Biphasic Calcium Phosphate Sphere Graft Combined with a Double-Layer Non-Crosslinked Collagen Membrane Technique for Ridge Preservation: A Randomized Controlled Animal Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal
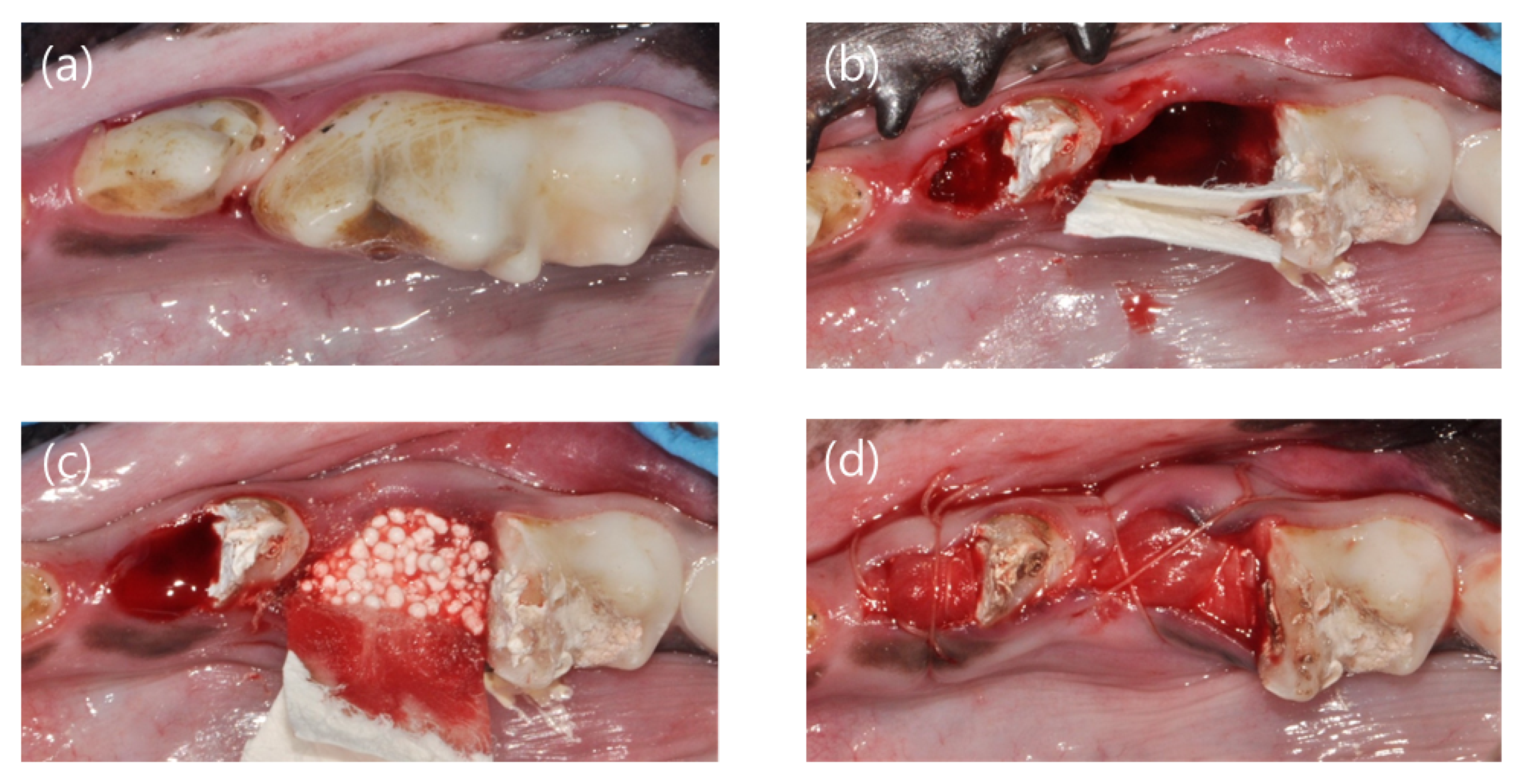
2.2. Ridge Preservation
2.3. Post-Operative Protocol
2.4. Sacrifice and Block Biopsy
2.5. Micro-CT Analysis
2.6. Histologic Processing
2.7. Histologic and Histomorphometric Analysis
2.8. Statistical Analysis
3. Results
3.1. Clinical Findings
3.2. Micro-CT Analysis
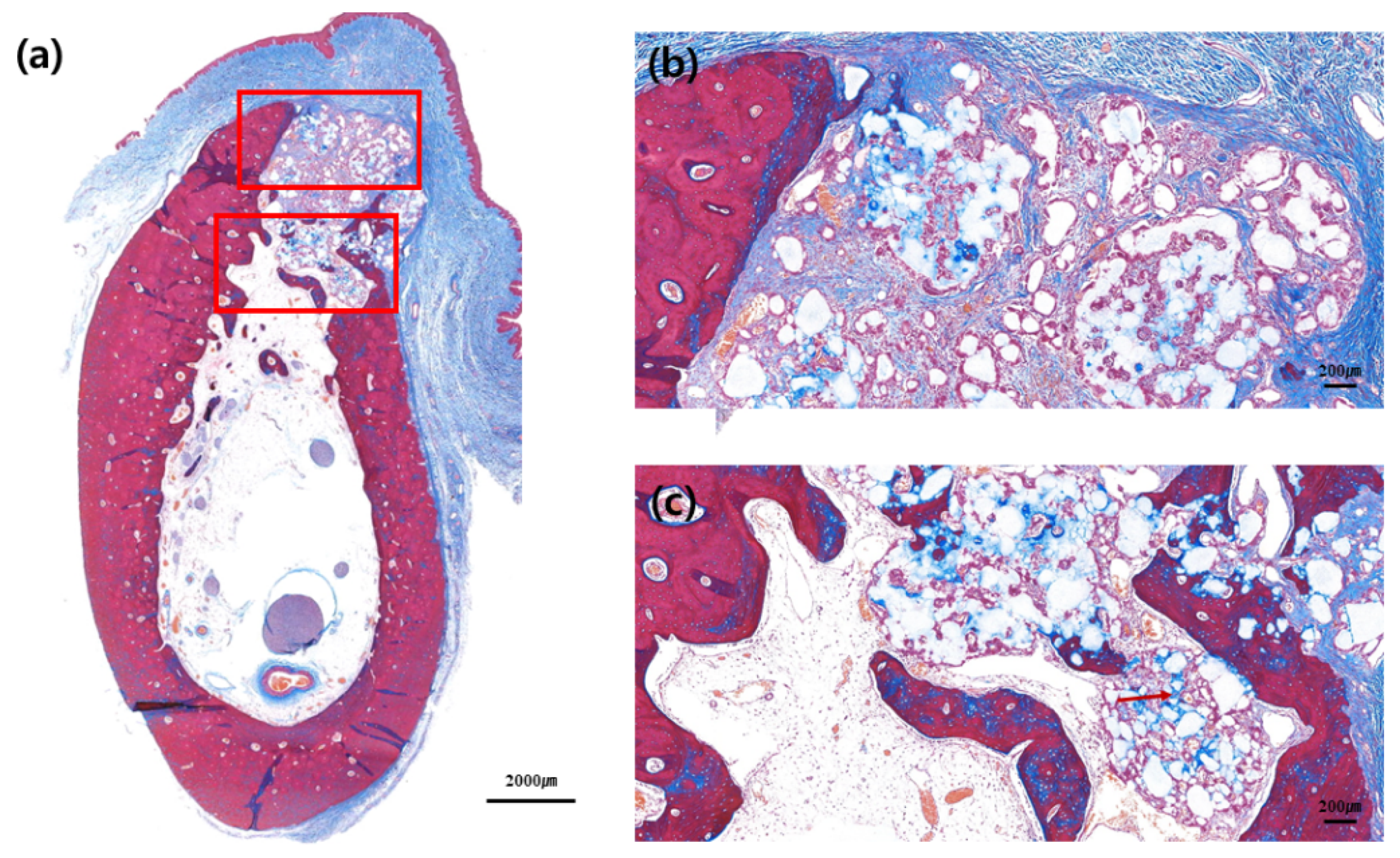
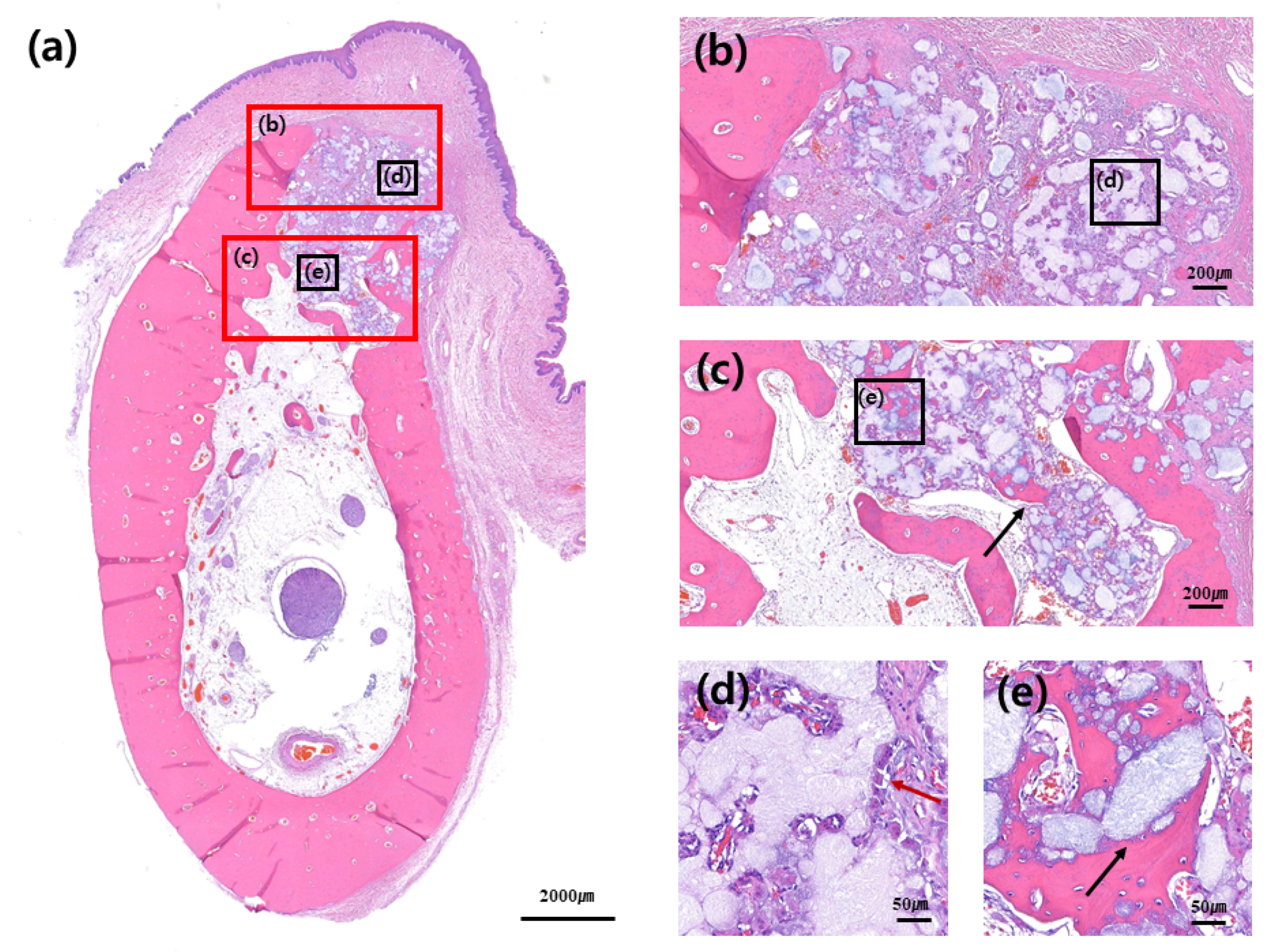
3.3. Hitologic Observation
3.4. Histomorphometric Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pietrokovski, J.; Massler, M. Title of the article Alveolar ridge resorption following tooth extraction. J. Prosthet. Dent. 1967, 17, 21–27. [Google Scholar] [CrossRef]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implants Res. 2012, 23 (Suppl. S5), 1–21. [Google Scholar] [CrossRef]
- Becker, W.; Becker, B.E.; Caffesse, R. A comparison of demineralized freeze-dried bone and autologous bone to induce bone formation in human extraction sockets. J. Periodontol. 1994, 65, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Becker, W.; Urist, M.; Becker, B.E.; Jackson, W.; Parry, D.A.; Bartold, M.; Vincenzzi, G.; De Georges, D.; Niederwanger, M. Clinical and histologic observations of sites implanted with intraoral autologous bone grafts or allografts. 15 human case reports. J. Periodontol. 1996, 67, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Artzi, Z.; Tal, H.; Dayan, D. Porous bovine bone mineral in healing of human extraction sockets: 2. Histochemical observations at 9 months. J. Periodontol. 2001, 72, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Gross, J. Ridge preservation using HTR synthetic bone following tooth extraction. Gen. Dent. 1995, 43, 364–367. [Google Scholar] [PubMed]
- Knapp, C.I.; Feuille, F.; Cochran, D.L.; Mellonig, J.T. Clinical and histologic evaluation of bone-replacement grafts in the treatment of localized alveolar ridge defects. Part 2: Bioactive glass particulate. J. Periodontics Restor. Dent. 2003, 23, 129–137. [Google Scholar]
- Lee, J.; Lee, J.B.; Koo, K.T.; Seol, Y.J.; Lee, Y.M. Flap Management in Alveolar Ridge Preservation: A Systematic Review and Meta-Analysis. J. Nam. Int. J. Oral Maxillofac. Implant. 2018, 33, 613–621. [Google Scholar] [CrossRef]
- Sela, M.N.; Steinberg, D.; Klinger, A.; Krausz, A.A.; Kohavi, D. Adherence of periodontopathic bacteria to bioabsorbable and non-absorbable barrier membranes in vitro. Clin. Oral Implant. Res. 1999, 10, 445–452. [Google Scholar] [CrossRef]
- Bunyaratavej, P.; Wang, H.L. Title of the article. Collagen Membr. A Rev. 2001, 72, 215–229. [Google Scholar]
- Tal, H.; Kozlovsky, A.; Artzi, Z.; Nemcovsky, C.E.; Moses, O. Cross-linked and non-cross-linked collagen barrier membranes disintegrate following surgical exposure to the oral environment: A histological study in the cat. Clin. Oral Implant. Res. 2008, 19, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Rothamel, D.; Schwarz, F.; Sager, M.; Herten, M.; Sculean, A.; Becker, J. Biodegradation of differently cross-linked collagen membranes: An experimental study in the rat. Clin. Oral Implant. Res. 2005, 16, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Cardaropoli, G.; Araujo, M.; Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J. Clin. Periodontol. 2003, 30, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Schwarz, F.; Song, H.Y.; Choi, Y.; Kang, K.R.; Koo, K.T. Ridge preservation of extraction sockets with chronic pathology using Bio-Oss((R)) Collagen with or without collagen membrane: An experimental study in dogs. Clin. Oral Implant. Res. 2017, 28, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Kozlovsky, A.; Aboodi, G.; Moses, O.; Tal, H.; Artzi, Z.; Weinreb, M.; Nemcovsky, C.E. Bio-degradation of a resorbable collagen membrane (Bio-Gide) applied in a double-layer technique in rats. Clin. Oral Implant. Res. 2009, 20, 1116–1123. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, D.Y.; Kim, K.H.; Ku, Y.; Rhyu, I.C.; Lee, Y.M. The efficacy of a double-layer collagen membrane technique for overlaying block grafts in a rabbit calvarium model. Clin. Oral Implant. Res. 2009, 20, 1124–1132. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. PLoS Biol. 2010, 8, e1000412. [Google Scholar] [CrossRef]
- Dempster, D.W.; Compston, J.E.; Drezner, M.K.; Glorieux, F.H.; Kanis, J.A.; Malluche, H.; Meunier, P.J.; Ott, S.M.; Recker, R.R.; Parfitt, A.M. Standardized nomenclature, symbols, and units for bone histomorphometry: A2012 update of the report of the ASBMR Histomorphometry Nomenclature Committee. J. Bone Miner. Res. 2013, 28, 2–17. [Google Scholar] [CrossRef] [Green Version]
- Naenni, N.; Sapata, V.; Bienz, S.P.; Leventis, M.; Jung, R.E.; Hämmerle, C.H.F.; Thoma, D.S. Effect of flapless ridge preservation with two different alloplastic materials in sockets with buccal dehiscence defects—volumetric and linear changes. Clin. Oral Investig. 2018, 22, 2187–2197. [Google Scholar] [CrossRef] [Green Version]
- Ho, K.N.; Salamanca, E.; Chang, K.C.; Shih, T.C.; Chang, Y.C.; Huang, H.M.; Teng, N.C.; Lin, C.T.; Feng, S.W.; Chang, W.J. A Novel HA/β-TCP-Collagen Composite Enhanced New Bone Formation for Dental Extraction Socket Preservation in Beagle Dogs. Materials (Basel) 2016, 9, 191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, H.K.; Cho, H.Y.; Lee, S.J.; Cho, I.W.; Shin, H.S.; Koo, K.T.; Lim, H.C.; Park, J.C. Alveolar ridge preservation with an open-healing approach using single-layer or double-layer coverage with collagen membranes. J. Periodontal Implant Sci. 2017, 47, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Susin, C.; Min, J.H.; Suh, H.Y.; Sang, E.J.; Ku, Y.; Wikesjo, U.M.; Koo, K.T. Extraction sockets: Erratic healing impeding factors. J. Clin. Periodontol. 2014, 41, 80–85. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | N | Vertical Distance (mm) | Bw1 (mm) | Bw2 (mm) | Bw4 (mm) | BV/TV (%) | BS/TV | TbPf | SMI |
|---|---|---|---|---|---|---|---|---|---|
| Control | 8 | 1.28 ± 0.41 | 4.46 ± 0.73 | 5.88 ± 1.10 | 6.89 ± 0.81 | 56.41 ± 9.91 | 10.69 ± 1.35 | 1.14 ± 1.07 | 0.60 ± 0.54 |
| Test | 8 | 0.53 ± 0.37 | 4.72 ± 0.83 | 5.22 ± 1.35 | 6.25 ± 1.43 | 57.00 ± 10.13 | 10.21 ± 1.98 | 0.49 ± 1.51 | 0.25 ± 0.80 |
| p-value | 0.026 | 0.699 | 0.310 | 0.310 | 1.000 | 0.907 | 0.381 | 0.569 |
| Groups | N | Connective Tissue (%) | Bone Graft Materials (%) | Mineralized Bone (%) |
|---|---|---|---|---|
| Control | 8 | 22.37 ± 12.18 | 46.15 ± 10.99 | 31.48 ± 7.41 |
| Test | 8 | 19.88 ± 9.45 | 37.87 ± 11.58 | 42.25 ± 9.73 |
| p-value | 0.818 | 0.589 | 0.041 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Lim, Y.-J.; Kim, B.; Koo, K.-T.; Lee, Y.-M. Biphasic Calcium Phosphate Sphere Graft Combined with a Double-Layer Non-Crosslinked Collagen Membrane Technique for Ridge Preservation: A Randomized Controlled Animal Study. Materials 2020, 13, 18. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13010018
Lee J, Lim Y-J, Kim B, Koo K-T, Lee Y-M. Biphasic Calcium Phosphate Sphere Graft Combined with a Double-Layer Non-Crosslinked Collagen Membrane Technique for Ridge Preservation: A Randomized Controlled Animal Study. Materials. 2020; 13(1):18. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13010018
Chicago/Turabian StyleLee, Jungwon, Young-Jun Lim, Bongju Kim, Ki-Tae Koo, and Yong-Moo Lee. 2020. "Biphasic Calcium Phosphate Sphere Graft Combined with a Double-Layer Non-Crosslinked Collagen Membrane Technique for Ridge Preservation: A Randomized Controlled Animal Study" Materials 13, no. 1: 18. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13010018