
Childhood Obesity and COVID-19 Lockdown: Remarks on Eating Habits of Patients Enrolled in a Food-Education Program

 ,
,
Abstract
:1. Introduction
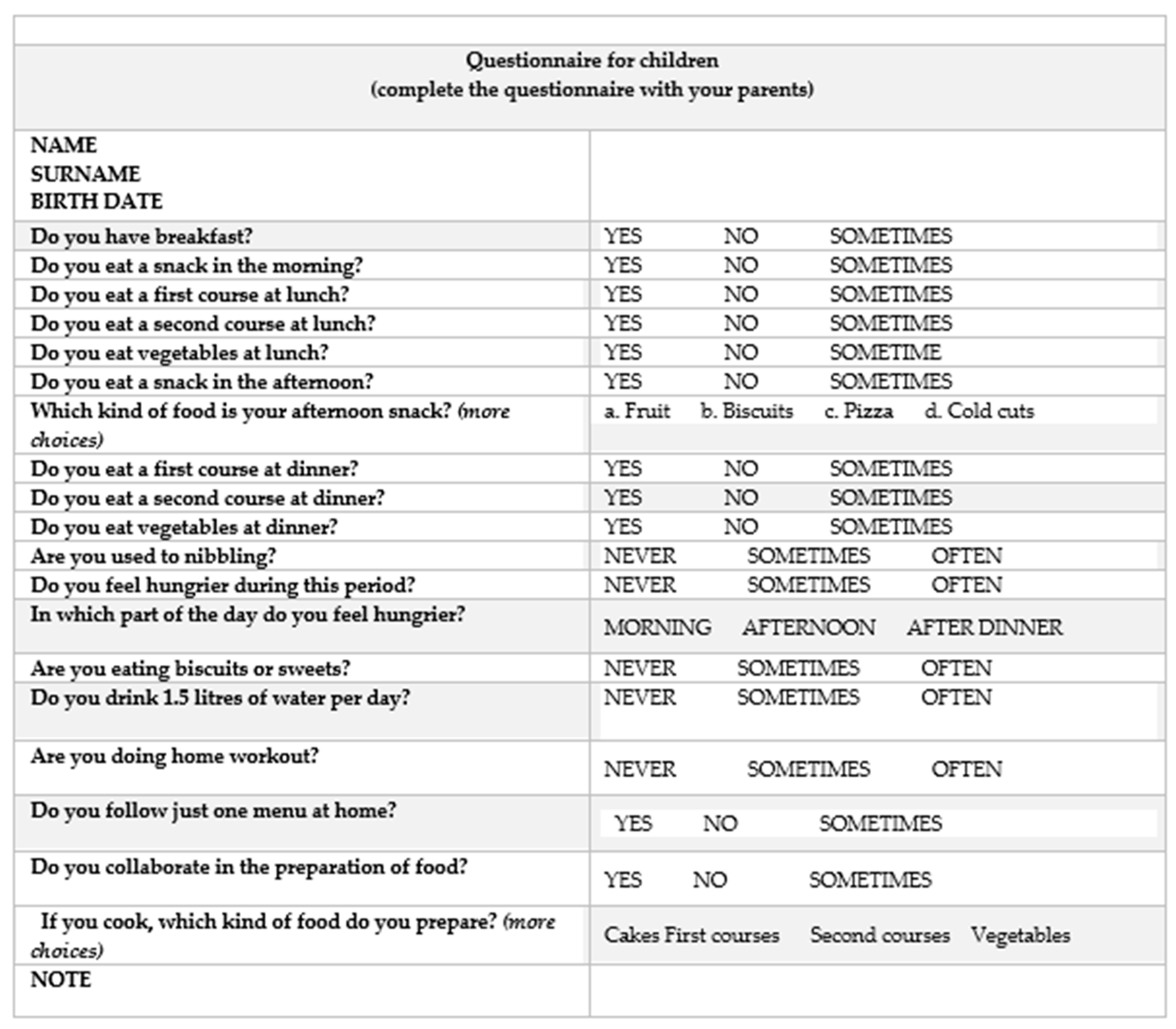
2. Materials and Methods
- “yes/no/sometimes” for 11 questions
- “often/never/sometimes” for 5 questions
- “morning/afternoon/after dinner” for one question
- types of food for 2 questions
- along with the email, families received instructions to fill in the questionnaire
- the questionnaire was to be completed by the child with the supervision of the parents
- child personal details must be entered
- only one answer was acceptable for questions with “yes/no/sometimes” or “never/sometimes/often” options
- it was specified when more answers were possible for two questions
- please send the questionnaire by replying to this email address
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Il Sistema di sorveglianza OKkio alla SALUTE: Risultati 2019. Available online: https://www.epicentro.iss.it/okkioallasalute/indagine-2019-dati (accessed on 20 November 2020).
- Franckle, R.; Adler, R.; Davison, K. Accelerated weight gain among children during summer versus school year and related racial/ethnic disparities: A systematic review. Prev. Chronic Dis. 2014, 11, E101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rundle, A.G.; Park, Y.; Herbstman, J.B.; Kinsey, E.W.; Wang, Y.C. COVID-19–Related School Closings and Risk of Weight Gain Among Children. Obesity 2020, 28, 1008–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef] [PubMed]
- Nagata, J.M.; Abdel Magid, H.S.; Pettee, G. Screen time for children and adolescents during the COVID-19 pandemic. Obesity 2020, 28, 1582–1583. [Google Scholar] [CrossRef] [PubMed]
- Lambrese, J.V. Helping children cope with the COVID-19 pandemic. Clevel. Clin. J. Med. 2020, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Singha, S.; Roy, D.; Sinhac, K.; Parveenc, S.; Sharmac, G.; Joshic, G. Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry Res. 2020, 293, 113429. [Google Scholar] [CrossRef] [PubMed]
- Emersona, L.M.; Ogieldab, C.; Rowse, G. A systematic review of the role of parents in the development of anxious cognitions in children. J. Anxiety Disord. 2019, 62, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Cherikh, F.; Frey, S.; Bel, C.; Attanasi, G.; Alifano, M.; Iannelli, A. Behavioral Food Addiction During Lockdown: Time for Awareness, Time to Prepare the Aftermath. Obes. Surg. 2020, 30, 3585–3587. [Google Scholar] [CrossRef] [PubMed]
- Chao, A.M.; Jastreboff, A.M.; White, M.A.; Grilo, C.M.; Sinha, R. Stress, Cortisol, and Other Appetite-Related Hormones: Prospective Prediction of 6-Month Changes in Food Cravings and Weight. Obesity 2017, 25, 713–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardel, M.I.; Atkinson, M.A.; Taveras, E.M.; Holm, J.C.; Kelly, A.S. Obesity Treatment Among Adolescents A Review of Current Evidence and Future Directions. JAMA Pediatr. 2020, 174, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Valerio, G.; Maffeis, C.; Saggese, G.; Ambruzzi, M.A.; Balsamo, A.; Bellone, S.; Bergamini, M.; Bernasconi, S.; Bona, G.; Calcaterra, V.; et al. Diagnosis, treatment and prevention of pediatric obesity: Consensus position statement of the Italian Society for Pediatric Endocrinology and Diabetology and the Italian Society of Pediatrics. Ital. J. Pediatr. 2018, 44, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattioli, A.V.; Pinti, M.; Farinetti, A.; Nasi, M. Obesity risk during collective quarantine for the COVID-19 epidemic. Obes. Med. 2020, 20, 100263. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, R.; Dubey, M.J.; Chatterjee, S.; Dubey, S. Impact of COVID-19 on children: Special focus on the psychosocial aspect. Minerva Pediatr. 2020, 72, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, G.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef] [PubMed]
- Michels, N.; Sioen, I.; Braet, C.; Eiben, G.; Hebestreit, A.; Huybrechts, I.; Vanaelst, B.; Vyncke, K.; De Henauw, S. Stress, emotional eating behaviour and dietary patterns in children. Appetite 2012, 59, 762–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Margaritis, I.; Houdart, S.; Ouadrhiri, Y.E.; Bigard, X.; Vuillemin, A.; Duché, P. How to deal with COVID-19 epidemicrelated lockdown physical inactivity and sedentary increase in youth? Adaptation of Anses’ benchmarks. Arch. Public Health 2020, 78, 52. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in Weight and Nutritional Habits in Adults with Obesity during the “Lockdown” Period Caused by the COVID-19 Virus Emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef]
- Lopez-Bueno, R.; Lopez-Sanchez, G.F.; Casajus, J.A.; Calatayud, J.; Gil-Salmeron, A.; Grabovac, I.; Tully, M.A.; Smith, L. Health-Related Behaviors Among School-Aged Children and Adolescents During the Spanish Covid-19 Confinement. Front. Pediatr. 2020, 8, 573. [Google Scholar] [CrossRef]
- Health Behaviour in School-Aged Children (HBSC). 2018. Available online: https://www.epicentro.iss.it/hbsc/pdf/HBSC-2018.pdf (accessed on 10 September 2020).
- Odone, A.; Lugo, A.; Amerio, A.; Borroni, E.; Bosetti, C.; Carreras, G.; Cavalieri d’Oro, G.; Colombo, P.; Fanucchi, T.; Ghislandi, S.; et al. COVID-19 lockdown impact on lifestyle habits of Italian adults. Acta Biomed. 2020, 91, 87–89. [Google Scholar] [PubMed]


{kind=link}
| Frequency (%) of Mealsand Family Habitsduring Lockdown | ||||||
| YES | NO | SOMETIMES | ||||
| BREAKFAST (*) | 75 (85.2%) | 0 (0.0%) | 13 (14.8%) | |||
| MIDMORNING SNACK (*) | 26 (29.5%) | 27 (30.7%) | 35 (39.8%) | |||
| FIRST COURSE AT LUNCH (*) | 63 (71.6%) | 7 (8.0%) | 18 (20.5%) | |||
| SECOND COURSE AT LUNCH (*) | 41 (46.6%) | 15 (17.0%) | 32 (36.4%) | |||
| VEGETABLES AT LUNCH (*) | 43 (48.9%) | 13 (14.8%) | 3 (36.4%) | |||
| AFTERNOON SNACK (*) | 72 (81.8%) | 1 (1.1%) | 15 (17.0%) | |||
| FIRST COURSE AT DINNER (*) | 5 (5.7%) | 64 (72.7%) | 19 (21.6%) | |||
| SECOND COURSE AT DINNER (*) | 76 (86.4%) | 2 (2.3%) | 10 (11.4%) | |||
| VEGETABLES AT DINNER (*) | 61 (69.3%) | 4 (4.5%) | 23 (26.1%) | |||
| FAMILY MENU (**) | 49 (55.7%) | 18 (20.5%) | 21 (23.9%) | |||
| COOKING FOOD (**) | 45 (51.1%) | 15 (17.0%) | 28 (31.8%) | |||
| Choice of different food for afternoon snack during lockdown | ||||||
| FRUIT | BISCUITS | PIZZA | COLD CUTS | |||
| FOOD FOR AFTERNOON SNACK | 72 (64.3%) | 25 (22.3%) | 4 (3.6%) | 11 (9.8%) | ||
| Frequency (%) of eating, drinking and lifestyle behaviours during lockdown | ||||||
| NEVER | SOMETIMES | OFTEN | ||||
| NIBBLING (a) | 26 (29.5%) | 46 (52.3%) | 16 (18.2%) | |||
| FEELING HUNGRY (a) | 18 (20.5%) | 44 (50.0%) | 26 (29.5%) | |||
| EATING SWEETIES AND BISCUITS (a) | 12 (13.6%) | 64 (72.7%) | 12 (13.6%) | |||
| DRINKING 1.5 LITERS OF WATER PER DAY (b) | 16 (18.2%) | 31 (35.2%) | 41 (46.6%) | |||
| HOME WORKOUT (c) | 27 (30.7%) | 42 (47.7%) | 19 (21.6%) | |||
| Children (%) and feeling hungry in different moments of the day | ||||||
| MORNING | AFTERNOON | AFTER DINNER | ||||
| FEELING HUNGRY DURING THE DAY | 14 (15.9%) | 62 (70.5%) | 12 (13.6%) | |||
| Different kinds of food cooked by the children | ||||||
| CAKES | FIRST COURSES | SECOND COURSES | VEGETABLES | |||
| FOOD COOKED | 35 (26.5%) | 48 (36.4%) | 26 (19.7%) | 23 (17.4%) | ||
| Consumption of Midmorning Snack and Feeling Hungry | ||||
| Feeling hungry | ||||
| NEVER | SOMETIMES | OFTEN | ||
| Consumption of midmorning snack | YES | 3 (11.5%) | 14 (53.9%) | 9 (34.6%) |
| NO | 9 (33.3%) | 12 (44.4%) | 6 (22.2%) | |
| SOMETIMES | 6 (17.1%) | 18 (51.4%) | 11 (31.4%) | |
| Consumption of midmorning snack and feeling hungry in a specific part of the day | ||||
| Feeling hungry in a specific part of the day | ||||
| MORNING | AFTERNOON | AFTER DINNER | ||
| Consumption of midmorning snack | YES | 4 (16.7%) | 16 (66.6%) | 4 (16.27%) |
| NO | 2 (7.4%) | 21 (77.8%) | 4 (14.8%) | |
| SOMETIMES | 8 (22.8%) | 25 (71.4%) | 2 (5.7%) | |
| Consumption of midmorning snack and nibbling | ||||
| Nibbling | ||||
| NEVER | SOMETIMES | OFTEN | ||
| Consumption of midmorning snack | YES | 9 (34.6%) | 8 (30.7%) | 9 (34.6%) |
| NO | 6 (22.2%) | 17 (62.9%) | 4 (14.8%) | |
| SOMETIMES | 11 (31.4%) | 21 (60%) | 3 (8.6%) | |
| Consumption of complete lunch | ||||
| YES | ||||
| First course, second course and vegetables | 19 (21.6%) | |||
| Consumption of complete lunch and feeling hungry in a specific part of the day | ||||
| Feeling hungry in a specific part of the day | ||||
| MORNING | AFTERNOON | AFTER DINNER | ||
| Consumption of complete lunch | YES | 3 (15.8%) | 13 (68.4%) | 3 (15.8%) |
| Consumption of midmorning snack and afternoon snack | ||||
| YES | ||||
| Midmorning snack and afternoon snack | 25(28.4%) | |||
| Consumption of midmorning snack and afternoon snack and nibbling | ||||
| Nibbling | ||||
| NEVER | SOMETIMES | OFTEN | ||
| Consumption of midmorning snack and afternoon snack | YES | 9 (36.0%) | 8 (32%) | 8 (32%) |
| Consumption of vegetables at lunch and dinner | ||||
| YES | ||||
| Vegetables at lunch and dinner | 41 (46.6%) | |||
| Group 1 Female (N = 56; 63.6%) | Group 2 Male (N = 32; 36.4%) | Chi-Square (p-Value) | Group 1 Female (N = 56; 63.6%) | Group 2 Male (N = 32; 36.4%) | Chi-Square (p-Value) | ||
|---|---|---|---|---|---|---|---|
| Do you have breakfast? | Are you used to nibbling? | ||||||
| YES | 44 (78.6%) | 31 (96.9%) | Χ2 = 5.419 (0.020) | NEVER | 13 (23.2%) | 13 (40.6%) | Χ2 = 6.457 (0.04) |
| SOMETIMES | 12 (21.4%) | 1 (3.1%) | SOMETIMES | 35 (62.5%) | 11 (34.4%) | ||
| NO | - | - | OFTEN | 8 (14.3%) | 8 (25.0%) | ||
| Do you eat a snack in the morning? | Do you feel hungrier during this period? | ||||||
| YES | 15 (26.8%) | 11 (34.4%) | Χ2 = 7.246 (0.027) | NEVER | 11 (19.6%) | 7 (21.9%) | Χ2 = 0.499 (0.779) |
| NO | 13 (23.2%) | 14 (43.8%) | SOMETIMES | 27 (48.2% | 17 (53.1%) | ||
| SOMETIMES | 28 (50.0%) | 7 (21.9%) | OFTEN | 18 (32.1%) | 8 (25.0%) | ||
| Do you eat a first course at lunch? | In which part of the day do you feel hungrier? | ||||||
| YES | 37 (66.1%) | 26 (81.3%) | Χ2 = 3.801 (0.150) | MORNING | 8 (14.3%) | 6 (18.8%) | Χ2 = 32.244 (<0.0001) |
| NO | 4 (7.1%) | 3 (9.4%) | AFTERNOON | 40 (71.4%) | 23 (71.9%) | ||
| SOMETIMES | 15 (26.8%) | 3 (9.4%) | AFTER DINNER | 8 (14.3%) | 3 (9.4%) | ||
| Do you eat a second course at lunch? | Are you eating biscuits or sweets? | ||||||
| YES | 23 (48.1%) | 18 (56.3%) | Χ2 = 2.005 (0.367) | NEVER | 8 (14.3%) | 4 (12.5%) | Χ2 = 0.919 (0.632) |
| NO | 10 (17.9%) | 5 (15.6%) | SOMETIMES | 39 (69.6%) | 25 (78.1%) | ||
| SOMETIMES | 23 (41.1%) | 9 (28.1%) | OFTEN | 9 (16.1%) | 3 (9.4%) | ||
| Do you eat vegetables at lunch? | Do you drink 1.5 litres of water per day? | ||||||
| YES | 30 (53.6%) | 13 (40.6%) | Χ2 = 1.488 (0.475) | NEVER | 11 (19.6%) | 5 (15.6%) | Χ2 = 3.438 (0.179) |
| NO | 7 (12.5%) | 6 (18.8%) | SOMETIMES | 23 (41.1%) | 8 (25.0%) | ||
| SOMETIMES | 19 (33.9%) | 13 (40.6%) | OFTEN | 22 (39.3%) | 19 59.4%) | ||
| Do you eat a snack in the afternoon? | Are you doing home workout? | ||||||
| YES | 44 (78.6%) | 28 (87.5%) | Χ2 = 3.684 (0.158) | NEVER | 15 (26.8%) | 12 (37.5%) | Χ2 = 1.117 (0.572) |
| NO | 0 (0%) | 1 (3.1%) | SOMETIMES | 28 (50.0%) | 14 (43.8%) | ||
| SOMETIMES | 12 (21.4%) | 3 (9.4%) | OFTEN | 13 (23.3%) | 6 (18.8%) | ||
| Which kind of food is your afternoon-snack? | Do you follow just one menu at home? | ||||||
| FRUIT | 45 (65.2%) | 27 (62.8%) | Χ2 = 0.545 (0.909) | NEVER | 25 (44.6%) | 24 (75.0%) | Χ2 = 7.647 (0.0022) |
| BISCUITS | 16 (23.2%) | 9 (20.9%) | SOMETIMES | 14 (25.0%) | 4 (12.5%) | ||
| PIZZA | 2 (2.9%) | 2 (4.7%) | OFTEN | 17 (30.4%) | 4 (12.5%) | ||
| COLD CUTS | 6 (8.7%) | 5 (11.6%) | |||||
| Do you eat a first course at dinner? | Do you collaborate in the preparation of food? | ||||||
| YES | 3 (5.4%) | 2 (6.3%) | Χ2 = 0.252 (0.882) | YES | 35 (62.5%) | 10 (31.5%) | Χ2 = 10.351) (0.006) |
| NO | 40 (71.4%) | 24 (75.0%) | NO | 5 (8.9%) | 10 (31.5%) | ||
| SOMETIMES | 13 (23.2%) | 6 (18.8%) | SOMETIMES | 16 (28.6%) | 12 (37.5%) | ||
| Do you eat a second course at dinner? | If you cook, which kind of food do you prepare? | ||||||
| YES | 49 (87.5%) | 27 (84.4%) | Χ2 = 3.698 (0.157) | SWEETIES | 25 (25.5%) | 10 (29.4%) | Χ2 = 2.323 (0.508) |
| NO | - | 2 (6.3%) | FIRST COURSE | 33 (33.7%) | 15 (44.1%) | ||
| SOMETIMES | 7 (12.5%) | 3 (9.4%) | SECOND COURSE | 21 (21.4%) | 5 (14.7%) | ||
| Do you eat vegetables at dinner? | VEGETABLES | 19 (19.4%) | 4 (16.7%) | ||||
| YES | 41 (73.2%) | 20 (62.5%) | Χ2 = 1.162 (0.559) | ||||
| NO | 2 (3.6%) | 2 (6.3%) | |||||
| SOMETIMES | 13 (23.2%) | 10 (31.3%) | |||||
| Group 1 Age ≤ 10 Years(N = 27; 30.7%) | Group 2 Age ≥11 Years(N = 61; 69.3%) | Chi-Square
(p-Value) | Group 1 Age ≤ 10 Years(N = 27; 30.7%) | Group 2 Age ≥ 11 Years(N = 61; 69.3%) | Chi-Square
(p-Value) | ||
|---|---|---|---|---|---|---|---|
| Do you have breakfast? | Are you used to nibbling? | ||||||
| YES | 24 (88.9%) | 51 (83.6%) | Χ2 = 0.415 (0.520) | NEVER | 8 (29.6%) | 18 (29.5%) | Χ2 = 0.004 (0.998) |
| SOMETIMES | 0 (0%) | 0 (0%) | SOMETIMES | 14 (51.8%) | 32 (52.4%) | ||
| NO | 3 (11.1%) | 10 (16.4%) | OFTEN | 5 (18.5%) | 11 (18.0%) | ||
| Do you eat a snack in the morning? | Do you feel hungrier during this period? | ||||||
| YES | 10 (37.0%) | 16 (26.2%) | Χ2 = 1.100 (0.577) | NEVER | 7 (25.9%) | 11 (18.0%) | Χ2 = 2.619 (0.270) |
| NO | 7 (25.9%) | 20 (32.8%) | SOMETIMES | 10 (37.0%) | 34 (55.7%) | ||
| SOMETIMES | 10 (37.0%) | 25 (40.9%) | OFTEN | 10 (37.0%) | 16 (26.2%) | ||
| Do you eat a first course at lunch? | In which part of the day do you feel hungrier? | ||||||
| YES | 18 (66.7%) | 45 (73.8%) | Χ2 = 0.717 (0.699) | MORNING | 6 (22.2%) | 8 (13.1%) | Χ2 = 6.053 (0.048) |
| NO | 2 (7.4%) | 5 (8.2%) | AFTERNOON | 21 (77.8%) | 42 (68.9%) | ||
| SOMETIMES | 7 (25.9%) | 11 (18.0%) | AFTER DINNER | 0 (0%) | 11 (18.0%) | ||
| Do you eat a second course at lunch? | Are you eating biscuits or sweets? | ||||||
| YES | 13 (48.2%) | 28 (45.9%) | Χ2 = 0.168 (0.919) | NEVER | 4 (14.8%) | 8 (13.1%) | Χ2 = 0.109 (0.974) |
| NO | 5 (18.5%) | 10 (16.4%) | SOMETIMES | 19 (70.4%) | 45 (73.8%) | ||
| SOMETIMES | 9 (33.3%) | 23 (37.7%) | OFTEN | 4 (14.8%) | 8 (13.1%) | ||
| Do you eat vegetables at lunch? | Do you drink 1.5 litres of water per day? | ||||||
| YES | 12 (44.4%) | 31 (50.8%) | Χ2 = 3.074 (0.215) | NEVER | 6 (22.2%) | 10 (16.4%) | Χ2 = 0.716 (0.699) |
| NO | 2 (7.4%) | 11 (18.0%) | SOMETIMES | 8 (29.6%) | 23 (37.7%) | ||
| SOMETIMES | 13 (48.1%) | 19 (31.1%) | OFTEN | 13 (48.1%) | 28 (45.9%) | ||
| Do you eat a snack in the afternoon? | Are you doing home workout? | ||||||
| YES | 25 (92.6%) | 47 (77.0%) | Χ2 = 3.118 (0.210) | NEVER | 7 (25.9%) | 20 (32.8%) | Χ2 = 4.163) (0.125) |
| NO | 0 (0%) | 1 (1.6%) | SOMETIMES | 17 (62.9%) | 25 (40.9%) | ||
| SOMETIMES | 2 (7.4%) | 13 (21.3%) | OFTEN | 3 (11.1%) | 16 (26.2%) | ||
| Which kind of food is your afternoon-snack? | Do you follow just one menu at home? | ||||||
| FRUIT | 21 (63.6%) | 51 (64.5%) | Χ2 = 0.144 (0.986) | NEVER | 13 (48.1%) | 36 (59.0%) | Χ2 = 2.044 (0.360) |
| BISCUITS | 8 (24.2%) | 17 (21.5%) | SOMETIMES | 8 (29.6%) | 10 (16.4%) | ||
| PIZZA | 1 (3.0%) | 3 (3.8%) | OFTEN | 6 (22.2%) | 15 (24.6%) | ||
| COLD CUTS | 3 (9.1%) | 8 (10.1%) | |||||
| Do you eat a first course at dinner? | Do you collaborate in the preparation of food? | ||||||
| YES | 3 (11.1%) | 2 (3.8%) | Χ2 = 2.870 (0.238) | YES | 15 (55.5%) | 30 (49.2%) | Χ2 = 0.321 (0.852) |
| NO | 17 (62.9%) | 47 (77.0%) | NO | 4 (14.8%) | 11 (18.0%) | ||
| SOMETIMES | 7 (25.9%) | 12 (19.7%) | SOMETIMES | 8 (29.6%) | 20 (32.8%) | ||
| Do you eat a second course at dinner? | If you cook, which kind of food do you prepare? | ||||||
| YES | 20 (74.1%) | 56 (91.8%) | Χ2 5.074 (0.079) | SWEETIES | 14 (31.8%) | 21 (23.9%) | Χ2 = 3.342 (0.342) |
| NO | 1 (3.7%) | 1 (1.6%) | FIRST COURSE | 12 (27.3%) | 36 (40.9%) | ||
| SOMETIMES | 6 (22.2%) | 4 (6.5%) | SECOND COURSE | 8 (18.2%) | 18 (20.4%) | ||
| Do you eat vegetables at dinner? | VEGETABLES | 10 (22.7%) | 13 (14.8%) | ||||
| YES | 17 (62.9%) | 44 (72.1%) | Χ2 = 1.060 (0.589) | ||||
| NO | 1 (3.7%) | 3 (4.9%) | |||||
| SOMETIMES | 9 (33.3%) | 14 (22.9%) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicodemo, M.; Spreghini, M.R.; Manco, M.; Wietrzykowska Sforza, R.; Morino, G. Childhood Obesity and COVID-19 Lockdown: Remarks on Eating Habits of Patients Enrolled in a Food-Education Program. Nutrients 2021, 13, 383. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020383
Nicodemo M, Spreghini MR, Manco M, Wietrzykowska Sforza R, Morino G. Childhood Obesity and COVID-19 Lockdown: Remarks on Eating Habits of Patients Enrolled in a Food-Education Program. Nutrients. 2021; 13(2):383. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020383
Chicago/Turabian StyleNicodemo, Mirella, Maria Rita Spreghini, Melania Manco, Rita Wietrzykowska Sforza, and Giuseppe Morino. 2021. "Childhood Obesity and COVID-19 Lockdown: Remarks on Eating Habits of Patients Enrolled in a Food-Education Program" Nutrients 13, no. 2: 383. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020383