
Czech and Slovak Dental Students’ Oral Health-Related Knowledge, Attitudes, and Behaviours (KAB): Multi-Country Cross-Sectional Study

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
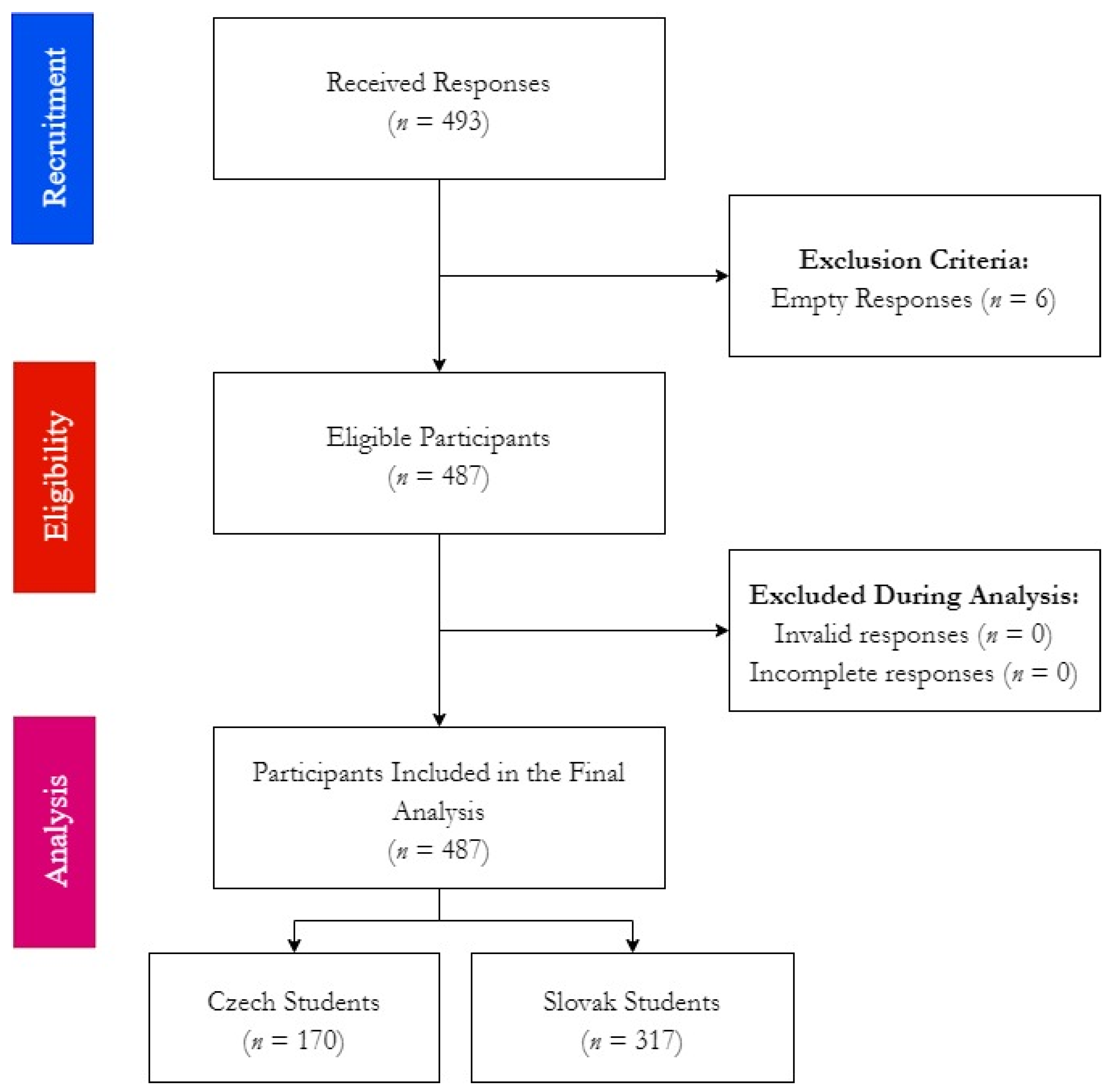
2.2. Participants
2.3. Instrument
2.3.1. HU-DBI Scoring System
2.3.2. Czech HU-DBI
2.3.3. Slovak HU-DBI
2.4. Ethics
2.5. Analyses
3. Results
3.1. Demographic Characteristics
3.2. Health Behaviours
3.3. HU-DBI Responses
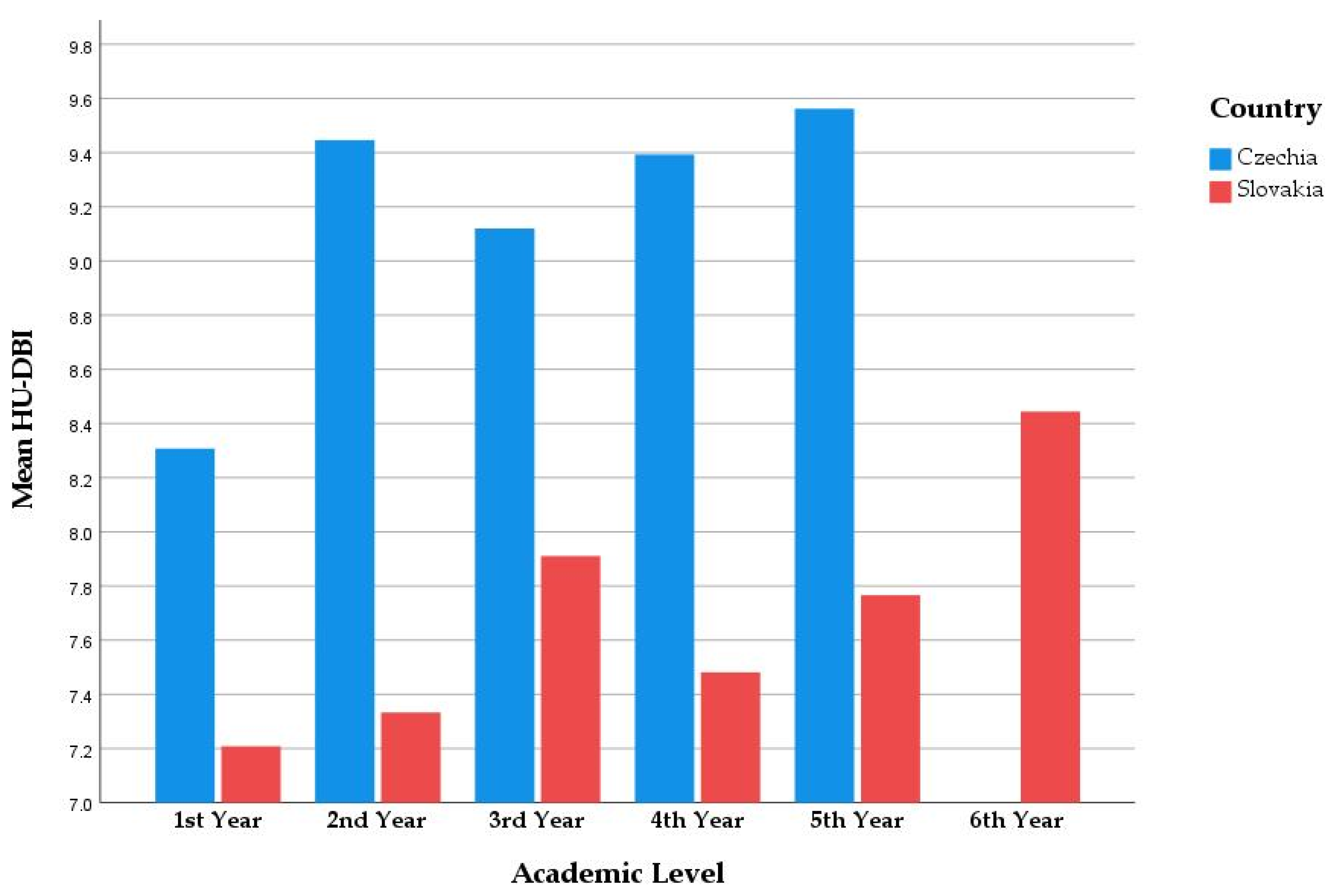
3.3.1. Academic Level
3.3.2. Gender
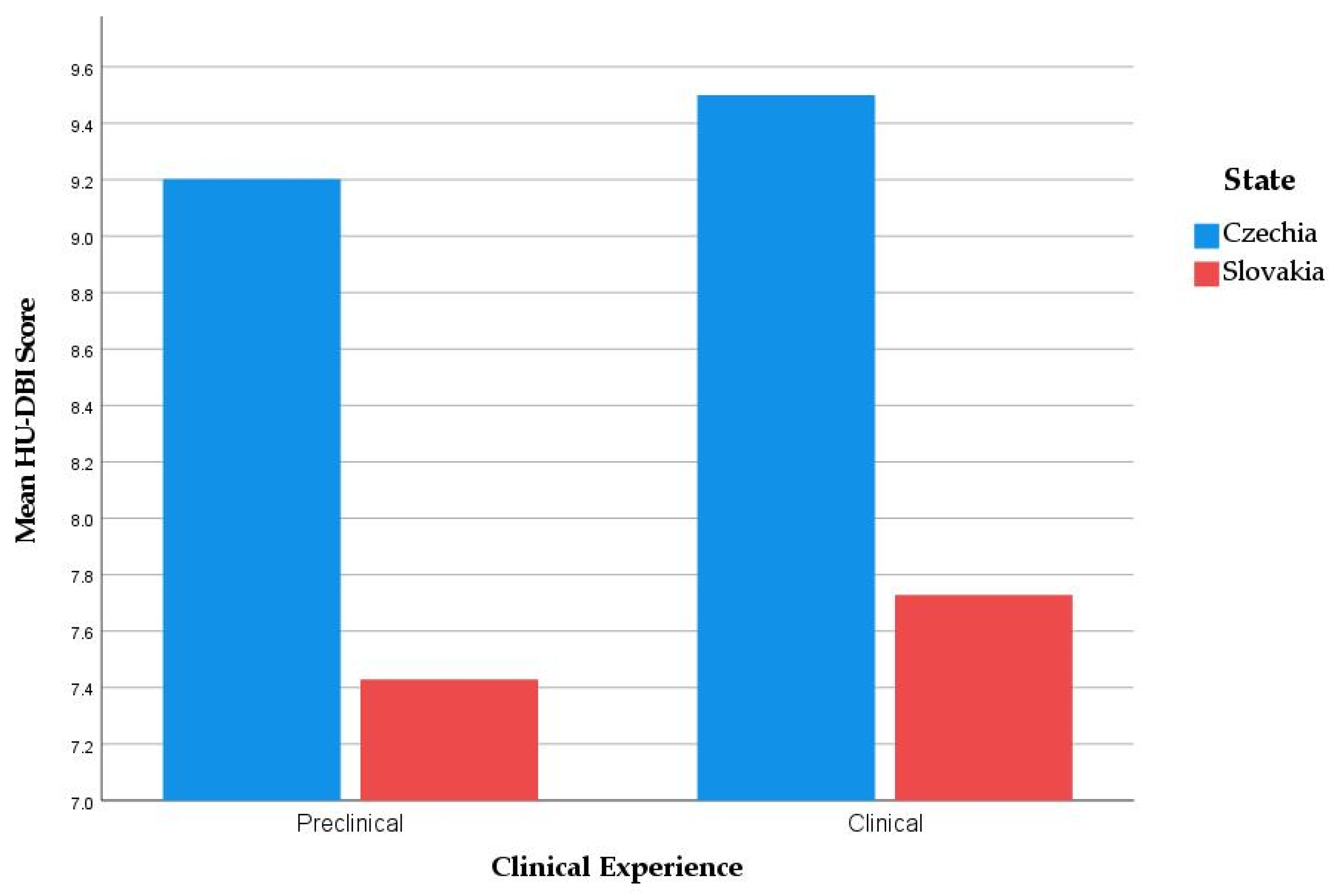
3.3.3. Clinical Experience
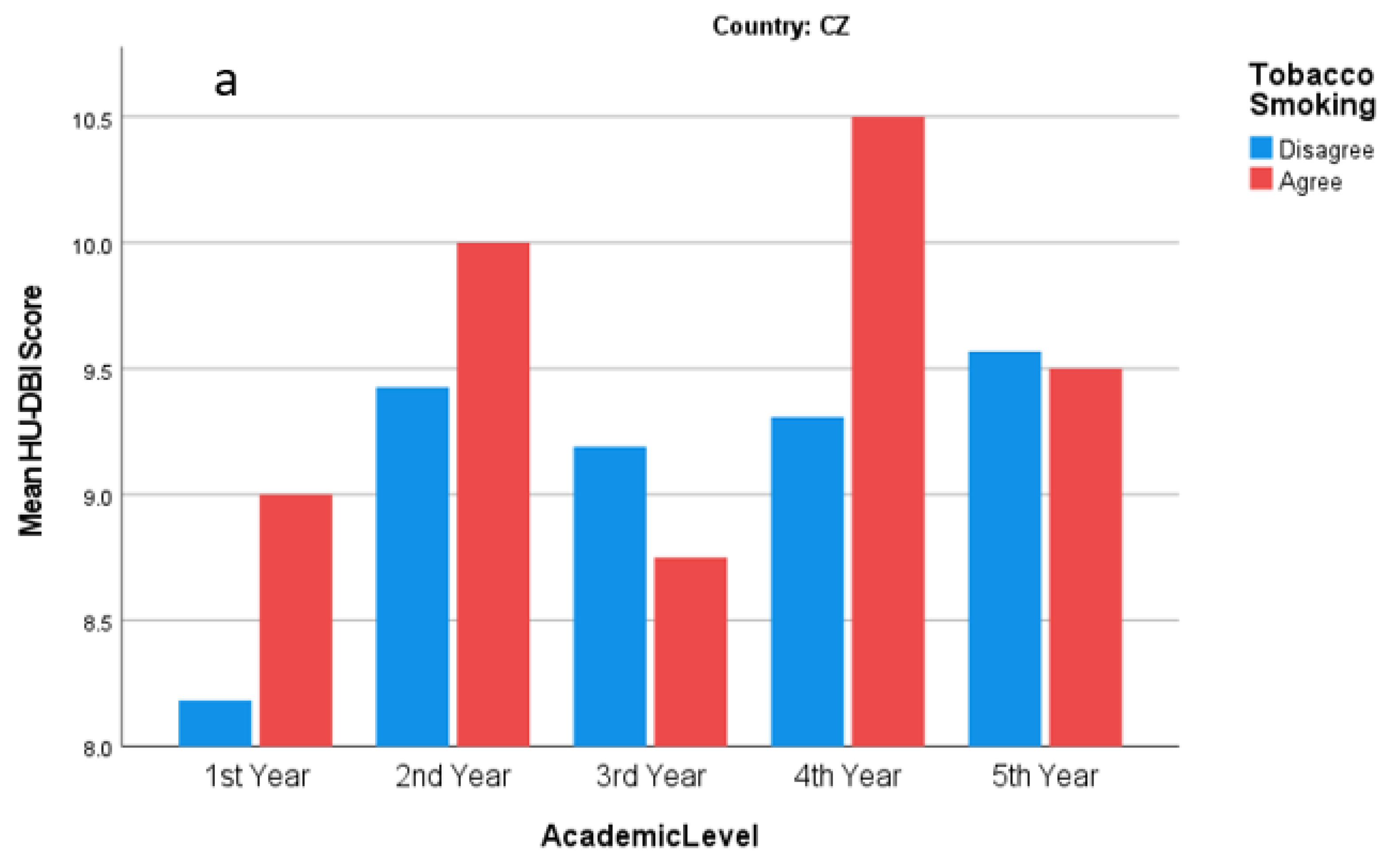
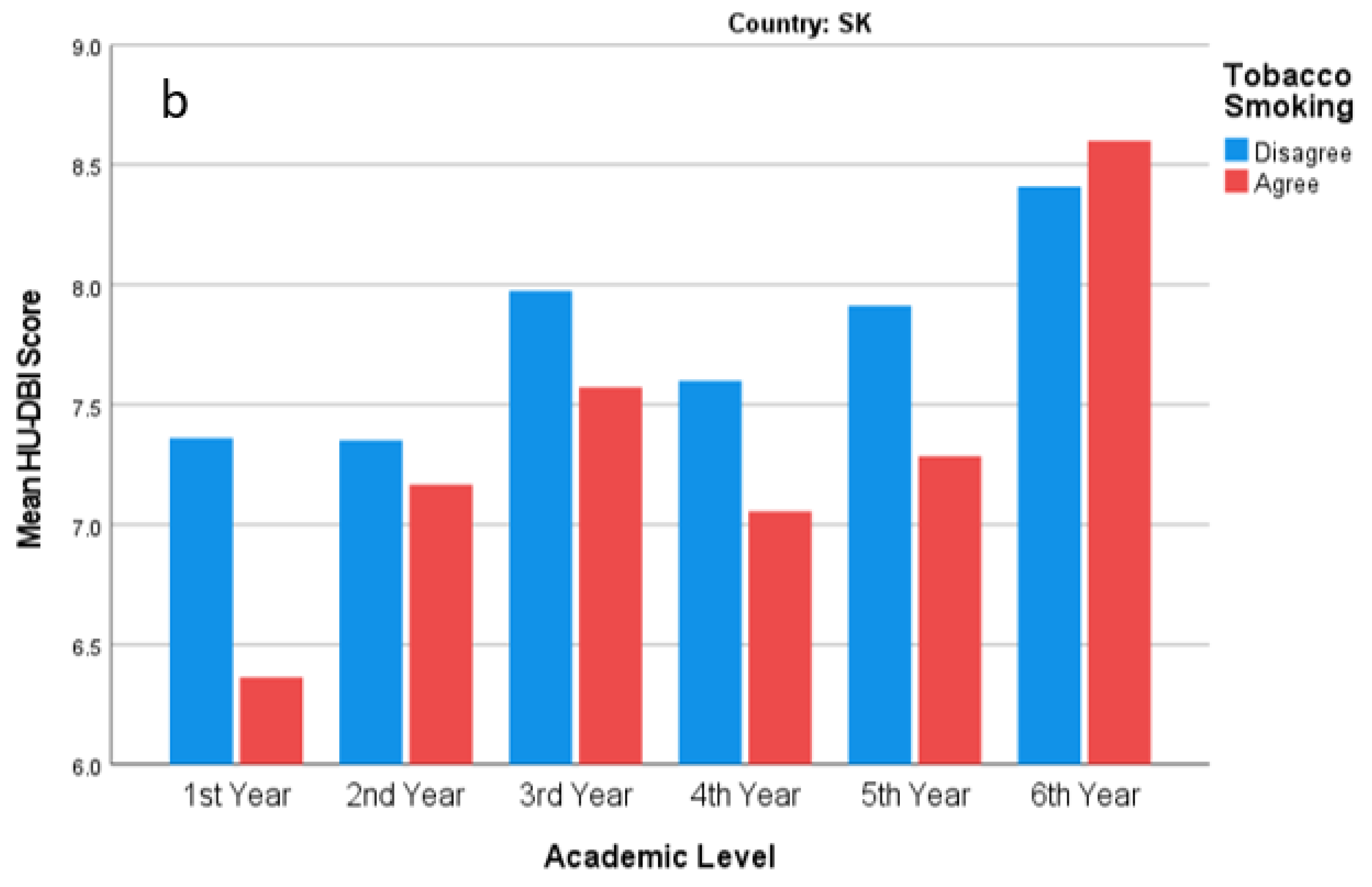
3.3.4. Tobacco Smoking
3.4. HU-DBI Scores
3.4.1. Czech Students
3.4.2. Slovak Students
3.5. Year-Over-Year Analysis
3.5.1. Czech Students
3.5.2. Slovak Students
3.6. Regression Analysis of State
3.7. Regression Analysis of Tobacco Smoking
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Language | Question Otázka Otázka | Agree Souhlasím Súhlasím | Disagree Nesouhlasím Nesúhlasím |
|---|---|---|---|---|
| 1 | EN | I do not worry much about visiting the dentist. | □ | □ |
| CZ | Nemám moc velký strach z návštěvy zubaře. | □ | □ | |
| SK | Nezáleží mi na návštevách u zubného lekára. | □ | □ | |
| 2 | EN | My gum tends to bleed when I brush my teeth. | □ | □ |
| CZ | Když si čistím zuby, moje dásně mají sklon krvácet. | □ | □ | |
| SK | Moje ďasná majú tendenciu krvácať pri čistení zubov. | □ | □ | |
| 3 | EN | I worry about the color of my teeth. | □ | □ |
| CZ | Záleží mi na barvě mých zubů. | □ | □ | |
| SK | Záleží mi na farbe mojich zubov. | □ | □ | |
| 4 | EN | I have noticed some white sticky deposits on my teeth. | □ | □ |
| CZ | Všiml(a) jsem si bílých lepivých nánosů na mých zubech. | □ | □ | |
| SK | Všimla/všimol som si biele usadeniny na mojich zuboch. | □ | □ | |
| 5 | EN | I use a child sized toothbrush. | □ | □ |
| CZ | Používám zubní kartáček s malou hlavičkou. | □ | □ | |
| SK | Používam zubnú kefku detskej veľkosti. | □ | □ | |
| 6 | EN | I think that I cannot help having false teeth when I am old. | □ | □ |
| CZ | Myslím si, že ve stáří budu nosit zubní protézy a nemůžu s tím nic dělat. | □ | □ | |
| SK | Myslím, že sa v budúcnosti nevyhnem noseniu protézy. | □ | □ | |
| 7 | EN | I am bothered by the color of my gum. | □ | □ |
| CZ | Vadí mi barva mých dásní. | □ | □ | |
| SK | Trápi ma farba mojich ďasien. | □ | □ | |
| 8 | EN | I think my teeth are getting worse despite my daily brushing. | □ | □ |
| CZ | Myslím si, že stav mých zubů se zhoršuje, i přesto, že si je každý den čistím. | □ | □ | |
| SK | Aj napriek dennému čisteniu zubov mám pocit, že sa stav mojich zubov zhoršuje. | □ | □ | |
| 9 | EN | I brush each of my teeth carefully. | □ | □ |
| CZ | Pečlivě si čistím každý zub zvlášť. | □ | □ | |
| SK | Čistím si poctivo každý zub. | □ | □ | |
| 10 | EN | I have never been taught professionally how to brush. | □ | □ |
| CZ | Nikdy jsem nebyl(a) odborně poučen(a), jak si mám čistit zuby. | □ | □ | |
| SK | Nikdy som neabsolvoval sedenie s hygienistkou ohľadom správnej techniky čistenia zubov. | □ | □ | |
| 11 | EN | I think I can clean my teeth well without using toothpaste. | □ | □ |
| CZ | Myslím si, že si mohu dobře vyčistit zuby i bez použití zubní pasty. | □ | □ | |
| SK | Myslím, že si viem dobre vyčistiť zuby bez použitia zubnej pasty. | □ | □ | |
| 12 | EN | I often check my teeth in a mirror after brushing. | □ | □ |
| CZ | Po čištění často kontroluji své zuby v zrcadle. | □ | □ | |
| SK | Často si kontrolujem zuby po vyčistení v zrkadle. | □ | □ | |
| 13 | EN | I worry about having bad breath. | □ | □ |
| CZ | Mám obavy, že je mi cítit z úst. | □ | □ | |
| SK | Obávam sa halitózy. | □ | □ | |
| 14 | EN | It is impossible to prevent gum disease with tooth brushing alone. | □ | □ |
| CZ | Není možné předcházet onemocnění dásní pouze pomocí čištění zubů. | □ | □ | |
| SK | Je nemožné predísť gingivitíde len s čistením zubov zubnou kefkou. | □ | □ | |
| 15 | EN | I put off going to dentist until I have a toothache. | □ | □ |
| CZ | Odkládám návštěvu zubního lékaře, dokud mě zuby nebolí. | □ | □ | |
| SK | Odkladám návštevu zubára až kým ma nezačnú bolieť zuby. | □ | □ | |
| 16 | EN | I have used a dye to see how clean my teeth are. | □ | □ |
| CZ | Použil(a) jsem barvící detektor plaku, abych si zkontroloval(a), jak jsou mé zuby vyčištěné. | □ | □ | |
| SK | Použil som v minulosti plak indikátor na zlepšenie orálnej hygieny. | □ | □ | |
| 17 | EN | I use a toothbrush which has hard bristles. | □ | □ |
| CZ | Používám kartáček s tvrdými štětinami. | □ | □ | |
| SK | Používam zubnú kefku s tvrdými štetinami. | □ | □ | |
| 18 | EN | I do not feel I have brushed well unless I brush with hard strokes. | □ | □ |
| CZ | Nemám pocit vyčištěných zubů, pokud na kartáček hodně netlačím. | □ | □ | |
| SK | Nemám pocit čistých zubov pokiaľ netlačím na zubnú kefku. | □ | □ | |
| 19 | EN | I feel I sometimes take too much time to brush my teeth. | □ | □ |
| CZ | Někdy mám pocit, že mi čištění zubů bere příliš mnoho času. | □ | □ | |
| SK | Mám pocit, že umývanie zubov mi zaberá príliš veľa času. | □ | □ | |
| 20 | EN | I have had my dentist tell me that I brush very well. | □ | □ |
| CZ | Můj zubní lékař mi řekl, že si čistím zuby velmi dobře. | □ | □ | |
| SK | Zubný lekár ma pochválil za orálnu hygiene. | □ | □ | |
| 21 | EN | I find myself using my smartphone/compute longer than I planned. | □ | □ |
| CZ | Používám svůj smartphone nebo počítač déle, než jsem plánoval(a). | □ | □ | |
| SK | Používam svoj počítač alebo telefón dlhšie, než by som chcel. | □ | □ | |
| 22 | EN | I consume tobacco at least once a week. | □ | □ |
| CZ | Alespoň jednou týdně kouřím cigarety. | □ | □ | |
| SK | Minimálne jeden krát za týždeň užívam tabakové výrobky. | □ | □ | |
| 23 | EN | I drink alcohol at least once a week. | □ | □ |
| CZ | Alespoň jednou týdně mám alkoholický nápoj. | □ | □ | |
| SK | Minimálne jeden krát do týždňa pijem alkohol. | □ | □ | |
| 24 | EN | I go to the dentist/ hygienist for regular check-up at least once a year. | □ | □ |
| CZ | Alespoň jednou ročně navštěvuji zubního lékaře nebo dentální hygienistku. | □ | □ | |
| SK | Navštevujem zubného lekára/hygienistku minimálne jedenkrát za rok. | □ | □ |
References
- World Health Assembly Resolution Paves the Way for Better Oral Health Care. Available online: https://www.who.int/news/item/27-05-2021-world-health-assembly-resolution-paves-the-way-for-better-oral-health-care (accessed on 23 January 2022).
- Sheiham, A.; Watt, R.G. The Common Risk Factor Approach: A rational basis for promoting oral health. Community Dent. Oral Epidemiol. 2000, 28, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral Diseases: A Global Public Health Challenge; Elsevier: Amsterdam, The Netherlands, 2019; Volume 394, pp. 249–260. [Google Scholar]
- Jin, L.J.; Lamster, I.B.; Greenspan, J.S.; Pitts, N.B.; Scully, C.; Warnakulasuriya, S. Global burden of oral diseases: Emerging concepts, management and interplay with systemic health. Oral Dis. 2016, 22, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Migliorati, C.A.; Madrid, C. The interface between oral and systemic health: The need for more collaboration. Clin. Microbiol. Infect. 2007, 13, 11–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skaret, E.; Soevdsnes, E.K. Behavioural science in dentistry. The role of the dental hygienist in prevention and treatment of the fearful dental patient. Int. J. Dent. Hyg. 2005, 3, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Werner, H.; Hakeberg, M.; Dahlström, L.; Eriksson, M.; Sjögren, P.; Strandell, A.; Svanberg, T.; Svensson, L.; Wide Boman, U. Psychological Interventions for Poor Oral Health. J. Dent. Res. 2016, 95, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Schou, L. The relevance of behavioural sciences in dental practice. Int. Dent. J. 2000, 50, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, N.; Livny, A.; Chestnutt, I.; Virtanen, J.; Gallagher, J.E. Dental Public Health Education in Europe: A survey of European Dental Schools to determine current practice and inform a core undergraduate programme. Community Dent. Health 2020, 37, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Wagle, M.; Trovik, T.A.; Basnet, P.; Acharya, G. Do dentists have better oral health compared to general population: A study on oral health status and oral health behavior in Kathmandu, Nepal. BMC Oral Health 2014, 14, 23. [Google Scholar] [CrossRef] [Green Version]
- Ghaffari, M.; Rakhshanderou, S.; Ramezankhani, A.; Buunk-Werkhoven, Y.A.B.; Noroozi, M.; Armoon, B. Are educating and promoting interventions effective in oral health?: A systematic review. Int. J. Dent. Hyg. 2018, 16, 48–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, C.; Santos, N.M.L.; Hilgert, J.B.; Hugo, F.N. Effectiveness of oral health education on oral hygiene and dental caries in schoolchildren: Systematic review and meta-analysis. Community Dent. Oral Epidemiol. 2018, 46, 30–37. [Google Scholar] [CrossRef]
- Ucheka, P.; Cinar, A.B.; Ling, J.; Derek, R. A systematic review of the use of common behavioural interventions in oral health and diabetes management. Orapuh J. 2021, 2, e819. [Google Scholar] [CrossRef]
- de Silva, A.M.; Hegde, S.; Akudo Nwagbara, B.; Calache, H.; Gussy, M.G.; Nasser, M.; Morrice, H.R.; Riggs, E.; Leong, P.M.; Meyenn, L.K.; et al. Community-based population-level interventions for promoting child oral health. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef] [Green Version]
- Cooper, A.M.; O’Malley, L.A.; Elison, S.N.; Armstrong, R.; Burnside, G.; Adair, P.; Dugdill, L.; Pine, C. Primary school-based behavioural interventions for preventing caries. Cochrane Database Syst. Rev. 2013, 2013. [Google Scholar] [CrossRef]
- Langford, R.; Bonell, C.P.; Jones, H.E.; Pouliou, T.; Murphy, S.M.; Waters, E.; Komro, K.A.; Gibbs, L.F.; Magnus, D.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst. Rev. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Al-wesabi, A.A.; Abdelgawad, F.; Sasahara, H.; El Motayam, K. Oral health knowledge, attitude and behaviour of dental students in a private university. BDJ Open 2019, 5, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polychronopoulou, A.; Kawamura, M. Oral self-care behaviours: Comparing Greek and Japanese dental students. Eur. J. Dent. Educ. 2005, 9, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Komabayashi, T.; Kwan, S.Y.L.; Hu, D.Y.; Kajiwara, K.; Sasahara, H.; Kawamura, M. A comparative study of oral health attitudes and behaviour using the Hiroshima University—Dental Behavioural Inventory (HU-DBI) between dental students in Britain and China. J. Oral Sci. 2005, 47, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Stacey, F.; Heasman, P.A.; Heasman, L.; Hepburn, S.; McCracken, G.I.; Preshaw, P.M. Smoking cessation as a dental intervention—Views of the profession. Br. Dent. J. 2006, 201, 109–113. [Google Scholar] [CrossRef]
- Vollath, S.E.; Bobak, A.; Jackson, S.; Sennhenn-Kirchner, S.; Kanzow, P.; Wiegand, A.; Raupach, T. Effectiveness of an innovative and interactive smoking cessation training module for dental students: A prospective study. Eur. J. Dent. Educ. 2020, 24, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Monaghan, N. What is the role of dentists in smoking cessation? Br. Dent. J. 2002, 193, 611–612. [Google Scholar] [CrossRef]
- Palacios, C.; Joshipura, K.J.; Willett, W.C. Nutrition and health: Guidelines for dental practitioners. Oral Dis. 2009, 15, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Curran, A.E.; Caplan, D.J.; Lee, J.Y.; Paynter, L.; Gizlice, Z.; Champagne, C.; Ammerman, A.S.; Agans, R. Dentists’ Attitudes About Their Role in Addressing Obesity in Patients: A national survey. J. Am. Dent. Assoc. 2010, 141, 1307–1316. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.A.M.; Moynihan, P.J. Attitudes and practices of dentists with respect to nutrition and periodontal health. Br. Dent. J. 2008, 205, E9. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E. Global Prevalence and Drivers of Dental Students’ COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 566. [Google Scholar] [CrossRef] [PubMed]
- Kateeb, E.; Danadneh, M.; Pokorná, A.; Klugarová, J.; Abdulqader, H.; Klugar, M.; Riad, A. Predictors of Willingness to Receive COVID-19 Vaccine: Cross-Sectional Study of Palestinian Dental Students. Vaccines 2021, 9, 954. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Huang, Y.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E. IADS-SCORE Universal Predictors of Dental Students’ Attitudes towards COVID-19 Vaccination: Machine Learning-Based Approach. Vaccines 2021, 9, 1158. [Google Scholar] [CrossRef] [PubMed]
- Lenčová, E.; Pikhart, H.; Broukal, Z. Early childhood caries trends and surveillance shortcomings in the Czech Republic. BMC Public Health 2012, 12, 547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexa, J.; Rečka, L.; Votápková, J.; Van Ginneken, E.; Spranger, A.; Wittenbecher, F. Health Systems in Transition. Czech Repub. Health Syst. Rev. 2015, 17, 117. [Google Scholar]
- Smatana, M.; Pažitný, P.; Kandilaki, D.; Laktišová, M.; Sedláková, D.; Palušková, M.; Van Ginneken, E.; Spranger, A. Health Systems in Transition: Slovakia. Slovakia Health Syst. Rev. 2016, 18, 150. [Google Scholar]
- Masaryk University Dentistry—Master’s Studies. Available online: https://www.muni.cz/en/bachelors-and-masters-study-programmes/23446-zubni-lekarstvi (accessed on 19 January 2022).
- Kawamura, M. Dental behavioral science. The relationship between perceptions of oral health and oral status in adults. Hiroshima Daigaku Shigaku Zasshi. 1988, 20, 273–286. [Google Scholar]
- Komabayashi, T.; Kawamura, M.; Kim, K.J.; Wright, F.A.C.; Declerck, D.; Freire, M.D.C.M.; Hu, D.Y.; Honkala, E.; Lévy, G.; Kalwitzki, M.; et al. The hierarchical cluster analysis of oral health attitudes and behaviour using the Hiroshima University—Dental Behavioural Inventory (HU-DBI) among final year dental students in 17 countries. Int. Dent. J. 2006, 56, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, M.; Sasahara, H.; Kawabata, K.; Iwamoto, Y.; Konishi, K.; Wright, F.A.C. Relationship between CPITN and oral health behaviour in Japanese adults. Aust. Dent. J. 1993, 38, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Harvard Humanitarian Initiative Welcome to KoBoToolbox. Available online: https://support.kobotoolbox.org/welcome.html (accessed on 4 January 2022).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. UroToday Int. J. 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jesseniova Lekárska Fakulta UK Študijný Program Zubné Lekárstvo. Available online: https://www.jfmed.uniba.sk/studium/uchadzaci/studijne-programy/studijny-program-zubne-lekarstvo/ (accessed on 19 January 2022).
- Slovenský Spolok Študentov Zubného Lekárstva. Available online: https://ssszl.sk/ (accessed on 19 January 2022).
- Inštitút Zamestnanosti Počet Študentov Zubárstva. Available online: https://www.iz.sk/30-grafov-o-zdravotnictve/studenti-zubari (accessed on 19 January 2022).
- Slovenská Komora Zubných Lekárov (SKZL) Aktuálna Situácia Zubného Lekárstva na Slovensku. Available online: https://www.skzl.sk/images/2019/TS/TS.pdf (accessed on 19 January 2022).
- Největší Lékařská Fakulta v ČR Má Tři Tisíce Studentů. Available online: https://www.doktorvlach.cz/2014/06/05/nejvetsi-lekarska-fakulta-v-cr-ma-tri-tisice-studentu/ (accessed on 19 January 2022).
- Centers for Disease Control and Prevention, (CDC) Epi InfoTM for Windows. Available online: https://www.cdc.gov/epiinfo/pc.html (accessed on 25 December 2020).
- Centers for Disease Control and Prevention (CDC) Population Survey or Descriptive Study. Available online: https://www.cdc.gov/epiinfo/user-guide/statcalc/samplesize.html (accessed on 1 December 2021).
- Riad, A.; Al-Khanati, N.M.; Issa, J.; Zenati, M.; Abdesslem, N.B.; Attia, S.; Krsek, M.; Afrashtehfar, K.; Tchounwou, P.B. Oral Health-Related Knowledge, Attitudes and Behaviours of Arab Dental Students: Multi-National Cross-Sectional Study and Literature Analysis 2000–2020. Int. J. Environ. Res. Public Health 2022, 19, 1658. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Põld, A.; Olak, J.; Howaldt, H.-P.; Klugar, M.; Krsek, M.; Attia, S. Estonian Dental Students’ Oral Health-Related Knowledge, Attitudes and Behaviours (KAB): National Survey-Based Study. Int. J. Environ. Res. Public Health 2022, 19, 1908. [Google Scholar] [CrossRef] [PubMed]
- RIAD, A.; Buchbender, M.; Howaldt, H.-P.; Klugar, M.; Krsek, M.; Attia, S. Oral Health Knowledge, attitudes, and behaviours (KAB) of German Dental Students: Descriptive Cross-sectional Study. Front. Med. 2022, 532. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Marx, R.G.; Menezes, A.; Horovitz, L.; Jones, E.C.; Warren, R.F. A comparison of two time intervals for test-retest reliability of health status instruments. J. Clin. Epidemiol. 2003, 56, 730–735. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- World Health Organization (WHO) Process of Translation and Adaptation of Instruments. Available online: https://web.archive.org/web/20200416020239/https://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 19 January 2022).
- World Medical Association. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA-J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Proton Technologies AG General Data Protection Regulation (GDPR) Compliance Guidelines. Available online: https://gdpr.eu/ (accessed on 1 May 2020).
- Wieslander, V.; Leles, C.; Srinivasan, M. Evaluation of oral-health behavioral attitudes of dental students in Switzerland and Brazil. J. Oral Sci. 2021, 63, 326–329. [Google Scholar] [CrossRef]
- Dias, A.R.d.S.S. Atitudes e Comportamentos de Saúde Oral em Estudantes de Medicina Dentária em Portugal e na Holanda—Um Estudo Comparativo; Universidade Católica Portuguesa: Lisboa, Portugal, 2015. [Google Scholar]
- Kawamura, M.; Honkala, E.; Widström, E.; Komabayashi, T. Cross-cultural differences of self-reported oral health behaviour in Japanese and Finnish dental students. Int. Dent. J. 2000, 50, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Gajić, M.; Lalić, M.; Kalevski, K.; Lazić, E.; Pavlović, M.; Ivanović, M.; Milić, J.; Matijević, D.; Vojinović, J. The application of artificial intelligence algorithms for testing the correlation between the state of oral health and adolescent behavior concerning oral health. Vojnosanit. Pregl. 2021, 78, 858–864. [Google Scholar] [CrossRef] [Green Version]
- Pacauskiene, I.M.; Smailiene, D.; Siudikienė, J.; Savanevskyte, J.; Nedzelskiene, I. Self-reported oral health behavior and attitudes of dental and technology students in Lithuania. Stomatologija 2014, 16, 65–71. [Google Scholar] [PubMed]
- Badovinac, A.; Božić, D.; Vučinac, I.; Vešligaj, J.; Vražić, D.; Plancak, D. Oral health attitudes and behavior of dental students at the University of Zagreb, Croatia. J. Dent. Educ. 2013, 77, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, A.L.; Kawamura, M.; Sasahara, H. An assessment of oral self-care among Romanian dental students using the Hiroshima University--Dental Behavioural Inventory. Oral Health Prev. Dent. 2007, 5, 95–100. [Google Scholar] [PubMed]
- Paraskevas, S.; Timmerman, M.F.; van der Velden, U.; van der Weijden, G.A. Additional Effect of Dentifrices on the Instant Efficacy of Toothbrushing. J. Periodontol. 2006, 77, 1522–1527. [Google Scholar] [CrossRef]
- Valkenburg, C.; Slot, D.E.; Bakker, E.W.P.; Van der Weijden, F.A. Does dentifrice use help to remove plaque? A systematic review. J. Clin. Periodontol. 2016, 43, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Sälzer, S.; Graetz, C.; Dörfer, C.E.; Slot, D.E.; Van der Weijden, F.A. Contemporary practices for mechanical oral hygiene to prevent periodontal disease. Periodontol. 2000 2020, 84, 35–44. [Google Scholar] [CrossRef]
- Olszowski, T.; Walczak, A.; Janiszewska-Olszowska, J.; Milona, M.; Higieny, Z.; Zdrowia Publicznego, E.; Uniwersytet Medyczny Szczecinie, P.; Stomatologii Ogólnej, Z. Self-assessment of oral health behaviors among dental students of Pomeranian Medical University in Szczecin. Problic Hig. Epidemiol. 2012, 93, 798–803. [Google Scholar]
- Kim, K.J.; Komabayashi, T.; Moon, S.E.; Goo, K.M.; Okada, M.; Kawamura, M. Oral health attitudes/behavior and gingival self-care level of Korean dental hygiene students. J. Oral Sci. 2001, 43, 49–53. [Google Scholar] [CrossRef]
- Lujo, M.; Meštrović, M.; Malcić, A.I.; Karlović, Z.; Matijević, J.; Jukić, S. Knowledge, attitudes and habits regarding oral health in first- and final-year dental students. Acta Clin. Croat. 2016, 55, 636–643. [Google Scholar] [CrossRef] [Green Version]
- Ivančić Jokić, N.; Bakarčić, D.; Cicvarić, O.; Šimunović-Erpušina, M.; Zukanović, A.; Hefler, G.; Nastić, V. Knowledge, attitudes and habits regarding oral health among nurses of Clinical hospital center Rijeka. Sestrin. Glas. 2021, 26, 19–23. [Google Scholar] [CrossRef]
- Grycová, P. The Importance and Use of Disclosing Agents in the Dental Hygienist´s Office. Available online: https://dspace.cuni.cz/bitstream/handle/20.500.11956/108138/130259996.pdf (accessed on 21 January 2022).
- Slávik, A. Dental Hygiene Awareness in Czech Republic. Available online: https://dspace.cuni.cz/bitstream/handle/20.500.11956/124083/130286075.pdf (accessed on 20 January 2022).
- Peker, K.; Uysal, O.; Bermek, G.; Uysal, Ö.; Bermek, G. Dental training and changes in oral health attitudes and behaviors in Istanbul dental students. J. Dent. Educ. 2010, 74, 1017–1023. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, S.; Dogan, B. Self reported dental health attitudes and behaviour of dental students in Turkey. Eur. J. Dent. 2011, 5, 253–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özkan Karaca, E.; Tunar, O.L. Evaluation of Oral Health Attitudes and Behaviors of Yeditepe University Dental Faculty Students. Yeditepe J. Dent. 2020, 16, 54–58. [Google Scholar] [CrossRef]
- Doğan, B. Differences in Oral Health Behavior and Attitudes Between Dental and Nursing Students. J. Marmara Univ. Inst. Health Sci. 2013, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Rong, W.S.; Wang, W.J.; Yip, K.H.K. Attitudes of dental and medical students in their first and final years of undergraduate study to oral health behaviour. Eur. J. Dent. Educ. 2006, 10, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, S.; Öztürk, M.; Barthel, C.R.; Bizhang, M.; Jordan, R.A. Cleaning efficacy and soft tissue trauma after use of manual toothbrushes with different bristle stiffness. J. Periodontol. 2011, 82, 267–271. [Google Scholar] [CrossRef]
- Hara, A.T.; González-Cabezas, C.; Creeth, J.; Parmar, M.; Eckert, G.J.; Zero, D.T. Interplay between fluoride and abrasivity of dentifrices on dental erosion–abrasion. J. Dent. 2009, 37, 781–785. [Google Scholar] [CrossRef] [PubMed]
- Racki, D.N.D.O.; Comim, L.D.; Dalla Nora, Â.; Zenkner, J.E.D.A.; Alves, L.S. Is Toothbrush Bristle Stiffness Associated with Erosive Tooth Wear in Adolescents? Findings from a Population-Based Cross-Sectional Study. Caries Res. 2021, 55, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Klusová, M. Dental and Periodontal Health in Students of Third Faculty of Medicine, Charles University. Available online: https://dspace.cuni.cz/bitstream/handle/20.500.11956/108133/130260004.pdf (accessed on 20 January 2022).
- Wiegand, A.; Schlueter, N. The Role of Oral Hygiene: Does Toothbrushing Harm? Monogr. Oral Sci. 2014, 25, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Wiegand, A.; Burkhard, J.P.M.; Eggmann, F.; Attin, T. Brushing force of manual and sonic toothbrushes affects dental hard tissue abrasion. Clin. Oral Investig. 2013, 17, 815–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiegand, A.; Schwerzmann, M.; Sener, B.; Carolina Magalhães, A.; Roos, M.; Ziebolz, D.; Imfeld, T.; Attin, T. Impact of toothpaste slurry abrasivity and toothbrush filament stiffness on abrasion of eroded enamel—An in vitro study. Acta Odontol. Scand. 2008, 66, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Ganss, C.; Schlueter, N.; Preiss, S.; Klimek, J. Tooth brushing habits in uninstructed adults—Frequency, technique, duration and force. Clin. Oral Investig. 2009, 13, 203–208. [Google Scholar] [CrossRef]
- Danser, M.M.; Timmerman, M.F.; Ijzerman, Y.; Bulthuis, H.; Van Der Velden, U.; Van Der Weijden, G.A. Evaluation of the incidence of gingival abrasion as a result of toothbrushing. J. Clin. Periodontol. 1998, 25, 701–706. [Google Scholar] [CrossRef]
- de Carli da Silva, G.; de Castilhos, E.D.; Masotti, A.S.; Rodrigues-Junior, S.A. Dental esthetic self-perception of Brazilian dental students. RSBO Rev. Sul-Brasileira Odontol. 2012, 9, 375–381. [Google Scholar]
- Curd, F.M.; Jasinevicius, T.R.; Graves, A.; Cox, V.; Sadan, A. Comparison of the shade matching ability of dental students using two light sources. J. Prosthet. Dent. 2006, 96, 391–396. [Google Scholar] [CrossRef]
- Jaju, R.A.; Nagai, S.; Karimbux, N.; Silva, J.D. Da Evaluating Tooth Color Matching Ability of Dental Students. J. Dent. Educ. 2010, 74, 1002–1010. [Google Scholar] [CrossRef]
- Samra, A.P.B.; Moro, M.G.; Mazur, R.F.; Vieira, S.; De Souza, E.M.; Freire, A.; Rached, R.N. Performance of Dental Students in Shade Matching: Impact of Training. J. Esthet. Restor. Dent. 2017, 29, E24–E32. [Google Scholar] [CrossRef]
- Vallittu, P.K.; Vallittu, A.S.J.; Lassila, V.P. Dental aesthetics—A survey of attitudes in different groups of patients. J. Dent. 1996, 24, 335–338. [Google Scholar] [CrossRef]
- Akarslan, Z.; Sadik, B.; Erten, H.; Karabulut, E. Dental esthetic satisfaction, received and desired dental treatments for improvement of esthetics. Indian J. Dent. Res. 2009, 20, 195. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Jiang, M.; Chen, W.; Smales, R.J.; Wang, Q.; Tang, L. Differences in facial profile and dental esthetic perceptions between young adults and orthodontists. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Theobald, A.H.; Wong, B.K.J.; Quick, A.N.; Thomson, W.M. The impact of the popular media on cosmetic dentistry. N. Z. Dent. J. 2006, 102, 58–63. [Google Scholar] [PubMed]
- Nomay, N. Public attitude and awareness towards their teeth color and dental bleaching in Saudi Arabia: A cross-sectional survey. J. Public Health Epidemiol. 2016, 8, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Šafaříková, E. The Attitude of Non-Professional and Professional Public to Dental Hygiene in the Czech Republic. Available online: https://dspace.cuni.cz/bitstream/handle/20.500.11956/103135/130205443.pdf (accessed on 20 January 2022).
- Czech Dental Chamber Ročenka ČSK 2020. Available online: https://www.dent.cz/o-nas/rocenky/ (accessed on 22 January 2022).
- Council of European Dentists (CED). The EU Manual of Dental Practice 2015; Kravitz, A.S., Bullock, A., Cowpe, J., Barnes, E., Eds.; Council of European Dentists: Brussels, Belgium, 2015. [Google Scholar]
- Cepova, E.; Cicvakova, M.; Kolarcik, P.; Markovska, N.; Geckova, A.M. Associations of multidimensional health literacy with reported oral health promoting behaviour among Slovak adults: A cross-sectional study. BMC Oral Health 2018, 18, 44. [Google Scholar] [CrossRef] [Green Version]
- Samohyl, M.; Babjakova, J.; Vondrova, D.; Jurkovicova, J.; Stofko, J.; Kollar, B.; Hirosova, K.; Filova, A.; Argalasova, L. Factors Associated with Non-Attendance at Dental Preventive Care in Slovak High School Students. Int. J. Environ. Res. Public Health 2021, 18, 1295. [Google Scholar] [CrossRef]
- Timková, S.; Kolarčik, P.; Gecková, A.M. Self-Reported Oral Health Related Behaviour and Gum Bleeding of Adolescents in Slovakia in Relation to Socioeconomic Status of Their Parents: Cross-Sectional Study Based on Representative Data Collection. Int. J. Environ. Res. Public Health 2019, 16, 2484. [Google Scholar] [CrossRef] [Green Version]
- Vašíčková, J.; Hollein, T.; Sigmundová, D.; Honkala, S.; Pavelka, J.; Kalman, M. Trends in children’s toothbrushing in the Czech republic from 1994 to 2014: Results of the HBSC study. Cent. Eur. J. Public Health 2017, 25, S57–S59. [Google Scholar] [CrossRef] [Green Version]
- Horowitz, A.M.; Kleinman, D.V. Oral Health Literacy: The New Imperative to Better Oral Health. Dent. Clin. N. Am. 2008, 52, 333–344. [Google Scholar] [CrossRef]
- Baskaradoss, J.K. Relationship between oral health literacy and oral health status. BMC Oral Health 2018, 18, 172. [Google Scholar] [CrossRef] [PubMed]
- Naghibi Sistani, M.M.; Yazdani, R.; Virtanen, J.; Pakdaman, A.; Murtomaa, H. Determinants of oral health: Does oral health literacy matter? ISRN Dent. 2013, 2013, 249591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magisterské Studium Zubní Lékařství 2020/2021 a 2021/2022—1. Lékařská Fakulta Univerzity Karlovy. Available online: https://www.lf1.cuni.cz/magisterske-studium-zubni-lekarstvi-v-akademickem-roce-20162017 (accessed on 22 January 2022).
- Zubní Lékařství—Verze 2019: Lékařská Fakulta UP. Available online: https://www.lf.upol.cz/studenti/magisterskyprogram/studijni-plany-sylaby/zubni-lekarstvi-verze-2019/ (accessed on 22 January 2022).
- Lekárska Fakulta Študijný Program Zubné Lekárstvo. Available online: https://www.fmed.uniba.sk/fileadmin/lf/studium/SK/info/SP-ZL.pdf (accessed on 22 January 2022).
- Lekárska Fakulta Študijné Plány. Available online: https://www.upjs.sk/public/media/13729/ZL_%202018-2019.docx.pdf (accessed on 22 January 2022).
- The World Bank Prevalence of Current Tobacco Use (% of Adults)—Czech Republic. Available online: https://data.worldbank.org/indicator/SH.PRV.SMOK?locations=CZ (accessed on 23 January 2022).
- The World Bank Prevalence of Current Tobacco Use (% of Adults)—Slovak Republic. Available online: https://data.worldbank.org/indicator/SH.PRV.SMOK?locations=SK (accessed on 23 January 2022).
- Zatoński, W.; Przewoźniak, K.; Sulkowska, U.; West, R.; Wojtyła, A. Tobacco smoking in countries of the European Union. Ann. Agric. Environ. Med. 2012, 19, 181–192. [Google Scholar] [PubMed]
- Tobacco Control Scale. Available online: https://www.tobaccocontrolscale.org/ (accessed on 23 January 2022).
- Hrubá, D.; Slezák, R. Antismoking education in Czech medical and dental faculties. Eur. J. Dent. Educ. 2004, 8, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Mravčík, V.; Chomynová, P.; Nechanská, B.; Černíková, T.; Csémy, L. Alcohol use and its consequences in the Czech Republic. Cent. Eur. J. Public Health 2019, 27, S15–S28. [Google Scholar] [CrossRef] [Green Version]
- Kážmér, L.; Csémy, L. Changing trends in adolescent alcohol use among Czech school-aged children from 1994 to 2014. J. Public Health Res. 2019, 8, 26–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baška, T.; Madarasová-Gecková, A.; Bašková, M.; Krajčovič, A. Decline in alcohol use among adolescents in Slovakia: A reason for optimism? Public Health 2016, 139, 203–208. [Google Scholar] [CrossRef]
- Fan, X.; Peters, B.A.; Jacobs, E.J.; Gapstur, S.M.; Purdue, M.P.; Freedman, N.D.; Alekseyenko, A.V.; Wu, J.; Yang, L.; Pei, Z.; et al. Drinking alcohol is associated with variation in the human oral microbiome in a large study of American adults. Microbiome 2018, 6, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, P.M.; Ravenel, M.C.; Shealy, A.E.; Thomas, S. Alcohol screening in dental patients: The prevalence of hazardous drinking and patients” attitudes about screening and advice. J. Am. Dent. Assoc. 2006, 137, 1692–1698. [Google Scholar] [CrossRef]
- Šmahel, D.; Blinka, L. Problematic Internet Use in the Czech Republic: Comparison Across Age Groups. In Proceedings of the Quality of Life in Child and Adolescent Mental Health, Budapest, Hungary, 22–26 August 2009. [Google Scholar]
- Do, K.Y.; Lee, K.S. Relationship between Problematic Internet Use, Sleep Problems, and Oral Health in Korean Adolescents: A National Survey. Int. J. Environ. Res. Public Health 2018, 15, 1870. [Google Scholar] [CrossRef] [Green Version]





| Variable | Outcome | Czech (n = 170) | Slovak (n = 317) | Total (n = 487) | Sig. |
|---|---|---|---|---|---|
| Gender | Female | 125 (73.5%) | 247 (77.9%) | 372 (76.4%) | 0.277 |
| Male | 45 (26.5%) | 70 (22.1%) | 115 (23.6%) | ||
| Academic Level | First Year | 13 (7.6%) | 72 (22.7%) | 85 (17.5%) | <0.001 |
| Second Year | 56 (32.9%) | 60 (18.9%) | 116 (23.8%) | <0.001 | |
| Third Year | 25 (14.7%) | 45 (14.2%) | 70 (14.4%) | 0.878 | |
| Fourth Year | 28 (16.5%) | 83 (26.2%) | 111 (22.8%) | 0.015 | |
| Fifth Year | 48 (28.2%) | 30 (9.5%) | 78 (16%) | <0.001 | |
| Sixth Year | N/A | 27 (8.5%) | 27 (5.5%) | N/A | |
| Clinical Experience | Preclinical | 94 (55.3%) | 177 (55.8%) | 271 (55.6%) | 0.909 |
| Clinical | 76 (44.7%) | 140 (44.2%) | 216 (44.4%) |
| Variable | Outcome | Czech (n = 170) | Slovak (n = 317) | Sig. | Female (n = 372) | Male (n = 115) | Sig. | Preclinical (n = 271) | Clinical (n = 216) | Sig. | Total (n = 487) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tobacco Smoking | Yes | 14 (8.2%) | 54 (17%) | 0.008 | 40 (10.8%) | 28 (24.3%) | <0.001 | 32 (11.8%) | 36 (16.7%) | 0.124 | 68 (14%) |
| No | 156 (91.8%) | 263 (83%) | 332 (89.2%) | 87 (75.7%) | 239 (88.2%) | 180 (83.3%) | 419 (86%) | ||||
| Alcohol Drinking | Yes | 60 (35.3%) | 113 (35.6%) | 0.938 | 115 (30.9%) | 58 (50.4%) | <0.001 | 92 (33.9%) | 81 (37.5%) | 0.416 | 173 (35.5%) |
| No | 110 (64.7%) | 204 (64.4%) | 257 (69.1%) | 57 (49.6%) | 179 (66.1%) | 135 (62.5%) | 314 (64.5%) | ||||
| Problematic Internet Use | Yes | 142 (83.5%) | 288 (90.9%) | 0.017 | 332 (89.2%) | 98 (85.2%) | 0.240 | 240 (88.6%) | 190 (88%) | 0.838 | 430 (88.3%) |
| No | 28 (16.5%) | 29 (9.1%) | 40 (10.8%) | 17 (14.8%) | 31 (11.4%) | 26 (12%) | 57 (11.7%) | ||||
| Regular Dental Check-up | Yes | 157 (92.4%) | 299 (94.3%) | 0.396 | 351 (94.4%) | 105 (91.3%) | 0.242 | 257 (94.8%) | 199 (92.1%) | 0.225 | 456 (93.6%) |
| No | 13 (7.6%) | 18 (5.7%) | 21 (5.6%) | 10 (8.7%) | 14 (5.2%) | 17 (7.9%) | 31 (6.4%) |
| Item | Response | State | 1st Year (n = 85) | 2nd Year (n = 116) | 3rd Year (n = 70) | 4th Year (n = 111) | 5th Year (n = 78) | 6th Year (n = 111) | Sig. U | Total (n = 487) | Sig. χ |
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. 1 | Agree | CZ | 9 (69.2%) | 51 (91.1%) | 25 (100%) | 25 (89.3%) | 45 (93.8%) | N/A | 0.015 | 155 (91.2%) | <0.001 |
| SK | 10 (13.9%) | 5 (8.3%) | 4 (8.9%) | 14 (16.9%) | 4 (13.3%) | 2 (7.4%) | 0.381 | 39 (12.3%) | |||
| No. 2 | Disagree | CZ | 12 (92.3%) | 56 (100%) | 25 (100%) | 28 (100%) | 48 (100%) | N/A | 0.055 | 169 (99.4%) | <0.001 |
| SK | 66 (91.7%) | 54 (90%) | 42 (93.3%) | 73 (88%) | 28 (93.3%) | 26 (96.3%) | 0.426 | 289 (91.2%) | |||
| No. 3 | Agree | CZ | 13 (100%) | 52 (92.9%) | 21 (84%) | 28 (100%) | 46 (95.8%) | N/A | 0.458 | 160 (94.1%) | 0.288 |
| SK | 69 (95.8%) | 58 (96.7%) | 42 (93.3%) | 81 (97.6%) | 28 (93.3%) | 27 (100%) | 0.284 | 305 (96.2%) | |||
| No. 4 | Agree | CZ | 2 (15.4%) | 10 (17.9%) | 3 (12%) | 3 (10.7%) | 10 (20.8%) | N/A | 0.664 | 28 (16.5%) | <0.001 |
| SK | 26 (36.1%) | 15 (25%) | 16 (35.6%) | 29 (34.9%) | 9 (30%) | 6 (22.2%) | 0.190 | 101 (31.9%) | |||
| No. 5 | Agree | CZ | 11 (84.6%) | 48 (85.7%) | 24 (96%) | 26 (92.9%) | 44 (91.7%) | N/A | 0.453 | 153 (90%) | <0.001 |
| SK | 1 (1.4%) | 0 (0%) | 1 (2.2%) | 7 (8.4%) | 1 (3.3%) | 2 (7.4%) | 0.122 | 12 (3.8%) | |||
| No. 6 | Disagree | CZ | 11 (84.6%) | 54 (96.4%) | 24 (96%) | 28 (100%) | 48 (100%) | N/A | 0.006 | 165 (97.1%) | <0.001 |
| SK | 51 (70.8%) | 41 (68.3%) | 35 (77.8%) | 56 (67.5%) | 18 (60%) | 20 (74.1%) | 0.751 | 221 (69.7%) | |||
| No. 7 | Agree | CZ | 1 (7.7%) | 1 (1.8%) | 1 (4%) | 0 (0%) | 1 (2.1%) | N/A | 0.318 | 4 (2.4%) | 0.001 |
| SK | 6 (8.3%) | 9 (15%) | 7 (15.6%) | 7 (8.4%) | 2 (6.7%) | 2 (7.4%) | 0.881 | 33 (10.4%) | |||
| No. 8 | Disagree | CZ | 12 (92.3%) | 52 (92.9%) | 23 (92%) | 26 (92.9%) | 46 (95.8%) | N/A | 0.605 | 159 (93.9%) | <0.001 |
| SK | 54 (75%) | 47 (78.3%) | 37 (82.2%) | 64 (77.1%) | 26 (86.7%) | 25 (92.6%) | 0.053 | 253 (79.8%) | |||
| No. 9 | Agree | CZ | 9 (69.2%) | 44 (78.6%) | 20 (80%) | 20 (71.4%) | 38 (79.2%) | N/A | 0.454 | 131 (77.1%) | 0.428 |
| SK | 49 (68.1%) | 50 (83.3%) | 39 (86.7%) | 69 (83.1%) | 22 (73.3%) | 25 (92.6%) | 0.013 | 254 (80.1%) | |||
| No. 10 | Disagree | CZ | 10 (76.9%) | 54 (96.4%) | 23 (92%) | 27 (96.4%) | 46 (95.8%) | N/A | 0.029 | 160 (94.1%) | <0.001 |
| SK | 52 (72.2%) | 43 (71.7%) | 34 (75.6%) | 59 (71.1%) | 26 (86.7%) | 22 (81.5%) | 0.347 | 236 (74.4%) | |||
| No. 11 | Agree | CZ | 7 (53.8%) | 50 (89.3%) | 19 (76%) | 23 (82.1%) | 44 (91.7%) | N/A | 0.001 | 143 (84.1%) | <0.001 |
| SK | 14 (19.4%) | 18 (30%) | 17 (37.8%) | 37 (44.6%) | 15 (50%) | 18 (66.7%) | <0.001 | 119 (37.5%) | |||
| No. 12 | Agree | CZ | 12 (92.3%) | 44 (78.6%) | 16 (64%) | 17 (60.7%) | 29 (60.4%) | N/A | 0.031 | 118 (69.4%) | 0.016 |
| SK | 58 (80.6%) | 49 (81.7%) | 35 (77.8%) | 67 (80.7%) | 21 (70%) | 21 (77.8%) | 0.760 | 251 (79.2%) | |||
| No. 13 | Agree | CZ | 6 (46.2%) | 20 (35.7%) | 10 (40%) | 10 (35.7%) | 16 (33.3%) | N/A | 0.397 | 62 (36.5%) | 0.567 |
| SK | 17 (23.6%) | 21 (35%) | 26 (57.8%) | 27 (32.5%) | 18 (60%) | 15 (55.6%) | 0.003 | 124 (39.1%) | |||
| No. 14 | Disagree | CZ | 10 (76.9%) | 51 (91.1%) | 18 (72%) | 27 (96.4%) | 38 (79.2%) | N/A | 0.862 | 144 (84.7%) | <0.001 |
| SK | 50 (69.4%) | 45 (75%) | 29 (64.4%) | 49 (59%) | 20 (66.7%) | 16 (59.3%) | 0.341 | 209 (65.9%) | |||
| No. 15 | Disagree | CZ | 12 (92.3%) | 54 (96.4%) | 24 (96%) | 27 (96.4%) | 44 (91.7%) | N/A | 0.941 | 161 (94.7%) | 0.160 |
| SK | 65 (90.3%) | 54 (90%) | 44 (97.8%) | 75 (90.4%) | 25 (83.3%) | 26 (96.3%) | 0.330 | 289 (91.2%) | |||
| No. 16 | Agree | CZ | 7 (53.8%) | 34 (60.7%) | 18 (72%) | 20 (71.4%) | 40 (83.3%) | N/A | 0.026 | 119 (70%) | <0.001 |
| SK | 24 (33.3%) | 16 (26.7%) | 18 (40%) | 27 (32.5%) | 16 (53.3%) | 17 (63%) | 0.008 | 118 (37.2%) | |||
| No. 17 | Agree | CZ | 2 (15.4%) | 0 (0%) | 1 (4%) | 0 (0%) | 0 (0%) | N/A | 0.006 | 3 (1.8%) | <0.001 |
| SK | 13 (18.1%) | 7 (11.7%) | 3 (6.7%) | 9 (10.8%) | 1 (3.3%) | 0 (0%) | 0.018 | 33 (10.4%) | |||
| No. 18 | Agree | CZ | 0 (0%) | 2 (3.6%) | 0 (0%) | 2 (7.1%) | 2 (4.2%) | N/A | 0.458 | 6 (3.5%) | <0.001 |
| SK | 18 (25%) | 8 (13.3%) | 2 (4.4%) | 11 (13.3%) | 5 (16.7%) | 2 (7.4%) | 0.053 | 46 (14.5%) | |||
| No. 19 | Agree | CZ | 4 (30.8%) | 26 (46.4%) | 15 (60%) | 17 (60.7%) | 28 (58.3%) | N/A | 0.080 | 90 (52.9%) | <0.001 |
| SK | 10 (13.9%) | 8 (13.3%) | 10 (22.2%) | 16 (19.3%) | 7 (23.3%) | 6 (22.2%) | 0.318 | 57 (18%) | |||
| No. 20 | Agree | CZ | 9 (69.2%) | 43 (76.8%) | 22 (88%) | 26 (92.9%) | 43 (89.6%) | N/A | 0.069 | 143 (84.1%) | 0.102 |
| SK | 53 (73.6%) | 46 (76.7%) | 35 (77.8%) | 66 (79.5%) | 23 (76.7%) | 24 (88.9%) | 0.105 | 247 (77.9%) |
| Item | Response | State | Female (n = 372) | Male (n = 115) | Sig. | Preclinical (n = 271) | Clinical (n = 216) | Sig. | Non-Smoker (n = 419) | Smoker (n = 68) | Sig. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. 1 | Agree | CZ | 116 (92.8%) | 39 (86.7%) | 0.228 * | 85 (90.4%) | 70 (92.1%) | 0.701 | 145 (92.9%) | 10 (71.4%) | 0.023 * |
| SK | 31 (12.6%) | 8 (11.4%) | 0.801 | 19 (10.7%) | 20 (14.3%) | 0.339 | 29 (11%) | 10 (18.5%) | 0.127 | ||
| Total | 147 (39.5%) | 47 (40.9%) | 0.796 | 104 (38.4%) | 90 (41.7%) | 0.461 | 174 (41.5%) | 20 (29.4%) | 0.058 | ||
| No. 2 | Disagree | CZ | 124 (99.2%) | 45 (100%) | 1.000 * | 93 (98.9%) | 76 (100%) | 1.000 * | 155 (99.4%) | 14 (100%) | 1.000 * |
| SK | 226 (91.5%) | 63 (90%) | 0.697 | 162 (91.5%) | 127 (90.7%) | 0.800 | 240 (91.3%) | 49 (90.7%) | 1.000 * | ||
| Total | 350 (94.1%) | 108 (93.9%) | 0.945 | 255 (94.1%) | 203 (94%) | 0.958 | 395 (94.3%) | 63 (92.6%) | 0.581 * | ||
| No. 3 | Agree | CZ | 122 (97.6%) | 38 (84.4%) | 0.004 * | 86 (91.5%) | 74 (97.4%) | 0.188 * | 146 (93.6%) | 14 (100%) | 1.000 * |
| SK | 241 (97.6%) | 64 (91.4%) | 0.028 * | 169 (95.5%) | 136 (97.1%) | 0.441 | 251 (95.4%) | 54 (100%) | 0.231 * | ||
| Total | 363 (97.6%) | 102 (88.7%) | <0.001 | 255 (94.1%) | 210 (97.2%) | 0.099 | 397 (94.7%) | 68 (100%) | 0.057 * | ||
| No. 4 | Agree | CZ | 19 (15.2%) | 9 (20%) | 0.457 | 15 (16%) | 13 (17.1%) | 0.841 | 24 (15.4%) | 4 (28.6%) | 0.252 * |
| SK | 77 (31.2%) | 24 (34.3%) | 0.622 | 57 (32.2%) | 44 (31.4%) | 0.883 | 88 (33.5%) | 13 (24.1%) | 0.178 | ||
| Total | 96 (25.8%) | 33 (28.7%) | 0.539 | 72 (26.6%) | 57 (26.4%) | 0.964 | 112 (26.7%) | 17 (25%) | 0.764 | ||
| No. 5 | Agree | CZ | 118 (94.4%) | 35 (77.8%) | 0.003 * | 83 (88.3%) | 70 (92.1%) | 0.411 | 140 (89.7%) | 13 (92.9%) | 1.000 * |
| SK | 8 (3.2%) | 4 (5.7%) | 0.308 * | 2 (1.1%) | 10 (7.1%) | 0.005 | 10 (3.8%) | 2 (3.7%) | 1.000 * | ||
| Total | 126 (33.9%) | 39 (33.9%) | 0.993 | 85 (31.4%) | 80 (37%) | 0.189 | 150 (35.8%) | 15 (22.1%) | 0.026 | ||
| No. 6 | Disagree | CZ | 122 (97.6%) | 43 (95.6%) | 0.609 * | 89 (94.7%) | 76 (100%) | 0.066 * | 151 (96.8%) | 14 (100%) | 1.000 * |
| SK | 177 (71.7%) | 44 (62.9%) | 0.157 | 127 (71.8%) | 94 (67.1%) | 0.375 | 184 (70%) | 37 (68.5%) | 0.833 | ||
| Total | 299 (80.4%) | 87 (75.7%) | 0.275 | 216 (79.7%) | 170 (78.7%) | 0.787 | 335 (80%) | 51 (75%) | 0.350 | ||
| No. 7 | Agree | CZ | 2 (1.2%) | 2 (4.4%) | 0.286 * | 3 (3.2%) | 1 (1.3%) | 0.629 * | 3 (1.9%) | 1 (7.1%) | 0.217 * |
| SK | 25 (10.1%) | 8 (11.4%) | 0.752 | 22 (12.4%) | 11 (7.9%) | 0.186 | 28 (10.6%) | 5 (9.3%) | 0.761 | ||
| Total | 27 (7.3%) | 10 (8.7%) | 0.611 | 25 (9.2%) | 12 (5.6%) | 0.129 | 31 (7.4%) | 6 (8.8%) | 0.681 | ||
| No. 8 | Disagree | CZ | 117 (93.6%) | 42 (93.3%) | 0.950 * | 87 (92.6%) | 72 (94.7%) | 0.756 * | 146 (93.6%) | 13 (92.9%) | 1.000 * |
| SK | 195 (78.9%) | 58 (82.9%) | 0.472 | 138 (78%) | 115 (82.1%) | 0.358 | 211 (80.2%) | 42 (77.8%) | 0.683 | ||
| Total | 312 (83.9%) | 100 (87%) | 0.423 | 225 (83%) | 187 (86.6%) | 0.281 | 357 (85.2%) | 55 (80.9%) | 0.360 | ||
| No. 9 | Agree | CZ | 98 (78.4%) | 33 (73.3%) | 0.488 | 73 (77.7%) | 58 (76.3%) | 0.836 | 121 (77.6%) | 10 (71.4%) | 0.740 * |
| SK | 199 (80.6%) | 55 (78.6%) | 0.712 | 138 (78%) | 116 (82.9%) | 0.279 | 213 (81%) | 41 (75.9%) | 0.396 | ||
| Total | 297 (79.8%) | 88 (76.5%) | 0.445 | 211 (77.9%) | 174 (80.6%) | 0.468 | 334 (79.7%) | 51 (75%) | 0.376 | ||
| No. 10 | Disagree | CZ | 120 (96%) | 40 (88.9%) | 0.132 * | 87 (92.6%) | 73 (96.1%) | 0.515 * | 147 (94.2%) | 13 (92.9%) | 0.587 * |
| SK | 186 (75.3%) | 50 (71.4%) | 0.512 | 129 (72.9%) | 107 (76.4%) | 0.472 | 196 (74.5%) | 40 (74.1%) | 0.945 | ||
| Total | 306 (82.3%) | 90 (78.3%) | 0.336 | 216 (79.7%) | 180 (83.3%) | 0.307 | 343 (81.9%) | 53 (77.9%) | 0.442 | ||
| No. 11 | Agree | CZ | 106 (84.8%) | 37 (82.2%) | 0.685 | 76 (80.9%) | 67 (88.2%) | 0.195 | 132 (84.6%) | 11 (78.6%) | 0.469 * |
| SK | 94 (38.1%) | 25 (35.7%) | 0.721 | 49 (27.7%) | 70 (50%) | <0.001 | 95 (36.1%) | 24 (44.4%) | 0.250 | ||
| Total | 200 (53.8%) | 62 (53.9%) | 0.978 | 125 (46.1%) | 137 (63.4%) | <0.001 | 227 (54.2%) | 35 (51.5%) | 0.678 | ||
| No. 12 | Agree | CZ | 90 (72%) | 28 (62.2%) | 0.222 | 72 (76.6%) | 46 (60.5%) | 0.024 | 108 (69.2%) | 10 (71.4%) | 1.000 * |
| SK | 198 (80.2%) | 53 (75.7%) | 0.419 | 142 (80.2%) | 109 (77.9%) | 0.606 | 212 (80.6%) | 39 (72.2%) | 0.167 | ||
| Total | 288 (77.4%) | 81 (70.4%) | 0.127 | 214 (79%) | 155 (71.8%) | 0.065 | 320 (76.4%) | 49 (72.1%) | 0.441 | ||
| No. 13 | Agree | CZ | 43 (34.4%) | 19 (42.2%) | 0.350 | 36 (38.3%) | 26 (34.2%) | 0.582 | 55 (35.3%) | 7 (50%) | 0.272 |
| SK | 94 (38.1%) | 30 (42.9%) | 0.468 | 64 (36.2%) | 60 (42.9%) | 0.225 | 99 (37.6%) | 25 (46.3%) | 0.235 | ||
| Total | 137 (36.8%) | 49 (42.6%) | 0.265 | 100 (36.9%) | 86 (39.8%) | 0.511 | 154 (36.8%) | 32 (47.1%) | 0.105 | ||
| No. 14 | Disagree | CZ | 110 (88%) | 34 (75.6%) | 0.047 | 79 (84%) | 65 (85.5%) | 0.789 | 133 (85.3%) | 11 (78.6%) | 0.452 * |
| SK | 163 (66%) | 46 (65.7%) | 0.965 | 124 (70.1%) | 85 (60.7%) | 0.081 | 181 (68.8%) | 28 (51.9%) | 0.017 | ||
| Total | 273 (73.4%) | 80 (69.6%) | 0.423 | 203 (74.9%) | 150 (69.4%) | 0.180 | 314 (74.9%) | 39 (57.4%) | 0.003 | ||
| No. 15 | Disagree | CZ | 117 (93.6%) | 44 (97.8%) | 0.448 * | 90 (95.7%) | 71 (93.4%) | 0.515 * | 148 (94.9%) | 13 (92.9%) | 0.548 * |
| SK | 229 (92.7%) | 60 (85.7%) | 0.069 | 163 (92.1%) | 126 (90%) | 0.515 | 244 (92.8%) | 45 (83.3%) | 0.035 * | ||
| Total | 346 (93%) | 104 (90.4%) | 0.362 | 253 (93.4%) | 197 (91.2%) | 0.373 | 392 (93.6%) | 58 (85.3%) | 0.017 | ||
| No. 16 | Agree | CZ | 87 (69.6%) | 32 (71.1%) | 0.850 | 59 (62.8%) | 60 (78.9%) | 0.022 | 109 (69.9%) | 10 (71.4%) | 1.000 * |
| SK | 99 (40.1%) | 19 (27.1%) | 0.048 | 58 (32.8%) | 60 (42.9%) | 0.065 | 97 (36.9%) | 21 (38.9%) | 0.781 | ||
| Total | 186 (50%) | 51 (44.3%) | 0.289 | 117 (43.2%) | 120 (55.6%) | 0.007 | 206 (49.2%) | 31 (45.6%) | 0.584 | ||
| No. 17 | Agree | CZ | 1 (0.8%) | 2 (4.4%) | 0.171 * | 3 (3.2%) | 0 (0%) | 0.254 | 3 (1.9%) | 0 (0%) | 1.000 * |
| SK | 24 (9.7%) | 9 (12.9%) | 0.448 | 23 (13%) | 10 (7.1%) | 0.090 | 31 (11.8%) | 2 (3.7%) | 0.076 | ||
| Total | 25 (6.7%) | 11 (9.6%) | 0.308 | 26 (9.6%) | 10 (4.6%) | 0.038 | 34 (8.1%) | 2 (2.9%) | 0.130 | ||
| No. 18 | Agree | CZ | 3 (2.4%) | 3 (6.7%) | 0.190 * | 2 (2.1%) | 4 (5.3%) | 0.409 | 6 (3.8%) | 0 (0%) | 1.000 * |
| SK | 34 (13.8%) | 12 (17.1%) | 0.479 | 28 (15.8%) | 18 (12.9%) | 0.457 | 38 (14.4%) | 8 (14.8%) | 0.945 | ||
| Total | 37 (9.9%) | 15 (13%) | 0.347 | 30 (11.1%) | 22 (10.2%) | 0.753 | 44 (10.5%) | 8 (11.8%) | 0.754 | ||
| No. 19 | Agree | CZ | 68 (54.4%) | 22 (48.9%) | 0.525 * | 45 (47.9%) | 45 (59.2%) | 0.141 | 81 (51.9%) | 9 (64.3%) | 0.375 |
| SK | 43 (17.4%) | 14 (20%) | 0.618 | 28 (15.8%) | 29 (20.7%) | 0.260 | 49 (18.6%) | 8 (14.8%) | 0.506 | ||
| Total | 111 (29.8%) | 36 (31.3%) | 0.765 | 73 (26.9%) | 74 (34.3%) | 0.080 | 130 (31%) | 17 (25%) | 0.315 | ||
| No. 20 | Agree | CZ | 106 (84.8%) | 37 (82.2%) | 0.685 | 74 (78.7%) | 69 (90.8%) | 0.032 | 132 (84.6%) | 11 (78.6%) | 0.469 * |
| SK | 193 (78.1%) | 54 (77.1%) | 0.859 | 134 (75.7%) | 113 (80.7%) | 0.286 | 206 (78.3%) | 41 (75.9%) | 0.698 | ||
| Total | 299 (80.4%) | 91 (79.1%) | 0.770 | 208 (76.8%) | 182 (84.3%) | 0.039 | 338 (80.7%) | 52 (76.5%) | 0.421 |
| Variable | Outcome | Knowledge (0–5) | Sig. | Attitudes (0–3) | Sig. | Behaviours (0–4) | Sig. | HU-DBI (0–12) | Sig. |
|---|---|---|---|---|---|---|---|---|---|
| State | Czech Republic | 4.35 ± 0.65 | <0.001 | 2.66 ± 0.56 | <0.001 | 2.33 ± 0.83 | 0.488 | 9.34 ± 1.29 | <0.001 |
| Slovakia | 3.55 ± 0.88 | 1.73 ± 0.85 | 2.28 ± 0.88 | 7.56 ± 1.73 | |||||
| Gender | Female | 3.83 ± 0.90 | 0.772 | 2.08 ± 0.88 | 0.376 | 2.33 ± 0.83 | 0.185 | 8.24 ± 1.76 | 0.316 |
| Male | 3.81 ± 0.87 | 1.99 ± 0.88 | 2.20 ± 0.98 | 8.00 ± 1.93 | |||||
| Academic Level | First Year | 3.49 ± 0.91 | <0.001 | 1.68 ± 0.76 | 0.002 | 2.20 ± 0.95 | 0.061 | 7.38 ± 1.56 | <0.001 |
| Second Year | 3.86 ± 0.85 | 2.23 ± 0.87 | 2.26 ± 0.89 | 8.35 ± 1.87 | |||||
| Third Year | 3.96 ± 0.79 | 2.03 ± 0.82 | 2.36 ± 0.92 | 8.34 ± 1.53 | |||||
| Fourth Year | 3.71 ± 1.02 | 1.98 ± 0.94 | 2.27 ± 0.82 | 7.96 ± 1.99 | |||||
| Fifth Year | 4.15 ± 0.76 | 2.35 ± 0.82 | 2.37 ± 0.81 | 8.87 ± 1.73 | |||||
| Sixth Year | 3.89 ± 0.58 | 2.00 ± 0.88 | 2.56 ± 0.70 | 8.44 ± 1.22 | |||||
| Clinical Experience | Preclinical | 3.77 ± 0.87 | 0.070 | 2.01 ± 0.85 | 0.097 | 2.27 ± 0.91 | 0.301 | 8.04 ± 1.75 | 0.016 |
| Clinical | 3.89 ± 0.91 | 2.12 ± 0.91 | 2.34 ± 0.80 | 8.35 ± 1.86 | |||||
| Tobacco Smoking | Yes | 3.62 ± 1.02 | 0.073 | 1.84 ± 0.89 | 0.024 | 2.18 ± 0.90 | 0.292 | 7.63 ± 2.01 | 0.012 |
| No | 3.86 ± 0.86 | 2.09 ± 0.87 | 2.32 ± 0.86 | 8.27 ± 1.75 | |||||
| Alcohol Drinking | Yes | 3.85 ± 0.89 | 0.532 | 2.02 ± 0.88 | 0.496 | 2.31 ± 0.88 | 0.782 | 8.18 ± 1.87 | 0.798 |
| No | 3.81 ± 0.89 | 2.07 ± 0.88 | 2.29 ± 0.86 | 8.18 ± 1.77 | |||||
| Problematic Internet Use | Yes | 3.79 ± 0.90 | 0.015 | 2.02 ± 0.89 | 0.016 | 2.30 ± 0.86 | 0.817 | 8.11 ± 1.83 | 0.036 |
| No | 4.11 ± 0.72 | 2.33 ± 0.72 | 2.26 ± 0.92 | 8.70 ± 1.50 | |||||
| Regular Dental Check-up | Yes | 3.84 ± 0.88 | 0.163 | 2.06 ± 0.87 | 0.556 | 2.33 ± 0.84 | 0.041 | 8.23 ± 1.78 | 0.016 |
| No | 3.58 ± 1.06 | 1.94 ± 1.00 | 1.90 ± 1.08 | 7.42 ± 2.03 |
| Variable | Outcome | Knowledge (0–5) | Sig. | Attitudes (0–3) | Sig. | Behaviours (0–4) | Sig. | HU-DBI (0–12) | Sig. |
|---|---|---|---|---|---|---|---|---|---|
| Gender | Female | 4.37 ± 0.67 | 0.336 | 2.70 ± 0.52 | 0.080 | 2.35 ± 0.81 | 0.631 | 9.42 ± 1.23 | 0.138 |
| Male | 4.29 ± 0.59 | 2.53 ± 0.63 | 2.27 ± 0.92 | 9.09 ± 1.44 | |||||
| Academic Level | First Year | 3.85 ± 0.80 | 0.044 | 2.15 ± 0.80 | 0.259 | 2.31 ± 0.86 | 0.596 | 8.31 ± 1.55 | 0.074 |
| Second Year | 4.32 ± 0.61 | 2.77 ± 0.47 | 2.36 ± 0.84 | 9.45 ± 1.14 | |||||
| Third Year | 4.40 ± 0.65 | 2.44 ± 0.65 | 2.28 ± 1.02 | 9.12 ± 1.48 | |||||
| Fourth Year | 4.46 ± 0.64 | 2.79 ± 0.42 | 2.14 ± 0.80 | 9.39 ± 1.10 | |||||
| Fifth Year | 4.42 ± 0.61 | 2.71 ± 0.50 | 2.44 ± 0.74 | 9.56 ± 1.29 | |||||
| Clinical Experience | Preclinical | 4.28 ± 0.66 | 0.119 | 2.60 ± 0.61 | 0.154 | 2.33 ± 0.89 | 0.901 | 9.20 ± 1.34 | 0.166 |
| Clinical | 4.43 ± 0.62 | 2.74 ± 0.47 | 2.33 ± 0.77 | 9.50 ± 1.22 | |||||
| Tobacco Smoking | Yes | 4.43 ± 0.65 | 0.620 | 2.57 ± 0.65 | 0.590 | 2.43 ± 1.09 | 0.541 | 9.43 ± 1.40 | 0.923 |
| No | 4.34 ± 0.65 | 2.67 ± 0.55 | 2.32 ± 0.81 | 9.33 ± 1.29 | |||||
| Alcohol Drinking | Yes | 4.35 ± 0.63 | 0.972 | 2.63 ± 0.55 | 0.538 | 2.43 ± 0.85 | 0.212 | 9.42 ± 1.20 | 0.786 |
| No | 4.35 ± 0.66 | 2.67 ± 0.56 | 2.27 ± 0.82 | 9.29 ± 1.34 | |||||
| Problematic Internet Use | Yes | 4.35 ± 0.65 | 0.718 | 2.68 ± 0.54 | 0.425 | 2.33 ± 0.81 | 0.964 | 9.36 ± 1.28 | 0.436 |
| No | 4.32 ± 0.61 | 2.57 ± 0.63 | 2.32 ± 0.98 | 9.21 ± 1.37 | |||||
| Regular Dental Check-up | Yes | 4.36 ± 0.63 | 0.352 | 2.66 ± 0.56 | 0.968 | 2.38 ± 0.77 | 0.076 | 9.39 ± 1.23 | 0.055 |
| No | 4.15 ± 0.80 | 2.69 ± 0.48 | 1.77 ± 1.30 | 8.62 ± 1.76 |
| Variable | Outcome | Knowledge (0–5) | Sig. | Attitudes (0–3) | Sig. | Behaviours (0–4) | Sig. | HU-DBI (0–12) | Sig. |
|---|---|---|---|---|---|---|---|---|---|
| Gender | Female | 3.56 ± 0.88 | 0.646 | 1.76 ± 0.84 | 0.392 | 2.32 ± 0.84 | 0.174 | 7.64 ± 1.68 | 0.248 |
| Male | 3.50 ± 0.88 | 1.64 ± 0.85 | 2.16 ± 1.02 | 7.30 ± 1.88 | |||||
| Academic Level | First Year | 3.43 ± 0.92 | 0.028 | 1.60 ± 0.73 | 0.074 | 2.18 ± 0.97 | 0.072 | 7.21 ± 1.51 | 0.002 |
| Second Year | 3.43 ± 0.83 | 1.73 ± 0.86 | 2.17 ± 0.92 | 7.33 ± 1.85 | |||||
| Third Year | 3.71 ± 0.76 | 1.80 ± 0.82 | 2.40 ± 0.86 | 7.91 ± 1.40 | |||||
| Fourth Year | 3.46 ± 1.00 | 1.71 ± 0.92 | 2.31 ± 0.83 | 7.48 ± 2.00 | |||||
| Fifth Year | 3.73 ± 0.79 | 1.77 ± 0.90 | 2.27 ± 0.91 | 7.77 ± 1.79 | |||||
| Sixth Year | 3.89 ± 0.58 | 2.00 ± 1.73 | 2.56 ± 0.70 | 8.44 ± 1.22 | |||||
| Clinical Experience | Preclinical | 3.50 ± 0.85 | 0.205 | 1.69 ± 0.80 | 0.317 | 2.23 ± 0.93 | 0.240 | 7.43 ± 1.62 | 0.032 |
| Clinical | 3.60 ± 0.90 | 1.78 ± 0.91 | 2.35 ± 0.82 | 7.73 ± 1.85 | |||||
| Tobacco Smoking | Yes | 3.41 ± 1.00 | 0.303 | 1.65 ± 0.85 | 0.394 | 2.11 ± 0.84 | 0.167 | 7.17 ± 1.89 | 0.113 |
| No | 3.57 ± 0.85 | 1.75 ± 0.85 | 2.32 ± 0.89 | 7.64 ± 1.69 | |||||
| Alcohol Drinking | Yes | 3.58 ± 0.89 | 0.355 | 1.70 ± 0.84 | 0.519 | 2.25 ± 0.89 | 0.598 | 7.53 ± 1.83 | 0.969 |
| No | 3.52 ± 0.87 | 1.75 ± 0.85 | 2.30 ± 0.88 | 7.58 ± 1.68 | |||||
| Problematic Internet Use | Yes | 3.51 ± 0.88 | 0.031 | 1.69 ± 0.85 | 0.015 | 2.29 ± 0.89 | 0.725 | 7.50 ± 1.75 | 0.033 |
| No | 3.90 ± 0.77 | 2.10 ± 0.72 | 2.21 ± 0.86 | 8.21 ± 1.47 | |||||
| Regular Dental Check-up | Yes | 3.57 ± 0.86 | 0.082 | 1.75 ± 0.84 | 0.092 | 2.30 ± 0.88 | 0.238 | 7.62 ± 1.71 | 0.017 |
| No | 3.17 ± 1.04 | 1.39 ± 0.92 | 2.00 ± 0.91 | 6.56 ± 1.79 |
| Pair | Knowledge | Attitudes | Behaviours | HU-DBI | ||||
|---|---|---|---|---|---|---|---|---|
| Mean Rank | Sig. | Mean Rank | Sig. | Mean Rank | Sig. | Mean Rank | Sig. | |
| 1st Year vs. 2nd Year | 25.92/37.11 | 0.042 | 22.69/37.86 | 0.002 | 33.96/35.24 | 0.822 | 21.88/38.04 | 0.007 |
| 2nd Year vs. 3rd Year | 40.05/43.12 | 0.544 | 44.43/33.32 | 0.014 | 41.04/40.90 | 0.978 | 42.58/37.46 | 0.350 |
| 3rd Year vs. 4th Year | 26.22/27.70 | 0.697 | 23.04/30.54 | 0.033 | 28.40/25.75 | 0.504 | 25.72/28.14 | 0.557 |
| 4th Year vs. 5th Year | 39.66/37.82 | 0.694 | 39.96/37.65 | 0.557 | 34.09/41.07 | 0.149 | 36.23/39.82 | 0.481 |
| Pair | Knowledge | Attitudes | Behaviours | HU-DBI | ||||
|---|---|---|---|---|---|---|---|---|
| Mean Rank | Sig. | Mean Rank | Sig. | Mean Rank | Sig. | Mean Rank | Sig. | |
| 1st Year vs. 2nd Year | 66.96/65.95 | 0.870 | 64.22/69.23 | 0.421 | 66.74/66.22 | 0.935 | 65.74/67.42 | 0.798 |
| 2nd Year vs. 3rd Year | 49.18/58.10 | 0.103 | 51.64/54.81 | 0.575 | 49.73/57.37 | 0.178 | 48.98/58.36 | 0.113 |
| 3rd Year vs. 4th Year | 69.43/61.83 | 0.229 | 66.86/63.22 | 0.575 | 67.27/63.00 | 0.506 | 67.81/62.70 | 0.450 |
| 4th Year vs. 5th Year | 54.77/63.17 | 0.190 | 56.39/58.70 | 0.727 | 57.31/56.13 | 0.857 | 55.87/60.13 | 0.535 |
| 5th Year vs. 6th Year | 28.05/30.06 | 0.591 | 27.17/31.04 | 0.352 | 26.45/31.83 | 0.188 | 26.38/31.91 | 0.198 |
| Predictor | Beta | S.E. | Wald | df | AOR | 95% CI | Sig. |
|---|---|---|---|---|---|---|---|
| Item No. 2: Disagree | −1.83 | 1.17 | 2.45 | 1 | 0.161 | 0.016–1.583 | 0.117 |
| Item No. 4: Agree | 0.20 | 0.32 | 0.38 | 1 | 1.22 | 0.655–2.253 | 0.537 |
| Item No. 6: Disagree | −2.07 | 0.51 | 16.40 | 1 | 0.13 | 0.047–0.344 | <0.001 |
| Item No. 8: Disagree | −0.90 | 0.43 | 4.36 | 1 | 0.41 | 0.176–0.947 | 0.037 |
| Item No. 10: Disagree | −0.76 | 0.44 | 2.92 | 1 | 0.47 | 0.196–1.118 | 0.087 |
| Item No. 11: Agree | −1.58 | 0.28 | 31.45 | 1 | 0.21 | 0.118–0.357 | <0.001 |
| Item No. 12: Agree | 0.35 | 0.29 | 1.41 | 1 | 1.42 | 0.797–2.516 | 0.236 |
| Item No. 14: Disagree | −0.74 | 0.31 | 5.72 | 1 | 0.48 | 0.262–0.876 | 0.017 |
| Item No. 16: Agree | −0.87 | 0.26 | 11.21 | 1 | 0.42 | 0.250–0.698 | <0.001 |
| Item No. 19: Agree | −1.62 | 0.28 | 34.32 | 1 | 0.20 | 0.115–0.340 | <0.001 |
| Tobacco Smoking: Yes | 0.89 | 0.41 | 4.71 | 1 | 2.43 | 1.090–5.425 | 0.030 |
| Problematic Internet Use: Yes | 0.12 | 0.36 | 0.10 | 1 | 1.12 | 0.553–2.279 | 0.748 |
| Observed Group | Predicted Group | Correct Percentage | ||
|---|---|---|---|---|
| Czech Republic | Slovakia | |||
| State | Czech Republic | 118 | 52 | 69.4% |
| Slovakia | 41 | 276 | 87.1% | |
| Overall | 80.9% | |||
| Predictor. | Beta | S.E. | Wald | df | AOR | 95% CI | Sig. |
|---|---|---|---|---|---|---|---|
| State: Slovakia | 0.79 | 0.33 | 5.59 | 1 | 2.20 | 1.14–4.21 | 0.018 |
| Gender: Male | 0.88 | 0.29 | 9.09 | 1 | 2.40 | 1.36–4.24 | 0.003 |
| Alcohol Drinking: Yes | 0.83 | 0.28 | 9.02 | 1 | 2.30 | 1.34–3.97 | 0.003 |
| Item No. 14: Agree | 0.63 | 0.28 | 4.91 | 1 | 1.87 | 1.08–3.26 | 0.027 |
| Item No. 15: Agree | 0.65 | 0.43 | 2.32 | 1 | 1.92 | 0.83–4.42 | 0.128 |
| Observed Group | Predicted Group | Correct Percentage | ||
|---|---|---|---|---|
| Non-Smoker | Smoker | |||
| Tobacco Smoking | Non-smoker | 416 | 3 | 99.3% |
| Smoker | 67 | 1 | 1.5% | |
| Overall | 85.6% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riad, A.; Chuchmová, V.; Staněk, J.; Hocková, B.; Attia, S.; Krsek, M.; Klugar, M. Czech and Slovak Dental Students’ Oral Health-Related Knowledge, Attitudes, and Behaviours (KAB): Multi-Country Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 2717. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052717
Riad A, Chuchmová V, Staněk J, Hocková B, Attia S, Krsek M, Klugar M. Czech and Slovak Dental Students’ Oral Health-Related Knowledge, Attitudes, and Behaviours (KAB): Multi-Country Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(5):2717. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052717
Chicago/Turabian StyleRiad, Abanoub, Veronika Chuchmová, Ján Staněk, Barbora Hocková, Sameh Attia, Martin Krsek, and Miloslav Klugar. 2022. "Czech and Slovak Dental Students’ Oral Health-Related Knowledge, Attitudes, and Behaviours (KAB): Multi-Country Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 5: 2717. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052717