Der Work Ability Index—Ein Leitfaden. Schriftenreihe Baua. Sonderschr. 2007, Bd.87. Available online: https://BAuA-Repositorium-Der+WorkAbility+Index-ein+Leitfaden-Bundesanstalt+für+Arbeitsschutz+und+Arbeitsmedizin (accessed on 2 February 2022).
- Dillmann, U.; Nilges, P.; Saile, H.; Gerbershagen, H.U. Assessing disability in chronic pain patients. Schmerz 1994, 8, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Soer, R.; Köke, A.J.A.; Speijer, B.L.G.N.; Vroomen, P.C.A.J.; Smeets, R.J.E.M.; Coppes, M.H.; Reneman, M.F.; Gross, D.P.; Groningen Spine Study Group. Reference values of the pain disability index in patients with painful musculoskeletal and spinal disorders: A cross-national study. Spine 2015, 40, 545. [Google Scholar] [CrossRef] [PubMed]
- Uhlenbusch, N.; Löwe, B.; Depping, M.K. Perceived burden in dealing with different rare diseases: A qualitative focus group study. BMJ Open 2019, 9, e033353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, D.M.; Currie, K.C. Depression, anxiety and their relationship with chronic diseases: A review of the epidemiology, risk and treatment evidence. Med. J. Aust. 2009, 190, 54. [Google Scholar] [CrossRef] [PubMed]
- Kole, A.; Faurisson, F. The Voice of 12,000 Patients—Experiences and Expectations of Rare Disease Patients on Diagnosis and Care in Europe; EURODIS: Paris, France, 2009. [Google Scholar]
- Hüppe, M.; Kükenshöner, S.; Böhme, K.; Bosse, F.; Casser, H.R.; Kohlmann, T.; Lindena, G.; Nagel, B.; Pfingsten, M.; Petzke, F. Pain therapy care in Germany—Do patients receiving day care differ from those receiving outpatient or inpatient care at the start of treatment? A further evaluation based on the KEDOQ-pain data set. Schmerz 2020, 34, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Courbier, S.; Berjonneau, E. Juggling Care and Daily Life—The Balancing Act of the Rare Disease Community—A Rare Barometer Survey; EURODIS: Paris, France, 2017; Available online: http://download2.eurordis.org.s3.amazonaws.com/rbv/2017_05_09_Social%20survey%20leaflet%20final.pdf (accessed on 24 February 2022).
- Depping, M.K.; Uhlenbusch, N.; von Kodolitsch, Y.; Klose, H.F.E.; Mautner, V.; Löwe, B. Supportive care needs of patients with rare chronic diseases: Multi-method, cross-sectional study. Orphanet J. Rare Dis. 2021, 16, 44. [Google Scholar] [CrossRef] [PubMed]
- Kriegisch, V.; Kuhn, B.; Dierks, M.-L.; Achenbach, J.; Briest, J.; Fink, M.; Dusch, M.; Amelung, V.; Karst, M. Bewertung der ambulanten ärztlichen schmerztherapie in deutschland. Schmerz 2021, 35, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Dietl, M.; Korczak, D. Versorgungssituation in der Schmerztherapie in Deutschland im Internationalen Vergleich Hinsichtlich über-, unter- oder Fehlversorgung; DIMDI: Cologne, Germany, 2011; Volume 111. [Google Scholar]
- Singer, S.; Maier, L.; Paserat, A.; Lang, K.; Wirp, B.; Kobes, J.; Porsch, U.; Mittag, M.; Toenges, G.; Engesser, D. Wartezeiten auf einen psychotherapieplatz vor und nach der psychotherapiestrukturreform. Psychotherapeut 2022, 67, 176–184. [Google Scholar] [CrossRef]
- Helgeson, V.S.; Zajdel, M. Adjusting to chronic health conditions. Annu. Rev. Psychol. 2017, 68, 545–571. [Google Scholar] [CrossRef] [PubMed]
- Nilges, P.; Diezemann, A. Chronischer schmerz—Konzepte, diagnostik und behandlung. Verhalt. Verhalt. 2018, 39, 167–186. [Google Scholar]
- Rückinger, S.; Boneberger, A. Epidemiologic challenges in rare diseases. Bundesgesundheitsblatt Gesundh. Gesundh. 2008, 51, 483–490. Available online: http://europepmc.org/abstract/MED/18696139 (accessed on 24 February 2022). [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total | ||
|---|---|---|---|
| Mean (SD)/% | |||
| Sociodemographics (n = 64) | Female | 42/65.6 | |
| Male | 22/34.4 | ||
| Age overall [years] | 44.8 (14.6) | ||
| Females | Mean (SD)/% | Min/Max | |
| Age of females | 40.4 (14.4)/ | 19/72 | |
| n | % | ||
| Age group 20–40 | 26 | 63.4 | |
| Age group 41–60 | 11 | 26.8 | |
| Age group >61 | 4 | 9.8 | |
| Males | Mean (SD)/% | Min/Max | |
| Age of males | 53.1 (11.2)/ | 33/80 | |
| n | % | ||
| Age group 20–40 | 3 | 13.6 | |
| Age group 41–60 | 15 | 68.2 | |
| Age group >61 | 4 | 18.2 | |
| mean (SD)/% | |||
| Employed (n = 63) | Yes | 40/63.5 | |
| No | 23/36.5 | ||
| Work Ability Index (n = 60) | Critical | /68.33 | |
| Moderate | /25.00 | ||
| Good | /6.67 | ||
| Very good | /0.00 | ||
| Short Form 12 (n = 55) | Physical | 32.3 (8.29) | |
| Psychological | 43.7 (12.23) | ||
| Pain Disability Index (n = 64) | 33.2 (16.35) | ||
| Number of rehabilitative interventions (n = 62) | 5.5 (1.9) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutenbrunner, C.; Schiller, J.; Goedecke, V.; Lemhoefer, C.; Boekel, A. Screening of Patient Impairments in an Outpatient Clinic for Suspected Rare Diseases—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 8874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19148874
Gutenbrunner C, Schiller J, Goedecke V, Lemhoefer C, Boekel A. Screening of Patient Impairments in an Outpatient Clinic for Suspected Rare Diseases—A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(14):8874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19148874
Chicago/Turabian StyleGutenbrunner, Christoph, Joerg Schiller, Vega Goedecke, Christina Lemhoefer, and Andrea Boekel. 2022. "Screening of Patient Impairments in an Outpatient Clinic for Suspected Rare Diseases—A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 14: 8874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19148874