
Does FGF21 Mediate the Potential Decrease in Sweet Food Intake and Preference Following Bariatric Surgery?

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Weight Loss after Bariatric Surgery
3.2. Associations between FGF21 and Sweet Food Intake, Hedonic Evaluation of Sweet Taste, and Sweet Taste Sensitivity in Patients with Obesity Scheduled for Bariatric Surgery
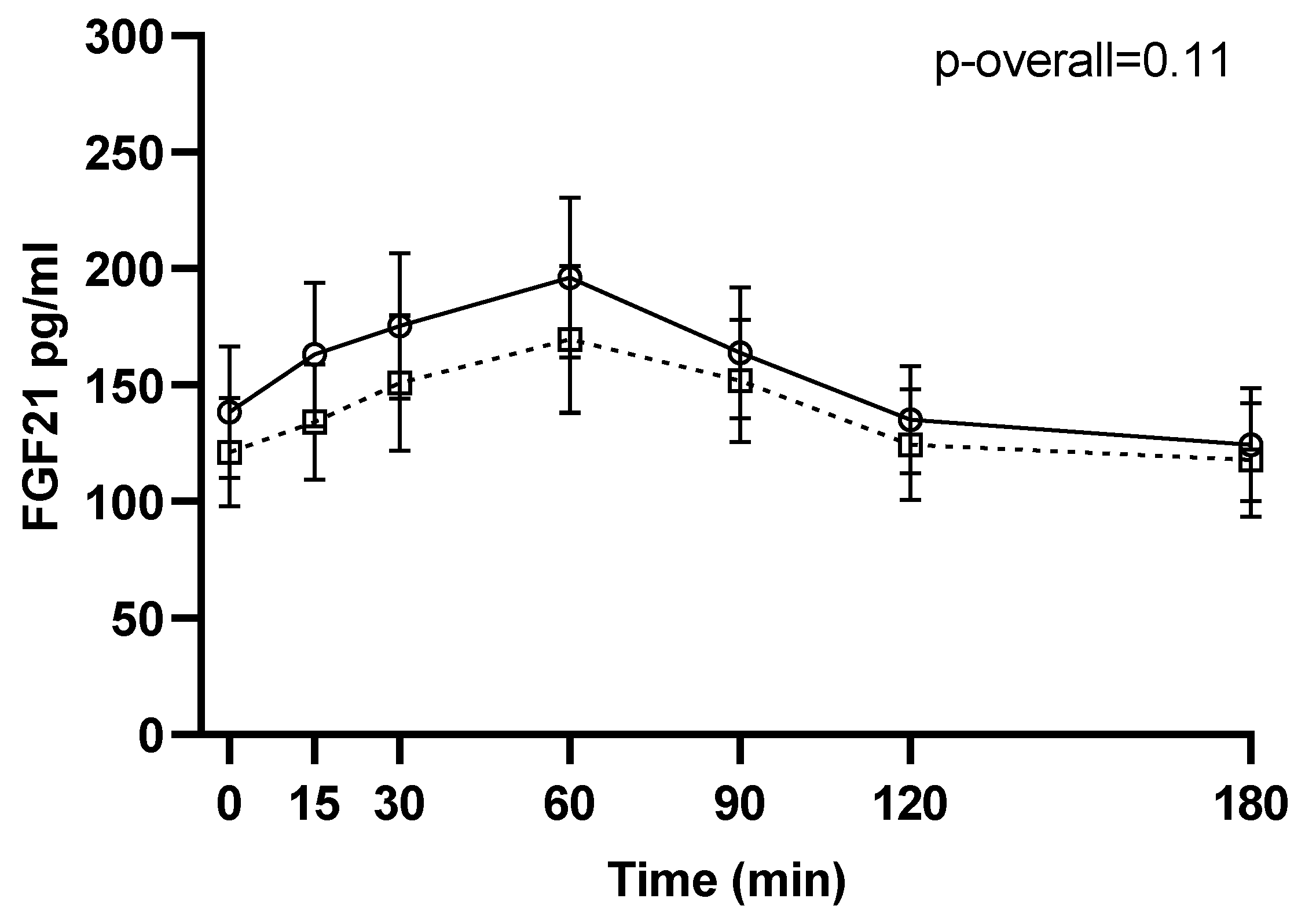
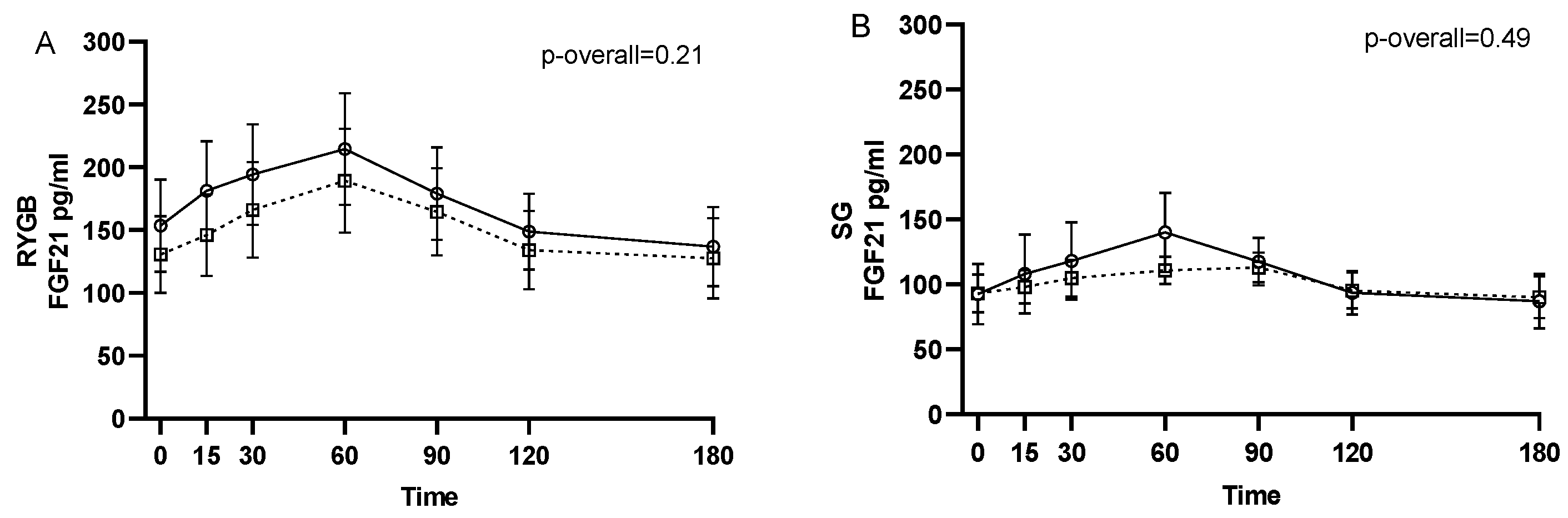
3.3. Effect of Bariatric Surgery on Circulating Intact FGF21
3.4. Associations between Pre- to Postoperative Changes in FGF21 and Changes in Sweet Food Intake, Hedonic Evaluation of Sweet Taste, and Sweet Taste Sensitivity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nance, K.; Eagon, J.C.; Klein, S.; Pepino, M.Y. Effects of sleeve gastrectomy vs. Roux-en-Y gastric bypass on eating behavior and sweet taste perception in subjects with obesity. Nutrients 2018, 10, 18. [Google Scholar] [CrossRef] [Green Version]
- Pepino, M.Y.; Bradley, D.; Eagon, J.C.; Sullivan, S.; Abumrad, N.A.; Klein, S. Changes in taste perception and eating behavior after bariatric surgery-induced weight loss in women. Obesity 2014, 22, E13–E20. [Google Scholar] [CrossRef] [PubMed]
- Coluzzi, I.; Raparelli, L.; Guarnacci, L.; Paone, E.; Del Genio, G.; le Roux, C.W.; Silecchia, G. Food Intake and Changes in Eating Behavior After Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2016, 26, 2059–2067. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.R.; Papantoni, A.; Veldhuizen, M.G.; Kamath, V.; Harris, C.; Moran, T.H.; Carnell, S.; Steele, K.E. Taste-related reward is associated with weight loss following bariatric surgery. J. Clin. Investig. 2020, 130, 4370–4381. [Google Scholar] [CrossRef]
- Laurenius, A.; Larsson, I.; Melanson, K.J.; Lindroos, A.K.; Lonroth, H.; Bosaeus, I.; Olbers, T. Decreased energy density and changes in food selection following Roux-en-Y gastric bypass. Eur. J. Clin. Nutr. 2013, 67, 168–173. [Google Scholar] [CrossRef]
- Miller, G.D.; Norris, A.; Fernandez, A. Changes in nutrients and food groups intake following laparoscopic Roux-en-Y gastric bypass (RYGB). Obes. Surg. 2014, 24, 1926–1932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ernst, B.; Thurnheer, M.; Wilms, B.; Schultes, B. Differential changes in dietary habits after gastric bypass versus gastric banding operations. Obes. Surg. 2009, 19, 274–280. [Google Scholar] [CrossRef]
- Nielsen, M.S.; Schmidt, J.B.; le Roux, C.W.; Sjödin, A. Effects of Roux-en-Y Gastric Bypass and Sleeve Gastrectomy on Food Preferences and Potential Mechanisms Involved. Curr. Obes. Rep. 2019, 8, 292–300. [Google Scholar] [CrossRef]
- Martin, B.; Dotson, C.D.; Shin, Y.-K.; Ji, S.; Drucker, D.J.; Maudsley, S.; Munger, S.D. Modulation of taste sensitivity by GLP-1 signaling in taste buds. Ann. N. Y. Acad. Sci. 2009, 1170, 98–101. [Google Scholar] [CrossRef] [Green Version]
- Takai, S.; Yasumatsu, K.; Inoue, M.; Iwata, S.; Yoshida, R.; Shigemura, N.; Yanagawa, Y.; Drucker, D.J.; Margolskee, R.F.; Ninomiya, Y. Glucagon-like peptide-1 is specifically involved in sweet taste transmission. FASEB J. 2015, 29, 2268–2280. [Google Scholar] [CrossRef] [Green Version]
- La Sala, M.S.; Hurtado, M.D.; Brown, A.R.; Bohórquez, D.V.; Liddle, R.A.; Herzog, H.; Zolotukhin, S.; Dotson, C.D. Modulation of taste responsiveness by the satiation hormone peptide YY. FASEB J. 2013, 27, 5022–5033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acosta, A.; Hurtado, M.D.; Gorbatyuk, O.; La Sala, M.; Duncan, D.; Aslanidi, G.; Campbell-Thompson, M.; Zhang, L.; Herzog, H.; Voutetakis, A.; et al. Salivary PYY: A putative bypass to satiety. PLoS ONE 2011, 6, e26137. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.-H.; Liu, X.-M.; Zhou, L.-H.; Wang, J.; Liu, G.-D. Expression of glucagon-like peptide-1 in the taste buds of rat circumvallate papillae. Acta Histochem. 2008, 110, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Talukdar, S.; Owen, B.M.; Song, P.; Hernandez, G.; Zhang, Y.; Zhou, Y.; Scott, W.T.; Paratala, B.; Turner, T.; Smith, A.; et al. FGF21 Regulates Sweet and Alcohol Preference. Cell Metab. 2016, 23, 344–349. [Google Scholar] [CrossRef] [Green Version]
- von Holstein-Rathlou, S.; BonDurant, L.D.; Peltekian, L.; Naber, M.C.; Yin, T.C.; Claflin, K.E.; Urizar, A.I.; Madsen, A.N.; Ratner, C.; Holst, B.; et al. FGF21 Mediates Endocrine Control of Simple Sugar Intake and Sweet Taste Preference by the Liver. Cell Metab. 2016, 23, 335–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Søberg, S.; Sandholt, C.H.; Jespersen, N.Z.; Toft, U.; Madsen, A.L.; von Holstein-Rathlou, S.; Grevengoed, T.J.; Christensen, K.B.; Bredie, W.L.P.; Potthoff, M.J.; et al. FGF21 Is a Sugar-Induced Hormone Associated with Sweet Intake and Preference in Humans. Cell Metab. 2017, 25, 1045–1053.e6. [Google Scholar] [CrossRef] [Green Version]
- Frayling, T.M.; Beaumont, R.N.; Jones, S.E.; Yaghootkar, H.; Tuke, M.A.; Ruth, K.S.; Casanova, F.; West, B.; Locke, J.; Sharp, S.; et al. A Common Allele in FGF21 Associated with Sugar Intake Is Associated with Body Shape, Lower Total Body-Fat Percentage, and Higher Blood Pressure. Cell Rep. 2018, 23, 327–336. [Google Scholar] [CrossRef] [Green Version]
- Meddens, S.F.W.; de Vlaming, R.; Bowers, P.; Burik, C.A.P.; Linnér, R.K.; Lee, C.; Okbay, A.; Turley, P.; Rietveld, C.A.; Fontana, M.A.; et al. Genomic analysis of diet composition finds novel loci and associations with health and lifestyle. Mol. Psychiatry 2020. [Google Scholar] [CrossRef]
- Nielsen, M.S.; Søberg, S.; Schmidt, J.B.; Chenchar, A.; Sjödin, A.; Gillum, M.P. Transient postprandial increase in intact circulating fibroblast growth factor-21 levels after Roux-en-Y gastric bypass: A randomized controlled clinical trial. PeerJ 2021, 9, e11174. [Google Scholar] [CrossRef]
- Haluzíková, D.; Lacinová, Z.; Kaválková, P.; Drápalová, J.; Křížová, J.; Bártlová, M.; Mráz, M.; Petr, T.; Vítek, L.; Kasalický, M.; et al. Laparoscopic sleeve gastrectomy differentially affects serum concentrations of FGF-19 and FGF-21 in morbidly obese subjects. Obesity 2013, 21, 1335–1342. [Google Scholar] [CrossRef]
- Jansen, P.L.M.; Van Werven, J.; Aarts, E.; Berends, F.; Janssen, I.; Stoker, J.; Schaap, F.G. Alterations of hormonally active fibroblast growth factors after Roux-en-Y gastric bypass surgery. Proc. Dig. Dis. 2011, 29, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Lips, M.A.; de Groot, G.H.; Berends, F.J.; Wiezer, R.; van Wagensveld, B.A.; Swank, D.J.; Luijten, A.; van Dijk, K.W.; Pijl, H.; Jansen, P.L.M.; et al. Calorie restriction and Roux-en-Y gastric bypass have opposing effects on circulating FGF21 in morbidly obese subjects. Clin. Endocrinol. 2014, 81, 862–870. [Google Scholar] [CrossRef] [Green Version]
- Vienberg, S.G.; Jacobsen, S.H.; Worm, D.; Hvolris, L.E.; Naver, L.; Almdal, T.; Hansen, D.L.; Wulff, B.S.; Clausen, T.R.; Madsbad, S.; et al. Increased glucose-stimulated FGF21 response to oral glucose in obese nondiabetic subjects after Roux-en-Y gastric bypass. Clin. Endocrinol. (Oxf). 2017, 86, 156–159. [Google Scholar] [CrossRef]
- Crujeiras, A.B.; Gomez-Arbelaez, D.; Zulet, M.A.; Carreira, M.C.; Sajoux, I.; de Luis, D.; Castro, A.I.; Baltar, J.; Baamonde, I.; Sueiro, A.; et al. Plasma FGF21 levels in obese patients undergoing energy-restricted diets or bariatric surgery: A marker of metabolic stress? Int. J. Obes. 2017, 41, 1570–1578. [Google Scholar] [CrossRef]
- Gómez-Ambrosi, J.; Gallego-Escuredo, J.M.; Catalán, V.; Rodríguez, A.; Domingo, P.; Moncada, R.; Valentí, V.; Salvador, J.; Giralt, M.; Villarroya, F.; et al. FGF19 and FGF21 serum concentrations in human obesity and type 2 diabetes behave differently after diet- or surgically-induced weight loss. Clin. Nutr. 2017, 36, 861–868. [Google Scholar] [CrossRef]
- Hosseinzadeh, A.; Roever, L.; Alizadeh, S. Surgery-Induced Weight Loss and Changes in Hormonally Active Fibroblast Growth Factors: A Systematic Review and Meta-Analysis. Obes. Surg. 2020, 30, 4046–4060. [Google Scholar] [CrossRef]
- Morrison, C.D.; Hao, Z.; Mumphrey, M.B.; Townsend, R.L.; Münzberg, H.; Ye, J.; Berthoud, H.-R. Roux-en-Y gastric bypass surgery is effective in fibroblast growth factor-21 deficient mice. Mol. Metab. 2016, 5, 1006. [Google Scholar] [CrossRef]
- Nielsen, M.S.; Christensen, B.J.; Schmidt, J.B.; Tækker, L.; Holm, L.; Lunn, S.; Ritz, C.; Wewer Albrechtsen, N.J.; Holst, J.J.; Schnurr, T.M.; et al. Predictors of weight loss after bariatric surgery—a cross-disciplinary approach combining physiological, social, and psychological measures. Int. J. Obes. 2020, 44, 2291–2302. [Google Scholar] [CrossRef]
- Christensen, B.J.; Schmidt, J.B.; Nielsen, M.S.; Tækker, L.; Holm, L.; Lunn, S.; Bredie, W.L.P.; Ritz, C.; Holst, J.J.; Hansen, T.; et al. Patient profiling for success after weight loss surgery (GO Bypass study): An interdisciplinary study protocol. Contemp. Clin. Trials Commun. 2018, 10, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Zhen, E.Y.; Jin, Z.; Ackermann, B.L.; Thomas, M.K.; Gutierrez, J.A. Circulating FGF21 proteolytic processing mediated by fibroblast activation protein. Biochem. J. 2016, 473, 605–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunshee, D.R.; Bainbridge, T.W.; Kljavin, N.M.; Zavala-Solorio, J.; Schroeder, A.C.; Chan, R.; Corpuz, R.; Wong, M.; Zhou, W.; Deshmukh, G.; et al. Fibroblast activation protein cleaves and inactivates fibroblast growth factor 21. J. Biol. Chem. 2016, 291, 5986–5996. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, M.S.; Christensen, B.J.; Ritz, C.; Rasmussen, S.; Hansen, T.T.; Bredie, W.L.P.; le Roux, C.W.; Sjödin, A.; Schmidt, J.B. Roux-En-Y Gastric Bypass and Sleeve Gastrectomy Does Not Affect Food Preferences When Assessed by an Ad libitum Buffet Meal. Obes. Surg. 2017, 27, 2599–2605. [Google Scholar] [CrossRef]
- Peryam, D.R.; Pilgrim, F.J. Hedonic scale method of measuring food preferences. Food Technol. 1957, 11, 9–14. [Google Scholar]
- ISO 3972:2011. Sensory Analysis—Methodology—Method of Investigating Sensitivity of Taste, 3rd ed.; International Organization for Standardization: Geneva, Switzerland, 2011; 10p. [Google Scholar]
- Lawless, H.T. A simple alternative analysis for threshold data determined by ascending forced-choice methods of limits. J. Sens. Stud. 2010, 25, 332–346. [Google Scholar] [CrossRef]
- R R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 12 August 2021).
- von Holstein-Rathlou, S.; Gillum, M.P. Fibroblast growth factor 21: An endocrine inhibitor of sugar and alcohol appetite. J. Physiol. 2019, 597, 3539–3548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ter Horst, K.W.; Gilijamse, P.W.; Demirkiran, A.; van Wagensveld, B.A.; Ackermans, M.T.; Verheij, J.; Romijn, J.A.; Nieuwdorp, M.; Maratos-Flier, E.; Herman, M.A.; et al. The FGF21 response to fructose predicts metabolic health and persists after bariatric surgery in obese humans. Mol. Metab. 2017, 6, 1493–1502. [Google Scholar] [CrossRef] [PubMed]
- Fjeldborg, K.; Pedersen, S.B.; Møller, H.J.; Richelsen, B. Reduction in serum fibroblast growth factor-21 after gastric bypass is related to changes in hepatic fat content. Surg. Obes. Relat. Dis. 2017, 13, 1515–1523. [Google Scholar] [CrossRef]
- Gälman, C.; Lundåsen, T.; Kharitonenkov, A.; Bina, H.A.; Eriksson, M.; Hafström, I.; Dahlin, M.; Amark, P.; Angelin, B.; Rudling, M. The circulating metabolic regulator FGF21 is induced by prolonged fasting and PPARalpha activation in man. Cell Metab. 2008, 8, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, M.S.; Andersen, I.N.S.K.; Lange, B.; Ritz, C.; le Roux, C.W.; Schmidt, J.B.; Sjödin, A.; Bredie, W.L.P. Bariatric Surgery Leads to Short-Term Effects on Sweet Taste Sensitivity and Hedonic Evaluation of Fatty Food Stimuli. Obesity 2019, 27, 1796–1804. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.S.; Rasmussen, S.; Just Christensen, B.; Ritz, C.; le Roux, C.W.; Berg Schmidt, J.; Sjödin, A. Bariatric Surgery Does Not Affect Food Preferences, but Individual Changes in Food Preferences May Predict Weight Loss. Obesity 2018, 26, 1879–1887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brolin, R.E.; Robertson, L.B.; Kenler, H.A.; Cody, R.P. Weight loss and dietary intake after vertical banded gastroplasty and Roux-en-Y gastric bypass. Ann. Surg. 1994, 220, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Trostler, N.; Mann, A.; Zilberbush, N.; Avinoach, E.; Charuzi, I. Weight Loss and Food Intake 18 Months following Vertical Banded Gastroplasty or Gastric Bypass for Severe Obesity. Obes. Surg. 1995, 5, 39–51. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| β ± SEM | R2 | p-Value | |
|---|---|---|---|
| Preprandial FGF21 | |||
| Subjective appetite for sweet, preprandial | 0.002 ± 0.003 | 24.5 | 0.42 |
| Subjective appetite for sweet, AUC | 0.27 ± 0.41 | 13.8 | 0.52 |
| Hedonic rating of an apple juice with 20 g sucrose | −0.005 ± 0.002 | 15.9 | 0.03 |
| Intake of carbohydrate (kJ) 1 | 0.04 ± 0.86 | 11.9 | 0.97 |
| Intake of food from the sweet category (%) 1 | 0.02 ± 0.01 | 13.1 | 0.12 |
| Detection threshold (g/L) | −0.002 ± 0.003 | 7.5 | 0.52 |
| Recognition threshold (g/L) | −0.01 ± 0.01 | 16.7 | 0.08 |
| Postprandial FGF21 (AUC) | |||
| Subjective appetite for sweet, AUC | 0.002 ± 0.002 | 14.7 | 0.37 |
| Hedonic rating of an apple juice with 20 g sucrose | −0.00001 ± 0.00001 | 17.6 | 0.02 |
| Intake of carbohydrate (kJ) 1 | −0.0003 ± 0.004 | 11.7 | 0.95 |
| Intake of food from the sweet category (%) 1 | 0.0001 ± 0.0001 | 9.6 | 0.26 |
| Detection threshold (g/L) | −0.00001 ± 0.0001 | 7.6 | 0.49 |
| Recognition threshold (g/L) | −0.00005 ± 0.00003 | 14.0 | 0.13 |
| β ± SEM | R2 | p-Value | |
|---|---|---|---|
| ΔPreprandial FGF21 | |||
| ΔSubjective appetite for sweet, preprandial | 0.01 ± 0.01 | 11.2 | 0.27 |
| ΔSubjective appetite for sweet, AUC | −0.45 ± 0.70 | 5.4 | 0.53 |
| ΔHedonic rating of an apple juice with 20 g sucrose | 0.004 ± 0.004 | 3.7 | 0.29 |
| ΔIntake of carbohydrate (kJ) 1 | 0.13 ± 1.21 | 9.2 | 0.91 |
| ΔIntake of food from the sweet category (%) 1 | −0.05 ± 0.03 | 11.9 | 0.10 |
| ΔDetection threshold (g/L) | −0.003 ± 0.01 | 14.8 | 0.65 |
| ΔRecognition threshold (g/L) | 0.003 ± 0.01 | 2.6 | 0.73 |
| ΔPostprandial FGF21 (AUC) | |||
| ΔSubjective appetite for sweet, AUC | 0.0002 ± 0.004 | 4.3 | 0.95 |
| ΔHedonic rating of an apple juice with 20 g sucrose | 0.00002 ± 0.00002 | 3.7 | 0.41 |
| ΔIntake of carbohydrate (kJ) 1 | 0.002 ± 0.01 | 10.0 | 0.81 |
| ΔIntake of food from the sweet category (%) 1 | −0.0003 ± 0.0002 | 12.1 | 0.13 |
| ΔDetection threshold (g/L) | −0.00002 ± 0.00003 | 11.9 | 0.50 |
| ΔRecognition threshold (g/L) | 0.00002 ± 0.00004 | 3.4 | 0.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nielsen, M.S.; Ritz, C.; Chenchar, A.; Bredie, W.L.P.; Gillum, M.P.; Sjödin, A. Does FGF21 Mediate the Potential Decrease in Sweet Food Intake and Preference Following Bariatric Surgery? Nutrients 2021, 13, 3840. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113840
Nielsen MS, Ritz C, Chenchar A, Bredie WLP, Gillum MP, Sjödin A. Does FGF21 Mediate the Potential Decrease in Sweet Food Intake and Preference Following Bariatric Surgery? Nutrients. 2021; 13(11):3840. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113840
Chicago/Turabian StyleNielsen, Mette S., Christian Ritz, Anne Chenchar, Wender L. P. Bredie, Matthew P. Gillum, and Anders Sjödin. 2021. "Does FGF21 Mediate the Potential Decrease in Sweet Food Intake and Preference Following Bariatric Surgery?" Nutrients 13, no. 11: 3840. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113840