
Chronotropic Response and Heart Rate Variability before and after a 160 m Walking Test in Young, Middle-Aged, Frail, and Non-Frail Older Adults


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
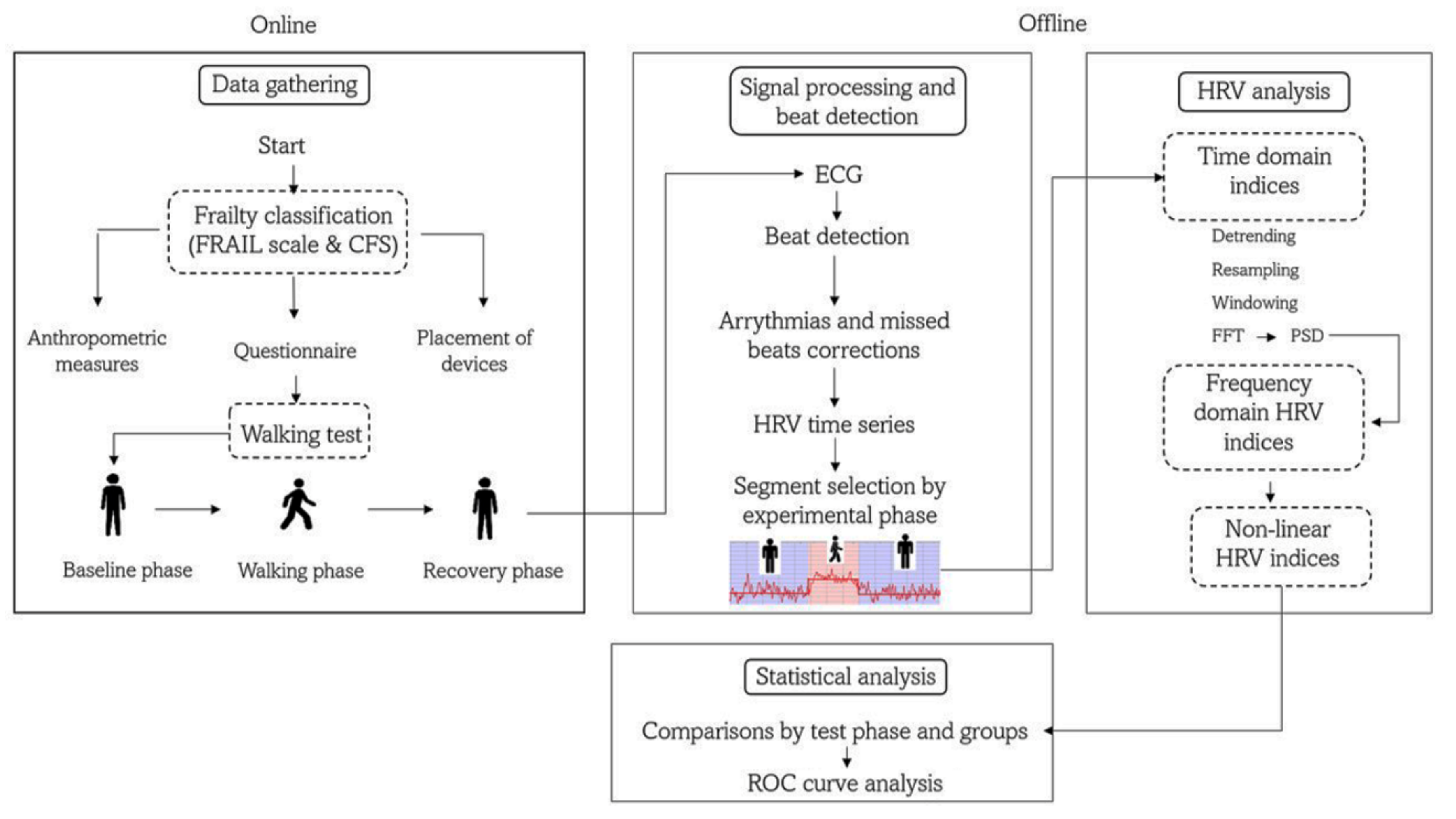
2.2. Study Protocol
2.3. ECG Recording and Beat Detection
2.4. HRV Analysis
2.5. HR Response Parameters
2.6. Statistical Analysis
3. Results
Descriptive Results
4. Discussion
4.1. Main Contributions of the Present Work
4.2. Average HR, HR Response, and Time Domain HRV Indices
4.3. Frequency Domain HRV Indices
4.4. Nonlinear HRV Indices
4.5. Pathophysiological and Clinical Implications
4.6. Perspectives
4.7. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Varadhan, R.; Seplaki, C.; Xue, Q.; Bandeen-Roche, K.; Fried, L. Stimulus-response paradigm for characterizing the loss of resilience in homeostatic regulation associated with frailty. Mech. Ageing Dev. 2008, 129, 666–670. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SAl Saedi, A.; Feehan, J.; Phu, S.; Duque, G. Current and emerging biomarkers of frailty in the elderly. Clin. Interv. Aging 2019, 14, 389–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsitz, L.A. Dynamics of Stability: The Physiologic Basis of Functional Health and Frailty. J. Gerontol. Ser. A 2002, 57, B115–B125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Hadley, E.C.; Walston, J.D.; Newman, A.B.; Guralnik, J.M.; Studenski, S.; Harris, T.B.; Ershler, W.B.; Ferrucci, L. From Bedside to Bench: Research Agenda for Frailty. Sci. Aging Knowl. Environ. 2005, 2005, pe24. [Google Scholar] [CrossRef]
- Ghachem, A.; Fried, L.P.; Legault, V.; Bandeen-Roche, K.; Presse, N.; Gaudreau, P.; Cohen, A.A. Evidence from two cohorts for the frailty syndrome as an emergent state of parallel dysregulation in multiple physiological systems. Biogerontology 2021, 22, 63–79. [Google Scholar] [CrossRef]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1966, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Chaves, P.H.M.; Varadhan, R.; Lipsitz, L.A.; Stein, P.K.; Windham, B.G.; Tian, J.; Fleisher, L.A.; Guralnik, J.M.; Fried, L.P. Physiological complexity underlying heart rate dynamics and frailty status in community-dwelling older women. J. Am. Geriatr. Soc. 2008, 56, 1698–1703. [Google Scholar] [CrossRef]
- Katayama, P.L.; Dias, D.P.M.; Silva, L.E.V.; Virtuoso-Junior, J.S.; Marocolo, M. Cardiac autonomic modulation in non-frail, pre-frail and frail elderly women: A pilot study. Aging Clin. Exp. Res. 2015, 27, 621–629. [Google Scholar] [CrossRef]
- Toosizadeh, N.; Ehsani, H.; Parthasarathy, S.; Carpenter, B.; Ruberto, K.; Mohler, J.; Parvaneh, S. Frailty and heart response to physical activity. Arch. Gerontol. Geriatr. 2021, 93, 104323. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ortuno, R.; Cogan, L.; O’Shea, D.; Lawlor, B.A.; Kenny, R.A. Orthostatic haemodynamics may be impaired in frailty. Age Ageing 2011, 40, 576–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, C.O.; Hoenig, H.H.; Varadhan, R.; Simonsick, E.M.; Fried, L.P. Relationships of Cardiac, Pulmonary, and Muscle Reserves and Frailty to Exercise Capacity in Older Women. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Varadhan, R.; Chaves, P.H.M.; Lipsitz, L.A.; Stein, P.K.; Tian, J.; Windham, B.G.; Berger, R.D.; Fried, L.P. Frailty and impaired cardiac autonomic control: New insights from principal components aggregation of traditional heart rate variability indices. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 682–687. [Google Scholar] [CrossRef]
- Newman, A.B.; Simonsick, E.M.; Naydeck, B.L.; Boudreau, R.M.; Kritchevsky, S.B.; Nevitt, M.C.; Pahor, M.; Satterfield, S.; Brach, J.S.; Studenski, S.A.; et al. Association of long-distance corridor walk performance with mortality, cardiovascular disease, mobility limitation, and disability. JAMA 2006, 295, 2018–2026. [Google Scholar] [CrossRef] [Green Version]
- Lopez, D.; Flicker, L.; Dobson, A. Validation of the frail scale in a cohort of older Australian women. J. Am. Geriatr. Soc. 2012, 60, 171–173. [Google Scholar] [CrossRef]
- Ibikunle, A.F.; Adedoyin, R.A.; Awotidebe, T.; Fasakin, O.M.; Okonj, A.M.; Odettunde, M. Validation of Three-Minute Walk Test for the Assessment of Functional Capacity among Patients with Hypertension. J. Clin. Exp. Cardiolog. 2020, 11, 662. [Google Scholar]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait Speed and Survival in Older Adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Nazari, G.; Bobos, P.; MacDermid, J.C.; Sinden, K.E.; Richardson, J.; Tang, A. Psychometric properties of the Zephyr bioharness device: A systematic review. BMC Sports Sci. Med. Rehabil. 2018, 10, 6. [Google Scholar] [CrossRef] [Green Version]
- Kubios HRV. Available online: https://www.kubios.com/ (accessed on 11 April 2022).
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef]
- Tarvainen, M.P. Biosignal Analysis and Medical Imaging Group (BSAMIG); Department of Applied Physics, University of Eastern Finland: Kuopio, Finland; Available online: https://uefconnect.uef.fi/en/group/biosignal-analysis-and-medical-imaging-research-group-bsamig/ (accessed on 11 April 2022).
- Tarvainen, M.P.; Ranta-Aho, P.O.; Karjalainen, P. An advanced detrending method with application to HRV analysis. IEEE Trans. Biomed. Eng. 2002, 49, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Niskanen, J.-P.; Tarvainen, M.P.; Ranta-Aho, P.O.; Karjalainen, P.A. Software for advanced HRV analysis. Comput. Methods Programs Biomed. 2004, 76, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Tarvainen, M.P.; Niskanen, J.-P.; Lipponen, J.A.; Ranta-Aho, P.O.; Karjalainen, P.A. Kubios HRV—Heart rate variability analysis software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Lipponen, J.A.; Tarvainen, M.P. A robust algorithm for heart rate variability time series artefact correction using novel beat classification. J. Med. Eng. Technol. 2019, 43, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Millán, L.A.; Castillo-Castillo, D.; Pérez-Pacheco, A.; Quispe-Siccha, R.; Angelova, M.; Rivera-Sánchez, J.; Fossion, R. Time-series based evaluation of physiological alterations in age-associated frailty during walking at self-selected velocity. AIP Conf. Proc. 2019, 2090, 050002. [Google Scholar] [CrossRef]
- Marple, S.L. Digital Spectral Analysis; Prentice-Hall International: Hoboken, NJ, USA, 1987. [Google Scholar]
- Tulppo, M.P.; Mäkikallio, T.H.; Takala, T.E.; Seppänen, T.; Huikuri, H.V. Quantitative beat-to-beat analysis of heart rate dynamics during exercise. Am. J. Physiol. 1996, 271 Pt 2, H244–H252. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [Green Version]
- Peng, C.K.; Havlin, S.; Stanley, H.E.; Goldberger, A.L. Quantification of scaling exponents and crossover phenomena in nonstationary heartbeat time series. Chaos 1995, 5, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Michael, S.; Graham, K.S.; Davis, G.M. Cardiac Autonomic Responses during Exercise and Post-exercise Recovery Using Heart Rate Variability and Systolic Time Intervals—A Review. Front. Physiol. 2017, 8, 301. [Google Scholar] [CrossRef] [Green Version]
- Gourine, A.V.; Ackland, G.L. Cardiac Vagus and Exercise. Physiology 2019, 34, 71–80. [Google Scholar] [CrossRef]
- Almeida-Santos, M.A.; Barreto-Filho, J.A.; Oliveira, J.L.; Reis, F.P.; Oliveira, C.C.D.C.; Sousa, A.C.S. Aging, heart rate variability and patterns of autonomic regulation of the heart. Arch. Gerontol. Geriatr. 2016, 63, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Umetani, K.; Singer, D.H.; McCraty, R.; Atkinson, M. Twenty-Four Hour Time Domain Heart Rate Variability and Heart Rate: Relations to Age and Gender Over Nine Decades. J. Am. Coll. Cardiol. 1998, 31, 593–601. [Google Scholar] [CrossRef]
- Takahashi, A.C.D.M.; Bonjorni, L.A.; Buto, M.S.S.; Vassimon-Barroso, V.; Minatel, V.; Rocha, S.M.A.; Ribeiro, F.H.M.; Montano, N.; Porta, A.; Catai, A.M. Short-term complexity of cardiovascular oscillations in frailty syndrome. In Proceedings of the 8th Conference of the European Study Group on Cardiovascular Oscillations (ESGCO), Trento, Italy, 25–28 May 2014; pp. 21–22. [Google Scholar] [CrossRef]
- Lipsitz, L.A. Physiological complexity, aging, and the path to frailty. Sci. Aging Knowl. Environ. 2004, 2004, pe16. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishna, R.; Dutt, D.N.; Yeragani, V.K. Nonlinear measures of heart rate time series: Influence of posture and controlled breathing. Auton. Neurosci. 2000, 83, 148–158. [Google Scholar] [CrossRef]
- Vuksanović, V.; Gal, V. Nonlinear and chaos characteristics of heart period time series: Healthy aging and postural change. Auton. Neurosci. 2005, 121, 94–100. [Google Scholar] [CrossRef]
- Parvaneh, S.; Howe, C.; Toosizadeh, N.; Honarvar, B.; Slepian, M.J.; Fain, M.; Mohler, J.; Najafi, B. Regulation of Cardiac Autonomic Nervous System Control across Frailty Statuses: A Systematic Review. Gerontology 2015, 62, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Walston, J.; Hadley, E.C.; Ferrucci, L.; Guralnik, J.M.; Newman, A.B.; Studenski, S.A.; Ershler, W.B.; Harris, T.; Fried, L.P. Research agenda for frailty in older adults: Toward a better understanding of physiology and etiology: Summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J. Am. Geriatr. Soc. 2006, 54, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Martínez, O.M.; Fossion, R.; Piceno, Y.G.; Lopez-Gomez, R.E.; López-Espinosa, E.; Jiménez-Estrada, I.; Quiroz-González, S. Heart Rate Variability and Psychometric Analysis in Patients with Hyperactive Heart Fire Syndrome. J. Acupunct. Meridian Stud. 2021, 14, 137–148. [Google Scholar] [CrossRef]
- Kabbach, E.Z.; Mazzuco, A.; Borghi-Silva, A.; Cabiddu, R.; Agnoleto, A.G.; Barbosa, J.F.; Junior, L.C.S.D.C.; Mendes, R.G. Increased parasympathetic cardiac modulation in patients with acute exacerbation of COPD: How should we interpret it? Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 2221–2230. [Google Scholar] [CrossRef] [Green Version]
- Hopf, H.-B.; Skyschally, A.; Heusch, G.; Peters, J. Low-frequency Spectral Power of Heart Rate Variability Is Not a Specific Marker of Cardiac Sympathetic Modulation. Anesthesiology 1995, 82, 609–619. [Google Scholar] [CrossRef]
- Ishaque, S.; Khan, N.; Krishnan, S. Trends in Heart-Rate Variability Signal Analysis. Front. Digit. Health 2021, 3, e639444. [Google Scholar] [CrossRef] [PubMed]
- Eskandari-Nojehdehi, M.; Parvaneh, S.; Ehsani, H.; Fain, M.; Toosizadeh, N. Frailty Identification using Heart Rate Dynamics: A Deep Learning Approach. IEEE J. Biomed. Health Inform. 2022. [Google Scholar] [CrossRef] [PubMed]
- Ruberto, K.; Ehsani, H.; Parvaneh, S.; Mohler, J.; Fain, M.; Sweitzer, N.K.; Toosizadeh, N. The association between heart rate behavior and gait performance: The moderating effect of frailty. PLoS ONE 2022, 17, e0264013. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | C1 | C2 | nF | F |
|---|---|---|---|---|
| (n = 21) | (n = 16) | (n = 15) | (n = 28) | |
| Age (years) | 22.0 ± 1.4 | 48.6 ± 8.9 * | 71.5 ± 8.2 *,** | 78 ± 5.4 *,**,|| |
| Sex | ||||
| Male | 9 (43%) | 6 (38%) | 9 (60%) | 8 (29%) |
| Female | 12 (57%) | 10 (62%) | 6 (40%) | 20 (71%) |
| Body mass index (kg/m2) | 23.8 ± 3.6 | 27.5 ± 5.9 | 27.4 ± 3.6 * | 26.4 ± 3.9 * |
| Physical activity | ||||
| Mild | 9 (43%) | 8 (50%) | 0 (0%) | 2 (7%) |
| Moderate | 12 (57%) | 8 (50%) | 6 (40%) | 20 (71%) |
| Comorbidities | ||||
| Hypertension | 0 | 3 | 4 | 15 |
| Mild cognitive | 0 | 0 | 0 | 14 |
| Diabetes | 0 | 0 | 2 | 10 |
| Depression | 0 | 0 | 2 | 9 |
| C1 (n = 21) | C2 (n = 16) | nF (n = 15) | F (n = 28) | p-Value | |
|---|---|---|---|---|---|
| Baseline | |||||
| HR (1/min) (bpm) | 81.2 (69.9–89.9) | 74.2 (65.1–84.4) | 76.4 (65.9–82.5) | 74.1 (67.2–84.5) | 0.462 |
| Mean RR (ms) | 747 (672–866) | 811 (713–924) | 788 (736–912) | 811 (721–908) | 0.540 |
| SDNN (ms) | 61.5 (46.7–76.4) | 48.6 (35.3–63.8) | 29.6 (27.6–46.7) **,|| | 33.2 (20.6–57.2) **,|| | 0.000 # |
| CV (%) | 82.5 (53.8–98.6) | 68.5 (46.8–102.0) | 42.9 (33.1–68.1) **,|| | 46.0 (26.5–88.6) ** | 0.007 # |
| RMSSD (ms) | 33.5 (25.5–42.1) | 27.9 (17.3–39.5) | 13.5 (7.7–25.7) **,|| | 22.4 (9.7–71.8) | 0.010 # |
| pNN30 (%) | 34.3 (24.6–45.1) | 22.4 (13.7–35.9) | 4.6 (1.2–32.6) ** | 3.7 (7.6–26.6) ** | 0.006 # |
| pNN50 (%) | 12 (3.00–22.00) | 6 (1.00–16.00) | 1 (0.00–7.00) **,|| | 2 (0.00–12.00) **,¶ | 0.004 # |
| LF (ms2) | 1202.5 (1066.2–1842.6) | 531.1 (473.5–1464.4) ** | 172.9 (74.5–916.0) **,|| | 167.8 (53.6–1041.0) **,|| | 0.000 # |
| HF (ms2) | 380.5 (247.1–1263.6) | 275.7 (176.9–617.7) | 67.5 (38.5–201.1) **,|| | 97.4 (186.8–2130.0) ** | 0.002 # |
| LF (nu) | 75.5 (64–85.5) | 74.0 (57.5–87.9) | 81.3 (69.0–89.3) | 59.8 (34.0–77.1) **,||,¶ | 0.011 # |
| HF (nu) | 24.0 (14.4–35.8) | 26.0 (12.0–42.4) | 18.6 (10.7–31.0) | 40.1 (22.9–64.9) **,||,¶ | 0.010 # |
| LF/HF | 3.14 (1.79–5.93) | 2.84 (1.35–7.33) | 4.38 (2.23–8.38) | 1.49 (0.52–3.37) **,||,¶ | 0.010 # |
| EDR (Hz) | 0.2 (0.16–0.21) | 0.18 (0.17–0.19) | 0.17 (0.14–0.19) | 0.19 (0.16–0.22) ¶ | 0.214 |
| Recovery | |||||
| HR (1/min) | 77.2 (67.00–88.2) * | 75.5 (61.7–86.2) | 75.2 (66.0–79.5) | 78.6 (69.1–87.6) * | 0.582 |
| Mean RR (ms) | 786 (685–900) * | 811 (700–983) | 801 (757–914) | 766 (694–873) * | 0.619 |
| SDNN (ms) | 59.1 (52.6–82.4) | 51.2 (42.4–61.7) ** | 29.7 (19.1–37.2) **,|| | 28.0 (21.9–49.6) **,|| | 0.000 # |
| CV (%) | 75.5 (58.8–122.3) | 68.5 (49.0–96.4) | 39.6 (24.5–58.0) **,|| | 41.1 (24.6–72.3) **,|| | 0.000 # |
| RMSSD (ms) | 37.9 (29.7–46.1) | 35.1 (14.4–39.0) | 15.0 (12.5–21.9) **,|| | 16.5 (8.3–58.7) ** | 0.003 # |
| pNN30 (%) | 39.7 (30.5–51.5) | 30.7 (17.5–44.8) | 4.4 (1.7–18.2) **,|| | 2.8 (5.4–20.9) **,|| | 0.000 # |
| pNN50 (%) | 16.00 (10.00–26.00) * | 12.00 (1.00–20.00) | 0.00 (0.00–2.00) **,|| | 1.00 (0.00–22.00) ** | 0.000 # |
| LF (ms2) | 1564.1 (1234.8–2595.7) | 916.5 (617.3–1414.6) ** | 362.7 (180.6–646.5) **,|| | 138.1 (144.6–950.7) **,|| | 0.000 # |
| HF (ms2) | 601.2 (482.0–1301.4) | 319.9 (221.5–651.6) | 77.0 (21.9–259.9) **,|| | 65.3 (189.5–1066.9) ** | 0.001 # |
| LF (nu) | 73.3 (60.4–80.1) | 77.0 (45.1–89.4) | 81.5 (68.5–86.5) | 68.8 (42.6–77.6) ¶ | 0.098 |
| HF (nu) | 26.7 (19.6–39.5) | 23.0 (10.6–54.9) | 18.4 (13.4–31.1) | 31.3 (22.3–57.2) ¶ | 0.101 |
| LF/HF | 2.74 (1.53–4.08) | 3.35 (0.82–8.43) | 4.49 (2.20–6.44) | 2.19 (0.75–3.47) ¶ | 0.102 |
| EDR (Hz) | 0.19 (0.16–0.23) | 0.17 (0.16–0.19) | 0.17 (0.13–0.19) | 0.18 (0.16–0.22) | 0.431 |
| HR response | |||||
| 39.0 (33.1–48.2) | 42 (29.8–59.6)) | 54 (26.3–84.7) | 115 (96.5–175.3) **,||,¶ | 0.000 # | |
| 107.0 (101.4–114.4) | 104.2 (91.2–107.9) | 98.3 (90.9–103.4) ** | 88.3 (87.1–100.2) | 0.013 # | |
| 2.4 (2.3–4.1) | 2.5 (1.5–5.1) | 1.8 (1.0–6.7) | 0.7 (0.6–1.9) **,||,¶ | 0.000 # | |
| (%) | 20.0 (12.2– 24.9) | 16.5 (−11.3–28.6) | 16.4 (1.3–26.2) | 15.2 (8.6–23.1) | 0.734 |
| (%) | −19.5 (−12.7–−23.3) | −15.9 (−10.1–−25.4) | −16.2 (−11.9–−26.2) | −8.8 (−5.0–36.9) **,||,¶ | 0.002 # |
| (%) | −3.9 (−4.9–−0.9) | 0.1 (−2.8–3.4) | 0.4 (−4.3–3.4) | 4.3 (0.5–8.6) **,||,¶ | 0.001 # |
| C1 (n = 21) | C2 (n = 16) | Nf (n = 15) | F (n = 28) | p-Value | |
|---|---|---|---|---|---|
| Baseline | |||||
| SD1 (ms) | 23.7 (18.0–29.8) | 19.8 (12.3–28.0) | 9.5 (5.4–18.2) **,|| | 15.9 (6.9–50.8) | 0.010 # |
| SD2 (ms) | 81.7 (64.3–104.1) | 67.0 (48.4–87.6) | 39.8 (38.4–63.1) **,|| | 39.8 (27.1–73.7) **,|| | 0.000 # |
| SD1/SD2 | 0.3 (0.2–0.4) | 0.3 (0.2–0.4) | 0.2 (0.2–0.3) | 0.3 (0.2–0.8) | 0.136 |
| ApEn | 1.11 (1.03–1.19) | 1.07 (1.03–1.13) | 1.04 (0.97–1.14) | 1.02 (0.95–1.11) ** | 0.149 |
| SampEn | 1.35 (1.18–1.63) | 1.27 (1.11–1.64) | 1.18 (1.03–1.51) | 1.16 (0.96–1.39) ||,¶ | 0.353 |
| α1 | 1.37 (1.16–1.47) | 1.40 (1.06–1.66) | 1.41 (1.26–1.57) | 1.08 (0.63–1.35) **,||,¶ | 0.006 # |
| Recovery | |||||
| SD1 (ms) | 26.8 (21.0–32.7) | 24.9 (10.2–27.6) | 10.6 (8.9–15.5) **,|| | 11.7 (5.8–41.6) ** | 0.003 # |
| SD2 (ms) | 79.8 (68.8–109.9) | 71.7 (54.6–74.4) ** | 40.5 (26.5–51.5) **,|| | 38.5 (30.1–61.6) **,|| | 0.000 # |
| SD1/SD2 | 0.3 (0.2–0.4) | 0.3 (0.2–0.5) | 0.3 (0.2–0.4) | 0.3 (0.2–0.8) | 0.381 |
| ApEn | 1.12 (0.97–1.17) | 1.06 (0.92–1.12) | 1.12 (1.01–1.18) | 1.02 (0.91–1.13) | 0.184 |
| SampEn | 1.52 (1.25–1.67) | 1.22 (0.94–1.71) | 1.39 (1.14–1.69) * | 1.21 (0.96–1.37) **,¶ | 0.065 |
| α1 | 1.27 (1.09–1.37) * | 1.40 (0.88–1.54) | 1.37 (1.18–1.51) | 1.17 (0.79–1.32) ¶ | 0.075 |
| AUC (95% CI) | p-Value | Best Cut off Value | |
|---|---|---|---|
| Baseline | |||
| pNN50 (%) | 0.583 (0.408–0.758) | 0.386 | 0.8 |
| LF (nu) | 0.765 (0.609–0.922) | 0.080 | 77.3 |
| HF (nu) | 0.768 (0.612–0.924) | 0.005 | 22.6 |
| LF/HF | 0.768 (0.612–0.924) | 0.005 | 3.4 |
| EDR (Hz) | 0.686 (0.526–0.847) | 0.051 | 0.2 |
| SampEn (beats) | 0.597 (0.420–0.774) | 0.090 | 1.2 |
| α1 | 0.745 (0.891–0.599) | 0.010 | 1.2 |
| Recovery | |||
| LF (nu) | 0.722 (0.554–0.890) | 0.020 | 78.6 |
| HF (nu) | 0.722 (0.554–0.890) | 0.020 | 21.4 |
| LF/HF | 0.722 (0.554–0.890) | 0.020 | 3.7 |
| SampEn | 0.724 (0.564–0.885) | 0.019 | 1.3 |
| α1 | 0.717 (0.557–0.876) | 0.023 | 1.2 |
| HR response | |||
| Δt (s) | 0.807 (0.652–0.962) | 0.006 | 74 |
| (bpm/s) | 0.824 (0.678–0.970) | 0.000 | 1.2 |
| ΔHRRB | 0.707 (0.544–0.870) | 0.083 | −3.8 |
| Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | |
|---|---|---|---|---|
| Baseline | ||||
| pNN50 > 0.8% | 43 (25–61) | 43 (17–69) | 60 (39–81) | 27 (9–46) |
| LF < 77.3 nu | 82 (68–96) | 71 (48–95) | 85 (72–99) | 67 (43–91) |
| HF >22.6 nu | 18 (4–32) | 29 (5–52) | 33 (9–57) | 15 (1–28) |
| LF/HF > 3.4 | 82 (68–96) | 71 (48–95) | 85 (72–99) | 67 (43–91) |
| EDR (Hz) > 0.2 | 36 (18–53) | 36 (11–61) | 53 (30–75) | 22 (5–39) |
| SampEn > 1.2 | 54 (35–72) | 64 (39–89) | 75 (56–94) | 41 (20–61) |
| α1 > 1.2 | 61 (43–79) | 86 (67–104) | 89 (76–103) | 52 (32–73) |
| Recovery | ||||
| LF < 78.6 nu | 79 (63–94) | 57 (31–83) | 79 (63–94) | 57 (31–83) |
| HF > 21.3 nu | 21 (6–37) | 43 (17–69) | 43 (17–69) | 21 (6–37) |
| LF/HF > 3.7 | 79 (63–94) | 57 (31–83) | 79 (63–94) | 57 (31–83) |
| SampEn > 1.3 | 71 (55–88) | 64 (39–89) | 80 (64–96) | 53 (29–77) |
| α1 > 1.2 | 64 (47–82) | 79 (57–100) | 86 (71–101) | 52 (31–74) |
| HR response | ||||
| Δt (s) | 81 (64–98) | 70 (42–98) | 85 (69–101) | 64 (35–92) |
| (bpm/s) | 76 (58–94) | 70 (42–98) | 84 (68–101) | 58 (30–86) |
| ΔHR > −3.6 | 54 (35–72) | 86 (67–104) | 88 (73–104) | 48 (28–68) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Álvarez-Millán, L.; Lerma, C.; Castillo-Castillo, D.; Quispe-Siccha, R.M.; Pérez-Pacheco, A.; Rivera-Sánchez, J.; Fossion, R. Chronotropic Response and Heart Rate Variability before and after a 160 m Walking Test in Young, Middle-Aged, Frail, and Non-Frail Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 8413. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19148413
Álvarez-Millán L, Lerma C, Castillo-Castillo D, Quispe-Siccha RM, Pérez-Pacheco A, Rivera-Sánchez J, Fossion R. Chronotropic Response and Heart Rate Variability before and after a 160 m Walking Test in Young, Middle-Aged, Frail, and Non-Frail Older Adults. International Journal of Environmental Research and Public Health. 2022; 19(14):8413. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19148413
Chicago/Turabian StyleÁlvarez-Millán, Lesli, Claudia Lerma, Daniel Castillo-Castillo, Rosa M. Quispe-Siccha, Argelia Pérez-Pacheco, Jesús Rivera-Sánchez, and Ruben Fossion. 2022. "Chronotropic Response and Heart Rate Variability before and after a 160 m Walking Test in Young, Middle-Aged, Frail, and Non-Frail Older Adults" International Journal of Environmental Research and Public Health 19, no. 14: 8413. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19148413