
A Comparison of Total Food Intake at a Personalised Buffet in People with Obesity, before and 24 Months after Roux-en-Y-Gastric Bypass Surgery


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
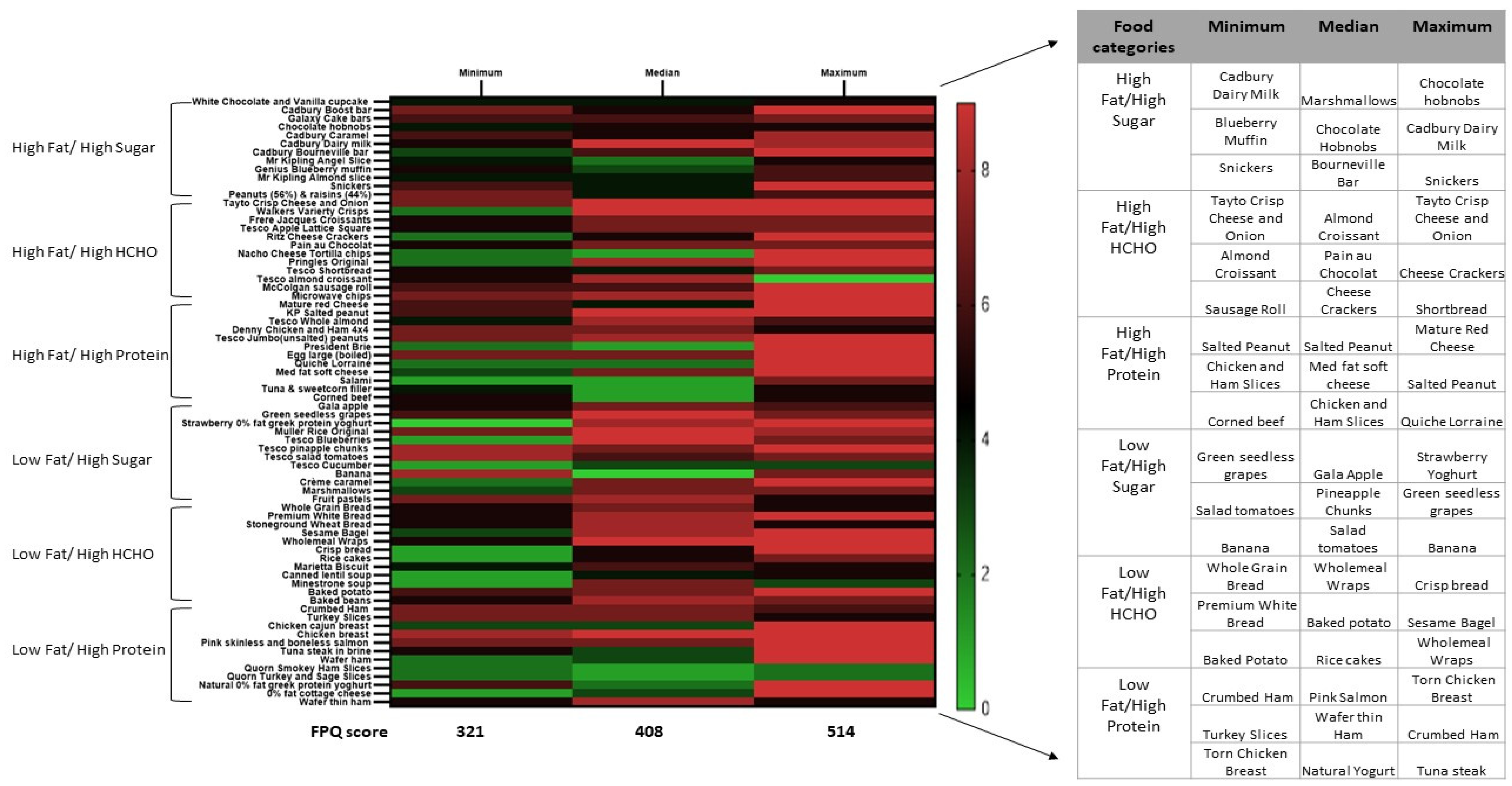
2.2. Food Preference Questionnaire
2.3. Study Visits
2.4. Experimental Power and Inferential Statistics
3. Results
3.1. Study Participants
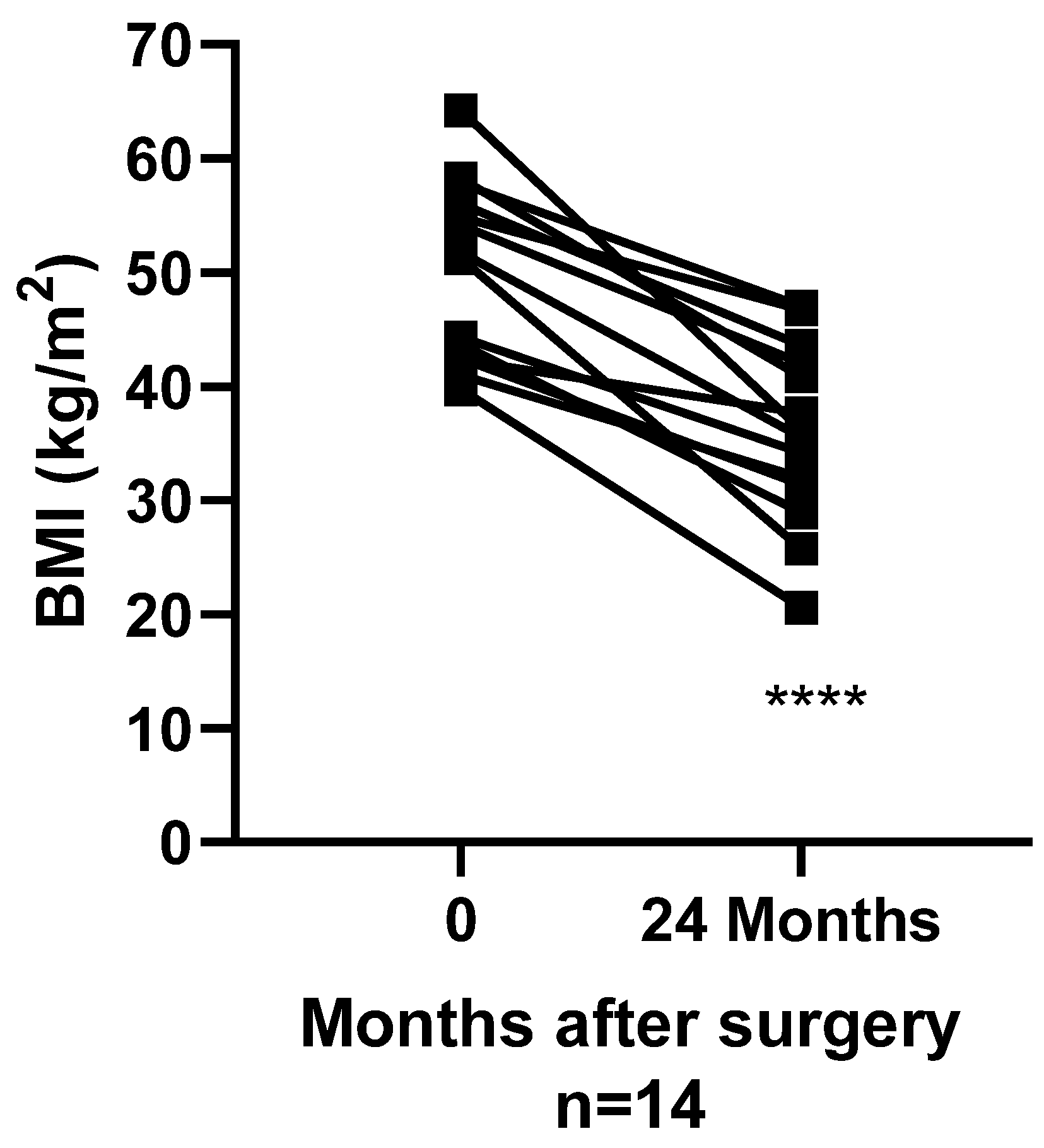
3.2. Surgery Induced Changes in BMI
3.3. Questionnaire Based Food Preference Ratings at Baseline
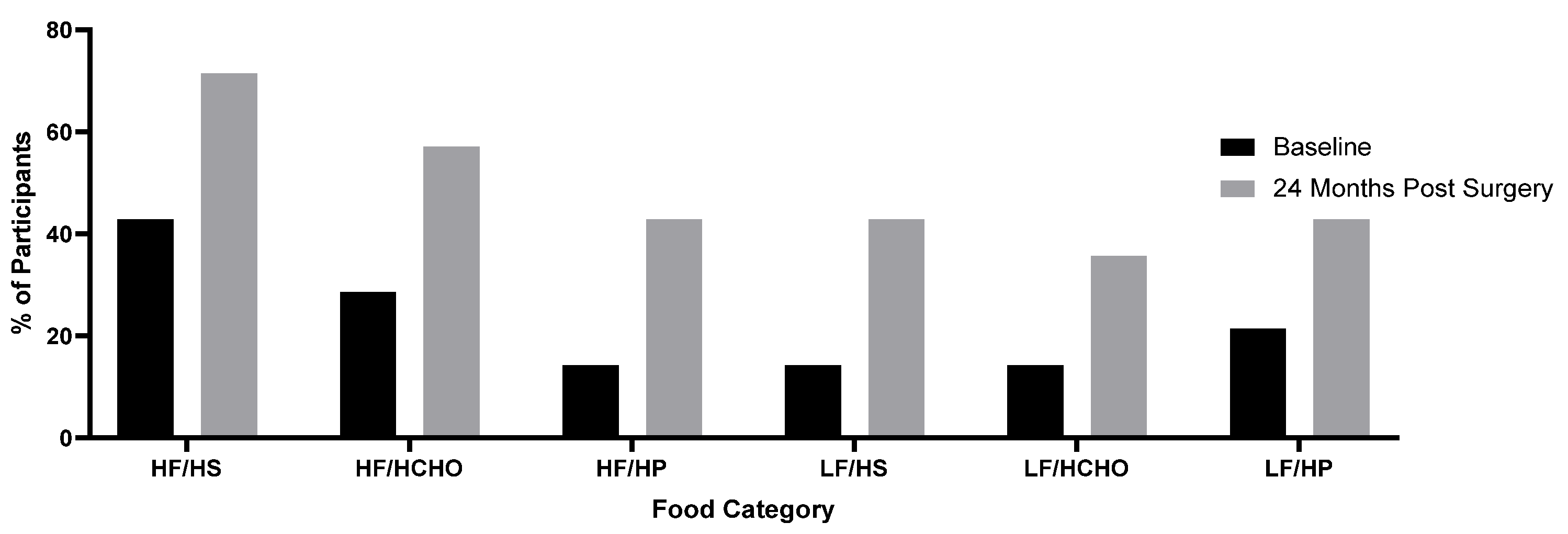
3.4. Changes in Absolute Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Food Preference Questionnaire | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Dislike Extremely | Dislike a Lot | Dislike | Dislike a Little | Neutral | Like a Little | Like | Like a Lot | Like Extremely | Allergy | |
| Crème caramel | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Marshmallows | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Fruit pastels | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Hobnob biscuit | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Caramel chocolate bar | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Dairy milk (milk chocolate) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Bournville (dark chocolate) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Snickers bar | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Almond slice | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Blueberry cupcake | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Peanuts and Raisin mix | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Angel slice | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Natural yoghurt low fat | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Cottage cheese | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Croissant | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Apple lattice pastry | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Pain au chocolat | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Salted cheese crackers | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Pringles original | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Shortbread | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Almond croissant | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Sausage roll | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Chips (fries) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Cheddar cheese | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Gala apple | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Seedless grapes | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Unsalted peanuts | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Brie cheese | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Egg (boiled) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Quiche Lorraine | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Soft cream cheese | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Salami | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Tuna and sweet corn | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Corned beef | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Chicken and ham slices | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Whole almonds | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| KP salted peanut | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Rice pudding | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Blueberries | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Pineapple chunks | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Tomato’s | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Banana | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| White chocolate cupcake | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Boost bar | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Chocolate Cake bar | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Brown sliced pan | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| White sliced pan | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Brown wheaten bread | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Sesame Bagel | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Whole meal wrap | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Whole meal cracker (Ryvita) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Rice cake | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Marietta biscuit | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Lentil soup | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Minestrone soup | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Baked potato | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Baked beans | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Crumbed ham | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Turkey slices | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Cheese and Onion crisp | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Salt and Vinegar crisp | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Skinless salmon | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Tuna steak | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Smoked ham | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Quorn Smokey ham slices | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Quorn Turkey and sage slices | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Cajun chicken breast | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Chicken breast | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Cucumber | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Tortilla chips | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Wafer thin ham | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Glenisk Strawberry 0% fat greek protein yoghurt 150 g | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
References
- Buchwald, H.; Oien, D.M. Metabolic/Bariatric Surgery Worldwide 2011. Obes. Surg. 2013, 23, 427–436. [Google Scholar] [CrossRef]
- Salminen, P.; Helmiö, M.; Ovaska, J.; Juuti, A.; Leivonen, M.; Peromaa-Haavisto, P.; Hurme, S.; Soinio, M.; Nuutila, P.; Victorzon, M. Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Roux-en-Y Gastric Bypass on Weight Loss at 5 Years among Patients with Morbid Obesity: The SLEEVEPASS Randomized Clinical Trial. JAMA 2018, 319, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Peterli, R.; Wölnerhanssen, B.; Peters, T.; Vetter, D.; Kröll, D.; Borbély, Y.; Schultes, B.; Beglinger, C.; Drewe, J.; Schiesser, M.; et al. Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Roux-en-Y Gastric Bypass on Weight Loss in Patients With Morbid Obesity: The SM-BOSS Randomized Clinical Trial. JAMA 2018, 319, 255–265. [Google Scholar] [CrossRef]
- Golzarand, M.; Toolabi, K.; Farid, R. The bariatric surgery and weight losing: A meta-analysis in the long- and very long-term effects of laparoscopic adjustable gastric banding, laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy on weight loss in adults. Surg. Endosc. 2017, 31, 4331–4345. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Ambrosi, J.; Andrada, P.; Valentí, V.; Rotellar, F.; Silva, C.; Catalán, V.; Rodríguez, A.; Ramírez, B.; Moncada, R.; Escalada, J.; et al. Dissociation of body mass index, excess weight loss and body fat percentage trajectories after 3 years of gastric bypass: Relationship with metabolic outcomes. Int. J. Obes. 2017, 41, 1379–1387. [Google Scholar] [CrossRef]
- Courcoulas, A.P.; Christian, N.J.; Belle, S.H.; Berk, P.D.; Flum, D.R.; Garcia, L.; Horlick, M.; Kalarchian, M.A.; King, W.C.; Mitchell, J.E.; et al. Weight Change and Health Outcomes at 3 Years after Bariatric Surgery among Individuals with Severe Obesity. JAMA 2013, 310, 2416–2425. [Google Scholar] [CrossRef] [Green Version]
- Farias, M.M.; Cuevas, A.M.; Rodriguez, F. Set-Point Theory and Obesity. Metab. Syndr. Relat. Disord. 2011, 9, 85–89. [Google Scholar] [CrossRef]
- Melby, C.L.; Paris, H.L.; Foright, R.M.; Peth, J. Attenuating the Biologic Drive for Weight Regain Following Weight Loss: Must What Goes Down Always Go Back Up? Nutrients 2017, 9, 468. [Google Scholar] [CrossRef] [Green Version]
- Miller, G.D.; Norris, A.; Fernandez, A. Changes in Nutrients and Food Groups Intake Following Laparoscopic Roux-en-Y Gastric Bypass (RYGB). Obes. Surg. 2014, 24, 1926–1932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurenius, A.; Larsson, I.; Bueter, M.; Melanson, K.J.; Bosaeus, I.; Forslund, H.B.; Lönroth, H.; Fändriks, L.; Olbers, T. Changes in eating behaviour and meal pattern following Roux-en-Y gastric bypass. Int. J. Obes. 2011, 36, 348–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurenius, A.; Larsson, I.; Melanson, K.J.; Lindroos, A.K.; Lönroth, H.; Bosaeus, I.; Olbers, T. Decreased energy density and changes in food selection following Roux-en-Y gastric bypass. Eur. J. Clin. Nutr. 2013, 67, 168–173. [Google Scholar] [CrossRef]
- Kruseman, M.; Leimgruber, A.; Zumbach, F.; Golay, A. Dietary, Weight, and Psychological Changes among Patients with Obesity, 8 Years after Gastric Bypass. J. Am. Diet. Assoc. 2010, 110, 527–534. [Google Scholar] [CrossRef]
- Giusti, V.; Theytaz, F.; Di Vetta, V.; Clarisse, M.; Suter, M.; Tappy, L. Energy and macronutrient intake after gastric bypass for morbid obesity: A 3-y observational study focused on protein consumption. Am. J. Clin. Nutr. 2015, 103, 18–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sjöström, L.; Lindroos, A.-K.; Peltonen, M.; Torgerson, J.; Bouchard, C.; Carlsson, B.; Dahlgren, S.; Larsson, B.; Narbro, K.; Sjöström, C.D.; et al. Lifestyle, Diabetes, and Cardiovascular Risk Factors 10 Years after Bariatric Surgery. N. Engl. J. Med. 2004, 351, 2683–2693. [Google Scholar] [CrossRef] [PubMed]
- Mathes, C.M.; Spector, A.C. Food selection and taste changes in humans after Roux-en-Y gastric bypass surgery: A direct-measures approach. Physiol. Behav. 2012, 107, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Le Roux, C.W.; Bueter, M.; Theis, N.; Werling, M.; Ashrafian, H.; Löwenstein, C.; Athanasiou, T.; Bloom, S.R.; Spector, A.C.; Olbers, T.; et al. Gastric bypass reduces fat intake and preference. Am. J. Physiol. Integr. Comp. Physiol. 2011, 301, R1057–R1066. [Google Scholar] [CrossRef] [Green Version]
- Shin, A.C.; Zheng, H.; Pistell, P.J.; Berthoud, H.-R. Roux-en-Y gastric bypass surgery changes food reward in rats. Int. J. Obes. 2010, 35, 642–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathes, C.M.; Bohnenkamp, R.A.; Blonde, G.D.; Letourneau, C.; Corteville, C.; Bueter, M.; Lutz, T.A.; le Roux, C.W.; Spector, A.C. Gastric bypass in rats does not decrease appetitive behavior towards sweet or fatty fluids despite blunting preferential intake of sugar and fat. Physiol. Behav. 2015, 142, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathes, C.M.; Letourneau, C.; Blonde, G.D.; Le Roux, C.W.; Spector, A.C. Roux-en-Y gastric bypass in rats progressively decreases the proportion of fat calories selected from a palatable cafeteria diet. Am. J. Physiol. Integr. Comp. Physiol. 2016, 310, R952–R959. [Google Scholar] [CrossRef] [Green Version]
- Olbers, T.; Björkman, S.; Lindroos, A.; Maleckas, A.; Lönn, L.L.; Sjöström, L.; Lönroth, H. Body Composition, Dietary Intake, and Energy Expenditure After Laparoscopic Roux-en-Y Gastric Bypass and Laparoscopic Vertical Banded Gastroplasty. Ann. Surg. 2006, 244, 715–722. [Google Scholar] [CrossRef]
- Ullrich, J.; Ernst, B.; Wilms, B.; Thurnheer, M.; Schultes, B. Roux-en Y Gastric Bypass Surgery Reduces Hedonic Hunger and Improves Dietary Habits in Severely Obese Subjects. Obes. Surg. 2012, 23, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Ernst, B.; Thurnheer, M.; Wilms, B.; Schultes, B. Differential Changes in Dietary Habits after Gastric Bypass versus Gastric Banding Operations. Obes. Surg. 2008, 19, 274–280. [Google Scholar] [CrossRef]
- Schoeller, D.A. Limitations in the assessment of dietary energy intake by self-report. Metabolism 1995, 44, 18–22. [Google Scholar] [CrossRef]
- Hill, R.; Davies, P.S.W. The validity of self-reported energy intake as determined using the doubly labelled water technique. Br. J. Nutr. 2001, 85, 415–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poppitt, S.; Swann, D.; Black, A.; Prentice, A. Assessment of selective under-reporting of food intake by both obese and non-obese women in a metabolic facility. Int. J. Obes. Relat. Metab. Disord. 1998, 22, 303–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapoor, N.; Al-Najim, W.; Le Roux, C.W.; Docherty, N.G. Shifts in Food Preferences after Bariatric Surgery: Observational Reports and Proposed Mechanisms. Curr. Obes. Rep. 2017, 6, 246–252. [Google Scholar] [CrossRef]
- Behary, P.; Miras, A. Food preferences and underlying mechanisms after bariatric surgery. Proc. Nutr. Soc. 2015, 74, 419–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schier, L.A.; Spector, A.C. The Functional and Neurobiological Properties of Bad Taste. Physiol. Rev. 2019, 99, 605–663. [Google Scholar] [CrossRef]
- Abdeen, G.; Le Roux, C.W. Mechanism Underlying the Weight Loss and Complications of Roux-en-Y Gastric Bypass. Review. Obes. Surg. 2015, 26, 410–421. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, M.S.; Christensen, B.J.; Ritz, C.; Rasmussen, S.; Hansen, T.T.; Bredie, W.L.P.; le Roux, C.W.; Sjödin, A.; Schmidt, J.B. Roux-En-Y Gastric Bypass and Sleeve Gastrectomy Does Not Affect Food Preferences When Assessed by an Ad libitum Buffet Meal. Obes. Surg. 2017, 27, 2599–2605. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.S.; Rasmussen, S.; Christensen, B.J.; Ritz, C.; le Roux, C.W.; Schmidt, J.B.; Sjödin, A. Bariatric Surgery Does Not Affect Food Preferences, but Individual Changes in Food Preferences May Predict Weight Loss. Obesity 2018, 26, 1879–1887. [Google Scholar] [CrossRef] [Green Version]
- Geiselman, P.J.; Anderson, A.M.; Dowdy, M.L.; West, D.B.; Redmann, S.M.; Smith, S.R. Reliability and Validity of a Macronutrient Self-Selection Paradigm and a Food Preference Questionnaire. Physiol. Behav. 1998, 63, 919–928. [Google Scholar] [CrossRef]
- Neff, K.J.H.; Le Roux, C. Bariatric surgery: A best practice article. J. Clin. Pathol. 2012, 66, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, E.J.; Augustin, J.L.; Schaefer, M.M.; Rasmussen, H.; Ordovas, J.; Dallal, G.E.; Dwyer, J. Lack of efficacy of a food-frequency questionnaire in assessing dietary macronutrient intakes in subjects consuming diets of known composition. Am. J. Clin. Nutr. 2000, 71, 746–751. [Google Scholar] [CrossRef]
- MacDiarmid, J.; Blundell, J. Assessing dietary intake: Who, what and why of under-reporting. Nutr. Res. Rev. 1998, 11, 231–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coluzzi, I.; Raparelli, L.; Guarnacci, L.; Paone, E.; Del Genio, G.; Le Roux, C.W.; Silecchia, G. Food Intake and Changes in Eating Behavior After Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2016, 26, 2059–2067. [Google Scholar] [CrossRef] [PubMed]
- Kenler, H.; E Brolin, R.; Cody, R.P. Changes in eating behavior after horizontal gastroplasty and Roux-en-Y gastric bypass. Am. J. Clin. Nutr. 1990, 52, 87–92. [Google Scholar] [CrossRef]
- Netto, B.D.M.; Earthman, C.P.; Farias, G.; Masquio, D.C.L.; Clemente, A.P.G.; Peixoto, P.; Bettini, S.C.; von Der Heyde, M.E.; Dâmaso, A.R. Eating patterns and food choice as determinant of weight loss and improvement of metabolic profile after RYGB. Nutrition 2017, 33, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Brolin, R.E.; Gorman, J.H.; Gorman, R.C.; Petschenik, A.J.; Bradley, L.J.; Kenler, H.A.; Cody, R.P. Are vitamin B12 and folate deficiency clinically important after roux-en-Y gastric bypass? J. Gastrointest. Surg. 1998, 2, 436–442. [Google Scholar] [CrossRef]
- Halmi, K.; Mason, E.; Falk, J.R.; Stunkard, A. Appetitive behavior after gastric bypass for obesity. Int. J. Obes. 1981, 5, 457–464. [Google Scholar]
- Al-Najim, W.; Docherty, N.G.; le Roux, C.W. Food Intake and Eating Behavior after Bariatric Surgery. Physiol. Rev. 2018, 98, 1113–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trostler, N.; Mann, A.; Zilberbush, N.; Avinoach, E.; Charuzi, I. Weight Loss and Food Intake 18 Months following Vertical Banded Gastroplasty or Gastric Bypass for Severe Obesity. Obes. Surg. 1995, 5, 39–51. [Google Scholar] [CrossRef]
- Zoon, H.F.; de Bruijn, S.E.; Smeets, P.A.; de Graaf, C.; Janssen, I.M.; Schijns, W.; Aarts, E.O.; Jager, G.; Boesveldt, S. Altered neural responsivity to food cues in relation to food preferences, but not appetite-related hormone concentrations after RYGB-surgery. Behav. Brain Res. 2018, 353, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.S.; Ritz, C.; Albrechtsen, N.J.W.; Holst, J.J.; le Roux, C.W.; Sjödin, A. Oxyntomodulin and Glicentin May Predict the Effect of Bariatric Surgery on Food Preferences and Weight Loss. J. Clin. Endocrinol. Metab. 2020, 105, e1064–e1074. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.; Peters, K.Z.; Denton, B.S.; Lee, K.A.; Chadchankar, H.; McCutcheon, J.E. Restriction of dietary protein leads to conditioned protein preference and elevated palatability of protein-containing food in rats. Physiol. Behav. 2017, 184, 235–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsanos, C.S.; Madura, J.A.; Roust, L.R. Essential amino acid ingestion as an efficient nutritional strategy for the preservation of muscle mass following gastric bypass surgery. Nutrition 2015, 32, 9–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathes, C.M.; Bohnenkamp, R.A.; Le Roux, C.; Spector, A.C. Reduced sweet and fatty fluid intake after Roux-en-Y gastric bypass in rats is dependent on experience without change in stimulus motivational potency. Am. J. Physiol. Integr. Comp. Physiol. 2015, 309, R864–R874. [Google Scholar] [CrossRef]
- Spector, A.C.; Kapoor, N.; Price, R.K.; Pepino, M.Y.; Livingstone, M.B.E.; Le Roux, C.W. Proceedings from the 2018 Association for Chemoreception Annual Meeting Symposium: Bariatric Surgery and Its Effects on Taste and Food Selection. Chem. Senses 2018, 44, 155–163. [Google Scholar] [CrossRef] [PubMed]



| Macronutrient Self-Selection Paradigm | |||
|---|---|---|---|
| High Simple Sugar | High Complex CHO | Low CHO/High Protein | |
| High Fat | Three foods | Three foods | Three foods |
| Fat > 40% | Fat > 40% | Fat > 40% | |
| Sugar > 30% | Comp Carb > 30% | Protein > 13% | |
| Low Fat | Three foods | Three foods | Three foods |
| Fat < 20% | Fat < 20% | Fat < 20% | |
| Sugar > 30% | Comp Carb > 30% | Protein > 13% | |
| Parameter | Values |
|---|---|
| Male/Female | 4/10 |
| Age (years) | 51.0 ± 7.8 |
| Body weight (kg) | 136 ± 23.8 |
| BMI (kg/m2) | 50.1 ± 7.8 |
| Waist Circumference (cm) | 140.5 ± 14.7 |
| Pre-Surgery | 24 Months Post-Surgery | Mean Difference (95% CI) | p-Value | |
|---|---|---|---|---|
| Total food intake (kJ) | 6510.3 ± 756.5 | 2540.1 ± 431.0 | −3971.8 (−5234.2 to −2707.1) | <0.01 |
| Intake from macronutrients | ||||
| Fat (kJ) | 2617.1 ± 318.8 | 1066.9 ± 225.5 | −1548.1 (−524.8 to −216.1) | <0.01 |
| Sugar (kJ) | 1312.5 ± 288.3 | 421.7 ± 115.9 | −890.8 (2195.7 to −334.5) | <0.01 |
| Total Carbohydrates (kJ) | 3102.4 ± 455.6 | 1013.8 ± 220.9 | −2088.7 (−2888.2 to −1289.1) | <0.01 |
| Protein (kJ) | 833.9 ± 87.0 | 472.8 ± 58.2 | −558.1 (−558.1 to −163.2) | <0.01 |
| Pre-Surgery | 24 Months Post-Surgery | Mean Difference | 95% CI | |
|---|---|---|---|---|
| Fat (%) | 40.6 ± 11.6 | 38.3 ± 18.1 | −2.26 | −14.1 to 9.5 |
| Sugar (%) | 18.7 ± 8.7 | 15.5 ± 12.1 | −3.15 | −13.1 to 6.8 |
| Total Carbohydrates (%) | 46.4 ± 10.5 | 38.4 ± 17.2 | −8.02 | −20.9 to 4.9 |
| Protein (%) | 13.4 ± 3.7 | 24.1 ± 17.4 | +10.72 | 0.3 to 21.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapoor, N.; al Najim, W.; Menezes, C.; Price, R.K.; O’Boyle, C.; Bodnar, Z.; Spector, A.C.; Docherty, N.G.; le Roux, C.W. A Comparison of Total Food Intake at a Personalised Buffet in People with Obesity, before and 24 Months after Roux-en-Y-Gastric Bypass Surgery. Nutrients 2021, 13, 3873. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113873
Kapoor N, al Najim W, Menezes C, Price RK, O’Boyle C, Bodnar Z, Spector AC, Docherty NG, le Roux CW. A Comparison of Total Food Intake at a Personalised Buffet in People with Obesity, before and 24 Months after Roux-en-Y-Gastric Bypass Surgery. Nutrients. 2021; 13(11):3873. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113873
Chicago/Turabian StyleKapoor, Natasha, Werd al Najim, Camilo Menezes, Ruth K Price, Colm O’Boyle, Zsolt Bodnar, Alan C Spector, Neil G Docherty, and Carel W le Roux. 2021. "A Comparison of Total Food Intake at a Personalised Buffet in People with Obesity, before and 24 Months after Roux-en-Y-Gastric Bypass Surgery" Nutrients 13, no. 11: 3873. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113873