
Effects of Three Different Family-Based Interventions in Overweight and Obese Children: The “4 Your Family” Randomized Controlled Trial

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
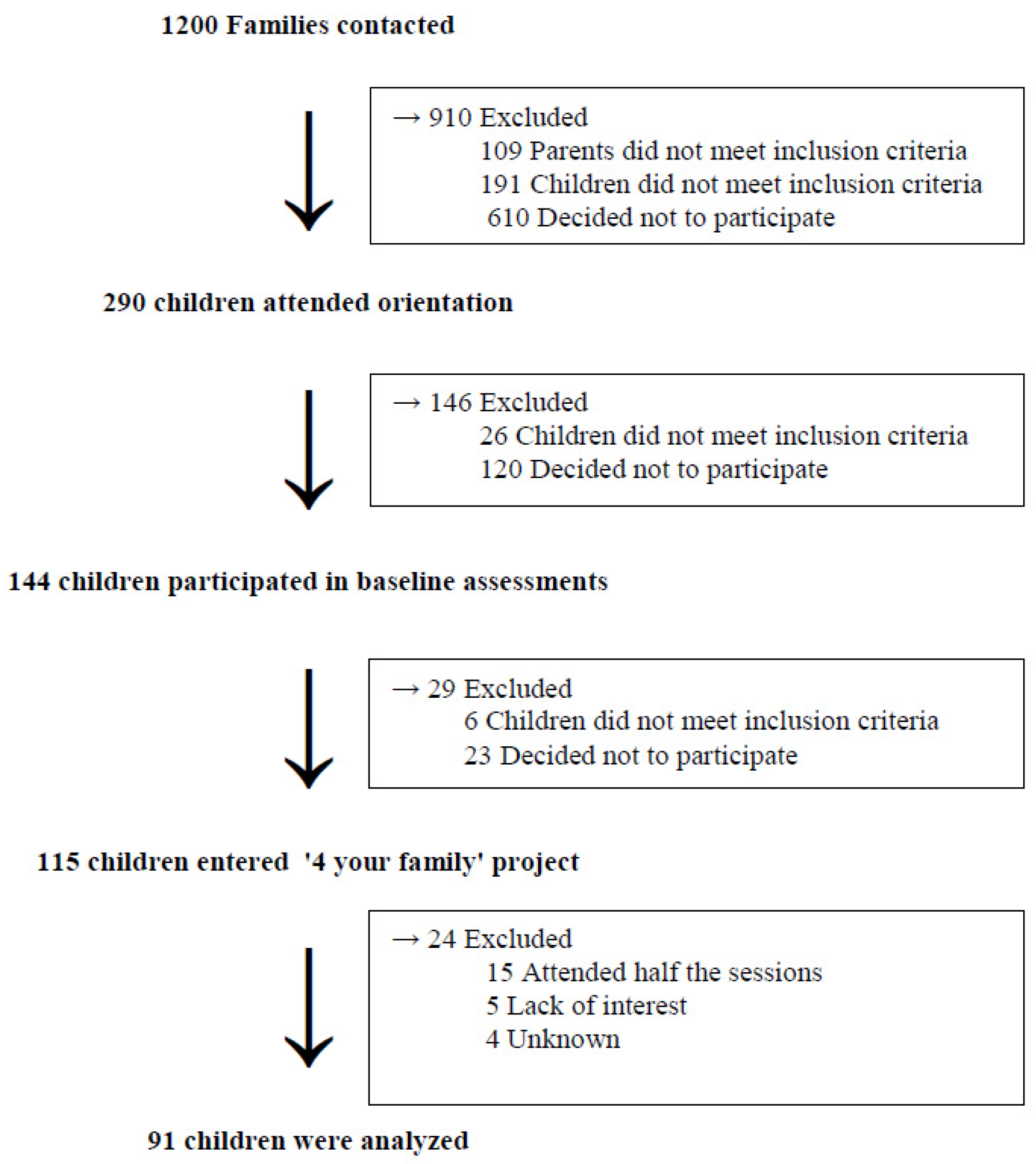
2.2. Study Procedure
2.3. Measurements
2.4. Dietary Assessment
2.5. Physical Activity Assessment and Sociodenographic Variables
2.6. Statistical Analysis
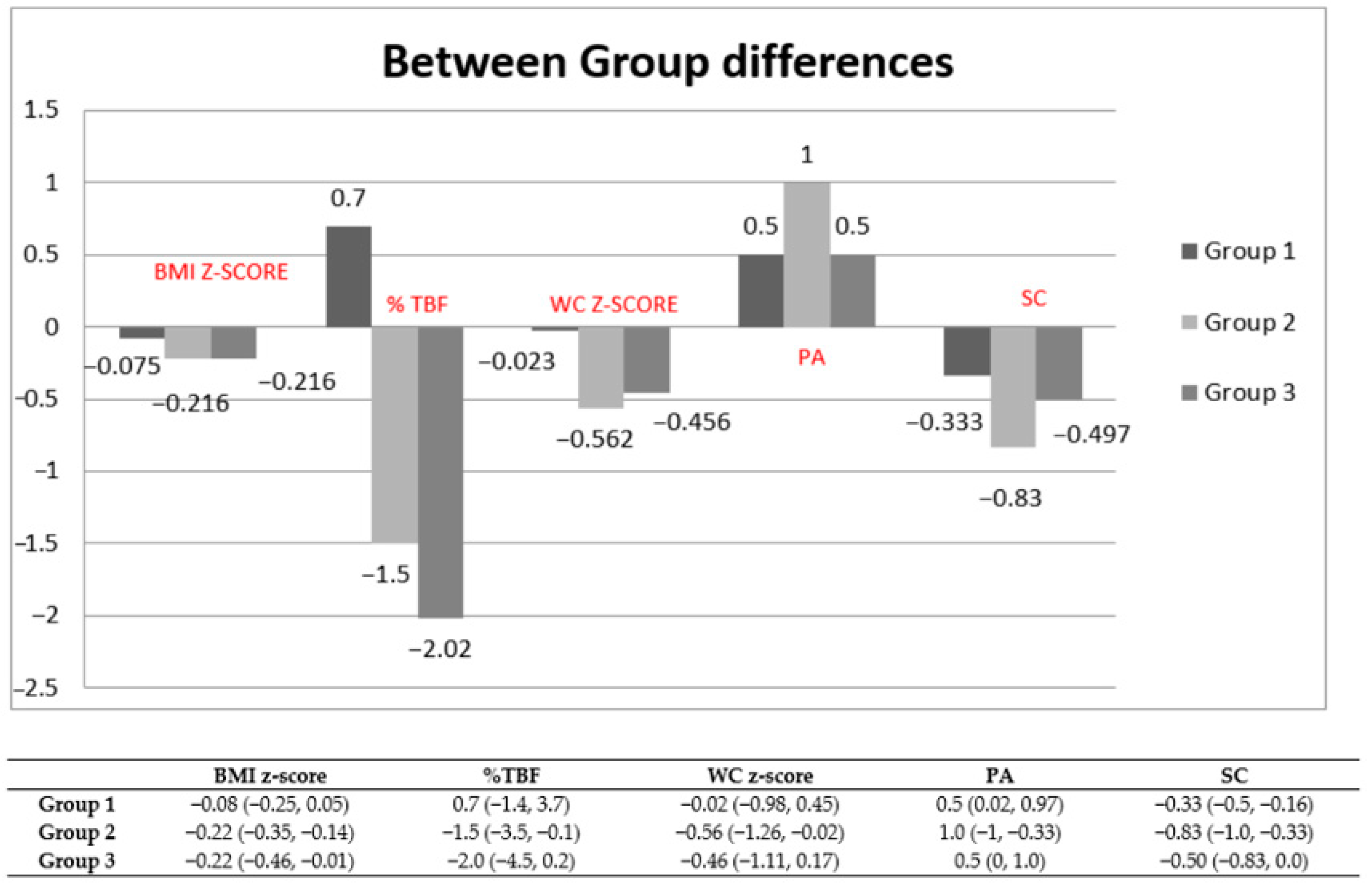
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NCD Risk Factor Collaboration (NCD-RisC). Rising rural body-mass index is the main driver of the global obesity epidemic. Nature 2019, 569, 260–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgiadis, G.; Nassis, G.P. Prevalence of overweight and obesity in a national representative sample of Greek children and adolescents. Eur. J. Clin. Nutr. 2007, 61, 1072–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moschonis, G.; Mougios, V.; Papandreou, C.; Lionis, C.; Chrousos, G.P.; Malandraki, E.; Manios, Y. “Leaner and less fit” children have a better cardiometabolic profile than their “heavier and more fit” peers, the Healthy Growth Study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Farajian, P.; Risvas, G.; Karasouli, K.; Pounis, G.D.; Kastorini, C.M.; Panagiotakos, D.B.; Zampelas, A.A. Very high childhood obesity prevalence and low adherence rates to the Mediterranean diet in Greek children, the GRECO study. Atherosclerosis 2011, 217, 525–530. [Google Scholar] [CrossRef]
- Coppock, J.H.; Ridolfi, D.R.; Hayes, J.F.; St. Paul, M.; Wilfley, D.E. Current approaches to the Management of Pediatric Overweight and Obesity. Curr. Treat. Options Cardiovasc. Med. 2014, 16, 343. [Google Scholar] [CrossRef] [Green Version]
- Berge, J.M. A review of familial correlates of child and adolescentobesity: What has the 21st century taught us so far? Inter. J. Adolesc. Med. Health 2009, 21, 457–483. [Google Scholar] [CrossRef]
- Kitzmann, K.M.; Beech, B.M. Family-based interventions for pediatric obesity, methodological and conceptual challenges from family psychology. J. Fam. Psychol. 2006, 20, 175–189. [Google Scholar] [CrossRef]
- Robertson, W.; Friede, T.; Blissett, J.; Rudolf, M.C.J.; Wallis, M.; Stewart-Brown, S. Pilot of “Families for Health”, community-based family intervention for obesity. Arch. Dis. Child. 2008, 93, 921–926. [Google Scholar] [CrossRef] [Green Version]
- Gerards, S.M.; Sleddens, E.F.; Dagnelie, P.C.; de Vries, N.K.; Kremers, S.P. Interventions addressing general parenting to prevent or treat childhood obesity. Int J. Pediatr. Obes. 2011, 6, e28–e45. [Google Scholar] [CrossRef]
- Herouvi, D.; Karanasios, E.; Karayianni, C.; Karavanaki, K. Cardiovascular disease in childhood, the role of obesity. Eur. J. Pediatrics 2013, 172, 721–732. [Google Scholar] [CrossRef]
- Mead, E.; Brown, T.; Rees, K.; Azevedo, L.B.; Whittaker, V.; Jones, D.; Olajide, J.; Mainardi, G.M.; Corpeleijn, E.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst. Rev. 2017, 6, CD012651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerards, S.M.; Dagnelie, P.C.; Jansen, M.W.; van der Goot, L.O.H.M.; de Vries, N.K.; Sanders, M.R.; Kremers, S.P.J. Lifestyle Triple P: A parenting intervention for childhood obesity. BMC Public Health 2012, 12, 267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miguel-Berges, M.L.; Santaliestra-Pasias, A.M.; Mouratidou, T.; De Miguel-Etayo, P.; Androutsos, A.; De Craemer, M.; Galcheva, S.; Koletzko, B.; Kulaga, Z.; Manios, Y.; et al. Combined Longitudinal Effect of Physical Activity and Screen Time on Food and Beverage Consumption in European Preschool Children, The ToyBox-Study. Nutrients 2019, 11, 1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Stralen, M.M.; Yıldırım, M.; Wulp, A.; te Velde, S.J.; Verloigne, M.; Doessegger, A.; Androutsos, O.; Kovacs, E.; Brug, J.; Chinapaw, M.J.M. Measured sedentary time and physical activity during the school day of European 10- to 12-year-old children, the ENERGY project. J. Sci. Med. Sport 2014, 17, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Karmali, S.; Ng, V.; Battram, D.; Burke, S.; Morrow, D.; Pearson, E.; Tucker, P.; Mantler, T.; Cramp, A.; Petrella, R.; et al. Coaching and/or education intervention for parents with overweight/obesity and their children, study protocol of a single-centre randomized controlled trial. BMC Public Health 2019, 19, 345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, W.; Thorogood, M.; Inglis, N.; Grainger, C.; Stewart-Brown, S. Two-year follow-up of the ‘Families for Health’ programme for the treatment of childhood obesity. Child. Care Health 2012, 38, 229–236. [Google Scholar] [CrossRef]
- Faith, M.S.; Van Horn, L.; Appel, L.J.; Burke, L.E.; Carson, J.A.S.; Franch, H.A.; Jakicic, J.M.; Kral, T.V.E.; Odoms-Young, A.; Wansink, B.; et al. Evaluating parents and adult caregivers as “agents of change” for treating obese children, evidence for parent behavior change strategies and research gaps, a scientific statement from the American Heart Association. Circulation 2012, 125, 1186–1207. [Google Scholar] [CrossRef] [Green Version]
- Wilfley, D.E.; Tibbs, T.L.; Van Buren, D.J.; Reach, K.P.; Walker, M.S.; Epstein, L.H. Lifestyle interventions in the treatment of childhood overweight, a meta-analytic review of randomized controlled trials. Health Psychol. 2007, 26, 521–532. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, N.; Shariff, Z.M.; Mukhtar, F.; Lye, M.S. Family-based intervention using face-to-face sessions and social media to improve Malay primary school children’s adiposity, a randomized controlled field trial of the Malaysian REDUCE programme. Nutr. J. 2018, 17, 74. [Google Scholar] [CrossRef] [Green Version]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide, international survey. Br. Med J. 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention, National Center for Health Statistics. Percentile Data Files with LMS Values. Available online: https://www.cdc.gov/growthcharts/percentile_data_files.htm (accessed on 14 January 2021).
- World Health Organization. Growth Reference 5–19 Years. Available online: https://www.who.int/growthref/who2007_bmi_for_age/en/ (accessed on 14 January 2021).
- McCarthy, H.D.; Jarrett, K.V.; Crawley, H.F. The development of waist circumference percentiles in British children aged 5.0–16.9 y. Eur. J. Clin. Nutr. 2001, 55, 902–907. [Google Scholar]
- Varagiannis, P.; Magriplis, E.; Risvas, G.; Vamvouka, K.; Nisianaki, A.; Papageorgiou, A.; Pervanidou, P.; Chrousos, G.; Zampelas, A. Validation of a Self-reported Food Frequency for Overweight and Obese Children, Using Parental 3-Day Food Records, The 4yourfamily Study. Nutr. Today 2019, 54, 151–158. [Google Scholar] [CrossRef]
- Moschonis, G.; Kalliora, A.C.; Costarelli, V.; Papandreou, C.; Koutoukidis, D.; Lionis, C.; Chrousos, G.P.; Manios, Y.; Healthy Growth Study Group. Identification of lifestyle patterns associated with obesity and fat mass in children, the Healthy Growth Study. Public Health Nutr. 2014, 17, 614–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oude Luttikhuis, H.; Baur, L.; Jansen, H.; Shrewsbury, V.A.; O’Malley, C.; Stolk, R.P.; Summerbell, C.D. WITHDRAWN, Interventions for treating obesity in children. Cochrane Database Syst. Rev. 2019, 7, 3. [Google Scholar]
- Ash, T.; Agaronov, A.; Young, T.; Aftosmes-Tobio, A.; Davison, K.K. Family-based childhood obesity prevention interventions, a systematic review and quantitative content analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 113. [Google Scholar] [CrossRef] [PubMed]
- Chai, L.K.; Collins, C.; May, C.; Brain, K.; Wong See, D.; Burrows, T. Effectiveness of family-based weight management interventions for children with overweight and obesity, an umbrella review. JBI Database Syst. Rev. Implement Rep. 2019, 17, 1341–1427. [Google Scholar] [CrossRef]
- Sacher, P.M.; Kolotourou, M.; Chadwick, P.M.; Cole, T.J.; Lawson, M.S.; Lucas, A.; Singhal, A. Randomized controlled trial of the MEND program, a family-based community intervention for childhood obesity. Obesity 2010, 18 (Suppl. 1), S62–S68. [Google Scholar] [CrossRef]
- Waters, E.; de Silva-Sanigorski, A.; Hall, B.J.; Brown, T.; Campbell, K.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, CD001871. [Google Scholar] [CrossRef]
- Kolsgaard, M.L.P.; Joner, G.; Brunborg, C.; Anderssen, S.A.; Tonstad, S.; Andersen, L.F. Reduction in BMI z-score and improvement in cardiometabolic risk factors in obese children and adolescents. The Oslo adiposity intervention study a hospital/public health nurse combined treatment. BMC Pediatr. 2011, 11, 47. [Google Scholar] [CrossRef] [Green Version]
- Robertson, W.; Fleming, J.; Kamal, A.; Hamborg, T.; Khan, K.A.; Griffiths, F.; Stewart-Brown, S.; Stallard, N.; Petrou, S.; Simkiss, D.; et al. Randomised controlled trial evaluating the effectiveness and cost-effectiveness of ‘Families for Health’, a family-based childhood obesity treatment intervention delivered in a community setting for ages 6 to 11 years. Health Technol. Assess. 2017, 21, 1–180. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in diet and lifestyle and long-term weight gain in women and men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef] [Green Version]
- FAO (Food and Agriculture Organization of the United Nations); WHO (World Health Organization); UNU (United Nations University). Human Energy Requirements. Report of a Joint FAO/WHO/UNU Expert Consultation; FAO Food and Nutrition Technical Report, Series No. 1; Rome, Italy, 2004; Available online: http://www.fao.org/3/y5686e/y5686e00.htm (accessed on 23 January 2021).
- Secretary of the Nordic Council of Ministers, Nordic Council of Ministers. Nordic Nutrition Recommendations 2012—Part-1; Secretary of the Nordic Council of Ministers, Nordic Council of Ministers: København, Denmark, 2013. [Google Scholar]
- Shang, L.; O’Loughlin, J.; Tremblay, A.; Gray-Donald, K. The association between food patterns and adiposity among Canadian children at risk of overweight. Appl. Physiol. Nutr. Metab. 2014, 39, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Nissinen, K.; Mikkilä, V.; Männistö, S.; Lahti-Koski, M.; Räsänen, L.; Viikari, J.; Raitakari, O.T. Sweets and sugar-sweetened soft drink intake in childhood in relation to adult BMI and overweight. The Cardiovascular Risk in Young Finns Study. Public Health Nutr. 2009, 12, 2018–2026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nago, E.S.; Lachat, C.K.; Dossa, R.A.; Kolsteren, P.W. Association of out-of-home eating with anthropometric changes, a systematic review of prospective studies. Crit. Rev. Food Sci. Nutr. 2014, 54, 1103–1116. [Google Scholar] [CrossRef] [PubMed]
- Bacardí-Gascon, M.; Pérez-Morales, M.E.; Jiménez-Cruz, A. A six month randomized school intervention and an 18-month follow-up intervention to prevent childhood obesity in Mexican elementary schools. Nutr. Hosp. 2012, 27, 755–762. [Google Scholar] [PubMed]
- Yackobovitch-Gavan, M.; Wolf Linhard, D.; Nagelberg, N.; Poraz, I.; Shalatin, S.; Phillip, M.; Meyerovitch, J. Intervention for childhood obesity based on parents only or parents and child compared with follow-up alone. Pediatr. Obes. 2018, 13, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.S.; Pate, R.R. Effects of exercise on BMI z-score in overweight and obese children and adolescents, a systematic review with meta-analysis. BMC Pediatr. 2014, 14, 225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C. Prevalence of Obesity among Adults and Youth: United States, 2015–2016. NCHS Data Brief 2017, 288, 1–8. [Google Scholar]
- Garrido-Miguel, M.; Oliveira, A.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Pozuelo-Carrascosa, D.P.; Soriano-Cano, A.; Martínez-Vizcaíno, V. Prevalence of Overweight and Obesity among European Preschool Children: A Systematic Review and Meta-Regression by Food Group Consumption. Nutrients 2019, 11, 1698. [Google Scholar] [CrossRef] [Green Version]
- Ruiter, E.L.M.; Saat, J.J.E.H.; Molleman, G.R.M.; Fransen, G.A.J.; Van Der Velden, K.; Van Jaarsveld, C.H.M.; Engels, R.C.M.E.; Assendelft, W.J.J. Parents’ underestimation of their child’s weight status. Moderating factors and change over time: A cross-sectional study. PLoS ONE 2020, 15, e0227761. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Group 1 | Group 2 | Group 3 | p-Value |
|---|---|---|---|---|
| Children (n) | 36 | 30 | 25 | |
| Sex (Males, n (%)) | 15 (42%) | 14 (47%) | 10 (40%) | p = 0.869 |
| Age (years) | 10.0 (9.0, 11.8) | 10.0 (9.0, 11.0) | 11.0 (9.5, 11.0) | p = 0.763 |
| Weight (kg) | 55.4 (49.7, 60.6) | 56.7 (44.7, 67.1) | 54.5 (48.8, 63.7) | p = 0.977 |
| Height (m) | 1.46 (0.08) | 1.46 (0.09) | 1.47 (0.09) | p = 0.905 |
| Obesity, n (%) | 23 (64%) | 21 (70%) | 15 (60%) | p = 0.733 |
| BMI | 25.5 (23.8, 27.8) | 26.4 (23.5, 28.6) | 25.2 (22.9, 28.4) | p = 0.953 |
| BMI z-score | 2.73 (0.6) | 2.66 (0.5) | 2.6 (0.8) | p = 0.722 |
| Total body fat (%) | 34.4 (6.6) | 34.1 (6.5) | 34 (7.1) | p = 0.970 |
| Waist circumference (cm) | 87.6 (81.6, 91.3) | 86.4 (77.5, 91.2) | 83.0 (77.5, 91.2) | p = 0.342 |
| Waist circumference z-score | 5.0 (4.2, 6.2) | 5.03 (3.7, 5.5) | 4.21 (3.1, 5.1) | p = 0.108 |
| Energy (kcal) | 1774 (402) | 1591 (284) | 1761 (388) | p = 0.096 |
| Physical activity (h/d) | 1.5 (1.0, 1.9) | 1.8 (1.5, 1.9) | 1.8 (1.3, 2.7) | p = 0.077 |
| Screen time (h/d) | 2.3 (1.5, 4.0) | 3.0 (2.0, 3.6) | 2.7 (1.7, 3.0) | p = 0.399 |
| Mother’s education (n (%)) | ||||
| ≤6 years | 0 (0%) | 1 (3%) | 2 (8%) | |
| ≤12 years | 16 (44 %) | 7 (24%) | 11 (44%) | p = 0.145 |
| >12 years | 20 (56 %) | 22 (73%) | 12 (48%) | |
| Father’s education (n (%)) | ||||
| ≤6 years | 3 (8%) | 2 (7%) | 6 (24%) | |
| ≤12 years | 16 (45%) | 8 (27%) | 4 (16%) | p = 0.053 |
| >12 years | 17 (47%) | 20 (66%) | 15 (60%) | |
| Mother’s employment (n (%)) | ||||
| Unempoloyed | 6 (17%) | 2 (7%) | 2 (8%) | |
| Homemaker | 6 (17%) | 11 (36%) | 9 (36%) | p = 0.276 |
| Employed | 24 (66%) | 17 (57%) | 14 (56%) | |
| Father’s employment (n (%)) | ||||
| Unemployed | 3 (8%) | 3 (10%) | 3 (12%) | |
| Homemaker | 0 (0%) | 0 (0%) | 0 (0%) | p = 0.894 |
| Employed | 33 (92%) | 27 (90%) | 22 (80%) |
| Children (n) | Group 1 n = 36 | Group 2 n = 30 | Group 3 n = 25 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 Month | 6 Months | p-Value a | 0 Month | 6 Months | p-Value b | 0 Month | 6 Months | p-Value a | p-Value b | Post-Hoc * | |
| Weight (kg) | 57.1 (11.9) | 61.1 (12) | 0.000 | 56.2 (13.1) | 57.8 (14.5) | 0.026 | 56.5 (11.5) | 58.9 (11.7) | 0.000 | 0.016 | Group 3 |
| Height (m) | 1.46 (0.08) | 1.51 (0.08) | 0.000 | 1.46 (0.09) | 1.49 (0.10) | 0.000 | 1.47 (0.09) | 1.51 (0.09) | 0.000 | 0.375 | |
| BMI (kg/m2) | 26.2 (3.4) | 26.6 (3.5) | 0.362 | 26.0 (3.8) | 25.3 (4.2) | 0.007 | 26.0 (3.9) | 25.4 (3.8) | 0.069 | 0.064 | |
| BMI z-score | 2.73 (0.6) | 2.60 (0.6) | 0.009 | 2.66 (0.5) | 2.38 (0.7) | 0.000 | 2.60 (0.8) | 2.36 (0.7) | 0.000 | 0.016 | Group 2 |
| %TBF | 34.4 (6.6) | 35.6 (6.6) | 0.057 | 34.1 (6.5) | 32.2 (7.8) | 0.013 | 34.0 (7.1) | 31.9 (7.8) | 0.020 | 0.001 | Group 3 |
| WC (cm) | 87.6 (7.5) | 87.2 (8.5) | 0.831 | 85.2 (9.7) | 82.2 (10.5) | 0.000 | 85.2 (9.8) | 83.5 (8.5) | 0.161 | 0.197 | |
| WC z-score | 5.27 (1.39) | 4.99 (1.51) | 0.135 | 4.70 (1.54) | 3.97 (1.71) | 0.000 | 4.63 (1.85) | 4.18 (1.71) | 0.045 | 0.112 | |
| Energy (kcal) | 1774 (402) | 1701 (403) | 0.078 | 1591 (284) | 1520 (266) | 0.136 | 1761 (388) | 1631 (354) | 0.000 | 0.334 | |
| Physical Activity (h/d) | 1.47 (1.0, 1.8) | 1.7 (1.5, 2.4) | 0.000 | 1.8 (1.5, 1.9) | 2.5 (1.8, 2.8) | 0.000 | 1.8 (1.2, 2.6) | 2.2 (1.5, 3.1) | 0.000 | 0.255 | |
| Screen time (h/d) | 2.3 (1.5, 4.0) | 2.4 (1.5, 3.4) | 0.000 | 3.0 (2.0, 3.6) | 2.0 (1.0, 3.1) | 0.000 | 2.7 (1.7, 3.0) | 2.0 (1.0, 3.0) | 0.001 | 0.010 | Group 2 |
| Food Category (Servings per Day) | Group 1 | Group 2 | Group 3 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 Month | 6 Months | p-Value a | 0 Month | 6 Months | p-Value a | 0 Month | 6 Months | p-Value a | p-Value b | Post Hoc * | |
| Fruit | 1.00 (0.43, 2.00) | 1.00 (0.42, 2.00) | 0.944 | 1.00 (0.43, 2.00) | 1.00 (1.00, 2.00) | 0.091 | 0.43 (0.21, 1.75) | 1.00 (1.0, 2.75) | 0.000 | 0.001 | Group 3 |
| Vegetable | 1.00 (0.42, 2.00) | 1.00 (0.43, 1.75) | 0.048 | 0.71 (0.11, 1.00) | 1.00 (0.42, 2.00) | 0.003 | 1.00 (0.21, 1.00) | 1.00 (0.42, 1.75) | 0.219 | 0.448 | |
| Whole wheat cereals/grains | 0.51 (0.14, 1.62) | 0.65 (0.17, 1.24) | 0.673 | 0.44 (0.13, 0.93) | 0.76 (0.25, 1.28) | 0.000 | 0.19 (0, 0.83) | 0.19 (0, 1.00) | 0.266 | 0.077 | |
| Dairy, low fat | 1.06 (0.24, 2.00) | 1.14 (0.69, 1.56) | 0.866 | 1.00 (0.35, 1.45) | 1.29 (0.89, 2.00) | 0.001 | 0.83 (0.40, 1.21) | 1.00 (0.35, 1.85) | 0.034 | 0.016 | Group 2 |
| Legumes | 0.14 (0.14, 0.28) | 0.14 (0.07, 0.28) | 0.567 | 0.14 (0.05, 0.28) | 0.14 (0.14, 0.29) | 0.338 | 0.14 (0.14, 0.28) | 0.14 (0.05, 0.30) | 0.500 | 0.328 | |
| Fish | 0.14 (0.05, 0.18) | 0.14 (0.05, 0.14) | 0.120 | 0.14 (0.05, 0.14) | 0.14 (0.13, 0.14) | 0.168 | 0.14 (0.01, 0.14) | 0.10 (0.05, 0.28) | 0.527 | 0.075 | |
| Sweet | 0.47 (0.24, 0.86) | 0.57 (0.30, 0.80) | 0.545 | 0.49 (0.29, 0.99) | 0.40 (0.29, 0.85) | 0.011 | 0.62 (0.26, 0.86) | 0.80 (0.61, 1.12) | 0.074 | 0.026 | Group 2 |
| Fast food | 0.14 (0.05, 0.23) | 0.19 (0.10, 0.23) | 0.282 | 0.14 (0.10, 0.19) | 0.10 (0.05, 0.19) | 0.004 | 0.10 (0.05, 0.31) | 0.15 (0.10, 0.26) | 0.695 | 0.018 | Group 2 |
| Processed meat | 0.05 (0, 0.28) | 0.10 (0.01, 0.37) | 0.807 | 0.1 (0.025, 0.64) | 0.05 (0, 0.35) | 0.026 | 0.20 (0.02, 0.33) | 0.19 (0.02,0.46) | 0.527 | 0.095 | |
| Sugar-sweetened beverages | 0.05 (0, 0.14) | 0.05 (0, 0.14) | 0.277 | 0.05 (0, 0.14) | 0.00 (0, 0.05) | 0.160 | 0.05 (0, 0.05) | 0.05 (0, 0.09) | 0.775 | 0.710 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varagiannis, P.; Magriplis, E.; Risvas, G.; Vamvouka, K.; Nisianaki, A.; Papageorgiou, A.; Pervanidou, P.; Chrousos, G.P.; Zampelas, A. Effects of Three Different Family-Based Interventions in Overweight and Obese Children: The “4 Your Family” Randomized Controlled Trial. Nutrients 2021, 13, 341. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020341
Varagiannis P, Magriplis E, Risvas G, Vamvouka K, Nisianaki A, Papageorgiou A, Pervanidou P, Chrousos GP, Zampelas A. Effects of Three Different Family-Based Interventions in Overweight and Obese Children: The “4 Your Family” Randomized Controlled Trial. Nutrients. 2021; 13(2):341. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020341
Chicago/Turabian StyleVaragiannis, Panagiotis, Emmanuella Magriplis, Grigoris Risvas, Katerina Vamvouka, Adamantia Nisianaki, Anna Papageorgiou, Panagiota Pervanidou, George P. Chrousos, and Antonis Zampelas. 2021. "Effects of Three Different Family-Based Interventions in Overweight and Obese Children: The “4 Your Family” Randomized Controlled Trial" Nutrients 13, no. 2: 341. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020341