Accuracy of Full-Guided and Half-Guided Surgical Templates in Anterior Immediate and Delayed Implantation: A Retrospective Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
- 18 years of age or older;
- At least 1 tooth having missed within 3–4 months or to be extracted in anterior zone, and the remaining teeth are adequate to support the surgical template;
- Sufficient bone tissue to insert an implant without any need for augmentation (the residual bone height ≥ 10 mm, the buccolingual width ≥ 7 mm, and the labial bone plate is complete without bone dehiscence and fenestration);
- Good treatment compliance.
- Presence of uncontrolled systemic diseases, infection or inflammation around the implant sites;
- Pregnancy or lactation;
- Poor oral hygiene habits;
- Psychiatric problems, alcohol, tobacco (>10 cigarettes per day) or drug abuse;
- Severe bruxism or clenching;
- Not able to complete the follow-up.
2.2. Data Acquisition
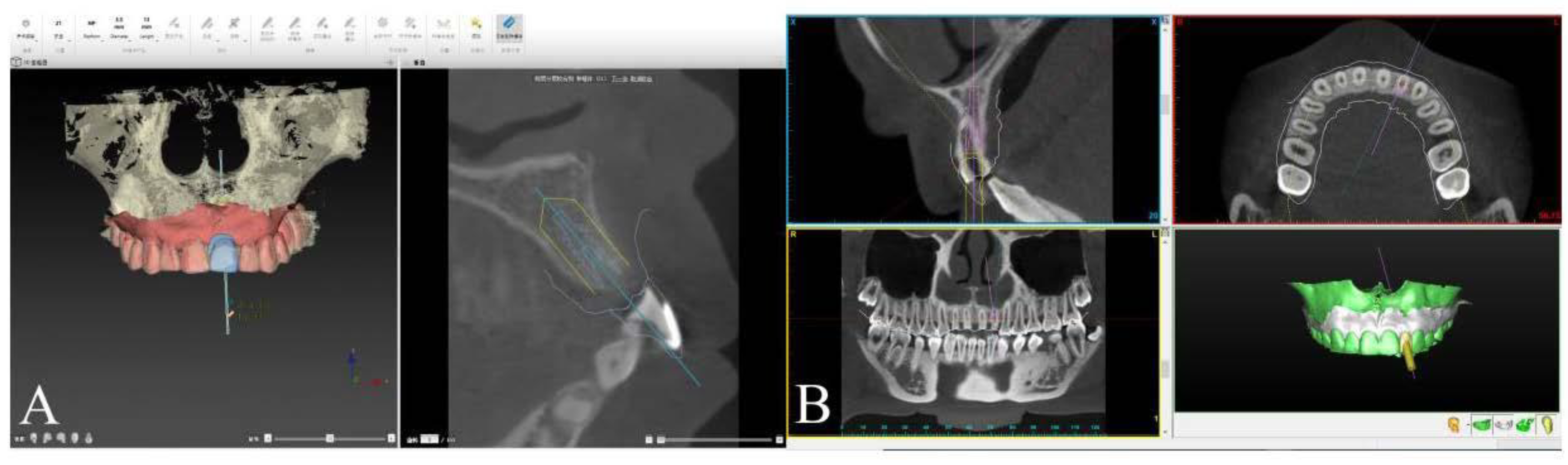
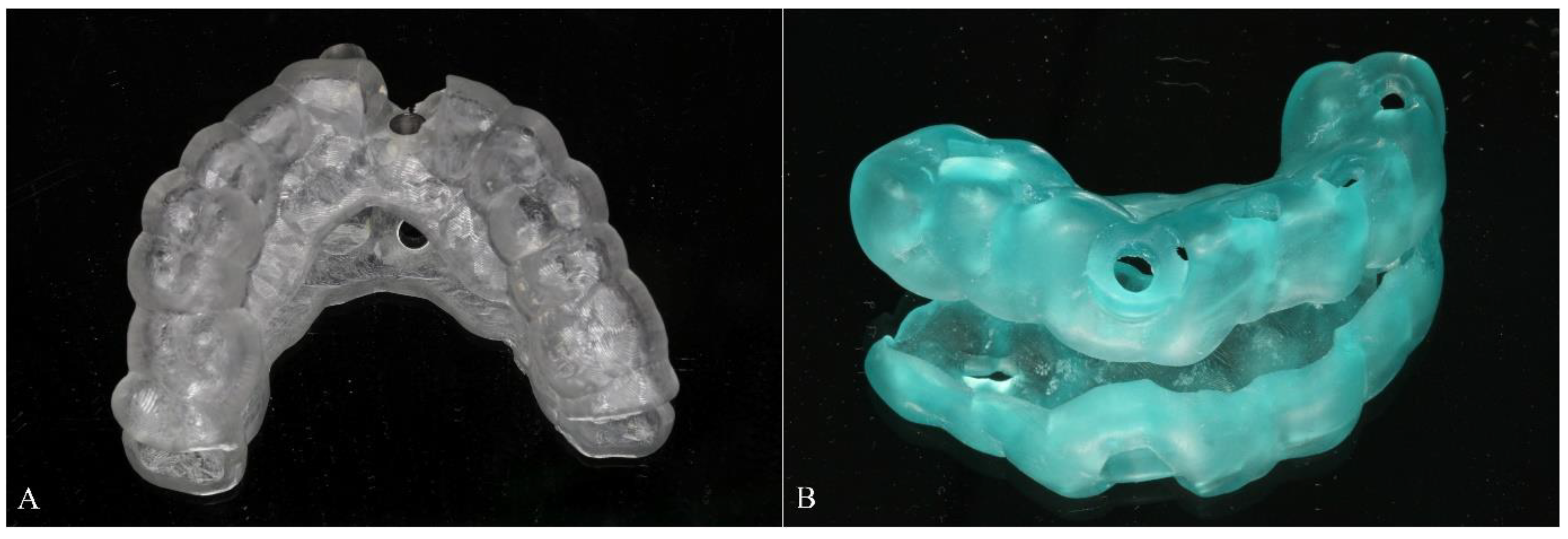
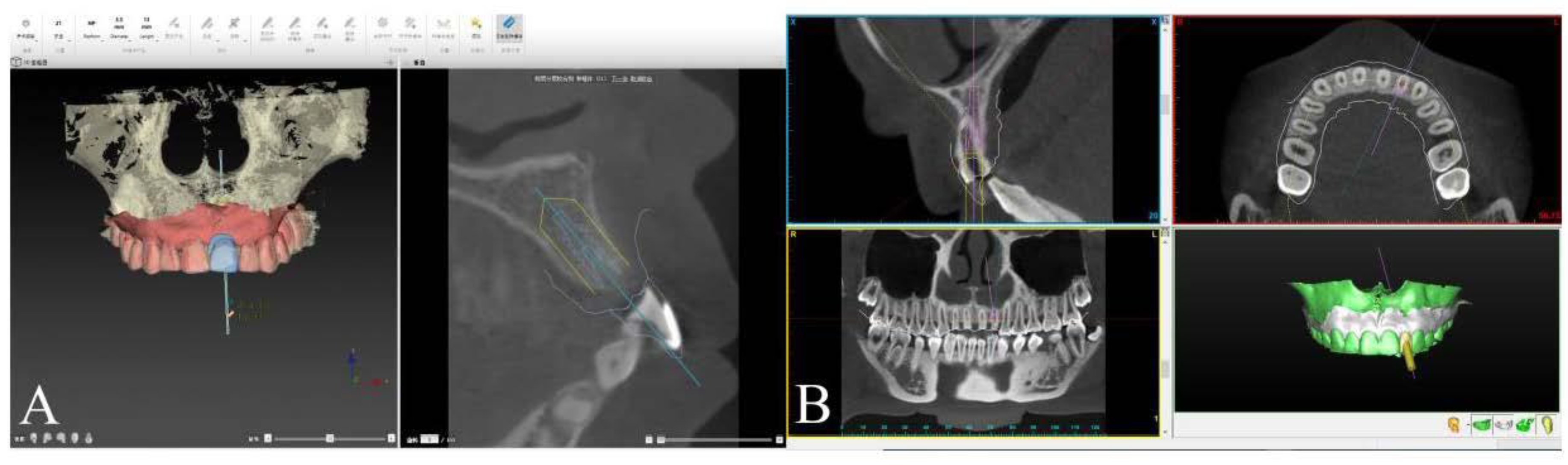
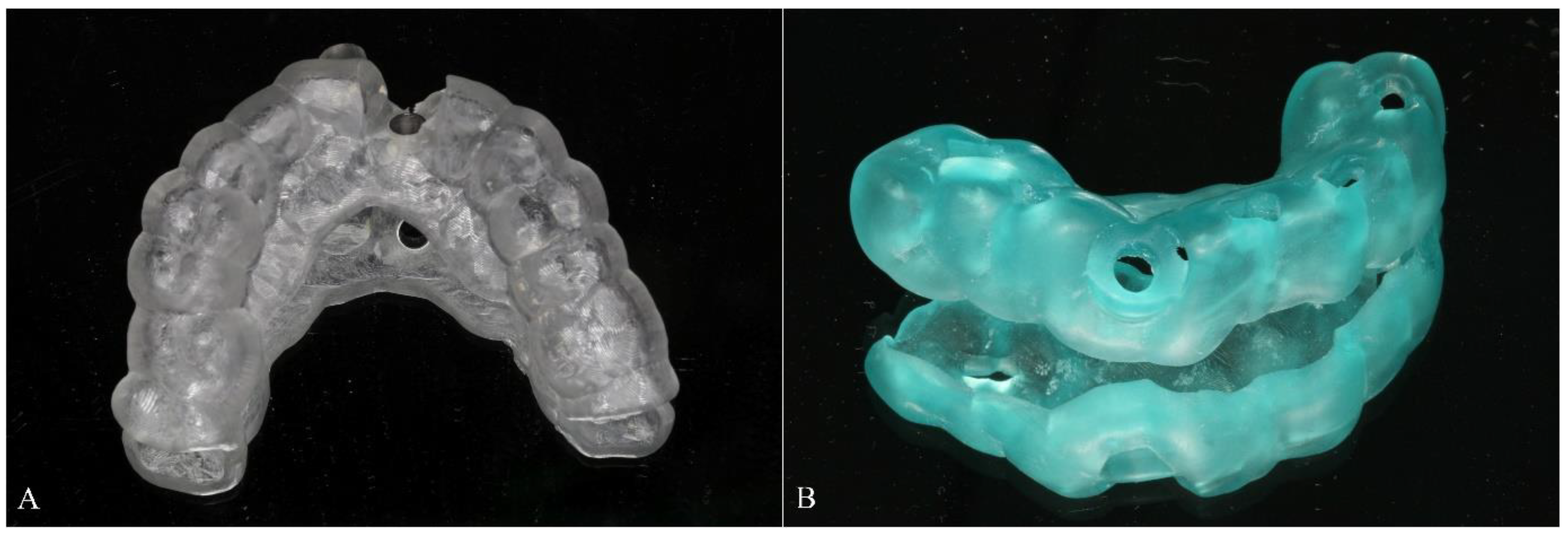
2.3. Implant Planning Procedure and Template Fabrication
2.4. Surgical Procedure
2.5. Accuracy Measurements
2.6. Statistical Analysis
3. Results
3.1. Details of Included Patients
3.2. Accuracy Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cassetta, M.; Giansanti, M.; Di Mambro, A.; Calasso, S.; Barbato, E. Accuracy of two stereolithographic surgical templates: A retrospective study. Clin. Implant Dent. Relat. Res. 2013, 15, 448–459. [Google Scholar] [CrossRef] [PubMed]
- Azari, A.; Nikzad, S. Computer-assisted implantology: Historical background and potential outcomes-a review. Int. J. Med. Robot. 2018, 4, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Park, C.J.; Lumbau, A.I.; Annucci, M.; Baldoni, E.; Koshovari, A.; Meloni, S.M. Customized 3D-Printed Titanium Mesh Developed to Regenerate a Complex Bone Defect in the Aesthetic Zone: A Case Report Approached with a Fully Digital Workflow. Materials 2020, 13, 3874. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.M.; Kaiser, D.A. Surgical guide for dental implant placement. J. Prosthet. Dent. 2000, 83, 248–251. [Google Scholar] [CrossRef]
- Almog, D.M.; Torrado, E.; Meitner, S.W. Fabrication of imaging and surgical guides for dental implants. J. Prosthet. Dent. 2001, 85, 504–508. [Google Scholar] [CrossRef]
- Chen, X.; Xu, L.; Wang, W.; Li, X.; Sun, Y.; Politis, C. Computer-aided design and manufacturing of surgical templates and their clinical applications: A review. Expert Rev. Med. Devices 2016, 13, 853–864. [Google Scholar] [CrossRef]
- Noharet, R.; Pettersson, A.; Bourgeois, D. Accuracy of implant placement in the posterior maxilla as related to 2 types of surgical guides: A pilot study in the human cadaver. J. Prosthet. Dent. 2014, 112, 526–532. [Google Scholar] [CrossRef]
- Cassetta, M.; Stefanelli, L.V.; Giansanti, M.; Calasso, S. Accuracy of implant placement with a stereolithographic surgical template. Int. J. Oral. Maxillofac. Implant. 2012, 27, 655–663. [Google Scholar]
- Gillot, L.; Cannas, B.; Friberg, B.; Vrielinck, L.; Rohner, D.; Pettersson, A. Accuracy of virtually planned and conventionally placed implants in edentulous cadaver maxillae and mandibles: A preliminary report. J. Prosthet. Dent. 2014, 112, 798–804. [Google Scholar] [CrossRef]
- Lee, J.; Lim, Y.J.; Kim, B.; Koo, K.T. Early Loading of Mandibular Molar Single Implants: 1 Year Results of a Randomized Controlled Clinical Trial. Materials 2020, 13, 3912. [Google Scholar] [CrossRef]
- Xu, L.W.; You, J.; Zhang, J.X.; Liu, Y.F.; Peng, W. Impact of Surgical Template on the Accuracy of Implant Placement. J. Prosthodont. 2016, 25, 641–646. [Google Scholar] [CrossRef] [PubMed]
- D’haese, J.; Ackhurst, J.; Wismeijer, D.; De, B.H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2017, 73, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Valente, F.; Schiroli, G.; Sbrenna, A. Accuracy of computer-aided oral implant surgery: A clinical and radiographic study. Int. J. Oral. Maxillofac. Implant. 2019, 24, 234–242. [Google Scholar]
- Pesun, I.J.; Gardner, F.M. Fabrication of a guide for radiographic evaluation and surgical placement of implants. J. Prosthet. Dent. 1995, 73, 548–552. [Google Scholar] [CrossRef]
- Hämmerle, C.H.; Cordaro, L.; Benic, G.I.; Bornstein, M.; Gamper, F.; Gotfredsen, K.; Harris, D.; Hürzeler, M.; Jacobs, R.; Kapos, T.; et al. Digital technologies to support planning, treatment, and fabrication processes and outcome assessments in implant dentistry. Summary and consensus statements. Clin. Oral. Implant. Res. 2015, 26, 97–101. [Google Scholar] [CrossRef] [Green Version]
- Spielau, T.; Hauschild, U.; Katsoulis, J. Computer-assisted, template-guided immediate implant placement and loading in the mandible: A case report. BMC Oral Health 2019, 19, 55. [Google Scholar] [CrossRef] [Green Version]
- Cassetta, M.; Di Mambro, A.; Giansanti, M.; Stefanelli, L.V.; Cavallini, C. The intrinsic error of a stereolithographic surgical template in implant guided surgery. Int. J. Oral Maxillofac. Surg. 2013, 42, 264–275. [Google Scholar] [CrossRef]
- Cassetta, M.; Di Mambro, A.; Giansanti, M.; Stefanelli, L.V.; Barbato, E. How Does an Error in Positioning the template affect the accuracy of implants inserted using a single fixed mucosa-supported stereolithographic surgical guide? Int. J. Oral Maxillofac. Surg. 2014, 43, 85–92. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 25–42. [Google Scholar] [CrossRef] [Green Version]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 416–435. [Google Scholar] [CrossRef] [Green Version]
- Im, C.H.; Park, J.M.; Kim, J.H.; Kang, Y.J.; Kim, J.H. Assessment of Compatibility between Various Intraoral Scanners and 3D Printers through an Accuracy Analysis of 3D Printed Models. Materials 2020, 13, 4419. [Google Scholar] [CrossRef] [PubMed]
- D’haese, J.; Van, D.V.T.; Komiyama, A.; Hultin, M.; De, B.H. Accuracy and complications using computer-designed stereolithographic surgical guides for oral rehabilitation by means of dental implants: A review of the literature. Clin. Implant Dent. Relat. Res. 2012, 14, 321–335. [Google Scholar] [CrossRef] [PubMed]
- Younes, F.; Cosyn, J.; De, B.T.; Cleymaet, R.; Bouckaert, E.; Eghbali, A. A randomized controlled study on the accuracy of free-handed, pilot-drill guided and fully guided implant surgery in partially edentulous patients. J. Clin. Periodontol. 2018, 45, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Beretta, M.; Poli, P.P.; Maiorana, C. Accuracy of computer-aided template guided oral implant placement: A prospective clinical study. J. Periodontal Implant Sci. 2014, 44, 184–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kühl, S.; Zürcher, S.; Mahid, T.; Müller-Gerbl, M.; Filippi, A.; Cattin, P. Accuracy of full guided vs. half-guided implant surgery. Clin. Oral Implant. Res. 2013, 24, 763–769. [Google Scholar] [CrossRef]
- Van, A.N.; Vercruyssen, M.; Coucke, W.; Teughels, W.; Jacobs, R.; Quirynen, M. Accuracy of computer-aided implant placement. Clin. Oral Implant. Res. 2012, 23, 112–123. [Google Scholar]
- Jung, R.E.; Schneider, D.; Ganeles, J.; Wismeijer, D.; Zwahlen, M.; Hämmerle, C.H.; Tahmaseb, A. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2009, 24, 92–109. [Google Scholar]
- Behneke, A.; Burwinkel, M.; Knierim, K.; Behneke, N. Accuracy assessment of cone beam computed tomography-derived laboratory-based surgical templates on partially edentulous patients. Clin. Oral Implant. Res. 2012, 23, 137–143. [Google Scholar] [CrossRef]
- Tadinada, A.; Jalali, E.; Jadhav, A.; Schincaglia, G.P.; Yadav, S. Artifacts in Cone Beam Computed Tomography Image Volumes: An Illustrative Depiction. J. Mass. Dent. Soc. 2015, 64, 12–15. [Google Scholar]
- Pettersson, A.; Komiyama, A.; Hultin, M.; Näsström, K.; Klinge, B. Accuracy of virtually planned and template guided implant surgery on edentate patients. Clin. Implant Dent. Relat. Res. 2012, 14, 527–537. [Google Scholar] [CrossRef] [Green Version]
- Giménez, B.; Özcan, M.; Martínez-Rus, F.; Pradíes, G. Accuracy of a digital impression system based on active wavefront sampling technology for implants considering operator experience, implant angulation, and depth. Clin. Implant Dent. Relat. Res. 2015, 17, e54–e64. [Google Scholar] [CrossRef] [PubMed]
- Giménez, B.; Pradíes, G.; Martínez-Rus, F.; Özcan, M. Accuracy of two digital implant impression systems based on confocal microscopy with variations in customized software and clinical parameters. Int. J. Oral Maxillofac. Implant. 2015, 30, 56–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, D.; Schober, F.; Grohmann, P.; Hammerle, C.H.; Jung, R.E. In-vitro evaluation of the tolerance of surgical instruments in templates for computer-assisted guided implantology produced by 3-D printing. Clin. Oral Implant. Res. 2015, 26, 320–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassetta, M.; Altieri, F.; Giansanti, M.; Bellardini, M.; Brandetti, G.; Piccoli, L. Is there a learning curve in static computer-assisted implant surgery? A prospective clinical study. Int. J. Oral Maxillofac. Surg. 2020, 49, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Ozan, O.; Orhan, K.; Turkyilmaz, I. Correlation between bone density and angular deviation of implants placed using CT-generated surgical guides. J. Craniofac. Surg. 2011, 22, 1755–1761. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | No. Patients (Ratio) | Sex (Ratio) | Age | Implant Sites | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Range | 11/21 | 12/22 | 13/23 | 31/41 | 32/42 | 33/43 | Total | |||
| Total patients | 63 (-) | 34 (54%) | 40.35 ± 13.74 | 18–70 | 43 | 27 | 8 | 2 | 5 | 1 | 76 |
| Full-guided template | 30 (48%) | 16 (53%) | 40.87 ± 13.87 | 18–70 | 21 | 9 | 3 | 1 | 3 | 0 | 37 |
| Half-guided template | 33 (52%) | 18 (55%) | 39.88 ± 13.61 | 18–61 | 22 | 8 | 5 | 1 | 2 | 1 | 39 |
| Immediate implantation | 32 (51%) | 19 (59%) | 40.72 ± 13.75 | 18–63 | 25 | 8 | 1 | 0 | 5 | 1 | 40 |
| Full-guided template | 13 (41%) | 9 (69%) | 40.69 ± 13.16 | 18–63 | 10 | 4 | 0 | 0 | 3 | 0 | 17 |
| Half-guided template | 19 (59%) | 10 (53%) | 40.74 ± 14.14 | 18–61 | 15 | 4 | 1 | 0 | 2 | 1 | 23 |
| Delayed implantation | 31 (49%) | 15 (48%) | 39.97 ± 13.72 | 18–70 | 18 | 9 | 7 | 2 | 0 | 0 | 36 |
| Full-guided template | 17 (55%) | 7 (41%) | 41.00± 14.39 | 18–70 | 11 | 5 | 3 | 1 | 0 | 0 | 20 |
| Half-guided template | 14 (45%) | 8 (57%) | 38.71 ± 12.75 | 23–58 | 7 | 4 | 4 | 1 | 0 | 0 | 16 |
| Group | Global Coronal Deviation | Global Apical Deviation | Depth Deviation | Angular Deviation | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD (mm) | Range (mm) | p-Value | Mean ± SD (mm) | Range (mm) | p-Value | Mean ± SD (mm) | Range (mm) | p-Value | Mean ± SD (°) | Range (°) | p-Value | |
| Immediate implantation | 0.91 ± 0.63 | 0.10–3.10 | 0.057 | 1.23 ± 0.63 | 0.40–3.30 | 0.980 | 0.73 ± 0.66 | 0.10–3.10 | 0.063 | 2.20 ± 1.40 | 0.30–6.20 | 0.353 |
| Delayed implantation | 0.71 ± 0.41 | 0.10–1.80 | 1.23 ± 0.54 | 0.20–2.60 | 0.49 ± 0.41 | 0.00–1.80 | 2.52 ± 1.56 | 0.20–6.30 | ||||
| Full-guided template | 0.59 ± 0.28 | 0.10–1.30 | 0.010 * | 0.99 ± 0.41 | 0.20–1.80 | <0.001 *** | 0.38 ± 0.26 | 0.00–1.10 | <0.001 *** | 1.91 ± 1.02 | 0.20–4.20 | 0.008 ** |
| Half-guided template | 1.04 ± 0.64 | 0.10–3.10 | 1.46 ± 0.64 | 0.50–3.30 | 0.84 ± 0.68 | 0.10–3.10 | 2.77 ± 1.72 | 0.40–6.30 | ||||
| Immediate implantation | ||||||||||||
| Full-guided template | 0.66 ± 0.26 | 0.10–1.00 | 0.005 ** | 0.96 ± 0.41 | 0.20–1.60 | 0.022 * | 0.46 ± 0.24 | 0.00–0.80 | 0.013 ** | 1.69 ± 0.94 | 0.20–3.30 | 0.034 * |
| Half-guided template | 1.10 ± 0.76 | 0.10–3.10 | 1.43 ± 0.70 | 0.50–3.30 | 0.93 ± 0.79 | 0.10–3.10 | 2.57 ± 1.57 | 0.40–6.30 | ||||
| Delayed implantation | ||||||||||||
| Full-guided template | 0.53 ± 0.29 | 0.20–1.30 | 0.509 | 1.10 ± 0.42 | 0.40–1.80 | 0.006 ** | 0.32 ± 0.26 | 0.10–1.10 | 0.008 ** | 2.09 ± 1.07 | 0.50–4.20 | 0.082 |
| Half-guided template | 0.94 ± 0.43 | 0.30–1.80 | 1.51 ± 0.55 | 0.60–2.20 | 0.71 ± 0.47 | 0.10–1.80 | 3.06 ± 1.92 | 0.50–5.59 | ||||
| Variable | Coronal Deviation | Apical Deviation | ||||
|---|---|---|---|---|---|---|
| Immediate Implantation | Delayed Implantation | Total Cases | Immediate Implantation | Delayed Implantation | Total Cases | |
| Full-guided vs. half-guided | −0.012 | −0.126 | −0.052 | −0.143 | −0.345 | −0.206 |
| Depth deviation | 0.917 *** | 0.746 *** | 0.873 *** | 0.703 *** | 0.408 | 0.600 *** |
| Intercept | 0.250 *** | 0.417 *** | 0.306 *** | 0.780 *** | 1.224 *** | 0.962 *** |
| N | 40 | 36 | 76 | 40 | 36 | 76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Zhang, X.; Wang, M.; Jiang, Q.; Mo, A. Accuracy of Full-Guided and Half-Guided Surgical Templates in Anterior Immediate and Delayed Implantation: A Retrospective Study. Materials 2021, 14, 26. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14010026
Chen Y, Zhang X, Wang M, Jiang Q, Mo A. Accuracy of Full-Guided and Half-Guided Surgical Templates in Anterior Immediate and Delayed Implantation: A Retrospective Study. Materials. 2021; 14(1):26. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14010026
Chicago/Turabian StyleChen, Yuan, Xiaoqing Zhang, Maoxia Wang, Qingling Jiang, and Anchun Mo. 2021. "Accuracy of Full-Guided and Half-Guided Surgical Templates in Anterior Immediate and Delayed Implantation: A Retrospective Study" Materials 14, no. 1: 26. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14010026