
Association between Vitamin D and Heart Failure Mortality in 10,974 Hospitalized Individuals

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
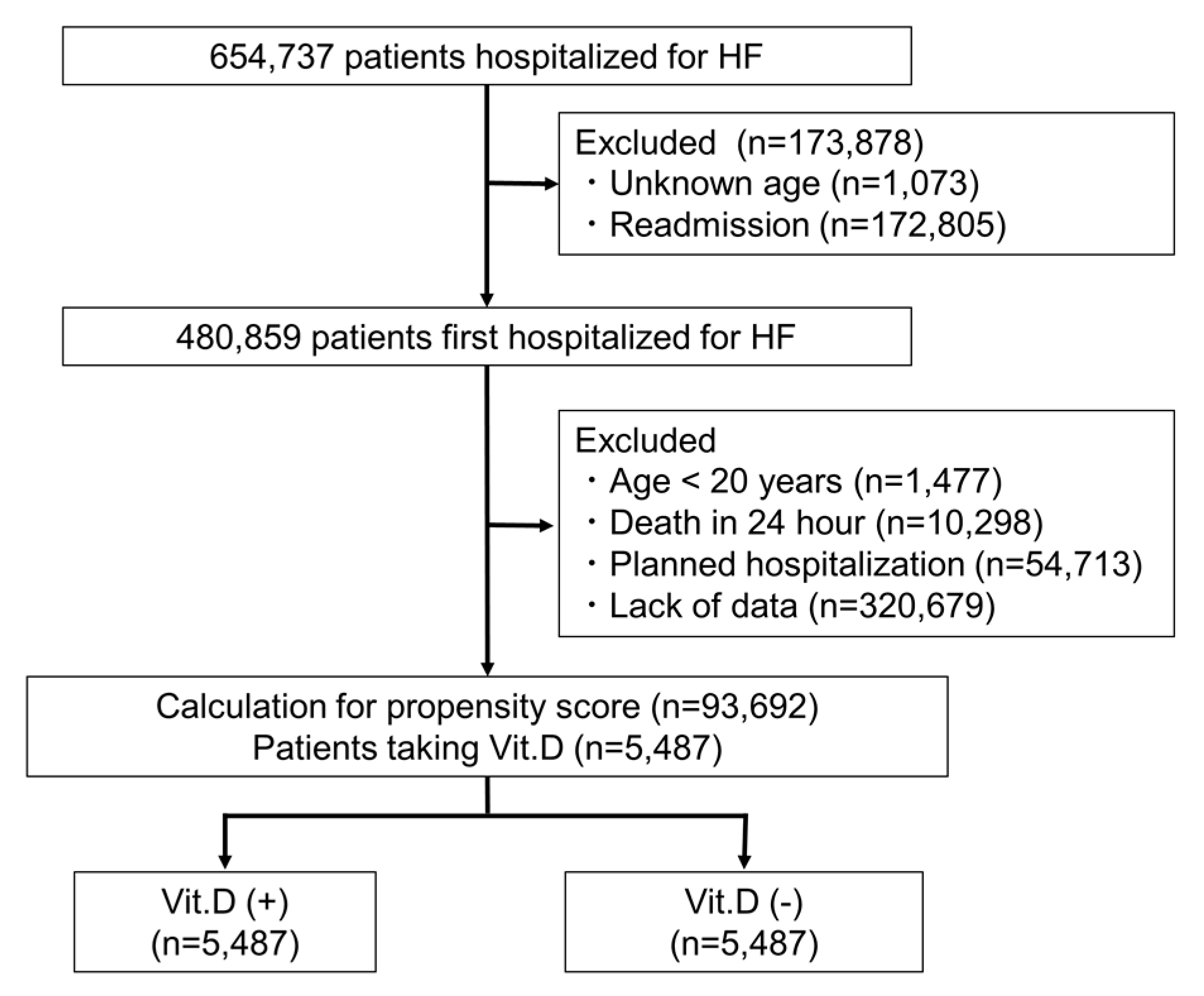
2.1. Study Population
2.2. Clinical Outcomes
2.3. Sample Matching
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
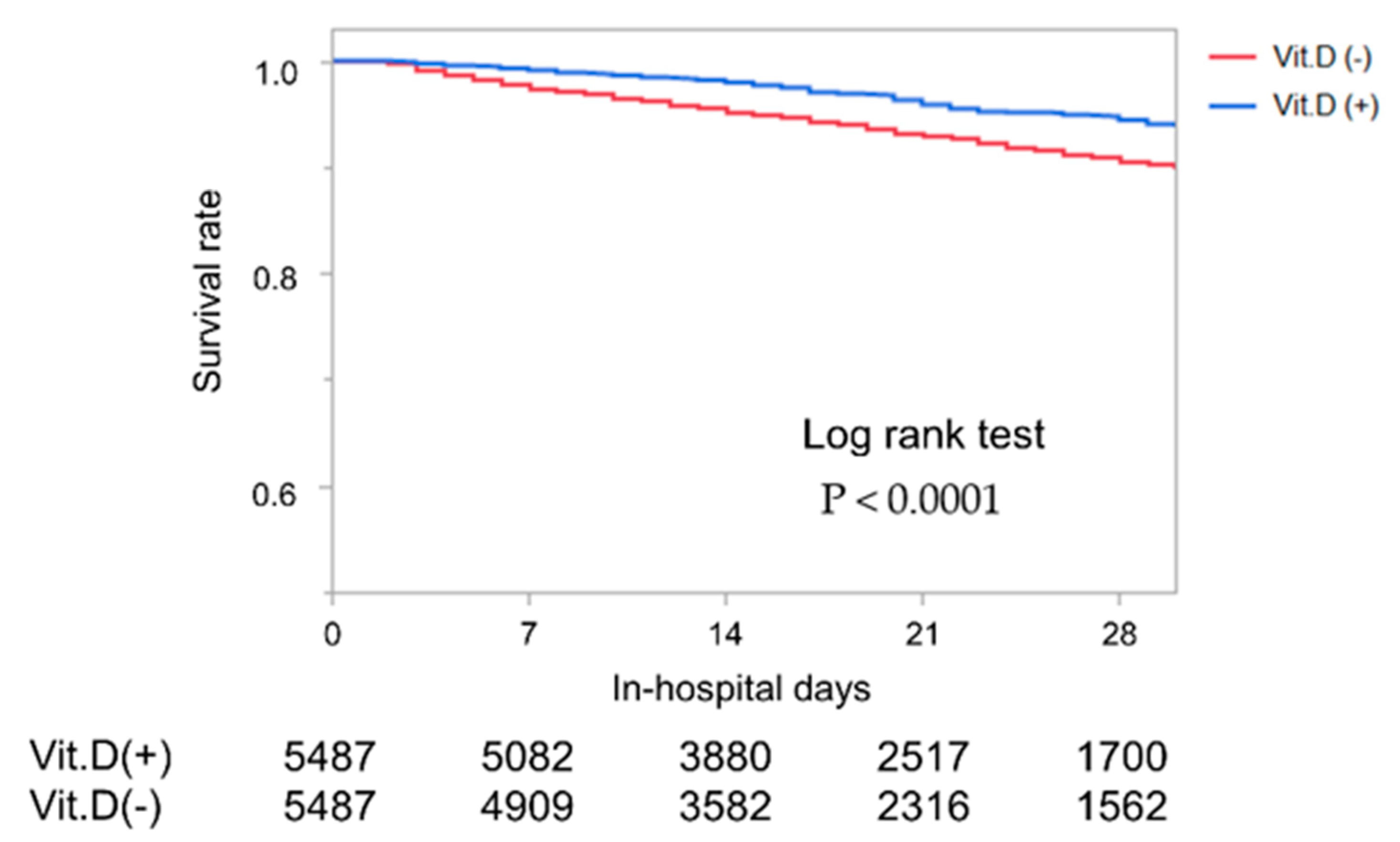
3.2. Outcomes
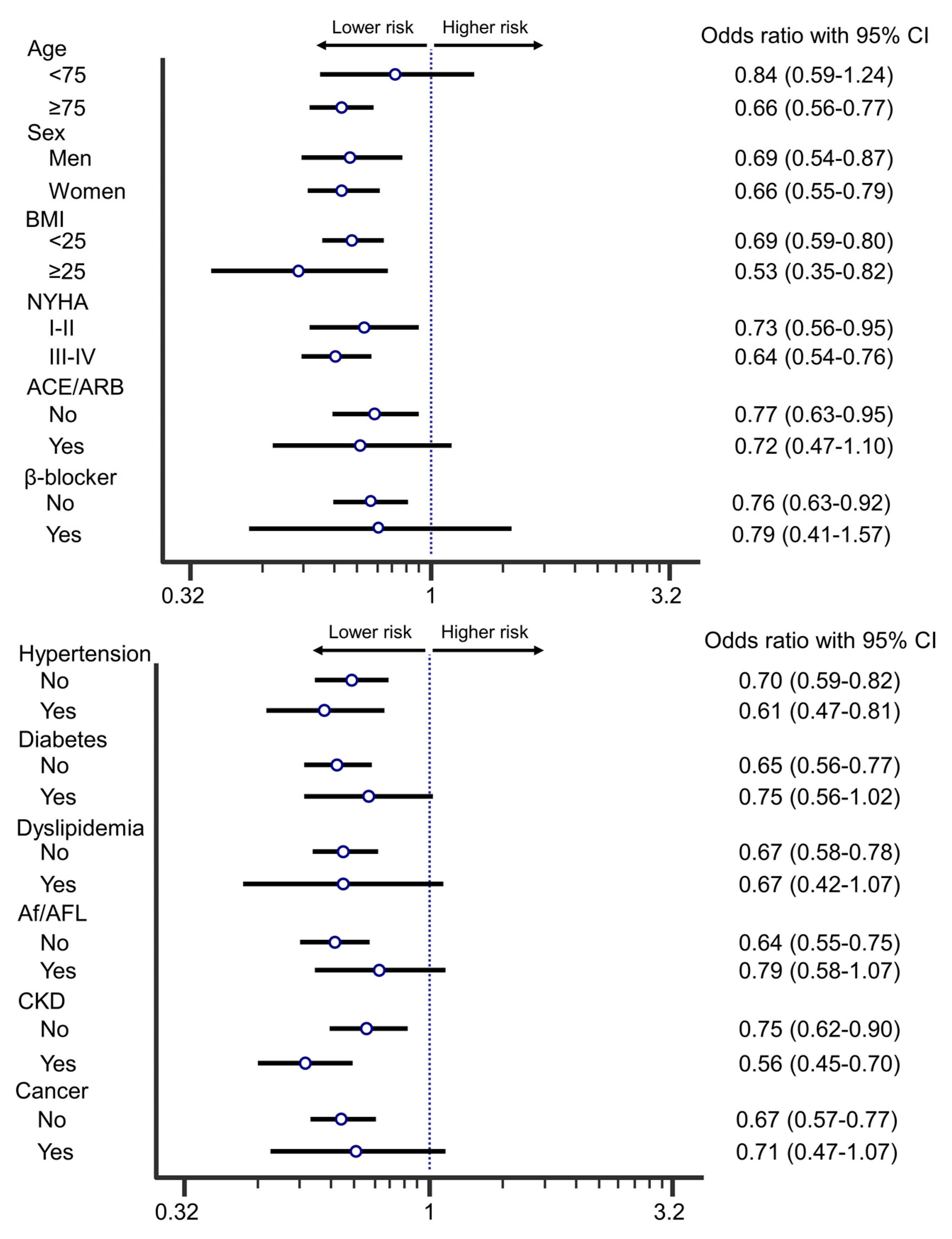
3.3. Subgroup-Analysis
4. Discussion
4.1. Impact of Vitamin D on HF Mortality
4.2. Mechanisms of Vitamin D for HF
4.3. Clinical Implication
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsutsui, H.; Isobe, M.; Ito, H.; Okumura, K.; Ono, M.; Kitakaze, M.; Kinugawa, K.; Kihara, Y.; Goto, Y.; Komuro, I.; et al. JCS 2017/JHFS 2017 Guideline on Diagnosis and Treatment of Acute and Chronic Heart Failure- Digest Version. Circ. J. 2019, 83, 2084–2184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidenreich, P.A.; Albert, N.M.; Allen, L.A.; Bluemke, D.A.; Butler, J.; Fonarow, G.C.; Ikonomidis, J.S.; Khavjou, O.; Konstam, M.A.; Maddox, T.M.; et al. Forecasting the impact of heart failure in the United States: A policy statement from the American Heart Association. Circ. Heart Fail. 2013, 6, 606–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.J. Vitamin D and Cardiovascular Disease. Annu. Rev. Med. 2016, 67, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Krul-Poel, Y.H.; Ter Wee, M.M.; Lips, P.; Simsek, S. Management of Endocrine Disease: The effect of vitamin D supplementation on glycaemic control in patients with type 2 diabetes mellitus: A systematic review and meta-analysis. Eur. J. Endocrinol. 2017, 176, R1–R14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewison, M. An update on vitamin D and human immunity. Clin. Endocrinol. 2012, 76, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Sabour, S.; Sagar, U.N.; Adams, S.; Whellan, D.J. Prevalence of hypovitaminosis D in cardiovascular diseases (from the National Health and Nutrition Examination Survey 2001 to 2004). Am. J. Cardiol. 2008, 102, 1540–1544. [Google Scholar] [CrossRef] [PubMed]
- Ameri, P.; Ronco, D.; Casu, M.; Denegri, A.; Bovio, M.; Menoni, S.; Ferone, D.; Murialdo, G. High prevalence of vitamin D deficiency and its association with left ventricular dilation: An echocardiography study in elderly patients with chronic heart failure. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 633–640. [Google Scholar] [CrossRef]
- Gardner, D.G.; Chen, S.; Glenn, D.J. Vitamin D and the heart. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 305, R969–R977. [Google Scholar] [CrossRef]
- Schleithoff, S.S.; Zittermann, A.; Tenderich, G.; Berthold, H.K.; Stehle, P.; Koerfer, R. Vitamin D supplementation improves cytokine profiles in patients with congestive heart failure: A double-blind, randomized, placebo-controlled trial. Am. J. Clin. Nutr. 2006, 83, 754–759. [Google Scholar] [CrossRef]
- Witham, M.D.; Crighton, L.J.; Gillespie, N.D.; Struthers, A.D.; McMurdo, M.E. The effects of vitamin D supplementation on physical function and quality of life in older patients with heart failure: A randomized controlled trial. Circ. Heart Fail. 2010, 3, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Witte, K.K.; Byrom, R.; Gierula, J.; Paton, M.F.; Jamil, H.A.; Lowry, J.E.; Gillott, R.G.; Barnes, S.A.; Chumun, H.; Kearney, L.C.; et al. Effects of Vitamin D on Cardiac Function in Patients With Chronic HF: The VINDICATE Study. J. Am. Coll. Cardiol. 2016, 67, 2593–2603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Win, S.; Hussain, I.; Hebl, V.B.; Dunlay, S.M.; Redfield, M.M. Inpatient Mortality Risk Scores and Postdischarge Events in Hospitalized Heart Failure Patients: A Community-Based Study. Circ. Heart Fail. 2017, 10. [Google Scholar] [CrossRef] [PubMed]
- Peterson, P.N.; Rumsfeld, J.S.; Liang, L.; Albert, N.M.; Hernandez, A.F.; Peterson, E.D.; Fonarow, G.C.; Masoudi, F.A.; American Heart Association Get With the Guidelines-Heart Failure Program. A validated risk score for in-hospital mortality in patients with heart failure from the American Heart Association get with the guidelines program. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hannan, E.L.; Wu, C.; Bennett, E.V.; Carlson, R.E.; Culliford, A.T.; Gold, J.P.; Higgins, R.S.; Smith, C.R.; Jones, R.H. Risk index for predicting in-hospital mortality for cardiac valve surgery. Ann. Thorac. Surg. 2007, 83, 921–929. [Google Scholar] [CrossRef]
- Fonarow, G.C. Clinical risk prediction tools in patients hospitalized with heart failure. Rev. Cardiovasc. Med. 2012, 13, e14–e23. [Google Scholar]
- Gaksch, M.; Jorde, R.; Grimnes, G.; Joakimsen, R.; Schirmer, H.; Wilsgaard, T.; Mathiesen, E.B.; Njolstad, I.; Lochen, M.L.; Marz, W.; et al. Vitamin D and mortality: Individual participant data meta-analysis of standardized 25-hydroxyvitamin D in 26916 individuals from a European consortium. PLoS ONE 2017, 12, e0170791. [Google Scholar] [CrossRef] [Green Version]
- Jiang, W.L.; Gu, H.B.; Zhang, Y.F.; Xia, Q.Q.; Qi, J.; Chen, J.C. Vitamin D Supplementation in the Treatment of Chronic Heart Failure: A Meta-analysis of Randomized Controlled Trials. Clin. Cardiol. 2016, 39, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Barbarawi, M.; Kheiri, B.; Zayed, Y.; Barbarawi, O.; Dhillon, H.; Swaid, B.; Yelangi, A.; Sundus, S.; Bachuwa, G.; Alkotob, M.L. Vitamin D supplementation and cardiovascular disease risks in more than 83,000 individuals in 21 randomized clinical trials: A meta-analysis. JAMA Cardiol. 2019, 4, 765–775. [Google Scholar] [CrossRef]
- Stuart, E.A.; Bradshaw, C.P.; Leaf, P.J. Assessing the generalizability of randomized trial results to target populations. Prev. Sci. 2015, 16, 475–485. [Google Scholar] [CrossRef] [Green Version]
- Davies, N.M.; Holmes, M.V.; Davey Smith, G. Reading Mendelian randomisation studies: A guide, glossary, and checklist for clinicians. BMJ 2018, 362, k601. [Google Scholar] [CrossRef] [Green Version]
- Weishaar, R.E.; Simpson, R.U. Involvement of vitamin D3 with cardiovascular function. II. Direct and indirect effects. Am. J. Physiol. 1987, 253, E675–E683. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Law, C.S.; Grigsby, C.L.; Olsen, K.; Hong, T.T.; Zhang, Y.; Yeghiazarians, Y.; Gardner, D.G. Cardiomyocyte-specific deletion of the vitamin D receptor gene results in cardiac hypertrophy. Circulation 2011, 124, 1838–1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaidya, A.; Williams, J.S. The relationship between vitamin D and the renin-angiotensin system in the pathophysiology of hypertension, kidney disease, and diabetes. Metabolism 2012, 61, 450–458. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Leung, D.Y.; Richers, B.N.; Liu, Y.; Remigio, L.K.; Riches, D.W.; Goleva, E. Vitamin D inhibits monocyte/macrophage proinflammatory cytokine production by targeting MAPK phosphatase-1. J. Immunol. 2012, 188, 2127–2135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caprio, M.; Mammi, C.; Rosano, G.M. Vitamin D: A novel player in endothelial function and dysfunction. Arch. Med. Sci. 2012, 8, 4–5. [Google Scholar] [CrossRef]
- Schluter, K.D.; Piper, H.M. Left ventricular hypertrophy and parathyroid hormone: A causal connection? Cardiovasc. Res. 1998, 39, 523–524. [Google Scholar] [CrossRef]
- Haden, S.T.; Brown, E.M.; Hurwitz, S.; Scott, J.; El-Hajj Fuleihan, G. The effects of age and gender on parathyroid hormone dynamics. Clin. Endocrinol. 2000, 52, 329–338. [Google Scholar] [CrossRef]
- Yamana, H.; Moriwaki, M.; Horiguchi, H.; Kodan, M.; Fushimi, K.; Yasunaga, H. Validity of diagnoses, procedures, and laboratory data in Japanese administrative data. J. Epidemiol. 2017, 27, 476–482. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Non Matching | Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| All | Vit.D (+) | Vit.D (−) | std.diff (%) | Vit.D (+) | Vit.D (−) | std.diff (%) | ||
| Number | (n = 93,692) | (n = 5487) | (n = 88,205) | (n = 5487) | (n = 5487) | |||
| Age average(years) | 79 ± 12 | 80 ± 11 | 79 ± 13 | 10.6 | 80 ± 11 | 81 ± 11 | 8.4 | |
| Age(%) | 20–30 | 0.2 | 0.1 | 0.2 | −1.7 | 0.1 | 0.1 | 2.7 |
| 30–40 | 0.8 | 0.4 | 0.8 | −6.2 | 0.4 | 0.4 | −0.2 | |
| 40–50 | 2.4 | 1.4 | 2.4 | −7.8 | 1.4 | 1.1 | 2.5 | |
| 50–60 | 4.8 | 3.6 | 4.8 | −6.3 | 3.6 | 3.1 | 2.6 | |
| 60–70 | 12.1 | 10.8 | 12.2 | −4.4 | 10.8 | 9.8 | 3.3 | |
| 70–80 | 23.0 | 23.8 | 22.9 | 2.0 | 23.8 | 22.1 | 3.9 | |
| 80–90 | 39.8 | 42.4 | 39.7 | 5.5 | 42.4 | 44.2 | −3.8 | |
| >90 | 17.0 | 17.6 | 17.0 | 1.7 | 17.6 | 19.3 | −4.2 | |
| Male (%) | 52.2 | 33.9 | 53.4 | −40.1 | 33.9 | 31.4 | 5.3 | |
| BMI | 22.7 ± 5.0 | 21.8 ± 4.1 | 22.7 ± 5.0 | −20.8 | 21.8 ± 4.1 | 21.7 ± 4.1 | 1.9 | |
| Smoking | 30.2 | 21.1 | 30.8 | −22.1 | 21.1 | 18.9 | 5.7 | |
| NYHA | 1 | 12.2 | 12.8 | 12.2 | 1.9 | 12.8 | 13.2 | −1.0 |
| 2 | 24.4 | 24.5 | 24.3 | 0.3 | 24.5 | 25.0 | −1.2 | |
| 3 | 32.2 | 32.1 | 32.2 | −0.2 | 32.1 | 31.8 | 0.8 | |
| 4 | 31.2 | 30.5 | 31.2 | −1.5 | 30.5 | 30.0 | 1.1 | |
| Comorbidities (%) | ||||||||
| Hypertension | 52.9 | 48.8 | 53.2 | −8.8 | 48.8 | 47.8 | 2.0 | |
| Diabetes mellitus | 26.8 | 26.1 | 26.8 | −1.7 | 26.1 | 25.1 | 2.2 | |
| Dyslipidemia | 18.6 | 16.2 | 18.8 | −6.7 | 16.2 | 14.9 | 3.7 | |
| Osteoporosis | 3.0 | 24.5 | 1.7 | 72.1 | 24.5 | 21.2 | 7.1 | |
| Hypoparathyroidism | <0.1 | 0.2 | <0.1 | 5.0 | 0.2 | <0.1 | 4.5 | |
| HCM | 3.4 | 1.4 | 3.5 | −14.1 | 1.4 | 1.6 | −2.0 | |
| DCM | 1.2 | 1.0 | 1.3 | −2.9 | 1.0 | 1.2 | −2.8 | |
| Cardiac Amyloidosis | 0.1 | 0.1 | 0.1 | −0.8 | 0.1 | 0.1 | <0.1 | |
| Cardiac Sarcoidosis | 0.3 | 0.5 | 0.3 | 3.0 | 0.5 | 0.2 | 4.5 | |
| Af/AFL | 35.5 | 27.5 | 36.0 | −18.3 | 27.5 | 27.2 | 0.8 | |
| AT | 0.9 | 0.6 | 0.9 | −2.9 | 0.6 | 0.7 | −0.9 | |
| Stroke | 8.3 | 7.5 | 8.3 | −3.3 | 7.5 | 7.2 | 1.1 | |
| MI | 10.3 | 7.9 | 10.5 | −9.1 | 7.9 | 7.2 | 2.6 | |
| PVD | 3.8 | 4.8 | 3.7 | 5.1 | 4.8 | 3.9 | 4.3 | |
| CKD | 14.1 | 38.6 | 12.6 | 62.5 | 38.6 | 35.3 | 6.9 | |
| Liver failure | 0.1 | 0.1 | 0.1 | −0.8 | 0.1 | 0.2 | −2.7 | |
| COPD | 7.4 | 6.1 | 7.5 | −5.6 | 6.1 | 5.3 | 3.6 | |
| RA | 1.3 | 4.2 | 1.2 | 19.0 | 4.2 | 4.9 | −3.2 | |
| Dementia | 6.2 | 6.9 | 6.2 | 3.1 | 6.9 | 7.0 | −0.4 | |
| Cancer | 11.0 | 11.0 | 11.0 | 0.1 | 11.0 | 10.6 | 1.3 | |
| Treatment (%) | ||||||||
| Catecholamine | 12.4 | 11.3 | 12.5 | −3.8 | 11.3 | 10.6 | 2.1 | |
| IABP | 1.0 | 0.9 | 1.0 | −1.1 | 0.9 | 1.1 | −1.7 | |
| PCPS | 0.1 | 0.0 | 0.2 | −3.6 | 0.0 | 0.1 | −0.5 | |
| Artificial Ventilation | 21.3 | 21.1 | 21.3 | −0.5 | 21.1 | 20.8 | 0.7 | |
| Hemodialysis | 4.6 | 29.5 | 3.1 | 76.8 | 29.5 | 28.3 | 2.6 | |
| PCI | 4.9 | 5.2 | 4.9 | 1.6 | 5.2 | 5.1 | 0.7 | |
| Drug (%) | ||||||||
| ACE-i/ARB | 19.7 | 19.4 | 19.8 | −0.8 | 19.4 | 21.0 | −3.9 | |
| βblocker | 9.1 | 8.0 | 9.2 | −4.1 | 8.0 | 8.6 | −1.9 | |
| Loop diuretic | 19.4 | 18.4 | 19.4 | −2.6 | 18.4 | 20.3 | −4.8 | |
| K-sparing diuretic | 10.1 | 7.4 | 10.3 | −10.3 | 7.4 | 8.4 | −3.7 | |
| Statin | 13.1 | 13.5 | 13.0 | 1.2 | 13.5 | 13.7 | −0.7 | |
| Hospital length (days) | 18 (12–28) | 19 (12–31) | 17 (12–27) | 13.1 | 19 (12–31) | 18 (11–30) | 14.9 | |
| Non Matching | Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| In-Hospital Mortality | Vit.D (+) | Vit.D (−) | OR (95%CI) | p-Value | Vit.D (+) | Vit.D (−) | OR (95%CI) | p-Value |
| Total (%) | 357 (6.5) | 7256 (8.2) | 0.79 (0.71–0.88) | <0.0001 | 357 (6.5) | 515 (9.4) | 0.67 (0.58–0.77) | <0.0001 |
| 7 days (%) | 48 (0.9) | 1761 (2.0) | 0.44 (0.33–0.58) | <0.0001 | 48 (0.9) | 138 (2.5) | 0.34 (0.25–0.48) | <0.0001 |
| 30 days (%) | 207 (3.8) | 5171 (5.9) | 0.64 (0.55–0.73) | <0.0001 | 207 (3.8) | 358 (6.5) | 0.56 (0.47–0.67) | <0.0001 |
| A: In all patients. See abbreviations in Table 1. | ||||
| All | ||||
| OR | Lower | Higher | p | |
| Vit.D | 0.63 | 0.49 | 0.81 | 0.0003 |
| Age | 1.06 | 1.05 | 1.08 | <0.0001 |
| BMI | 0.93 | 0.90 | 0.96 | <0.0001 |
| NYHA | 1.18 | 1.04 | 1.33 | 0.0070 |
| Male | 1.00 | 0.74 | 1.35 | 0.9884 |
| Smoking | 0.93 | 0.67 | 1.31 | 0.6867 |
| HT | 0.39 | 0.30 | 0.51 | <0.0001 |
| DM | 0.80 | 0.60 | 1.07 | 0.1398 |
| DL | 0.83 | 0.57 | 1.22 | 0.3445 |
| MI | 1.17 | 0.76 | 1.80 | 0.4721 |
| PVD | 1.88 | 1.19 | 2.96 | 0.0064 |
| Stroke | 0.96 | 0.62 | 1.50 | 0.8659 |
| Dementia | 1.21 | 0.78 | 1.87 | 0.4000 |
| COPD | 0.95 | 0.56 | 1.59 | 0.8370 |
| RA | 1.10 | 0.65 | 1.89 | 0.7187 |
| CKD | 1.65 | 1.19 | 2.30 | 0.0030 |
| Cancer | 0.84 | 0.57 | 1.24 | 0.3764 |
| Hemodialysis | 0.84 | 0.58 | 1.22 | 0.3669 |
| Artificial Ventilation | 2.55 | 1.95 | 3.33 | <0.0001 |
| PCI | 0.22 | 0.10 | 0.47 | <0.0001 |
| IABP | 1.04 | 0.44 | 2.43 | 0.9355 |
| Catecholamines | 4.59 | 3.50 | 6.02 | <0.0001 |
| Osteoporosis | 0.76 | 0.48 | 1.19 | 0.2331 |
| HCM | 0.61 | 0.18 | 2.09 | 0.4338 |
| Sarcoidosis | 2.60 | 0.55 | 12.18 | 0.2253 |
| Af/AFL | 0.68 | 0.51 | 0.92 | 0.0107 |
| B: In patients with vitamin D supplementation. See abbreviations in Table 1. | ||||
| Vitamin D (+) | ||||
| OR | Lower | Higher | p | |
| Age | 1.07 | 1.04 | 1.09 | <0.0001 |
| BMI | 0.97 | 0.92 | 1.02 | 0.2186 |
| NYHA | 1.22 | 1.01 | 1.48 | 0.0379 |
| Male | 0.62 | 0.37 | 1.02 | 0.0589 |
| Smoking | 1.10 | 0.64 | 1.87 | 0.7396 |
| HT | 0.33 | 0.22 | 0.52 | <0.0001 |
| DM | 0.70 | 0.44 | 1.11 | 0.1257 |
| DL | 1.11 | 0.64 | 1.90 | 0.7187 |
| MI | 1.36 | 0.71 | 2.59 | 0.3519 |
| PVD | 2.24 | 1.18 | 4.27 | 0.0138 |
| Stroke | 1.25 | 0.66 | 2.37 | 0.4844 |
| Dementia | 1.17 | 0.59 | 2.31 | 0.6536 |
| COPD | 0.86 | 0.38 | 1.94 | 0.7122 |
| RA | 0.80 | 0.30 | 2.12 | 0.6558 |
| CKD | 1.68 | 0.95 | 2.99 | 0.0746 |
| Cancer | 1.09 | 0.60 | 1.98 | 0.7663 |
| Hemodialysis | 0.98 | 0.52 | 1.85 | 0.9510 |
| Artificial Ventilation | 2.18 | 1.44 | 3.31 | 0.0003 |
| PCI | 0.19 | 0.06 | 0.64 | 0.0075 |
| IABP | 1.34 | 0.40 | 4.49 | 0.6352 |
| Catecholamines | 4.91 | 3.24 | 7.43 | <0.0001 |
| Osteoporosis | 0.61 | 0.36 | 1.04 | 0.0707 |
| HCM | 1.57 | 0.34 | 7.23 | 0.5659 |
| Sarcoidosis | 2.14 | 0.26 | 17.31 | 0.4763 |
| Af/AFL | 0.66 | 0.41 | 1.06 | 0.0822 |
| C: In patients without vitamin D supplementation. See abbreviations in Table 1. | ||||
| Vitamin D (−) | ||||
| OR | Lower | Higher | p | |
| Age | 1.07 | 1.04 | 1.09 | <0.0001 |
| BMI | 0.91 | 0.87 | 0.95 | <0.0001 |
| NYHA | 1.14 | 0.97 | 1.33 | 0.1111 |
| Male | 1.36 | 0.93 | 2.01 | 0.1153 |
| Smoking | 0.83 | 0.54 | 1.30 | 0.4209 |
| HT | 0.43 | 0.30 | 0.60 | <0.0001 |
| DM | 0.87 | 0.59 | 1.28 | 0.4857 |
| DL | 0.64 | 0.37 | 1.10 | 0.1087 |
| MI | 1.06 | 0.59 | 1.90 | 0.8573 |
| PVD | 1.53 | 0.79 | 2.95 | 0.2038 |
| Stroke | 0.77 | 0.40 | 1.45 | 0.4106 |
| Dementia | 1.20 | 0.67 | 2.15 | 0.5442 |
| COPD | 1.01 | 0.51 | 1.99 | 0.9816 |
| RA | 1.19 | 0.61 | 2.31 | 0.6059 |
| CKD | 1.55 | 1.02 | 2.36 | 0.0386 |
| Cancer | 0.75 | 0.45 | 1.26 | 0.2757 |
| Hemodialysis | 0.78 | 0.48 | 1.26 | 0.3036 |
| Artificial Ventilation | 3.03 | 2.12 | 4.32 | <0.0001 |
| PCI | 0.25 | 0.09 | 0.65 | 0.0048 |
| IABP | 0.74 | 0.21 | 2.59 | 0.6374 |
| Catecholamines | 4.72 | 3.26 | 6.82 | <0.0001 |
| Osteoporosis | 1.85 | 0.76 | 4.50 | 0.1746 |
| HCM | 0.24 | 0.03 | 2.05 | 0.1939 |
| Sarcoidosis | 3.58 | 0.35 | 36.60 | 0.2815 |
| Af/AFL | 0.70 | 0.48 | 1.02 | 0.0632 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kusunose, K.; Okushi, Y.; Okayama, Y.; Zheng, R.; Abe, M.; Nakai, M.; Sumita, Y.; Ise, T.; Tobiume, T.; Yamaguchi, K.; et al. Association between Vitamin D and Heart Failure Mortality in 10,974 Hospitalized Individuals. Nutrients 2021, 13, 335. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020335
Kusunose K, Okushi Y, Okayama Y, Zheng R, Abe M, Nakai M, Sumita Y, Ise T, Tobiume T, Yamaguchi K, et al. Association between Vitamin D and Heart Failure Mortality in 10,974 Hospitalized Individuals. Nutrients. 2021; 13(2):335. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020335
Chicago/Turabian StyleKusunose, Kenya, Yuichiro Okushi, Yoshihiro Okayama, Robert Zheng, Miho Abe, Michikazu Nakai, Yoko Sumita, Takayuki Ise, Takeshi Tobiume, Koji Yamaguchi, and et al. 2021. "Association between Vitamin D and Heart Failure Mortality in 10,974 Hospitalized Individuals" Nutrients 13, no. 2: 335. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020335